



Introduction
The risk of stroke recurrence is high after acute minor stroke or transient ischemic attack (TIA). [1] The Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack study showed that combination of clopidogrel and aspirin with 24 hours could reduce the risk of stroke in 90 days without increasing the risk of hemorrhage. [2] However, the subsequent analysis found that the application of clopidogrel and aspirin compared with aspirin alone reduced the risk of recurrent stroke only in patients who were non-carriers of the CYP2C19 loss-of-function (LOF) alleles. [3] The polymorphisms of the CYP2C19 gene have been identified to play a significant role in the metabolism of clopidogrel. [4] Previous study showed that about 40-60% Asian participants were carriers of CYP2C19 LOF alleles, who could not benefit from clopidogrel. [3]
Ticagrelor is a new, oral, direct-acting, and reversible P2Y12 ADP receptor blocker which does not require metabolic activation. Several studies showed that ticagrelor possessed a faster and greater antiplatelet effect and was more effective than clopidogrel irrespective of variants in the CYP2C19 genotype in cardiovascular disease. [5, 6] The Acute Stroke or Transient Ischemic Attack Treated with Aspirin or Ticagrelor and Patient Outcomes (SOCRATES) trial was the first study to compare the efficacy and safety of ticagrelor versus aspirin in patients with acute ischemic stroke or TIA, but did not find a significant result. [7] However, the subgroup analysis of the SOCRATES trial [8] indicated that ticagrelor might be superior to aspirin at preventing atherosclerotic origin cerebrovascular events. Whether patients can benefit from more intensive antiplatelet therapy-combination of ticagrelor and aspirin remains controversial. Recently, the Platelet Reactivity In Non-disabling Cerebrovascular Events (PRINCE) study reported that patients with minor stroke or TIA treated with ticagrelor/aspirin had a lower proportion of high on-treatment platelet reactivity (HOPR), especially in carriers of the CYP2C19 LOF alleles compared with those treated with clopidogrel/aspirin. [9]
This sub-analysis aimed to investigate the effect of ticagrelor/aspirin on HOPR and inhibition of platelet aggregation (IPA) during study time course stratified by CYP2C19 metabolizer status compared with clopidogrel/aspirin.
Results
Study flow was shown in Figure 1. We conducted valid measurements in 376 and 373 patients for VerifyNow P2Y12 assay at 2 hours and 24 hours after first dose respectively. A total of 365 out of 675 patients with acute minor stroke and TIA were finally included in our early test sub-study with no patient missed CYP2C19 genotype data or lost to follow up. Patients included tended to be older, have a history of dyslipidemia, use statin and aspirin before randomization (Table 1). Among the 365 included patients, 105 (28.8%) of them were female, the average age was 61.7±8.5 years, 199 (54.5%) of them were classified as carriers of CYP2C19 LOF alleles, 180 (49.3%) of them received ticagrelor/aspirin therapy and 185 (50.7%) of them received clopidogrel/aspirin therapy (Table 2). Baseline characteristics between LOF allele carriers and non-carriers were well balanced.
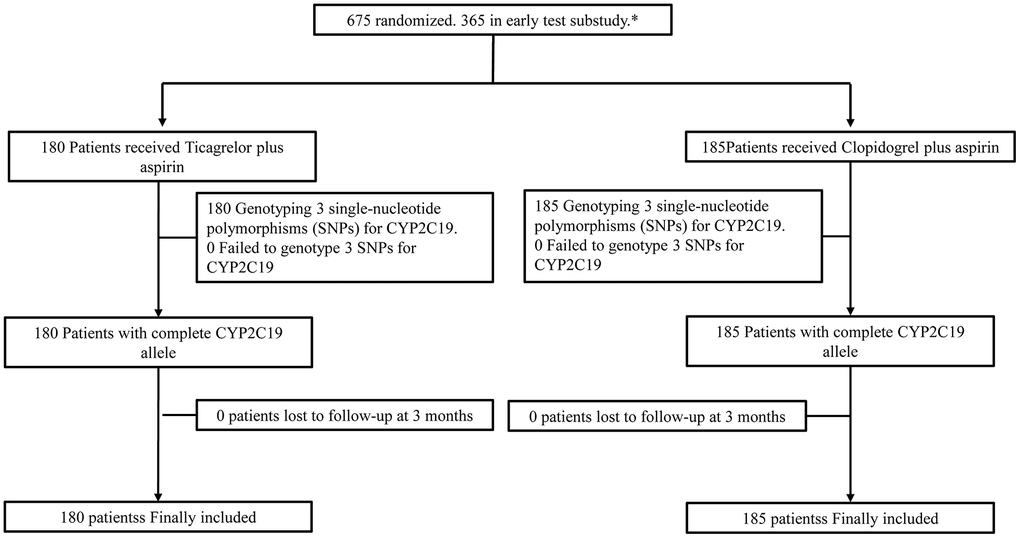
Figure 1. Flow chart.
Table 1. Baseline characteristics of patients included and excluded.
| Characteristic | Included (N=365) | Excluded (N=310) | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years), mean (SD) | 61.7±8.5 | 59.7±8.8 | 0.002 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female sex, n (%) | 105 (28.8%) | 76 (24.5%) | 0.21 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg), mean (SD) | 153.8±21.6 | 153.5±22.2 | 0.91 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg), mean (SD) | 88.0±13.0 | 89.2±12.9 | 0.24 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body-mass index (kg/m2) a, mean (SD) | 24.9±3.8 | 25.1±3.8 | 0.45 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse rate (beats/min), mean (SD) | 76.2±10.7 | 75.0±11.0 | 0.14 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medical history (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 229 (62.7%) | 182 (58.7%) | 0.29 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 29 (8.0%) | 12 (3.9%) | 0.03 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes mellitus | 87 (23.8%) | 77 (24.8%) | 0.76 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ischemic stroke | 68 (18.6%) | 53 (17.1%) | 0.60 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TIA | 11 (3.0%) | 7 (2.3%) | 0.54 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Coronary artery disease | 18 (4.9%) | 33 (10.7%) | 0.005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Known atrial fibrillation | 1 (0.3%) | 3 (1.0%) | 0.51 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Flutter valvular heart disease | 0 (0.0%) | 1 (0.3%) | 0.28 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulmonary embolism | 0 (0.0%) | 0 (0.0%) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-smoker | 179 (49.0%) | 126 (40.7%) | 0.07 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 158 (43.3%) | 161 (51.9%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ex-smoker | 28 (7.7%) | 23 (7.4%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Drug use before randomization (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Proton-pump inhibitor | 3 (0.8%) | 2 (0.7) | 0.79 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 44 (12.1%) | 22 (7.1%) | 0.03 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 90 (24.7%) | 56 (18.1%) | 0.04 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clopidogrel | 10 (2.7%) | 5 (1.6%) | 0.32 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ticagrelor | 0 (0.0%) | 0 (0.0%) | - | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean time to randomization after onset of symptoms (h), mean (SD) | 14.0±6.6 | 14.3±6.8 | 0.49 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Time to randomization after onset of symptoms (%) | 0.43 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <12 hr | 148 (40.6%) | 135 (43.6%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥12 hr | 217 (59.5%) | 175 (56.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Qualifying event (%) | 0.67 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Minor stroke | 307 (84.1%) | 257 (82.9%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TIAb | 58 (15.9%) | 53 (17.1%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline ABCD2 score among patients with TIA as qualifying eventc | 0.33 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median | 5.0 | 5.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interquartile range | 4.0-5.0 | 4.0-5.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SSS-TOAST stroke subtype (%)d | 0.17 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Large-artery atherosclerosis | 156 (50.8%) | 148 (57.6%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardioaortic embolism | 7 (2.3%) | 6 (2.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Small-artery occlusion | 120 (39.1%) | 93 (36.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other causes | 13 (4.2%) | 3 (1.2%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Undetermined causes | 11 (3.6%) | 7 (2.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unkown | 7 (2.3%) | 2 (0.8%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unclassified | 4 (1.3%) | 5 (1.9%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aThe body-mass index is the weight in kilograms divided by the square of the height in meters. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bTIA indicates transient ischemic attack. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cABCD2 stroke risk scores range from 0 to 7, with higher scores meaning higher risk; data provided in the table only for the group of 111 patients whose qualifying event was TIA for inclusion in the trial. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| dSSS-TOAST stroke subtype=Stop Stroke Study Trial of Org 10172 in Acute Stroke Treatment stroke aetiology classification (supplementary appendix, SSS-TOAST classification criteria); data provided in the table are only for the group of 564 patients whose qualifying event was minor stroke for inclusion in the trial | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Baseline characteristics of patients received ticagrelor/aspirin and clopidogrel/aspirin stratified by CYP2C19 metabolizer status.
| Characteristic | Carrier | Non-carrier | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total (n = 199) | Ticagrelor/aspirin (n = 100) | Clopidogrel/aspirin (n =99) | p | Total (n = 166) | Ticagrelor/aspirin (n = 80) | Clopidogrel/aspirin (n = 86) | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years), mean (SD) | 61.3±9.1 | 61.8±8.6 | 60.8±9.5 | 0.44 | 62.3±7.8 | 62.5±7.5 | 62.1±8.1 | 0.72 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female sex, n (%) | 48 (24.1%) | 19 (19%) | 29(29.3%) | 0.09 | 57 (34.3%) | 33 (41.3%) | 24 (27.9%) | 0.07 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg), mean (SD) | 153.2±21.9 | 153.5±21.6 | 153.0±22.3 | 0.86 | 154.3±21.4 | 152.6±24.2 | 155.9±18.4 | 0.33 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg), mean (SD) | 88.3±13.2 | 88.6±12.4 | 88.1±14.1 | 0.79 | 87.7±12.7 | 86.4±12.8 | 88.8±12.5 | 0.22 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body-mass index (kg/m2)a, mean (SD) | 25.1±3.7 | 24.9±2.7 | 25.3±4.5 | 0.40 | 24.7±3.8 | 24.9±4.0 | 24.5±3.7 | 0.45 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse rate (beats/min), mean (SD) | 77.0±10.0 | 75.5±8.5 | 77.9±11.3 | 0.10 | 75.7±11.5 | 76.6±10.3 | 74.9±12.5 | 0.35 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medical history (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 124 | 67(67%) | 57(57.6%) | 0.17 | 105 | 48 (60%) | 57 (66.3%) | 0.40 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 16 | 10(10%) | 6(6.1%) | 0.31 | 13 | 6 (7.5%) | 7 (8.1%) | 0.02 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes mellitus | 47 | 24(24%) | 23(23.2%) | 0.90 | 40 | 18 (22.5%) | 22 (25.6%) | 0.64 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ischemic stroke | 36 | 18(18%) | 18(18.2%) | 0.97 | 32 | 12 (15%) | 20 (23.3%) | 0.18 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TIA | 6 | 1(1%) | 5(5.1%) | 0.09 | 5 | 3 (3.8%) | 2 (2.3%) | 0.59 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Coronary artery disease | 9 | 4(4%) | 5(5.1%) | 0.72 | 9 | 6 (7.5%) | 3 (3.5%) | 0.25 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Known atrial fib rillation | 1 | 0(0%) | 1(1.0%) | - | 0 | 0 | 0 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Flutter valvular heart disease | 0 | 0 | 0 | - | 0 | 0 | 0 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulmonary embolism | 0 | 0 | 0 | - | 0 | 0 | 0 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status (%) | 0.72 | 0.80 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-smoker | 92 | 44(44%) | 48(48.5%) | 87 | 44 (55%) | 43 (50%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 86 | 44(44%) | 42(42.4%) | 72 | 33 (41.3%) | 39 (45.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ex-smoker | 21 | 12(12%) | 9(9.1%) | 7 | 3 (3.8%) | 4 (4.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Drug use before randomization (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Proton-pump inhibitor | 3 | 1(1%) | 2(2.0%) | 0.55 | 0 | 0 | 0 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 25 | 16(16%) | 9(9.1%) | 0.14 | 19 | 8 (10%) | 11 (12.8%) | 0.57 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 50 | 29(29%) | 21(21.2%) | 0.21 | 40 | 22 (27.5%) | 18 (20.9%) | 0.32 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clopidogrel | 6 | 1(1%) | 5(5.1%) | 0.10 | 4 | 2 (2.5%) | 2 (2.3%) | 0.94 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ticagrelor | 0 | 0 | 0 | - | 0 | 0 | 0 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean time to randomization after onset of symptoms (h), mean (SD) | 13.9±6.6 | 14.5±6.6 | 13.3±6.5 | 0.22 | 14.1±6.6 | 13.7±6.6 | 14.4±6.6 | 0.47 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Time to randomization after onset of symptoms (%) | 0.07 | 0.30 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <12 hr | 78 | 33(33%) | 45(45.5%) | 96 | 43 (53.8%) | 53 (61.6%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥12 hr | 121 | 67(67%) | 54(54.5%) | 70 | 37 (46.3%) | 33 (38.4%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Qualifying event (%) | 199 | 0.10 | 166 | 0.87 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Minor stroke | 173 | 83(83%) | 90(90.9%) | 134 | 65 (81.3%) | 69 (80.2%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TIAb | 26 | 17(17%) | 9(9.1%) | 32 | 15 (18.8%) | 17 (19.8%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline ABCD2 score among patients with TIA as qualifying eventc | 0.30 | 0.23 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median | 5.0 | 5.0 | 5.0 | 5.0 | 5.0 | 4.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interquartile range | 4.0-6.0 | 4.0-5.0 | 4.0-7.0 | 4.0-5.0 | 4.0-6.0 | 4.0-5.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SSS-TOAST stroke subtype (%)d | 0.37 | 0.47 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Large-artery atherosclerosis | 90 | 42 (24.3%) | 48 (27.8%) | 66 | 36 (26.9%) | 30 (22.4%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardioaortic embolism | 4 | 3 (1.7%) | 1 (0.6%) | 3 | 2 (1.5%) | 1 (0.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Small-artery occlusion | 62 | 33 (19.1%) | 29 (16.8%) | 58 | 23 (17.2%) | 35 (26.1%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other causes | 10 | 3 (1.7%) | 7 (4.0%) | 3 | 2 (1.5%) | 1 (0.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Undetermined causes | 7 | 2 (1.2%) | 5 (2.9%) | 4 | 2 (1.5%) | 2 (1.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 4 | 0 (0.0%) | 4 (2.3%) | 3 | 1 (0.7%) | 2 (1.5%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unclassified | 3 | 2 (1.2%) | 1 (06%) | 1 | 1 (0.7%) | 0 (0.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aThe body-mass index is the weight in kilograms divided by the square of the height in meters. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bTIA indicates transient ischemic attack. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cABCD2 stroke risk scores range from 0 to 7, with higher scores meaning higher risk; data provided in the table only for the group of 111 patients whose qualifying event was TIA for inclusion in the trial. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| dSSS-TOAST stroke subtype=Stop Stroke Study Trial of Org 10172 in Acute Stroke Treatment stroke aetiology classification (supplementary appendix, SSS-TOAST classification criteria); data provided in the table are only for the group of 564 patients whose qualifying event was minor stroke for inclusion in the trial. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
High on-treatment platelet reactivity
For carriers and non-carriers, proportions of HOPR were significantly lower during ticagrelor/aspirin therapy compared with clopidogrel/aspirin therapy at 2 hours, 24 hours, 7 days, respectively (all p<0.05), which were similar at baseline (Table 3). The proportion of HOPR in the ticagrelor/aspirin group was only significantly lower than that in the clopidogrel/aspirin group in carriers, while no significant difference was found in proportions of HOPR between ticagrelor/aspirin group and clopidogrel/aspirin group in non-carriers at 90 days (HOPR proportion among carriers, 8.0% with ticagrelor/aspirin therapy vs 38.6% with clopidogrel/aspirin therapy; risk ratio (RR), 0.21; 95% confidence intervals (CI), 0.09-0.41; p<0.001; HOPR proportion among non-carriers, 12.3% with ticagrelor/aspirin therapy vs 22.7% with clopidogrel/aspirin therapy; RR, 0.54; 95% CI, 0.25-1.11; p=0.11; p=0.37 for interaction). The Ticagrelor/aspirin therapy was more effective in reducing proportion of HOPR independent of CYP2C19 metabolizer status and seemed to eliminate HOPR at 24 hours in both carriers and non-carriers (Figure 2).
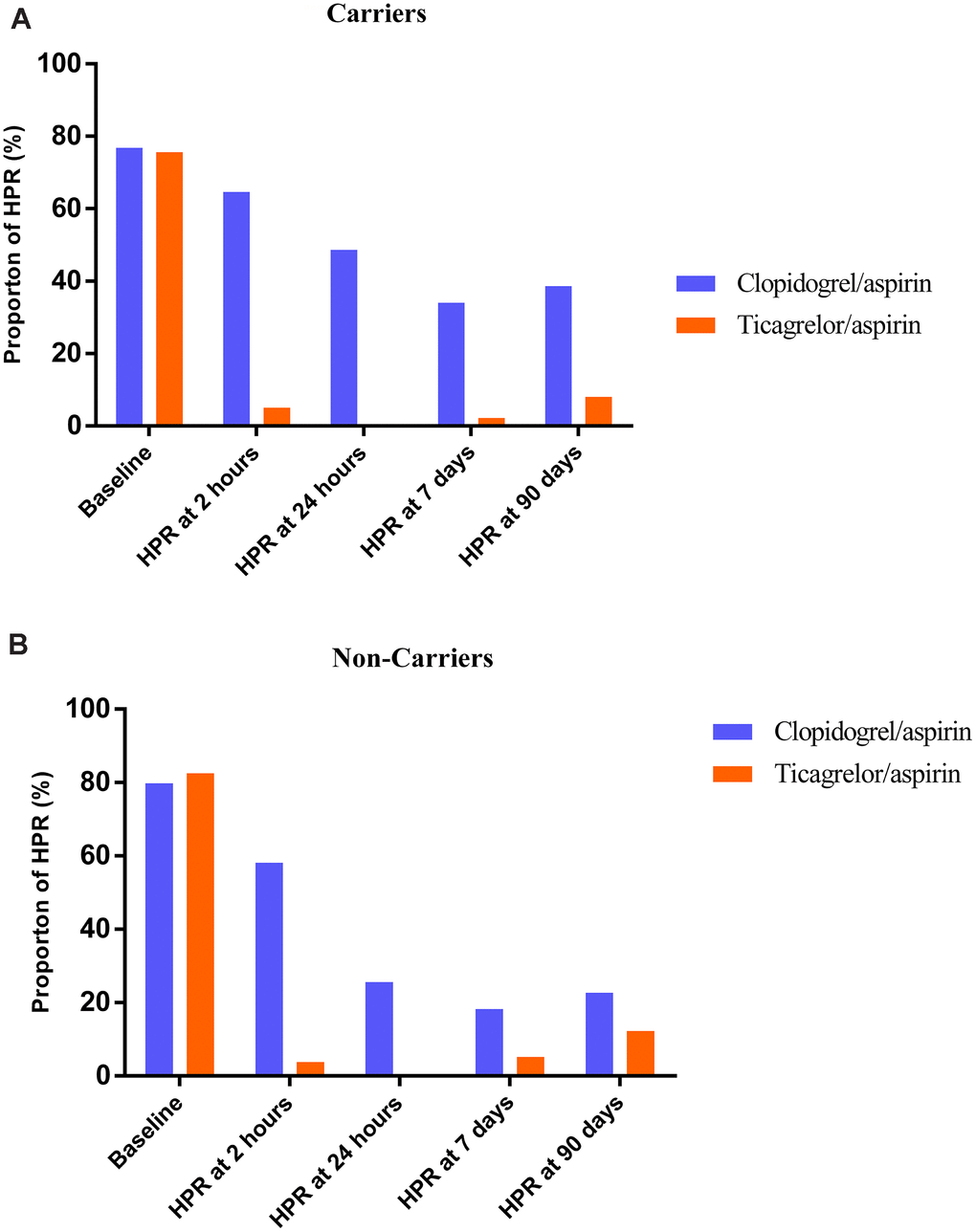
Figure 2. Effect of Ticagrelor/aspirin therapy compared with Clopidogrel/aspirin therapy on high on-treatment platelet reactivity (HOPR) during study time course stratified by metabolizer status. (A) Carriers; (B) Non-carriers.
Table 3. Effect of ticagrelor/aspirin as compared with clopidogrel/aspirin on high on-treatment platelet reactivity (HOPR) during study time course stratified by metabolizer status.
| Carriersa | Non-carriersb | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ticagrelor/aspirin | Clopidogrel/aspirin | Risk ratio (95% CI) | p | Ticagrelor/aspirin | Clopidogrel/aspirin | Risk ratio (95% CI) | p | p value for interaction | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline | 75/99 (75.6%) | 76/99(76.8%) | 0.99(0.84-1.16) | 0.87 | 66/80(82.5%) | 67/84(79.8%) | 1.03(0.89-1.21) | 0.65 | 0.86 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOPRc at 2 hours | 5/100(5.0%) | 64/99(64.6%) | 0.08(0.03-0.16) | <0.001 | 3/80(3.8%) | 50/86(58.1%) | 0.07(0.02-0.17) | <0.001 | 0.86 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOPR at 24 hours | 0/100(0%) | 48/99(48.6%) | - | 1.0 | 0/80(0%) | 22/86(25.6%) | - | 1.0 | 0.26 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOPR at 7 days | 2/93(2.2%) | 33/97(34.0%) | 0.06(0.01-0.20) | <0.001 | 4/77(5.2%) | 15/82(18.3%) | 0.28(0.08-0.74) | 0.02 | 0.37 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOPR at 90 days | 7/88(8.0%) | 32/83(38.6%) | 0.21(0.09-0.41) | <0.001 | 9/73(12.3%) | 17/75(22.7%) | 0.54(0.25-1.11) | 0.11 | 0.37 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aLoss-of-function allele carriers, defined as patients with at least one CYP2C19 loss-of-function allele (ie, *2 or *3): *1/*2, *1/*3, *2/*2, *2/*3, *3/*3, *2/*17, or *3/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bLoss-of-function non-carriers were defined as patients with no CYP2C19 loss-of-function allele: *1/*1, *1/*17, or *17/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cHOPR, high on-treatment platelet reactivity, defined as the P2Y12 reaction unit (PRU) >208 measured using the VerifyNow P2Y12 assay. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Inhibition of platelet aggregation
IPA was higher at all time points except at baseline in patients treated with ticagrelor/aspirin therapy compared with those treated with clopidogrel/aspirin therapy in both carriers and non-carriers of CYP2C19 LOF alleles (all p<0.001 for 2h, 24h, 7d and 90d-IPA, respectively; Table 4). IPA was similar in carriers and non-carriers treated with ticagrelor/aspirin therapy, while was different between carriers and non-carriers treated with clopidogrel/aspirin therapy (Figure 3).
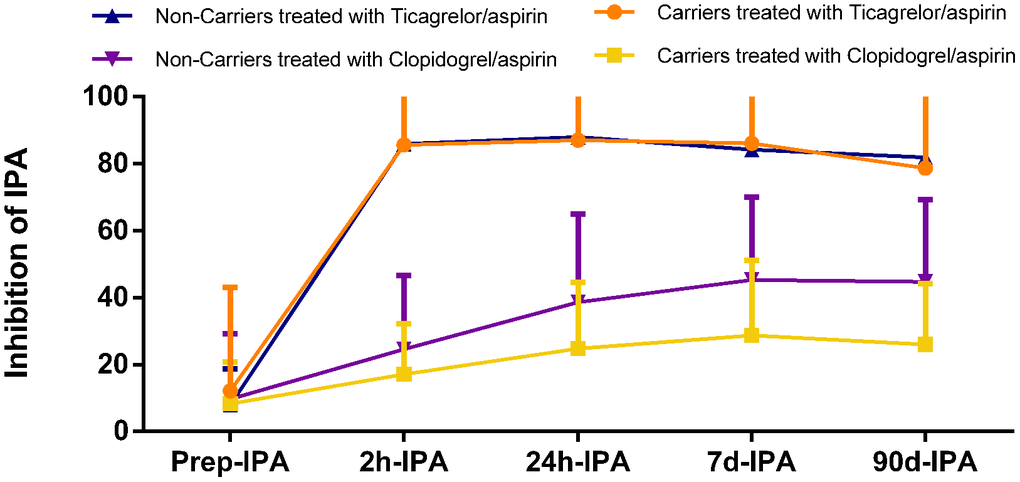
Figure 3. Inhibition of platelet aggregation (IPA) of Ticagrelor/aspirin therapy as compared with Clopidogrel/aspirin therapy during study time course stratified by metabolizer status.
Table 4. Inhibition of platelet aggregation (IPA) of ticagrelor/aspirin as compared with clopidogrel/aspirin treatment during study time course stratified by metabolizer status.
| Carriersa | Non-carriersb | p value for interaction | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ticagrelor/aspirin | Clopidogrel/aspirin | β (95% CI) | p | Ticagrelor/aspirin | Clopidogrel/aspirin | β (95% CI) | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prer-IPA | 12.1 ± 30.9 | 8.3 ± 12.5 | 3.77 (-6.20-13.73) | 0.46 | 7.9 ± 10.9 | 9.7 ± 19.6 | -1.78 (-9.24-5.68) | 0.64 | 0.42 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2h-IPA | 85.6 ± 17.5 | 17.1 ± 15.2 | 68.54 (63.27-73.79) | <0.001 | 85.9 ± 19.2 | 24.6 ± 22.1 | 61.35 (54.51-68.19) | <0.001 | 0.10 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 24h-IPA | 87.0 ± 15.9 | 24.8 ± 19.8 | 62.13 (56.90-67.35) | <0.001 | 88.0 ± 13.0 | 38.6 ± 26.4 | 49.40 (42.95-55.85) | <0.001 | 0.003 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7d-IPA | 86.1 ± 25.2 | 28.7 ± 22.4 | 57.34 (50.34-64.35) | <0.001 | 84.2 ± 19.3 | 45.3 ± 24.8 | 38.84 (31.84-45.83) | <0.001 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 90d-IPA | 78.7 ± 26.1 | 26.0 ±18.2 | 52.65 (45.49-59.81) | <0.001 | 81.9 ± 24.0 | 44.7 ± 24.6 | 37.24 (29.08-45.41) | <0.001 | 0.006 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aLoss-of-function allele carriers, defined as patients with at least one CYP2C19 loss-of-function allele (ie, *2 or *3): *1/*2, *1/*3, *2/*2, *2/*3, *3/*3, *2/*17, or *3/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bLoss-of-function non-carriers were defined as patients with no CYP2C19loss-of-function allele: *1/*1, *1/*17, or *17/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Only several new-onset strokes occurred at 7 days while no myocardial infarction, death or fatal/life-threatening events happened. The incidence of new-onset stroke did not differ between ticagrelor/aspirin therapy and clopidogrel/aspirin therapy either in carriers (rates with 5.0% for ticagrelor/aspirin therapy vs 5.1% for clopidogrel/aspirin therapy; hazard ratios (HR), 0.94; 95% CI 0.71-1.25; p=0.64; Table 5) or non-carriers (rates with 1.3% for ticagrelor/aspirin therapy vs 5.8% for clopidogrel/aspirin therapy; HR, 1.01; 95% CI, 0.74-1.38; p=0.94; p=0.83 for interaction; Table 5). Only one other bleeding event occurred in carriers treated with clopidogrel/aspirin therapy. No patient developed myocardial infarction, death or life-threatening events at 7days.
Table 5. Major clinical events and safety of ticagrelor/aspirin as compared with clopidogrel/aspirin at 7 days stratified by metabolizer status.
| Carriersa | Non-carriersb | p valune for interaction | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ticagrelor/aspirin | Clopidogrel/aspirin | Hazard ratio (95% CI) | p | Ticagrelor/aspirin | Clopidogrel/aspirin | Hazard ratio (95% CI) | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| New-onset strokec | 5/100(5.0%) | 5/99 (5.1%) | 0.94(0.71-1.25) | 0.64 | 1/80(1.3%) | 5/86 (5.8%) | 1.01(0.74-1.38) | 0.94 | 0.83 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Myocardial infarction | 0/100 | 0/99 | - | - | 0/80 | 0/86 | - | - | 1.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Death | 0/100 | 0/99 | - | - | 0/80 | 0/86 | - | - | 1.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| fatal/life-threatening events | 0/100 | 0/99 | - | - | 0/80 | 0/86 | - | - | 1.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other events | 0/100 | 1/99 (1.0%) | - | 0.31 | 0/80 | 0/86 | - | - | 0.96 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aLoss-of-function allele carriers, defined as patients with at least one CYP2C19 loss-of-function allele (ie, *2 or *3): *1/*2, *1/*3, *2/*2, *2/*3, *3/*3, *2/*17, or *3/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| bLoss-of-function non-carriers were defined as patients with no CYP2C19 loss-of-function allele: *1/*1, *1/*17, or *17/*17. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cNew-onset stroke, including ischemic and hemorrhagic stroke occurs on 7 days. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
In the present study, ticagrelor/aspirin therapy tended to have stronger platelet inhibition and more rapid onset in platelet inhibition compared with clopidogrel/aspirin therapy irrespective of CYP2C19 metabolizer status in patients with ischemic stroke and TIA. In addition, ticagrelor/aspirin therapy in our study showed a near elimination of HOPR at 24 hours in both CYP2C19 LOF carriers and non-carriers.
Clopidogrel as the main prescription for minor acute stroke has some limitations, such as irreversible platelet inhibition, relatively slow onset of action, and variable effect on platelet function and prognosis of stroke influenced by genetic factors, comorbidities and adjunctive pharmacotherapy. [10–12] Moreover, previous studies showed that even high-dose clopidogrel administration was not able to overcome the variability of antiplatelet effects caused by CYP2C19 LOF alleles. [13, 14] The randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease study firstly characterized the onset and offset of the antiplatelet effect of ticagrelor compared with clopidogrel. [15] The study showed that ticagrelor achieved a significant antiplatelet effect within 30 minutes and a greater antiplatelet effect during maintenance therapy compared with clopidogrel. Gurbel et al. investigated the antiplatelet effect of ticagrelor in clopidogrel non-responders, who received 300mg clopidogrel per day for 2 to 4 weeks before study and the absolute change in platelet aggregation was ≤10%, and found that ticagrelor had stronger platelet inhibition and was not influenced by clopidogrel response status. [16] In addition, the study indicated an additional platelet inhibition (≈20% increase in IPA) during switching from clopidogrel to ticagrelor in clopidogrel responders. Our study was consistent with previous study that ticagrelor/aspirin therapy achieved greater inhibition of platelet function and more rapid onset compared with clopidogrel/aspirin therapy in the present study.
Previous study identified patients with IPA <40% as resistant. [17] In the present study, IPAs of both carriers and non-carriers treated with ticagrelor/aspirin were much higher than 40% 2 hours after administration. While IPAs of carriers with clopidogrel/aspirin therapy were consistently lower than 40%, and non-carriers with clopidogrel/aspirin therapy had IPA increasing to nearly 40% after 24 hours, and reaching more than 40% in the 7 days after administration. Luo and his colleagues reported that the combination of an elevated PRU and a decreased IPA was associated with significantly higher incidence of major adverse cardiac events than one or neither. [18] However, the present study was not powerful enough to show whether proportion of HOPR and IPA were associated with clinical outcomes of acute minor stroke and TIA patients.
Previous study showed that CYP2C19 LOF alleles were associated with increased risk of cardiac-cerebral vascular events and poorer clinical outcomes, [3, 19, 20] especially in Asians. [21] Kazi et al. suggested that genotype-guided personalized therapy may improve the cost-effectiveness of the newer antiplatelet agents, additionally, ticagrelor was considered to be the most cost-effective for carriers and non-carriers of CYP2C19 LOF alleles in acute coronary disease. [22] Although the SOCRATES study did not achieve a significant result, it indicated that combination of ticagrelor and aspirin might be effective in Asian patients. [23, 24] As reported, there was a high risk of another stroke after minor stroke and TIA in the first two weeks, with particularly high events rates in the first two days. [1, 25] In our study, the ticagrelor/aspirin therapy could quickly take effect on IPA within 2 hours and almost diminished the HOPR at 24 hours both in carriers and non-carriers of CYP2C19 LOF alleles, while clopidogrel/aspirin therapy seemed to reach maximal effect until 7 days. Our results indicated that ticagrelor/aspirin therapy might be a more appropriate strategy for acute minor stroke and TIA patients carrying CYP2C19 LOF allele. Considering the high cost of platelet function test and expensive charge of ticagrelor, perhaps, the genotype-guided personalized combination therapy of ticagrelor and aspirin may be more cost effective. Further study on the efficacy of more intensive platelet inhibition on prognosis of acute minor stroke and TIA is needed.
Our study has several limitations. First, the number of included patients is small. The calculated number of included patients of the PRINCE study was 952 patients to achieve the primary outcome. The interim analysis based on 476 patients (50% of the projected necessary sample size) with intact data conducted by data safety monitoring board, achieved a prespecified threshold for efficacy, so the study was terminated in advance. Our study is a sub-analysis and we reviewed the previous articles on antiplatelet effects of ticagrelor and clopidogrel, the number of included patients was always between 100-200. Thus, the sample size of our study could be effective. Second, CYP2C19 gene could also be found in other disease, which will affect platelet aggregation through other factors not only clopidogrel. It may affect the conclusion of this manuscript. Third, the present study showed that the inhibition of platelet function was maximized at 24 hours of ticagrelor/aspirin therapy (Figure 3), while previous studies showed the maximal antiplatelet effect occurred at 1-2 hours, [16, 26] which may due to the inconsecutive testing.
In conclusion, ticagrelor/aspirin therapy was associated with greater platelet inhibition and more rapid onset in platelet inhibition compared with clopidogrel/aspirin therapy both in carriers and non-carriers of CYP2C19 LOF alleles with acute minor stroke or TIA.
Materials and Methods
Study participants and protocol
We derived data from the PRINCE trial. Details on design and major results of the PRINCE trial have been published elsewhere. [27] Briefly, it was a prospective, multicenter, randomized, open-label, active-controlled and blinded-endpoint trial conducted in China compared ticagrelor (loading dose of 180 mg followed by 90 mg twice daily till day 90) combined with aspirin (loading dose of 100-300mg followed by 100 mg once daily till day 21) and clopidogrel (loading dose of 300mg followed by 75 mg daily till day 90) combined with aspirin (loading dose of 100-300mg followed by 100 mg once daily till day 21) among 675 patients with acute minor stroke defined as National Institutes of Health Stroke Scale score of ≤3 or those with a moderate to high risk TIA defined as ABCD2 stroke risk score of ≥4 or ≥50% stenosis of cervical or intracranial vessel that was responsible for the presentation within 24 hours of symptom onset. Participants were from 26 hospitals in China between August 2015 and March 2017 to estimate whether ticagrelor/aspirin therapy was safe and superior to clopidogrel/aspirin therapy in inhibiting the 90-day platelet reactivity. The protocol and data collection were approved by ethics committee of Beijing Tiantan Hospital and all participated study centers. All patients or their representatives provided written consent before enrollment.
Considering that CYP2C19 gene can affect many other P450 metabolized drugs, if the patient is taking a drug affected by the CYP2C19 genotype in prior to enrollment, we will recommend stopping the drug or switching to an alternative drug. Detailed information of drug combination was collected. And such patients will be labeled and treated accordingly. All medicine including Chinese herbal medicine that may affect function of platelet is prohibited during the trial. Other medicine such as lipid-lowering medicine, antidiabetic, antihypertensive drugs, can be normally used.
The early test sub-study was pre-specified. Patients included in the sub-study additionally received VerifyNow P2Y12 assay testing 2 hours and 24 hours after taking the first agents (Figure 1).
The primary outcomes of our study were the proportions of patients with HOPR and IPA at baseline, 2 hours, 24 hours, 7 days and 90 days, respectively. The HOPR was defined as PRU>208. Percentage of IPA was calculated using standard formulas, where PA was platelet aggregation, b was pre-dosing, and t was post-dosing: IPA (%) = 100% × (PAb – PAt)/PAb.
The primary safety outcome was major clinical events including new-onset ischemic or hemorrhagic stroke, myocardial infarction, death, and major bleeding according to the Platelet Inhibition and Patient Outcomes (PLATO) study including fatal/life-threatening bleed, major bleed and others, at 7 days.
The PRU and IPA are tested by the VerifyNow P2Y12 assay, a turbidimetric-based optical detection system, according to the manufacturer’s instructions. The VerifyNow P2Y12 assay was well studied and used widely in testing P2Y12 receptor activity. The device measured platelet-induced aggregation as an increase in light transmittance and used a proprietary algorithm to report values of PRU. [28]
Genotyping
Three single-nucleotide polymorphisms for CYP2C19 (National Center for Biotechnology Information [NCBI] Genome build 37.1, GenBank NG_008384), including CYP2C19*2 (681G>A, rs4244285), CYP2C19*3 (636G>A, rs4986893), and CYP2C19*17 (-806C>T, rs12248560), were genotyped in all participants recruited. Details of genotyping were published. [9]
We used common consensus star allele nomenclature to categorize patients by CYP2C19 metabolizer status based on *2, *3, and *17 genotypes. [29] Gain-of-function allele carriers were defined as who had at least one gain-of-function allele (*17) and LOF allele carriers were defined as who had at least one LOF allele (*2 or *3). [3] Patients with at least two *2 or *3 alleles (*2/*2, *2/*3, or *3/*3) were classified as "poor metabolizers", those with one *2 or *3 allele (*1/*2 or *1/*3) were classified as "intermediate metabolizers", those with at least one *17 allele (*1/*17 or *17/*17) were classified as "ultra-metabolizers", those without any *2, *3, or *17 allele (*1/*1) were classified as "extensive metabolizers", and those with one *17 and a LOF allele (*2/*17 or *3/*17) were classified as "unknown metabolizers" [30] due to the uncertain clinical consequences. [31]
Statistical analysis
All statistical analysis was performed using the SAS 9.4 (SAS Institute Inc, Cary, NC). All reported p values were two-sided with p<0.05 considered significant. The baseline characteristics were compared between patients included and excluded, and between two treatment groups in carriers and non-carriers of CYP2C19 LOF alleles. Categorical variables were presented in proportions, and continuous variables were presented in means ±SD or medians with interquartile ranges. Nonparametric Kruskal-Wallis test was used to compare group differences for nominal variables, and χ2 tests or Fisher’s exact test for dichotomous variables. The proportions of HOPR and IPAs at 2 hours, 24 hours, 7 days and 90 days were respectively compared between the two therapy groups using genmod models adjusted by the high platelet reactivity status at baseline, RR with 95% CI was presented for HOPR, and β with 95% CI was presented for IPA. Differences in the rates of new-onset stroke, myocardial infarction, death, and bleeding events during 7-day follow-up were assessed using Cox proportional hazards regression and HR with 95% CI. Whether the treatment effect differed in certain genotype categories was assessed by testing the treatment-by-genotype interaction effect using genmod models for the primary outcome and Cox models for the primary safety outcome.
Author Contributions
Mengyuan Zhou and Weiqi Chen collected data and wrote manuscript; Yuesong Pan performed the data analysis and joined in clinical data discussion; Yi Lin, Xia Meng, Xingquan Zhao, Liping Liu, Jinxi Lin, Hao Li, and Yongjun Wang participated in study design and critical discussion; Yilong Wang responsible for study design, critical discussion and manuscript revision.
Acknowledgments
Thanks to all the participating hospitals in the study and thank all enrolled patients and their families.
Conflicts of Interest
Authors have no potential conflicts of interest.
Funding
The study was supported by grants from the National Natural Science Foundation of China (81901177, 81825007, and 81971091); Beijing Outstanding Young Scientist Program (No. BJJWZYJH01201910025030); The “Thirteenth-Five” Key Development and Research Plan by the Ministry of Science and Technology of the People’s Republic of China (No. 2017YFC1307900); Beijing Hospitals Authority Youth Programme (QML20190501); Beijing Science and Technology Plan by Beijing Municipal Science and Technology Commission (No. D171100003017001); Beijing Tiantan Hospital, Capital Medical University (2018-YQN-1, 2020MP01); Beijing Excellent Talents Training and Supporting- Top Youth Team by Beijing Municipal Science and Technology Commission (No. 2016000021223TD03); Youth Beijing Scholar Program; Beijing Talent Project - Class A: Innovation and Development (No. 2018A12) and Young Elite Scientist Sponsorship Program (2020QNRC001).
References
- 1. Amarenco P, Lavallée PC, Labreuche J, Albers GW, Bornstein NM, Canhão P, Caplan LR, Donnan GA, Ferro JM, Hennerici MG, Molina C, Rothwell PM, Sissani L, et al, and TIAregistry.org Investigators. One-year risk of stroke after transient ischemic attack or minor stroke. N Engl J Med. 2016; 374:1533–42. https://doi.org/10.1056/NEJMoa1412981 [PubMed]
- 2. Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, Wang C, Li H, Meng X, Cui L, Jia J, Dong Q, Xu A, et al, and CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. 2013; 369:11–19. https://doi.org/10.1056/NEJMoa1215340 [PubMed]
- 3. Wang Y, Zhao X, Lin J, Li H, Johnston SC, Lin Y, Pan Y, Liu L, Wang D, Wang C, Meng X, Xu J, Wang Y, and CHANCE investigators. Association between CYP2C19 loss-of-function allele status and efficacy of clopidogrel for risk reduction among patients with minor stroke or transient ischemic attack. JAMA. 2016; 316:70–78. https://doi.org/10.1001/jama.2016.8662 [PubMed]
- 4. Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brandt JT, Walker JR, Antman EM, Macias W, Braunwald E, Sabatine MS. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009; 360:354–62. https://doi.org/10.1056/NEJMoa0809171 [PubMed]
- 5. Wallentin L, James S, Storey RF, Armstrong M, Barratt BJ, Horrow J, Husted S, Katus H, Steg PG, Shah SH, Becker RC, and PLATO investigators. Effect of CYP2C19 and ABCB1 single nucleotide polymorphisms on outcomes of treatment with ticagrelor versus clopidogrel for acute coronary syndromes: a genetic substudy of the PLATO trial. Lancet. 2010; 376:1320–28. https://doi.org/10.1016/S0140-6736(10)61274-3 [PubMed]
- 6. Storey RF, Angiolillo DJ, Patil SB, Desai B, Ecob R, Husted S, Emanuelsson H, Cannon CP, Becker RC, Wallentin L. Inhibitory effects of ticagrelor compared with clopidogrel on platelet function in patients with acute coronary syndromes: the PLATO (PLATelet inhibition and patient outcomes) PLATELET substudy. J Am Coll Cardiol. 2010; 56:1456–62. https://doi.org/10.1016/j.jacc.2010.03.100 [PubMed]
- 7. Johnston SC, Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, Held P, Jonasson J, Minematsu K, Molina CA, Wang Y, Wong KS, and SOCRATES Steering Committee and Investigators. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. N Engl J Med. 2016; 375:35–43. https://doi.org/10.1056/NEJMoa1603060 [PubMed]
- 8. Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, Held P, Hill MD, Jonasson J, Kasner SE, Ladenvall P, Minematsu K, Molina CA, Wang Y, et al, and SOCRATES Steering Committee and Investigators. Efficacy and safety of ticagrelor versus aspirin in acute stroke or transient ischaemic attack of atherosclerotic origin: a subgroup analysis of SOCRATES, a randomised, double-blind, controlled trial. Lancet Neurol. 2017; 16:301–10. https://doi.org/10.1016/S1474-4422(17)30038-8 [PubMed]
- 9. Wang Y, Chen W, Lin Y, Meng X, Chen G, Wang Z, Wu J, Wang D, Li J, Cao Y, Xu Y, Zhang G, Li X, et al, and PRINCE Protocol Steering Group. Ticagrelor plus aspirin versus clopidogrel plus aspirin for platelet reactivity in patients with minor stroke or transient ischaemic attack: open label, blinded endpoint, randomised controlled phase II trial. BMJ. 2019; 365:l2211. https://doi.org/10.1136/bmj.l2211 [PubMed]
- 10. Gurbel PA, Antonino MJ, Tantry US. Recent developments in clopidogrel pharmacology and their relation to clinical outcomes. Expert Opin Drug Metab Toxicol. 2009; 5:989–1004. https://doi.org/10.1517/17425250903107772 [PubMed]
- 11. Jia DM, Chen ZB, Zhang MJ, Yang WJ, Jin JL, Xia YQ, Zhang CL, Shao Y, Chen C, Xu Y. CYP2C19 polymorphisms and antiplatelet effects of clopidogrel in acute ischemic stroke in China. Stroke. 2013; 44:1717–19. https://doi.org/10.1161/STROKEAHA.113.000823 [PubMed]
- 12. Zhang Y, Zhang S, Ding Z. Role of P2Y12 receptor in thrombosis. Adv Exp Med Biol. 2017; 906:307–24. https://doi.org/10.1007/5584_2016_123 [PubMed]
- 13. Mega JL, Hochholzer W, Frelinger AL
3rd , Kluk MJ, Angiolillo DJ, Kereiakes DJ, Isserman S, Rogers WJ, Ruff CT, Contant C, Pencina MJ, Scirica BM, Longtine JA, et al. Dosing clopidogrel based on CYP2C19 genotype and the effect on platelet reactivity in patients with stable cardiovascular disease. JAMA. 2011; 306:2221–28. https://doi.org/10.1001/jama.2011.1703 [PubMed] - 14. Zhang L, Yang J, Zhu X, Wang X, Peng L, Li X, Cheng P, Yin T. Effect of high-dose clopidogrel according to CYP2C19*2 genotype in patients undergoing percutaneous coronary intervention- a systematic review and meta-analysis. Thromb Res. 2015; 135:449–58. https://doi.org/10.1016/j.thromres.2014.12.007 [PubMed]
- 15. Gurbel PA, Bliden KP, Butler K, Tantry US, Gesheff T, Wei C, Teng R, Antonino MJ, Patil SB, Karunakaran A, Kereiakes DJ, Parris C, Purdy D, et al. Randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease: the ONSET/OFFSET study. Circulation. 2009; 120:2577–85. https://doi.org/10.1161/CIRCULATIONAHA.109.912550 [PubMed]
- 16. Gurbel PA, Bliden KP, Butler K, Antonino MJ, Wei C, Teng R, Rasmussen L, Storey RF, Nielsen T, Eikelboom JW, Sabe-Affaki G, Husted S, Kereiakes DJ, et al. Response to ticagrelor in clopidogrel nonresponders and responders and effect of switching therapies: the RESPOND study. Circulation. 2010; 121:1188–99. https://doi.org/10.1161/CIRCULATIONAHA.109.919456 [PubMed]
- 17. Ari H, Ozkan H, Karacinar A, Ari S, Koca V, Bozat T. The EFFect of hIgh-dose ClopIdogrel treatmENT in patients with clopidogrel resistance (the EFFICIENT trial). Int J Cardiol. 2012; 157:374–80. https://doi.org/10.1016/j.ijcard.2010.12.083 [PubMed]
- 18. Luo Y, Li J, Liu X, Xu J, Ye Z, Yao Y, Liu X, Lai Y. Combination of P2Y12 reaction unit and percentage of platelet inhibition assessed by VerifyNow P2Y12 assay is a useful predictor of long-term clinical outcomes in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Thromb Res. 2016; 139:114–20. https://doi.org/10.1016/j.thromres.2016.01.020 [PubMed]
- 19. Shuldiner AR, O’Connell JR, Bliden KP, Gandhi A, Ryan K, Horenstein RB, Damcott CM, Pakyz R, Tantry US, Gibson Q, Pollin TI, Post W, Parsa A, et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA. 2009; 302:849–57. https://doi.org/10.1001/jama.2009.1232 [PubMed]
- 20. Mega JL, Simon T, Collet JP, Anderson JL, Antman EM, Bliden K, Cannon CP, Danchin N, Giusti B, Gurbel P, Horne BD, Hulot JS, Kastrati A, et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: a meta-analysis. JAMA. 2010; 304:1821–30. https://doi.org/10.1001/jama.2010.1543 [PubMed]
- 21. Sorich MJ, Rowland A, McKinnon RA, Wiese MD. CYP2C19 genotype has a greater effect on adverse cardiovascular outcomes following percutaneous coronary intervention and in Asian populations treated with clopidogrel: a meta-analysis. Circ Cardiovasc Genet. 2014; 7:895–902. https://doi.org/10.1161/CIRCGENETICS.114.000669 [PubMed]
- 22. Kazi DS, Garber AM, Shah RU, Dudley RA, Mell MW, Rhee C, Moshkevich S, Boothroyd DB, Owens DK, Hlatky MA. Cost-effectiveness of genotype-guided and dual antiplatelet therapies in acute coronary syndrome. Ann Intern Med. 2014; 160:221–32. https://doi.org/10.7326/M13-1999 [PubMed]
- 23. Wang Y, Minematsu K, Wong KS, Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, Held P, Jonasson J, Molina CA, Johnston SC, and SOCRATES Steering Committee and Investigators. Ticagrelor in Acute Stroke or Transient Ischemic Attack in Asian Patients: From the SOCRATES Trial (Acute Stroke or Transient Ischemic Attack Treated With Aspirin or Ticagrelor and Patient Outcomes). Stroke. 2017; 48:167–73. https://doi.org/10.1161/STROKEAHA.116.014891 [PubMed]
- 24. Moris D, Bakoyiannis C, Avgerinos E. Letter by moris et al regarding article, “Ticagrelor in acute stroke or transient ischemic attack in Asian patients: from the SOCRATES trial (acute stroke or transient ischemic attack treated with aspirin or ticagrelor and patient outcomes)”. Stroke. 2017; 48:e110. https://doi.org/10.1161/STROKEAHA.116.016502 [PubMed]
- 25. Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000; 284:2901–06. https://doi.org/10.1001/jama.284.22.2901 [PubMed]
- 26. Husted S, Emanuelsson H, Heptinstall S, Sandset PM, Wickens M, Peters G. Pharmacodynamics, pharmacokinetics, and safety of the oral reversible P2Y12 antagonist AZD6140 with aspirin in patients with atherosclerosis: a double-blind comparison to clopidogrel with aspirin. Eur Heart J. 2006; 27:1038–47. https://doi.org/10.1093/eurheartj/ehi754 [PubMed]
- 27. Wang Y, Lin Y, Meng X, Chen W, Chen G, Wang Z, Wu J, Wang D, Li J, Cao Y, Xu Y, Zhang G, Li X, et al, and PRINCE Protocol Steering Group. Effect of ticagrelor with clopidogrel on high on-treatment platelet reactivity in acute stroke or transient ischemic attack (PRINCE) trial: rationale and design. Int J Stroke. 2017; 12:321–25. https://doi.org/10.1177/1747493017694390 [PubMed]
- 28. Corliss BM, Polifka AJ, Harris NS, Hoh BL, Fox WC. Laboratory assessments of therapeutic platelet inhibition in endovascular neurosurgery: comparing results of the VerifyNow P2Y12 assay to thromboelastography with platelet mapping. J Neurosurg. 2018; 129:1160–65. https://doi.org/10.3171/2017.6.JNS17535 [PubMed]
- 29. Scott SA, Sangkuhl K, Stein CM, Hulot JS, Mega JL, Roden DM, Klein TE, Sabatine MS, Johnson JA, Shuldiner AR, and Clinical Pharmacogenetics Implementation Consortium. Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin Pharmacol Ther. 2013; 94:317–23. https://doi.org/10.1038/clpt.2013.105 [PubMed]
- 30. Paré G, Mehta SR, Yusuf S, Anand SS, Connolly SJ, Hirsh J, Simonsen K, Bhatt DL, Fox KA, Eikelboom JW. Effects of CYP2C19 genotype on outcomes of clopidogrel treatment. N Engl J Med. 2010; 363:1704–14. https://doi.org/10.1056/NEJMoa1008410 [PubMed]
- 31. Scott SA, Sangkuhl K, Gardner EE, Stein CM, Hulot JS, Johnson JA, Roden DM, Klein TE, Shuldiner AR, and Clinical Pharmacogenetics Implementation Consortium. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and clopidogrel therapy. Clin Pharmacol Ther. 2011; 90:328–32. https://doi.org/10.1038/clpt.2011.132 [PubMed]