



Introduction
Breast cancer is mainly an aging disease, with only 5%-7% of new breast cancer cases diagnosed in young women (aged ≤40 years) in the developed world [1, 2]. However, a higher proportion of Asian women were diagnosed at a young age, especially in China, which could reach up to 22% in newly diagnosed breast cancer cases [3–5]. Young breast cancer patients represent a unique subgroup, including more advanced stages and have more aggressive tumor biology including higher tumor grade, hormone receptor negative, human epidermal growth factor receptor-2 (HER2) positive, lymphovascular invasion compared to their older counterparts [6, 7]. Aggressive biologic features have been related to inferior outcomes [1, 8–10]. However, even after adjustment for the factors mentioned above, young age remains a significant adverse prognostic factor for breast cancer-related death [11–14]. As a higher proportion of young women are diagnosed with breast cancer in developing countries, breast cancer will undoubtedly be the leading cause of cancer-related deaths and have a significant burden.
The traditional anatomic tumor (T), node (N), and metastasis (M) staging system was essential for prognostic assessment and treatment decision-making in breast cancer [15]. As the understanding of heterogeneous features in breast cancer has evolved, the lack of biologic information in the traditional American Joint Committee on Cancer (AJCC) anatomic stages has become a limitation in its prognostic assessment [15]. In light of this, the most recent AJCC 8th edition of the pathological prognostic staging system had incorporated the biologic features including histologic grade, estrogen receptor (ER), progesterone receptor (PR), and HER2 status [16, 17]. Several recent studies have validated the prognostic effect of the new staging system in breast cancer [18–20]. However, the prognostic impact of tumor biologic factors incorporated in the current staging system of young patients remains controversial [21–33]. Several prior studies showed similar or inferior outcomes related to ER-positive status in young women [21–27], while others indicated better survival rates associated with ER-positive status [28, 29]. Moreover, the effect of HER2 status on outcomes of breast cancer had an impact on the receipt of anti-HER2 therapy. HER2 positive status was associated with inferior outcomes before the era of anti-HER2 therapy, while it was related to better survival during the era of anti-HER2 therapy [30–33]. Therefore, it is not clear whether the newly proposed staging system holds true for young patients. In light of this, we conducted this validation study to evaluate the newly proposed pathological prognostic stages in young breast cancer patients using a large cohort form Surveillance, Epidemiology, and End Results (SEER) database.
Results
Patient Characteristics
Overall, 12811 women were included and assigned to both the 7th AJCC anatomic stages and the 8th AJCC pathological prognostic stages. Figure 1 depicts the patient selection flowchart for this study. Patient baseline characteristics are summarized in Table 1. The majority of women were aged 31-40 years (88.1%), with infiltrating ductal carcinoma (IDC) subtype (84.6%), stage T1-2 (86.4%), ER positive (72.7%), and HER2 negative (76.3%) disease. Pathological nodal stages included 53.5%, 33.7%, 8.5% and 4.4% in N0, N1/N1mi, N2, and N3, respectively.
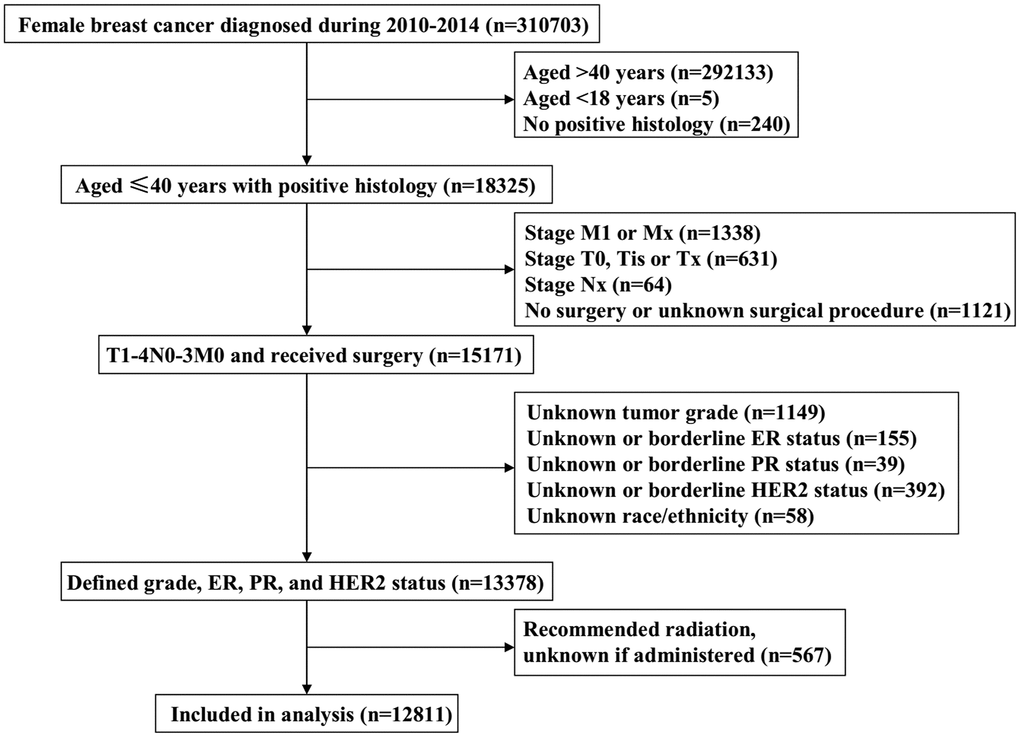
Figure 1. The patient selection flowchart of the study.
Table 1. Patient baseline characteristics.
| Variables | n (%) |
| Age (years) | |
| 18-30 | 1528 (11.9) |
| 31-40 | 11283 (88.1) |
| Race/ethnicity | |
| Non-Hispanic White | 6891 (53.8) |
| Non-Hispanic Black | 1803 (14.1) |
| Hispanic (All Races) | 2444 (19.1) |
| Other | 1673 (13.1) |
| Histological subtype | |
| Infiltrating ductal carcinoma | 10836 (84.6) |
| Invasive lobular carcinoma | 353 (2.8) |
| Other | 1622 (12.7) |
| T stage | |
| T1 | 5582 (43.6) |
| T2 | 5480 (42.8) |
| T3 | 1364 (10.6) |
| T4 | 385 (3.0) |
| N stage | |
| N0 | 6848 (53.5) |
| N1 | 4317 (33.7) |
| N2 | 1086 (8.5) |
| N3 | 560 (4.4) |
| Grade | |
| Well differentiated | 1191 (9.3) |
| Moderately differentiated | 4584 (35.8) |
| Poorly/undifferentiated | 7036 (54.9) |
| ER status | |
| Negative | 3502 (27.3) |
| Positive | 9309 (72.7) |
| PR status | |
| Negative | 4577 (35.7) |
| Positive | 8234 (64.3) |
| HER2 status | |
| Negative | 9773 (76.3) |
| Positive | 3038 (23.7) |
| Local treatment | |
| BCS+RT | 3033 (23.7) |
| BCS alone | 895 (7.0) |
| MAST | 5328 (41.6) |
| MAST+RT | 3555 (27.7) |
| Chemotherapy | |
| No | 2863 (22.3) |
| Yes | 9948 (77.7) |
BCS, breast-conservation surgery; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; MAST, mastectomy; N, nodal; RT, radiotherapy; T, tumor.
Regarding local and systemic treatments, 69.3% of patients underwent mastectomy and 30.7% of them were treated with lumpectomy. Of the lumpectomy patients, 77.2% received adjuvant radiotherapy, whereas 40.0% of patients were treated with adjuvant radiotherapy following mastectomy. Of the entire cohort, 77.7% of patients received chemotherapy.
Restaging
The stage-by-stage differences between the AJCC 7th and 8th edition-based stages are summarized in Table 2. Significant differences were found in the stage breakdown between the two edition staging systems (P<0.001). In the entire cohort, 52.8% of patients in the 7th AJCC staging system were restaged to the 8th AJCC pathological prognostic staging system, including 10.7% upstaged and 42.1% downstaged (Table 2). Overall, 92.0% of patients in the 7th edition stage IB disease were downstaged to IA disease according to the 8th edition criteria. In addition, 57.3%, 60.4%, 64.1%, and 74.8% of the 7th edition stage IIA, IIB, IIIA, and IIIC patients were also significantly downstaged, respectively (Table 2).
Table 2. The stage-by-stage differences between the 7th and 8th edition staging systems.
| 8th AJCC pathological prognostic staging system | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7th AJCC anatomic staging system | IA (%) | IB (%) | IIA (%) | IIB (%) | IIIA (%) | IIIB (%) | IIIC (%) | Total | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IA | 3359 (85.8) | 557 (14.2) | 0 | 0 | 0 | 0 | 0 | 3916 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IB | 297 (92.0) | 26 (8.0) | 0 | 0 | 0 | 0 | 0 | 323 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIA | 1411 (39.4) | 642 (17.9) | 1532 (42.7) | 0 | 0 | 0 | 0 | 3585 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIB | 99 (4.0) | 970 (38.9) | 436 (17.5) | 531 (21.3) | 460 (18.4) | 0 | 0 | 2496 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIA | 0 | 536 (33.2) | 152 (9.4) | 347 (21.5) | 326 (20.2) | 18 (1.1) | 236 (14.7) | 1615 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIB | 0 | 0 | 0 | 0 | 63 (19.9) | 148 (46.8) | 105 (33.2) | 316 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIC | 0 | 0 | 0 | 0 | 145 (25.9) | 274 (48.9) | 141 (25.2) | 560 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | 5166 (40.3) | 2731 (21.3) | 2120 (16.5) | 878 (6.9) | 994 (7.8) | 440 (3.4) | 482 (3.8) | 12811 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Orange boxes, light green boxes, and blue boxes represent those who were upstaged, downstaged, and unchanged, respectively. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For patients with IDC, 13.0% were upstaged and 40.7% were downstaged, whereas 1.1% of invasive lobular carcinoma patients were upstaged and 62.6% were downstaged (P <0.001). For patients with stage N1, N2, and N3 diseases, 64.6%, 64.0%, and 74.8% of them were downstaged (P <0.001). For patients with poorly/undifferentiated disease, 34.1% of them were downstaged, and 18.3% were upstaged. Patients with ER (38.8% vs. 2.7%, P<0.001) and PR (29.9% vs. 4.3%, P<0.001) negative disease had a more proportion of upstaging compared to those with ER and PR positive diseases. Moreover, 14.1% of HER2 negative disease were upstaged, whereas no patients were upstaged in HER2 positive patients (P<0.001) (Table 3).
Table 3. Demographic and tumor characteristics by stage change from the 7th to the 8th edition of the AJCC breast cancer staging manual.
| Variables | Downstage (%) | No change (%) | Up stage (%) | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18-30 | 662 (40.7) | 708 (46.3) | 198 (13.0) | 0.012 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 31-40 | 4750 (42.1) | 5355 (47.5) | 1178 (10.4) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race/ethnicity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic White | 2914 (42.3) | 3308 (48.0) | 669 (9.7) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic Black | 666 (36.9) | 863 (47.9) | 274 (15.2) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hispanic (All Races) | 1050 (43.0) | 1102 (45.1) | 292 (11.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 742 (44.4) | 790 (47.2) | 141 (8.4) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histological subtype | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Infiltrating ductal carcinoma | 4419 (40.8) | 5176 (47.8) | 1241 (11.5) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Invasive lobular carcinoma | 221 (62.6) | 128 (36.3) | 4 (1.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 732 (45.1) | 759 (46.8) | 131 (8.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | 1255 (22.5) | 3748 (67.1) | 579 (10.4) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 3215 (58.7) | 1817 (33.2) | 448 (8.2) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 794 (58.2) | 326 (23.9) | 244 (17.9) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 108 (28.1) | 172 (44.7) | 105 (27.3) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | 1470 (21.5) | 4696 (68.6) | 682 (10.0) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 2788 (64.6) | 999 (23.1) | 530 (12.3) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 695 (64.0) | 227 (20.9) | 164 (15.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 419 (74.8) | 141 (25.2) | 0 (0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well differentiated | 459 (38.5) | 732 (61.5) | 0 (0) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately differentiated | 2515 (54.9) | 1979 (43.2) | 90 (2.0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Poorly/undifferentiated | 2398 (34.1) | 3352 (47.6) | 1286 (18.3) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ER status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 94 (2.7) | 2048 (58.5) | 1360 (38.8) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 5278 (56.7) | 4015 (43.1) | 16 (0.2) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PR status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 197 (4.3) | 3010 (65.8) | 1370 (29.9) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 5175 (62.8) | 3053 (37.1) | 6 (0.1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HER2 status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 3985(40.8) | 4412 (45.1) | 1376 (14.1) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 1387(45.7) | 1651 (54.3) | 0 (0) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; N, nodal; T, tumor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
BCSS between the 7th and 8th edition of staging systems
With a median follow-up of 47 months, 1069 patients died, and 934 (87.4%) of them died with breast cancer-related disease. A significant difference was found in breast cancer-specific survival (BCSS) between the 7th and 8th edition of staging systems. The BCSS curves indicated more overlap lines in the 7th edition stages compared to the 8th edition stages. In the 7th AJCC staging system, curves of stage IA and IB diseases were overlapped, and curves of stage IIIB and IIIC diseases were also overlapped. Significantly differences regarding the BCSS curves were found among the 8th edition stages. The 5-year BCSS rates for the 7th edition stages were 97.0% for stage IA, 96.4% for stage IB, 93.6% for stage IIA, 89.3% for stage IIB, 81.7% for stage IIIA, 71.9% for stage IIIB, and 70.3% for stage IIIC (P<0.001) (Figure 2A). The 5-year BCSS rates for the 8th edition stages were 97.8%, 92.6%, 90.0%, 85.2%, 79.9%, 75.9%, and 56.2% in stage IA, IB, IIA, IIB, IIIA, IIIB, and IIIC diseases, respectively (P<0.001) (Figure 2B). The receiver operating characteristics (ROC) analysis showed that the new staging system had a better role in predicting the BCSS compared to 7th edition stages (area under the curve [AUC]: 0.773 vs. 0.728, P<0.001) (Figure 3).
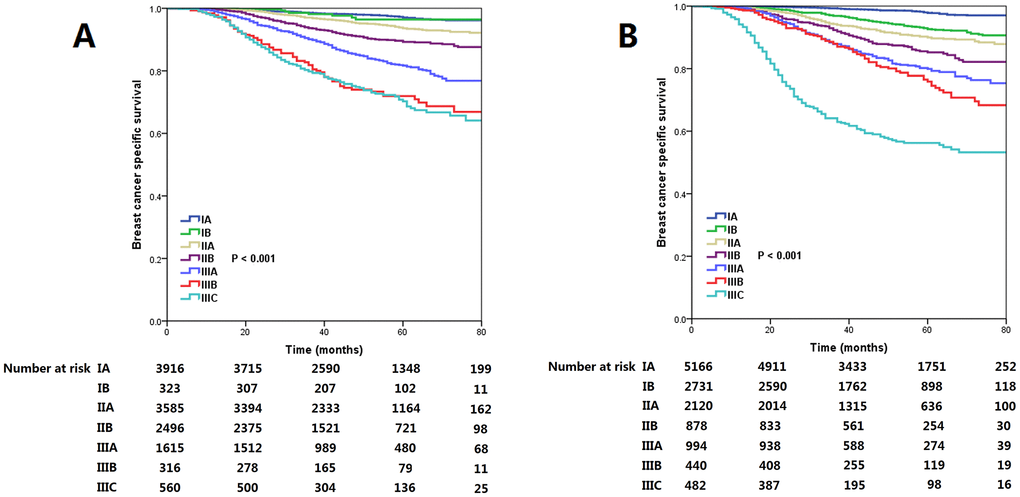
Figure 2. The breast cancer specific survival curves by the 7th (A) and 8th (B) edition of the AJCC staging systems.
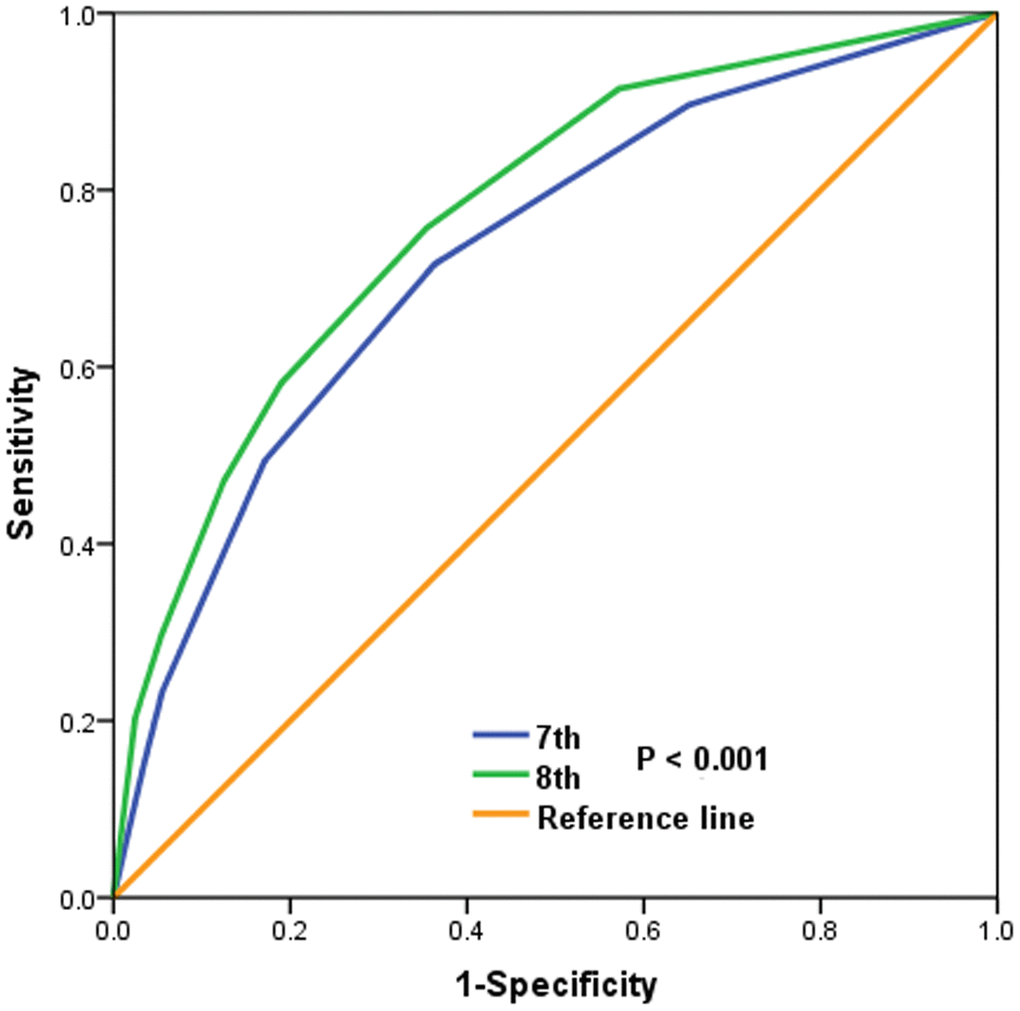
Figure 3. ROC analyses for prediction the breast cancer specific survival by the 7th and 8th edition of the AJCC staging systems.
Multivariate prognostic analysis
A Cox proportional hazard model was performed to analyze the prognostic effect among all available potential prognostic factors associated with BCSS. The results showed that race/ethnicity, T stage, N stage, tumor grade, ER, PR, and HER2 status were the independent prognostic factors related to BCSS (Table 4).
Table 4. Multivariate prognostic analysis including available potential prognostic factors.
| Variables | HR | 95%CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18-30 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 31-40 | 0.924 | 0.770-1.109 | 0.396 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race/ethnicity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic White | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic Black | 1.407 | 1.192-1.661 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hispanic (All Races) | 1.262 | 1.070-1.489 | 0.006 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.795 | 0.625-1.013 | 0.063 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histological subtype | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Infiltrating ductal carcinoma | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lobular carcinoma | 1.430 | 0.961-2.126 | 0.078 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.812 | 0.656-1.005 | 0.056 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 1.560 | 1.308-1.861 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 2.492 | 2.022-3.071 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 4.338 | 3.361-5.600 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 2.124 | 1.799-2.507 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 3.959 | 3.239-4.840 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 5.680 | 4.561-7.075 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Well differentiated | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderately differentiated | 2.038 | 1.237-3.359 | 0.005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Poorly/undifferentiated | 3.316 | 2.020-5.442 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ER status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 0.600 | 0.493-0.731 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PR status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 0.636 | 0.520-0.779 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HER2 status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Negative | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Positive | 0.464 | 0.389-0.553 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; HR, hazard ratio; PR, progesterone receptor; N, nodal; T, tumor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Next, we also performed a Cox proportional hazard analysis to compare the prognostic effect of the two stage groups on BCSS. The results showed that the 8th AJCC pathological prognostic staging system had superior overall discriminatory power to predict the BCSS. The hazard ratio (HR) of BCSS increased with the staging. When using stage IA as the reference, all categories in the 8th AJCC pathological prognostic stages showed worse BCSS with gradually increased HRs. In contrast, the 7th anatomic stages had no significant difference in BCSS using the multivariate prognostic analysis (Table 5).
Table 5. Multivariate prognostic analysis including the 7th and 8th edition staging systems.
| Variables | HR | 95%CI | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 18-30 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 31-40 | 0.925 | 0.771-1.110 | 0.402 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race/ethnicity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic White | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hispanic Black | 1.432 | 1.213-1.690 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hispanic (All Races) | 1.300 | 1.102-1.534 | 0.002 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.808 | 0.635-1.029 | 0.084 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histological subtype | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Infiltrating ductal carcinoma | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Invasive lobular carcinoma | 1.454 | 0.987-2.141 | 0.058 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.841 | 0.680-1.039 | 0.109 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7th AJCC anatomic stages | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IA | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IB | 1.165 | 0.613-2.611 | 0.526 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIA | 0.792 | 0.569-1.101 | 0.165 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIB | 0.816 | 0.580-1.147 | 0.241 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIA | 0.900 | 0.627-1.292 | 0.568 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIB | 0.986 | 0.628-1.546 | 0.950 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIC | 1.154 | 0.755-1.764 | 0.508 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 8th AJCC pathological prognostic stages | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IA | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IB | 3.474 | 2.645-4.562 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIA | 5.032 | 3.847-6.582 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIB | 7.821 | 5.841-10.473 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIA | 10.983 | 8.395-14.370 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIB | 13.468 | 9.938-18.253 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIC | 32.847 | 25.226-42.771 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; HR, hazard ratio; PR, progesterone receptor; N, nodal; T, tumor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
T stage and N stage remain the essential indicators influencing the survival outcome of breast cancer [15]. Before the 8th breast cancer prognostic stages were proposed, the traditional anatomic stages had been widely used to predict the prognosis and guide adjuvant treatment decisions. However, the traditional anatomic TNM stages might not be sufficient to reflect the survival of all patients and draw up the subsequent decision-making process. To provide more accurate prognostic information for breast cancer patients, the novel pathological prognostic stages have incorporated the ER, PR, HER2, and grade into the anatomic TNM stages [16, 17]. In our study, we validated the prognostic performance of 8th AJCC pathological prognostic stages in young breast cancer patients. In BCSS analyses, the 8th edition of AJCC prognostic stages had a better distinguish of survival compared to the traditional anatomic staging, suggesting that the newly proposed pathological prognostic stages also have prognostic significance in young patients. Our study showed that the 8th edition of AJCC pathological prognostic staging was also true when adjusted by young breast cancer patients.
We sought to investigate how many patients would be restaged in the pathological prognostic stages compared to the traditional anatomic stages. A recent study from National Cancer Data Base (n=493854) including all ages of patients, patients were diagnosed with early T stage (T1, 70.6%; T2, 25.6%; T3, 3.1%; T4, 0.7%) and N stage (N0, 75.3%; N1, 18.3%; N2, 4.4%; N3, 2.0%) compared to our study, with stage changed in 36.6% of patients (6.8% upstaged and 29.7% downstaged) [18]. A prior SEER study (n=168076) indicated that 53.2% of patients were restaged, 22.1% of patients downstaged and 31.2% of patients were upstaged [19]. In addition, a large cohort included patients from Korea (n=24014), 45.5% of patients were restaged, including 26.1% were upstaged and 19.4% were downstaged [20]. In our study, only 43.6% and 53.5% of patients were T1 stage and node-negative disease, respectively. Of the entire cohort, 52.8% of patients were restaged, including 42.1% were downstaged and 10.7% were upstaged when pathological prognostic stages were compared to anatomic stages. The differences in the distributions of the anatomic stage between young and their older counterparts may possibly explain the higher percentage of patients downstaged in young patients.
It does appear that conflicting results regarding the role of tumor biology, including tumor grade, ER, PR, and HER2 status in young breast cancer. Several prior studies showed similar or inferior outcomes related to ER positive status in young patients [21–27], while others demonstrated superior outcomes associated with ER positive status [28, 29]. It was hypothesized that young patients have lower compliance with hormonal therapy [34]. However, patients who were untreated with systemic therapy also showed inferior survival outcomes in young luminal-B patients [14]. In addition, the prognostic effect of HER2 status on survival outcomes had an impact on the receipt of the anti-HER2 therapy [29–33]. A study from Japan showed that the triple-negative breast cancer had the worst outcomes in patients aged ≤40 years, while comparable outcomes were found among the luminal A, luminal B, and HER2 overexpression subtypes [35]. Similar results were also found from the European Organisation for Research and Treatment of Cancer clinical trials [36]. However, the data on tamoxifen use was largely missing in this study, and anti-HER2 therapy was also not recorded. In the present study, patients with hormone receptor positive disease had better BCSS compared to those with hormone receptor negative disease, and we believed this was due to the advances of hormone therapy. In addition, our study also indicated that HER2-positive patients had significantly better BCSS compared to those with HER2-negative disease, which was also due to the progress of anti-HER2 treatment.
Since most patients determined in the 8th edition of the AJCC stages received multimodal therapy, including chemotherapy, hormone therapy, and anti-HER2 targeted therapy. In the current practice, patients with ER positive, PR positive, and HER2 positive were more likely to be assigned to lower stages when other staging factors were the same, while patients with ER negative, PR negative, and HER2 negative status were more likely to be assigned to higher stages. Therefore, the prognosis reflected by the new staging system was the prognosis after comprehensive standardized treatment based on the patient's clinical and biologic characteristics [16, 17]. Patients with lower stage did not mean that the patients needed less treatment, but reflected that the patients had better biologic characteristics or more effective treatment. Although patients included in our study did not have the record on hormone therapy and anti-HER2 therapy, our patients were in the era of contemporary treatment. In addition, this study confirmed that pathological prognostic stages provided more accurate information on survival compared to the anatomic stage. However, it should be noted that the AJCC 8th edition stages could accurately assess the prognosis of patients based on the routine application of anti-HER2 therapy. Therefore, the application of the newly proposed AJCC staging system should be minded in countries or regions where anti-HER2 therapy is still expensive and cannot be widely used.
A previous SEER study showed that at 0-5 years after diagnosis, ER negative patients had a higher risk of breast cancer-specific mortality than ER positive patients. However, at 5-10 years after diagnosis, ER positive disease had increased risk of breast cancer-specific mortality compared to ER negative patients [28]. Similar results from the Prospective Study of Outcomes in Sporadic and Hereditary Breast Cancer (POSH) study also showed better 5-year distant recurrence-free survival for ER positive disease compared to ER negative disease (78.5% vs. 72.5%). However, comparable 8-year distant recurrence-free survival was found between ER positive and ER negative disease [37]. The long-term study from POSH also confirmed patients with ER positive tumors had comparable overall survival compared to those with ER negative tumors in both HER2 positive and HER2 negative subgroups [38]. It should be noted that the median follow-up was only 47 in our study. In addition, the median follow-up was only 37.6 months in patients that included in the determination of the 8th AJCC pathological prognostic staging system [16, 17]. Extended use of hormone therapy has currently recommended in young patients [39, 40], but the use of hormone therapy in our study and the patient's determination of the 8th AJCC pathological prognostic staging system have not yet reached 10-years. Therefore, long-term follow-up results are still needed to verify the effect of the new staging system in young breast cancer patients.
The significant strength of our study is that we used a large population-based cohort to evaluate the prognostic performance of the newly proposed pathological prognostic staging system in younger patients. In addition, the patients included in this study were in the modern treatment mode, which makes our study valuable and unique. However, several limitations should be recognized in our study. First, potential intrinsic bias should not be neglected by the nature of the retrospective studies. Second, the details of hormone therapy, anti-HER2 treatment, and chemotherapy were not recorded in the SEER database, which might impact the prognostic assessment. Third, the length of follow-up was inadequate in our study. Finally, long-term results regarding the outcomes for patients with various pathological prognostic stages are needed to further validate the prognostic performance of newly proposed pathological prognostic staging system in younger patients.
In conclusion, our study suggests that the novel pathological staging system could provide more accurate prognostic stratification for young women with breast cancer because of the high proportion of stage migration. More studies with long-term follow-up are needed to confirm the validity of this staging system and guide treatment-decision making in younger breast cancer patients.
Materials and Methods
Patients
Young women diagnosed with breast cancer from 2010 to 2014 were identified using the SEER database. SEER database is a population-based cancer registry, which including information on cancer incidence, demographic and tumor features, the first course of treatment, and outcomes for approximately 28% of the United States population [41]. We identified patients who met the following criteria: T1-4N0-3M0 invasive breast cancer; aged ≤40 years; treatment with breast-conservation surgery or mastectomy; available variables including tumor grade, ER status, PR status, HER2 status, and race/ethnicity. Patients with aged <18 years, non-positive pathological diagnoses, and unavailable of local treatment procedures were excluded. The present study was exempted from approval by the Institutional Review Board due to the de-identified information was included in the SEER program.
Variables
We identified the following patients’ demographic and clinicopathological information: age, race/ethnicity, T stage, N stage, tumor grade, histology, ER, PR, and HER2 status. Moreover, the receipt of chemotherapy and local treatment procedures, including surgery and radiotherapy, were also identified in this study. The pathological prognostic stages were assigned according to the newly proposed AJCC breast cancer pathological prognostic staging manual [16, 17].
Statistical analysis
Comparisons of the proportions of upstage or downstage classifications between the 7th edition of the AJCC anatomic stages and the 8th edition of the AJCC pathological prognostic stages were performed using the chi-squared test or fisher's exact test. BCSS was estimated from the time of diagnosis of breast cancer to the time of death from breast cancer or the follow-up cutoff. Survival curves were plotted using the Kaplan–Meier method and the significant difference among different stages was compared using the log-rank test. The AUC was estimated to compare the model fit using the ROC curve. Cox proportional hazards model was used to determine the independent prognostic factors associated with BCSS. All statistical analyses were conducted by IBM SPSS 22.0 software package (IBM Corp., Armonk, NY). Two-sided P values <0.05 were considered statistically significant.
Author Contributions
LCY and SGW designed the study; JZ, JL, CLL, LH, and JW collected and analyzed the data; JZ, JL, and CLL wrote the article; all authors provided study materials and approved the article.
Conflicts of Interest
The authors declare that they have no conflicts of interests.
Funding
This work was partly supported by the National Natural Science Foundation of China (No. 81802600), the Commission Young and Middle-aged Talents Training Project of Fujian Health Commission (No. 2019-ZQNB-25), and the Fundamental Research Funds for the Central Universities (No. 20720180042).
References
- 1. American Cancer Society. Breast Cancer Facts and Figures 2013-2014. Atlanta (GA): American Cancer Society; 2013.
- 2. Brinton LA, Sherman ME, Carreon JD, Anderson WF. Recent trends in breast cancer among younger women in the United States. J Natl Cancer Inst. 2008; 100:1643–48. https://doi.org/10.1093/jnci/djn344 [PubMed]
- 3. Lin CH, Chuang PY, Chiang CJ, Lu YS, Cheng AL, Kuo WH, Huang CS, Lai MS, You SL, Tang CH. Distinct clinicopathological features and prognosis of emerging young-female breast cancer in an East Asian country: a nationwide cancer registry-based study. Oncologist. 2014; 19:583–91. https://doi.org/10.1634/theoncologist.2014-0047 [PubMed]
- 4. Nematolahi S, Ayatollahi SMT. A comparison of breast cancer survival among young, middle-aged, and elderly patients in southern Iran using Cox and empirical Bayesian additive hazard models. Epidemiol Health. 2017; 39:e2017043. https://doi.org/10.4178/epih.e2017043 [PubMed]
- 5. Wang K, Ren Y, Li H, Zheng K, Jiang J, Zou T, Ma B, Li H, Liu Q, Ou J, Wang L, Wei W, He J, Ren G. Comparison of Clinicopathological Features and Treatments between Young (≤40 Years) and Older (>40 Years) Female Breast Cancer Patients in West China: A Retrospective, Epidemiological, Multicenter, Case Only Study. PLoS One. 2016; 11:e0152312. https://doi.org/10.1371/journal.pone.0152312 [PubMed]
- 6. Azim HA
Jr , Partridge AH. Biology of breast cancer in young women. Breast Cancer Res. 2014; 16:427. https://doi.org/10.1186/s13058-014-0427-5 [PubMed] - 7. Tichy JR, Lim E, Anders CK. Breast cancer in adolescents and young adults: a review with a focus on biology. J Natl Compr Canc Netw. 2013; 11:1060–69. https://doi.org/10.6004/jnccn.2013.0128 [PubMed]
- 8. Wapnir IL, Anderson SJ, Mamounas EP, Geyer CE
Jr , Jeong JH, Tan-Chiu E, Fisher B, Wolmark N. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five National Surgical Adjuvant Breast and Bowel Project node-positive adjuvant breast cancer trials. J Clin Oncol. 2006; 24:2028–37. https://doi.org/10.1200/JCO.2005.04.3273 [PubMed] - 9. Anders CK, Fan C, Parker JS, Carey LA, Blackwell KL, Klauber-DeMore N, Perou CM. Breast carcinomas arising at a young age: unique biology or a surrogate for aggressive intrinsic subtypes? J Clin Oncol. 2011; 29:e18–20. https://doi.org/10.1200/JCO.2010.28.9199 [PubMed]
- 10. Fu J, Wu L, Fu W, Tan Y, Xu T, Hong Z, Wang F, Li S. How Young Is Too Young in Breast Cancer?-Young Breast Cancer Is Not a Unique Biological Subtype. Clin Breast Cancer. 2018; 18:e25–39. https://doi.org/10.1016/j.clbc.2017.05.015 [PubMed]
- 11. Bharat A, Aft RL, Gao F, Margenthaler JA. Patient and tumor characteristics associated with increased mortality in young women (< or =40 years) with breast cancer. J Surg Oncol. 2009; 100:248–51. https://doi.org/10.1002/jso.21268 [PubMed]
- 12. Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, Lindman H. Breast cancer in young women: poor survival despite intensive treatment. PLoS One. 2009; 4:e7695. https://doi.org/10.1371/journal.pone.0007695 [PubMed]
- 13. Narod SA. Breast cancer in young women. Nat Rev Clin Oncol. 2012; 9:460–70. https://doi.org/10.1038/nrclinonc.2012.102 [PubMed]
- 14. Azim HA
Jr , Michiels S, Bedard PL, Singhal SK, Criscitiello C, Ignatiadis M, Haibe-Kains B, Piccart MJ, Sotiriou C, Loi S. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin Cancer Res. 2012; 18:1341–51. https://doi.org/10.1158/1078-0432.CCR-11-2599 [PubMed] - 15. Plichta JK, Campbell BM, Mittendorf EA, Hwang ES. Anatomy and Breast Cancer Staging: Is It Still Relevant? Surg Oncol Clin N Am. 2018; 27:51–67. https://doi.org/10.1016/j.soc.2017.07.010 [PubMed]
- 16. AJCC cancer staging manual. New York: Springer International Publishing, 2018.
- 17. Giuliano AE, Connolly JL, Edge SB, Mittendorf EA, Rugo HS, Solin LJ, Weaver DL, Winchester DJ, Hortobagyi GN. Breast Cancer-Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017; 67:290–303. https://doi.org/10.3322/caac.21393 [PubMed]
- 18. Plichta JK, Ren Y, Thomas SM, Greenup RA, Fayanju OM, Rosenberger LH, Hyslop T, Hwang ES. Implications for Breast Cancer Restaging Based on the 8th Edition AJCC Staging Manual. Ann Surg. 2020; 271:169–176. https://doi.org/10.1097/SLA.0000000000003071 [PubMed]
- 19. Shao N, Xie C, Shi Y, Ye R, Long J, Shi H, Shan Z, Thompson AM, Lin Y. Comparison of the 7th and 8th edition of American Joint Committee on Cancer (AJCC) staging systems for breast cancer patients: a Surveillance, Epidemiology and End Results (SEER) Analysis. Cancer Manag Res. 2019; 11:1433–42. https://doi.org/10.2147/CMAR.S185212 [PubMed]
- 20. Kim I, Choi HJ, Ryu JM, Lee SK, Yu JH, Kim SW, Nam SJ, Lee JE. Prognostic Validation of the American Joint Committee on Cancer 8th Staging System in 24,014 Korean Patients with Breast Cancer. J Breast Cancer. 2018; 21:173–81. https://doi.org/10.4048/jbc.2018.21.2.173 [PubMed]
- 21. Aebi S, Gelber S, Castiglione-Gertsch M, Gelber RD, Collins J, Thürlimann B, Rudenstam CM, Lindtner J, Crivellari D, Cortes-Funes H, Simoncini E, Werner ID, Coates AS, Goldhirsch A. Is chemotherapy alone adequate for young women with oestrogen-receptor-positive breast cancer? Lancet. 2000; 355:1869–74. https://doi.org/10.1016/s0140-6736(00)02292-3 [PubMed]
- 22. Ahn SH, Son BH, Kim SW, Kim SI, Jeong J, Ko SS, Han W; Korean Breast Cancer Society. Poor outcome of hormone receptor-positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea–a report from the Korean Breast Cancer Society. J Clin Oncol. 2007; 25:2360–8. https://doi.org/10.1200/JCO.2006.10.3754 [PubMed]
- 23. Larson KE, Grobmyer SR, Valente SA. Evaluation of recurrence patterns and survival in modern series of young women with breast cancer. Breast J. 2018; 24:749–54. https://doi.org/10.1111/tbj.13041 [PubMed]
- 24. Sopik V, Sun P, Narod SA. The prognostic effect of estrogen receptor status differs for younger versus older breast cancer patients. Breast Cancer Res Treat. 2017; 165:391–402. https://doi.org/10.1007/s10549-017-4333-2 [PubMed]
- 25. Plichta JK, Rai U, Tang R, Coopey SB, Buckley JM, Gadd MA, Specht MC, Hughes KS, Taghian AG, Smith BL. Factors Associated with Recurrence Rates and Long-Term Survival in Women Diagnosed with Breast Cancer Ages 40 and Younger. Ann Surg Oncol. 2016; 23:3212–20. https://doi.org/10.1245/s10434-016-5404-z [PubMed]
- 26. Cao JQ, Truong PT, Olivotto IA, Olson R, Coulombe G, Keyes M, Weir L, Gelmon K, Bernstein V, Woods R, Speers C, Tyldesley S. Should women younger than 40 years of age with invasive breast cancer have a mastectomy? 15-year outcomes in a population-based cohort. Int J Radiat Oncol Biol Phys. 2014; 90:509–17. https://doi.org/10.1016/j.ijrobp.2014.06.041 [PubMed]
- 27. Bollet MA, Sigal-Zafrani B, Mazeau V, Savignoni A, de la Rochefordière A, Vincent-Salomon A, Salmon R, Campana F, Kirova YM, Dendale R, Fourquet A. Age remains the first prognostic factor for loco-regional breast cancer recurrence in young (<40 years) women treated with breast conserving surgery first. Radiother Oncol. 2007; 82:272–80. https://doi.org/10.1016/j.radonc.2007.01.001 [PubMed]
- 28. Yu KD, Wu J, Shen ZZ, Shao ZM. Hazard of breast cancer-specific mortality among women with estrogen receptor-positive breast cancer after five years from diagnosis: implication for extended endocrine therapy. J Clin Endocrinol Metab. 2012; 97:E2201–09. https://doi.org/10.1210/jc.2012-2423 [PubMed]
- 29. De Lima Vazquez F, Silva TB, Da Costa Vieira RA, Da Costa AM, Scapulatempo C, Fregnani JH, Mauad EC, Longatto A, Syrjänen KJ. Retrospective analysis of breast cancer prognosis among young and older women in a Brazilian cohort of 738 patients, 1985-2002. Oncol Lett. 2016; 12:4911–24. https://doi.org/10.3892/ol.2016.5360 [PubMed]
- 30. Andrulis IL, Bull SB, Blackstein ME, Sutherland D, Mak C, Sidlofsky S, Pritzker KP, Hartwick RW, Hanna W, Lickley L, Wilkinson R, Qizilbash A, Ambus U, et al, and Toronto Breast Cancer Study Group. neu/erbB-2 amplification identifies a poor-prognosis group of women with node-negative breast cancer. J Clin Oncol. 1998; 16:1340–49. https://doi.org/10.1200/JCO.1998.16.4.1340 [PubMed]
- 31. Perez EA, Romond EH, Suman VJ, Jeong JH, Sledge G, Geyer CE
Jr , Martino S, Rastogi P, Gralow J, Swain SM, Winer EP, Colon-Otero G, Davidson NE, et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2-positive breast cancer: planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J Clin Oncol. 2014; 32:3744–52. https://doi.org/10.1200/JCO.2014.55.5730 [PubMed] - 32. Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, Tjulandin S, Zambetti M, Vazquez F, Byakhow M, Lichinitser M, Climent MA, Ciruelos E, Ojeda B, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010; 375:377–84. https://doi.org/10.1016/S0140-6736(09)61964-4 [PubMed]
- 33. Alabdulkareem H, Pinchinat T, Khan S, Landers A, Christos P, Simmons R, Moo TA. The impact of molecular subtype on breast cancer recurrence in young women treated with contemporary adjuvant therapy. Breast J. 2018; 24:148–53. https://doi.org/10.1111/tbj.12853 [PubMed]
- 34. Murphy CC, Bartholomew LK, Carpentier MY, Bluethmann SM, Vernon SW. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: a systematic review. Breast Cancer Res Treat. 2012; 134:459–78. https://doi.org/10.1007/s10549-012-2114-5 [PubMed]
- 35. Yoshida M, Shimizu C, Fukutomi T, Tsuda H, Kinoshita T, Akashi-Tanaka S, Ando M, Hojo T, Fujiwara Y. Prognostic factors in young Japanese women with breast cancer: prognostic value of age at diagnosis. Jpn J Clin Oncol. 2011; 41:180–89. https://doi.org/10.1093/jjco/hyq191 [PubMed]
- 36. van der Hage JA, Mieog JS, van de Velde CJ, Putter H, Bartelink H, van de Vijver MJ. Impact of established prognostic factors and molecular subtype in very young breast cancer patients: pooled analysis of four EORTC randomized controlled trials. Breast Cancer Res. 2011; 13:R68. https://doi.org/10.1186/bcr2908 [PubMed]
- 37. Copson E, Maishman T, Gerty S, Eccles B, Stanton L, Cutress RI, Altman DG, Durcan L, Simmonds P, Jones L, Tapper W, Eccles D, and POSH study steering group. Ethnicity and outcome of young breast cancer patients in the United Kingdom: the POSH study. Br J Cancer. 2014; 110:230–41. https://doi.org/10.1038/bjc.2013.650 [PubMed]
- 38. Copson E, Eccles B, Maishman T, Gerty S, Stanton L, Cutress RI, Altman DG, Durcan L, Simmonds P, Lawrence G, Jones L, Bliss J, Eccles D, and POSH Study Steering Group. Prospective observational study of breast cancer treatment outcomes for UK women aged 18-40 years at diagnosis: the POSH study. J Natl Cancer Inst. 2013; 105:978–88. https://doi.org/10.1093/jnci/djt134 [PubMed]
- 39. Munzone E, Colleoni M. Optimal management of luminal breast cancer: how much endocrine therapy is long enough? Ther Adv Med Oncol. 2018; 10:1758835918777437. https://doi.org/10.1177/1758835918777437 [PubMed]
- 40. Mathew A, Davidson NE. Adjuvant endocrine therapy for premenopausal women with hormone-responsive breast cancer. Breast. 2015 (Suppl 2); 24:S120–25. https://doi.org/10.1016/j.breast.2015.07.027 [PubMed]
- 41. Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence - SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975-2016 varying) - Linked To County Attributes - Total U.S., 1969-2017 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2019, based on the November 2018 submission. https://seer.cancer.gov/.