



Introduction
Several studies have reported an inverse relation between height and incidence or morality of cardiovascular disease [1–10].
Although it is believed that a decline in hemoglobin levels might be a normal consequence of aging, various studies have provided accumulating evidence that anemia reflects poor health and increased risk of poor outcomes in the elderly [11,12].
On the other hand, active hematopoietic (red) bone
marrow, which plays an important role in hemato-poiesis, declines with age and is transformed into fatty (yellow) marrow from the periphery towards the axial skeleton [13]. Since the volume of bone marrow is smaller in subjects with a shorter stature compared to those with a taller stature, any reduction in the activity of hematopoietic bone marrow (hematopoiesis) could be of crucial importance for the former group.
However, no epidemiological studies clarifying the correlation between height and hematopoietic activity among elderly subjects have been conducted.
Previously, we reported that height indicates the capacity of vascular repair in elderly men with hypertension [14]. We also reported a significant positive association between hemoglobin and hypertension [15], hypertension-induced vascular damage [16], and atherosclerosis [17]. These studies indicate that hemoglobin level should act as an evaluator of the correlation between height and hematopoietic capacity, since hemoglobin level is an indicator of the necessity of vascular maintenance and hematopoietic activity.
In addition to the above, height is known to be significantly correlated with age in Japanese men [10]. Since the aim of our present study was to evaluate the influence of height on reduced capacity of hematopoietic bone marrow (hematopoiesis) with aging, we a conducted cross sectional study of elderly Japanese men within a narrow age range (65-69 years) who participated in a general health check-up in 2013-2015.
Results
No significant correlation was found between height and age in the present study population (simple correlation coefficient (r) =-0.11 (P=0.088)).
The characteristics of the study population accounting for hemoglobin concentration are shown in Table 1. Subjects with a high hemoglobin concentration (≥14.5 g/dL) had significantly higher reticulocytes, WBCs, systolic blood pressure, diastolic blood pressure, BMI, and triglycerides compared to those with a low hemoglobin concentration (<14.5 g/dL).
Table 1. Characteristics of the study population
| High hemoglobin (≥14.5 g/dL) | Low hemoglobin (<14.5 g/dL) | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of participants | 122 | 127 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 67.5 ± 1.3 | 67.2 ± 1.3 | 0.118 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reticulocytes, ‰ | 12.13 ± 3.53 | 10.43 ± 3.36 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White blood cells, cells/μL | 5739 ± 1360 | 5231 ± 1317 | 0.003 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure, mmHg | 137 ± 17 | 131 ± 18 | 0.003 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure, mmHg | 82 ± 11 | 76 ± 12 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body mass index (BMI), kg/m2 | 22.4 ± 1.8 | 21.9 ± 1.8 | 0.043 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum HDL-cholesterol (HDL), mg/dL | 57 ± 13 | 59 ± 15 | 0.425 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum triglycerides (TG), mg/dL | 114 ± 55 | 112 ± 106 | 0.043 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hemoglobin A1c (HbA1c), % | 5.8 ± 0.7 | 5.6 ± 0.5 | 0.132 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum aspartate aminotransferase (AST), IU/L | 25 ± 10 | 24 ± 7 | 0.280 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum γ-glutamyltranspeptidase (γ-GTP), IU/L | 48 ± 46 | 41 ± 34 | 0.077 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum uric acid (UA), mg/dL | 6.0 ± 1.2 | 5.8 ± 1.2 | 0.324 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum creatinine, mg/dL | 0.83 ± 0.14 | 0.84 ± 0.15 | 0.355 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Height, cm | 164.3 ± 6.2 | 164.2 ± 4.9 | 0.900 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Values are mean ± standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2 shows the simple correlation coefficient by simple regression analysis. Height showed a slight but significant positive correlation with reticulocytes for total subjects and subjects with a high hemoglobin concentration, but not for subjects with a low hemoglobin concentration (simple correlation coefficient (r) =0.13, p=0.047 for total subjects, r=0.21, p=0.019 for subjects with a high hemoglobin concentration, and r=0.02, p=0.810 for subjects with low hemoglobin).
Table 2. Simple correlation analysis of reticulocytes and other variables
| Total | High hemoglobin (≥14.5 g/dL) | Low hemoglobin (<14.5 g/dL) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| r | p | r | p | r | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of participants | 249 | 122 | 127 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | -0.07 | 0.276 | -0.16 | 0.087 | -0.04 | 0.691 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure | -0.04 | 0.577 | -0.14 | 0.137 | -0.04 | 0.691 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure | -0.06 | 0.376 | -0.15 | 0.093 | -0.09 | 0.336 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body mass index (BMI) | 0.09 | 0.166 | 0.05 | 0.553 | 0.06 | 0.470 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum HDL-cholesterol (HDL) | -0.08 | 0.221 | -0.15 | 0.092 | 0.01 | 0.910 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum triglycerides (TG) | 0.22 | 0.001 | 0.26 | 0.004 | 0.15 | 0.092 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hemoglobin A1c (HbA1c) | 0.01 | 0.892 | 0.05 | 0.617 | -0.09 | 0.300 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum aspartate aminotransferase (AST) | 0.13 | 0.038 | 0.17 | 0.057 | 0.05 | 0.593 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum γ-glutamyltranspeptidase (γ-GTP), IU/L | 0.28 | <0.001 | 0.36 | <0.001 | 0.16 | 0.070 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum uric acid (UA) | 0.12 | 0.061 | 0.12 | 0.205 | 0.10 | 0.271 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum creatinine | 0.02 | 0.809 | 0.01 | 0.917 | 0.05 | 0.570 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White blood cells | 0.32 | <0.001 | 0.42 | <0.001 | 0.15 | 0.085 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Height | 0.13 | 0.047 | 0.21 | 0.019 | 0.02 | 0.810 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| r: simple correlation coefficient. TG, γ-GTP and serum creatinine are calculated in logarithm values. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
From simple linear regression analysis, a linear correlation was observed between reticulocytes and height for total subjects and subjects with a high hemoglobin concentration, but not for subjects with a low hemoglobin concentration (Figure 1).
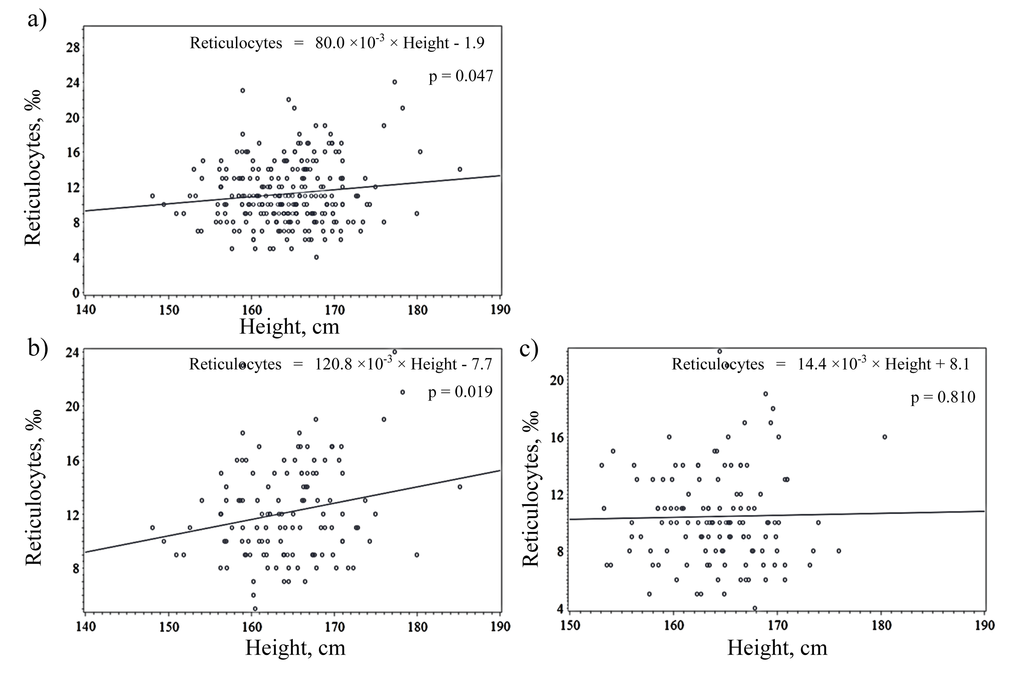
Figure 1. Simple linear regression analysis of reticulocytes and height among (a) total subjects, (b) subjects with high hemoglobin and (c) subjects with low hemoglobin.
After further adjustment for known cardiovascular risk factors and other hematological parameters (white blood cell count), this correlation became slightly stronger, as shown in Table 3 (β=0.18, p=0.003 for total subjects, β=0.28, p=0.001 for subjects with a high hemoglobin concentration, and β=0.03, p=0.717 for subjects with a low hemoglobin concentration).
Table 3. Multivariable correlation analysis of reticulocytes and other variables
| Total | High hemoglobin (≥14.5 g/dL) | Low hemoglobin (<14.5 g/dL) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β | 95% CI | p | β | 95% CI | p | β | 95% CI | p | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of participants | 249 | 122 | 127 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | -0.01 | (-0.12, 0.11) | 0.932 | -0.08 | (-0.23, 0.07) | 0.282 | 0.010 | (-0.18, 0.20) | 0.917 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure | -0.06 | (-0.18, 0.06) | 0.323 | -0.12 | (-0.28, 0.03) | 0.127 | -0.05 | (-0.22, 0.14) | 0.625 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body mass index (BMI) | 0.06 | (-0.05, 0.18) | 0.276 | 0.07 | (-0.09, 0.23) | 0.399 | 0.08 | (-0.10, 0.24) | 0.419 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum HDL-cholesterol (HDL) | 0.01 | (-0.12, 0.15) | 0.827 | -0.03 | (-0.22, 0.15) | 0.708 | 0.07 | (-0.13, 0.25) | 0.532 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum triglycerides (TG) | 0.13 | (-0.004, 0.26) | 0.056 | 0.12 | (-0.07, 0.34) | 0.190 | 0.13 | (-0.07, 0.29) | 0.232 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hemoglobin A1c (HbA1c) | -0.02 | (-0.14, 0.10) | 0.775 | 0.02 | (-0.13, 0.16) | 0.849 | -0.11 | (-0.32, 0.08) | 0.241 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum aspartate aminotransferase (AST) | 0.06 | (-0.07, 0.19) | 0.379 | 0.09 | (-0.08, 0.23) | 0.325 | -0.02 | (-0.25, 0.21) | 0.846 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum γ-glutamyltranspeptidase (γ-GTP) | 0.19 | (0.06, 0.33) | 0.006 | 0.28 | (0.09, 0.47) | 0.005 | 0.12 | (-0.09, 0.31) | 0.268 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum uric acid (UA) | 0.05 | (-0.07, 0.18) | 0.393 | -0.04 | (-0.20, 0.13) | 0.674 | 0.08 | (-0.11, 0.26) | 0.432 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum creatinine | 0.002 | (-0.12, 0.13) | 0.979 | 0.04 | (-0.13, 0.21) | 0.627 | 0.02 | (-0.17, 0.20) | 0.849 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White blood cells | 0.31 | (0.19, 0.43) | <0.001 | 0.39 | (0.22, 0.55) | <0.001 | 0.17 | (-0.02, 0.35) | 0.081 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Height | 0.18 | (0.06, 0.29) | 0.003 | 0.28 | (0.11, 0.39) | 0.001 | 0.03 | (-0.16, 0.23) | 0.717 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β: Standardized parameter estimate calculated by multiple linear regression analysis. CI: Confidence interval. TG, γ-GTP and serum creatinine are calculated in logarithm values. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
We also evaluated the correlation between height and reticulocytes limited to elderly subjects (Age≥67) (n=140), and found that the significant correlation became slightly stronger: β=0.26 (0.11, 0.40), p=0.001 for total subjects, β=0.31 (0.08, 0.47), p=0.006 for subjects with a high hemoglobin concentration (n=72), and β=0.21 (-0.03, 0.48), p=0.084 for subjects with a low hemoglobin concentration (n=68).
Discussion
The main finding of the present study was a significant positive correlation between height and reticulocyte in elderly Japanese men, especially in subjects with a high hemoglobin concentration, independent of known cardiovascular risk factors and other hematological parameters (WBC).
In a previous study, we reported an inverse association between height and normocytic normochromic anemia in Japanese men [10]. Since normocytic normochromic anemia might be caused by reduced productivity of hemoglobin in the bone marrow, we surmised that height might indicate hematopoiesis. However, a wide range of age groups (40-89 years) were employed in that study, which might have acted as a strong confounding factor with for the correlation between height and anemia and obscured the presence of any direct hematopoiesis. The present study employed subjects in a narrow age range (65-69 years) that showed no significant correlation with height (r=-0.11, p=0.088), and used reticulocyte, which directly indicates hemoglobin productivity.
However, the mechanisms underlying the positive correlation between reticulocyte and height among elderly men are not yet clear. The side population of hematopoietic stem cells in the bone marrow decreases as individuals age [18,19], which may be associated with increased frequency of anemia seen in the elderly [20]. Neumann reported a decline in active hematopoietic (red) bone marrow with age and transformation into fatty (yellow) marrow from the periphery towards the axial skeleton [13]. Since the volume of bone marrow is smaller in subjects with a shorter stature compared to those with a taller stature, any reduction in the capacity of the hematopoietic bone marrow could be of crucial importance to individuals in the former group. In our additional analysis limited to elderly subjects (age≥67), the slightly stronger correlation between height and reticulocytes among total subjects and subjects with a high hemoglobin concentration might support the above-mentioned mechanism.
We also found that the significant positive correlation between height and reticulocytes is limited to subjects with a high hemoglobin concentration. Since hemoglobin is independently positively associated with hypertension [15], hypertension-induced vascular damage [16], and atherosclerosis [17], subjects with a high hemoglobin concentration should have higher hematogenesis activity and vascular repair than subjects with low a hemoglobin concentration. Therefore, the analysis limited to subjects with a high hemoglobin concentration should emphasize hematopoietic capacity since the productivity of reticulocytes could increase by a limited level in elderly subjects.
Possible limitations of this study warrant consideration. Because creatinine clearance data were not available and estimated glomerular filtration rate (GFR) is not an effective tool for evaluating kidney function for a comparison of associations with various body heights [10,21,22], we could not perform an analysis adjusted for exact renal function. However, our study showed that the correlation between height and reticulocyte remained significant even after adjustment for serum creatinine. Next, because data for serum iron and vitamin concentrations were not available as well, we were not able to evaluate the influence of these factors. Although height is significantly positively correlated with reticulocytes in elderly Japanese men with a normal BMI, we were not able to conduct meaningful statistical analyses for subjects with an abnormal BMI status (e.g., low (<18.5kg/m2) or high (≥25.0kg/m2)) due to the limited number of participants. Since 25.6% subjects had a high BMI and 12.2% subjects had a low BMI in our present study, the influence of these subjects on the general population is tangible. However, abnormal BMI status might act as a strong confounding factor on the correlation between height and reticulocytes. Therefore, to evaluate the correlation between height and reticulocytes in these subjects, analyses with a larger population and stratification by BMI status should be conducted. Finally, because this was a cross-sectional study, causal relationships were not able to be established.
In conclusion, a significant positive correlation between height and reticulocyte was seen in elderly Japanese men. Height could act as a surrogate marker of hematopoiesis in the elderly. Since short stature is reported to be correlated with a high mortality and/or incidence of cardiovascular disease [1–10], and anemia reflects poor health and increased vulnerability to poor outcomes in older persons [11,12], these results might represent an efficient tool to clarify the underlying mechanism of risk for short stature.
Materials and Methods
Study population
To avoid the influence of age on height, this study was comprised of subjects in a narrow age range. The original population included 409 men 65 to 69 years old residing in rural communities in Nagasaki Prefecture in western Japan. Participants were recruited in 2013-2015. To avoid the influence of inflammatory and hematological disease, subjects with high and low white blood cell count (≥10,000 cells/μL (n=2) and 1,000 cells/μL< (n=1), respectively) were excluded. Also, to avoid the influence of medication activating the bone marrow, subjects taking medication for anemia (n=3) were excluded.
Since hemoglobin value shows a strong positive correlation with body mass index [15,17], and another study reported a J- or U-shaped correlation between BMI and mortality [23], abnormal BMI status might act as a strong confounding factor for the correlation between height and reticulocyte. Therefore, to avoid the influence of undernutrition and hypernutrition, subjects with a BMI<18.5kg/m2 (n=50) and BMI≥25kg/m2 (n=103), respectively, were excluded. Subjects with no evaluable laboratory data (n=1) were also excluded, leaving a total of 249 subjects participating in the study. Written consent forms were available in Japanese to ensure comprehensive understanding of the study objectives, and informed consent was signed by the participants. This study was approved by the Ethics Committee for Human Use of Nagasaki University (project registration number 0501120073).
Data collection and laboratory measurements
Trained interviewers obtained information on medical history. Body weight and height of patients wearing light clothing were measured using an automatic body composition analyzer (BF-220; Tanita, Tokyo, Japan), and body mass index (BMI; kg/m2) was calculated.
Fasting blood samples were collected in an EDTA-2K tube and a siliconized tube. Samples from the EDTA-2K tube were used to measure white blood cell count (WBC) and reticulocyte using the flow cytometry method at SRL, Inc. (Tokyo, Japan). Serum triglyceride (TG), serum high density lipoprotein (HDL) cholesterol, serum aspartate aminotransferase (AST), serum γ-glutamyltranspeptidase (γ-GTP), hemoglobin A1c (HbA1C), serum uric acid, and serum creatinine were measured using standard laboratory procedures at SRL, Inc. (Tokyo, Japan).
Statistical analysis
Characteristics of the study population stratified by hemoglobin levels concentration were expressed as mean ±standard deviation. Simple and partial correlation analysis adjusted for known cardiovascular risk factors and WBC were performed to evaluate reticulocytes and other existing parameters. We also performed simple and multiple linear regression analysis to evaluate the same. Since intercorrelation with systolic blood pressure was r= 0.73 (P<0.001), diastolic blood pressure was not analyzed as a confounding factor. Because TG, γ-GTP, and serum creatinine had a skewed distribution, logarithmic transformation was performed for the simple and partial correlation analysis, and linear regression analysis. All statistical analyses were performed with the SAS system for Windows (version 9.4; SAS Inc., Cary, NC). Probability values of less than 0.05 were considered to be statistically significant.
Acknowledgements
We are grateful to the staff of Goto City Hall and Saza Town Hall for their outstanding support.
Funding
This work was supported financially by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (No.15K07243, No.25440255, No.25291107).
Conflicts of Interest
The authors of this manuscript declare no conflict of interests.
References
- 1. Jousilahti P, Tuomilehto J, Vartiainen E, Eriksson J, Puska P. Relation of adult height to cause-specific and total mortality: a prospective follow-up study of 31,199 middle-aged men and women in Finland. Am J Epidemiol. 2000; 151:1112–20. https://doi.org/10.1093/oxfordjournals.aje.a010155 [PubMed]
- 2. Hart CL, Hole DJ, Smith GD. Risk factors and 20-year stroke mortality in men and women in the Renfrew/Paisley study in Scotland. Stroke. 1999; 30:1999–2007. https://doi.org/10.1161/01.STR.30.10.1999 [PubMed]
- 3. McCarron P, Greenwood R, Ebrahim S, Elwood P, Smith GD, and The Caerphilly and Speedwell Collaborative Studies. Adult height is inversely associated with ischaemic stroke. The Caerphilly and Speedwell collaborative studies. J Epidemiol Community Health. 2000; 54:239–40. https://doi.org/10.1136/jech.54.3.239 [PubMed]
- 4. McCarron P, Hart CL, Hole D, Smith GD. The relation between adult height and haemorrhagic and ischaemic stroke in the Renfrew/Paisley study. J Epidemiol Community Health. 2001; 55:404–05. https://doi.org/10.1136/jech.55.6.404 [PubMed]
- 5. Wannamethee SG, Shaper AG, Whincup PH, Walker M. Adult height, stroke, and coronary heart disease. Am J Epidemiol. 1998; 148:1069–76. https://doi.org/10.1093/oxfordjournals.aje.a009584 [PubMed]
- 6. Honjo K, Iso H, Inoue M, Tsugane S. Adult height and the risk of cardiovascular disease among middle aged men and women in Japan. Eur J Epidemiol. 2011; 26:13–21. https://doi.org/10.1007/s10654-010-9515-8 [PubMed]
- 7. Hozawa A, Murakami Y, Okamura T, Kadowaki T, Nakamura K, Hayakawa T, Kita Y, Nakamura Y, Okayama A, Ueshima H, and NIPPON DATA80 Research Group. Relation of adult height with stroke mortality in Japan: NIPPON DATA80. Stroke. 2007; 38:22–26. https://doi.org/10.1161/01.STR.0000251806.01676.60 [PubMed]
- 8. McCarron P, Okasha M, McEwen J, Smith GD. Height in young adulthood and risk of death from cardiorespiratory disease: a prospective study of male former students of Glasgow University, Scotland. Am J Epidemiol. 2002; 155:683–87. https://doi.org/10.1093/aje/155.8.683 [PubMed]
- 9. Song YM, Smith GD, Sung J. Adult height and cause-specific mortality: a large prospective study of South Korean men. Am J Epidemiol. 2003; 158:479–85. https://doi.org/10.1093/aje/kwg173 [PubMed]
- 10. Shimizu Y, Nakazato M, Sekita T, Kadota K, Miura Y, Arima K, Yamasaki H, Goto H, Takamura N, Aoyagi K, Maeda T. Height and drinking status in relation to risk of anemia in rural adult healthy Japanese men: the Nagasaki Islands study. Aging Male. 2015; 18:100–05. https://doi.org/10.3109/13685538.2014.942841 [PubMed]
- 11. Shavelle RM, MacKenzie R, Paculdo DR. Anemia and mortality in older persons: does the type of anemia affect survival? Int J Hematol. 2012; 95:248–56. https://doi.org/10.1007/s12185-012-1007-z [PubMed]
- 12. Zakai NA, Katz R, Hirsch C, Shlipak MG, Chaves PH, Newman AB, Cushman M. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: the Cardiovascular Health Study. Arch Intern Med. 2005; 165:2214–20. https://doi.org/10.1001/archinte.165.19.2214 [PubMed]
- 13. Cooper B. The origins of bone marrow as the seedbed of our blood: from antiquity to the time of Osler. Proc Bayl Univ Med Cent. 2011; 24:115–18. [PubMed]
- 14. Shimizu Y, Sato S, Koyamatsu J, Yamanashi H, Nagayoshi M, Kadota K, Maeda T. Height is an indicator of vascular maintenance capacity in older men. Geriatr Gerontol Int. Epub ahead of print. [PubMed]
- 15. Shimizu Y, Nakazato M, Sekita T, Kadota K, Arima K, Yamasaki H, Takamura N, Aoyagi K, Maeda T. Association between the hemoglobin levels and hypertension in relation to the BMI status in a rural Japanese population: the Nagasaki Islands Study. Intern Med. 2014; 53:435–40. https://doi.org/10.2169/internalmedicine.53.1353 [PubMed]
- 16. Shimizu Y, Kadota K, Nakazato M, Noguchi Y, Koyamatsu J, Yamanashi H, Nagayoshi M, Nagata S, Arima K, Maeda T. Hemoglobin as a possible biochemical index of hypertension-induced vascular damage. J Physiol Anthropol. 2016; 35:4. https://doi.org/10.1186/s40101-016-0085-7 [PubMed]
- 17. Shimizu Y, Nakazato M, Sekita T, Kadota K, Yamasaki H, Takamura N, Aoyagi K, Maeda T. Association between hemoglobin levels and arterial stiffness for general Japanese population in relation to body mass index status: the Nagasaki Islands study. Geriatr Gerontol Int. 2014; 14:811–18. https://doi.org/10.1111/ggi.12171 [PubMed]
- 18. Brusnahan SK, McGuire TR, Jackson JD, Lane JT, Garvin KL, O’Kane BJ, Berger AM, Tuljapurkar SR, Kessinger MA, Sharp JG. Human blood and marrow side population stem cell and Stro-1 positive bone marrow stromal cell numbers decline with age, with an increase in quality of surviving stem cells: correlation with cytokines. Mech Ageing Dev. 2010; 131:718–22. https://doi.org/10.1016/j.mad.2010.10.002 [PubMed]
- 19. Garvin K, Feschuk C, Sharp JG, Berger A. Does the number or quality of pluripotent bone marrow stem cells decrease with age? Clin Orthop Relat Res. 2007; 465:202–07. [PubMed]
- 20. Guralnik JM, Ershler WB, Schrier SL, Picozzi VJ. Anemia in the elderly: a public health crisis in hematology. Hematology (Am Soc Hematol Educ Program). 2005; 2005:528–32. https://doi.org/10.1182/asheducation-2005.1.528 [PubMed]
- 21. Shimizu Y, Nakazato M, Sekita T, Kadota K, Arima K, Yamasaki H, Goto H, Shirahama S, Takamura N, Aoyagi K, Maeda T. Relationship between adult height and body weight and risk of carotid atherosclerosis assessed in terms of carotid intima-media thickness: the Nagasaki Islands study. J Physiol Anthropol. 2013; 32:19. https://doi.org/10.1186/1880-6805-32-19 [PubMed]
- 22. Shimizu Y, Imano H, Ohira T, Kitamura A, Kiyama M, Okada T, Ishikawa Y, Shimamoto T, Yamagishi K, Tanigawa T, Iso H, and CIRCS Investigators. Adult height and body mass index in relation to risk of total stroke and its subtypes: the circulatory risk in communities study. J Stroke Cerebrovasc Dis. 2014; 23:667–74. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.06.009 [PubMed]
- 23. Engeland A, Bjørge T, Selmer RM, Tverdal A. Height and body mass index in relation to total mortality. Epidemiology. 2003; 14:293–99. https://doi.org/10.1097/01.EDE.0000047889.30616.73 [PubMed]