



Introduction
Esophageal carcinoma (EC) is one of the leading causes of cancer-related mortality worldwide [1]. Unlike esophageal adenocarcinoma, which is prevalent in western countries, the prevalence of esophageal squamous cell carcinoma (ESCC) is higher in China [2]. Definitive concurrent chemoradiotherapy (dCRT) is the standard alternative curative management for patients with locally advanced disease who are not eligible for surgery [3]. Despite an effective treatment response obtained from dCRT, approximately 33% of these patients may have the residual disease and develop recurrent disease within a year after complete remission [4, 5]. There is a lack of consensus on the standard therapeutic strategy for those with post-dCRT residual lesions. Indeed, local treatment with systemic chemotherapy remains the second-line therapy once progression is confirmed in most residual or recurrent cases [6]. However, increased incidence of toxicities associated with intravenous chemotherapy and inconvenience to patients has led to unsatisfactory treatment compliance and interruption of therapy. Compared to the intravenous route, an oral chemotherapeutic regimen may present lower toxicity and therefore, could be a feasible approach for maintenance therapy in patients with post-dCRT residual lesions.
An oral combination of tegafur, gimeracil, and oteracil potassium, named S-1, has been widely used in treating multiple types of cancers, especially in Japan. Upon internalization into cells, S-1 is converted into fluorouracil and shares similar anticancer properties as intravenous 5-Fu [7, 8]. Capecitabine is a fluoropyrimidine that enzymatically converts to 5-Fu by thymidine phosphorylase in tumor tissues, when the drug is administered orally, and has been approved to replace 5-Fu for the treatment of advanced esophagogastric cancer [9]. Since 5-Fu is one of the standard chemotherapeutics for ESCC, S-1 or capecitabine may potentially substitute 5-Fu in ESCC patients who cannot tolerate or refuse intravenous chemotherapy. In fact, patients with unresectable and recurrent ESCC achieved a promising response and showed minimum safety concerns with S-1/capecitabine monotherapy after failing first-line standard treatment [10]. These findings were confirmed in prospective studies that demonstrated the feasibility of S-1/ capecitabine combined with definitive radiation for treating ESCC [11].
Angiogenesis is one of the pivotal cancer hallmarks that promotes cancer growth and metastasis, including esophageal carcinoma, and is a target of biologicals such as bevacizumab, which blocks the vascular endothelial growth factor, VEGF, and drugs such as the multi-receptor tyrosine kinase inhibitors (TKIs) that target the VEGF receptor, VEGFR. Apatinib, one of several oral TKIs that has demonstrated high selectivity for VEGFR-2, and was given approval by the Chinese FDA in 2014 as one of the later-line treatments for gastric cancer [12]. Though the efficacy and safety of apatinib were demonstrated in a retrospective study of advanced ESCC patients who failed prior treatment [13], mono anti-angiogenic approaches have not been very successful in tumor control. Nevertheless, studies have now shown that a combination of anti-angiogenic drugs and chemotherapy may be beneficial [14]. For instance, Zhao et al. reported that a combination of apatinib and S-1 was effective and safe as a second-line treatment for advanced ESCC patients [15]. Based on these findings, we performed this retrospective analysis to evaluate the safety and efficacy of a combination therapy consisting of apatinib, and S-1/capecitabine as the oral maintenance therapy for ESCC patients with post-dCRT residual lesions.
Results
Baseline clinical characteristics
Between December 2016 and December 2019, a total of 39 eligible ESCC patients were enrolled in this study. Patient demographics and tumor characteristics are listed in Table 1. The median age of patients was 61 years (range, 44 - 75), and 34 (87.2%) were male and five (12.8%) female. Patients were diagnosed with ESCC stage II (6; 15.4%) and stage III (33; 84.6%) and completed at least one concurrent chemotherapy cycle with single-agent (18%), taxol and platinum (TP) (20.5%), or platinum and fluorouracil (PF) (61.5%). The median radiation (RT) dose was 60 Gy (range, 50.4 – 64) and 20 (51.3%) patients received RT at ≥ 60Gy. After the completion of dCRT, 14 (35.9%) patients had stable disease (SD) and the remaining 25 (64.1%) achieved partial remission (PR). Seven patients were confirmed with fistula after dCRT. Primary esophageal residual disease was reported in 12 (30.7%) patients, 13 (33.3%) only had regional lymph nodes residual disease, and 14 (35.9%) had the residual disease at both sites. Ten of 39 patients were confirmed with the residual disease by biopsy pathology.
Table 1. Clinical characteristics.
| Characteristics | Patients No. (%) |
| Age (years) | |
| Median(Range) | 61(44-75) |
| >60 | 20(51.3) |
| ≤ 60 | 19(48.7) |
| Gender | |
| Male | 34(87.2) |
| Female | 5(12.8) |
| Tumor location | |
| Cervical | 6(15.4) |
| Upper | 9(23.1) |
| Middle | 13(33.3) |
| Lower | 9(23.1) |
| Multiple | 2(5.1) |
| Length (cm) | |
| <5 | 16(41.0) |
| ≥ 5 | 23(59.0) |
| TNM stage | |
| II | 6(15.4) |
| III | 33(84.6) |
| Concurrent Chemotherapy | |
| Single-agent | 7(18) |
| TP | 8(20.5) |
| PF | 24(61.5) |
| Radiation Dose (Gy) | |
| Median(Range) | 60(50.4-64) |
| <60 | 19(48.7) |
| ≥60 | 20(51.3) |
| Response after dCRT | |
| PR | 25(64.1) |
| SD | 14(35.9) |
| Combined with fistula | |
| Yes | 7(17.9) |
| No | 32(82.1) |
| Residual disease sites | |
| Primary lesion only | 12(30.7) |
| Regional lymph nodes only | 13(33.3) |
| Primary lesion combined with Regional lymph nodes | 14(35.9) |
| Pathological residual disease | |
| Yes | 10(25.6) |
| No | 29(74.4) |
Response to treatment
The treatment regimens and patient response are listed in Table 2. Nineteen (48.7%) patients received sequential therapy regiments, which include S1/capecitabine given alone at first 1-2 cycles followed by dual therapy consisting of S1/capecitabine and apatinib for the remaining treatment cycles until disease progression or intolerable toxicities. S1/capecitabine combined with apatinib on treatment initiation was administered to 20 (51.3%) patients. S-1 was replaced with capecitabine once during the treatment course in seven (17.9%) patients. The median number of the treatment cycle is 12 (2- 31). Among those 39 patients, five patients refused the continuation of the regimen due to the intolerance of toxicities before the confirmed progression of the tumor. At the last follow-up, 15 patients are still in continuation of this maintenance treatment. None of the patients achieved complete remission (CR), while five (12.8%) achieved PR. The overall response rate (ORR) was 12.8% (5/39). Twenty-nine (29/39, 74.4%) patients achieved SD, and five (5/39, 12.8%) had progressive disease (PD), yielding a disease control rate (DCR) of 87.2%.
Table 2. Treatment and response.
| Maintenance therapy | N(%) |
| S1/capecitabine alone followed by S1/capecitabine combined with Apatinib | 19(48.7) |
| S1/capecitabine concurrent with Apatinib | 20(51.3) |
| No. of cycles | |
| Median(Range) | 12(2-31) |
| Treatment response | |
| PR | 5(12.8) |
| SD | 29(74.4) |
| PD | 5(12.8) |
Toxicity
Table 3 shows the toxicity associated with treatment in the cohort. Most were grade 1 to 2 in severity and overlapped with apatinib’s toxicity spectrum. Of the 13 patients who developed secondary hypertension, 10 (25.6%) presented with grade 1 and 2, and three (7.7%) with grade 3. The second common adverse event was proteinuria, with one (2.6%) patient showing grade 4 toxicity, which disappeared rapidly after discontinuing apatinib. One (2.6%) patient presented with the hand-foot syndrome of grade 3 severity. Thus, a total of five (12.8%) patients presented with grade 3 to 4 non-hematological toxicity, and none with hematological toxicity. Other adverse events including fatigue, liver enzyme elevation, bleeding, hoarseness, and diarrhea, as well as anemia (8; 20.5%), leukocytopenia (3; 7.7%), and thrombocytopenia (3; 7.7%) were of grade 1 and 2 severity. No treatment-related hemorrhage or hemoptysis was found.
Table 3. Treatment-related toxicity.
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-Hematological | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Secondary hypertension | 4(10.2) | 6(15.4) | 3(7.7) | 0(0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Proteinuria | 10(25.6) | 1(2.6) | 0(0) | 1(2.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hand–foot syndrome | 7(17.9) | 3(7.7) | 1(2.6) | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fatigue | 4(10.3) | 2(5.1) | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver enzyme elevation | 6(15.4) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bleeding | 2(5.1) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hoarseness | 1(2.6) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diarrhea | 1(2.6) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hematological | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anemia | 8(20.5) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leukocytopenia | 2(5.1) | 1(2.6) | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thrombocytopenia | 3(7.7) | 0 | 0 | 0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Acute toxicity was evaluated according to the Common Terminology Criteria for Adverse Events version 3.0 (CTCAE 3.0). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Survival
At the time of the last follow-up, 19 patients survived from the disease, while 20 died of tumor recurrence or metastases. The median PFS and OS of the whole cohort were 27.5 (95%CI: 14.9-40.1) and 38.1 (95%CI: 31.3-44.8) months, respectively. The Kaplan–Meier curves showed 1- and 3-year PFS rates of 82.1% and 32.3%, respectively. The OS rates at 1-, 3-, and 5-years of all enrolled patients were 89.7%, 56.5%, and 28.3%, respectively (Figure 1).
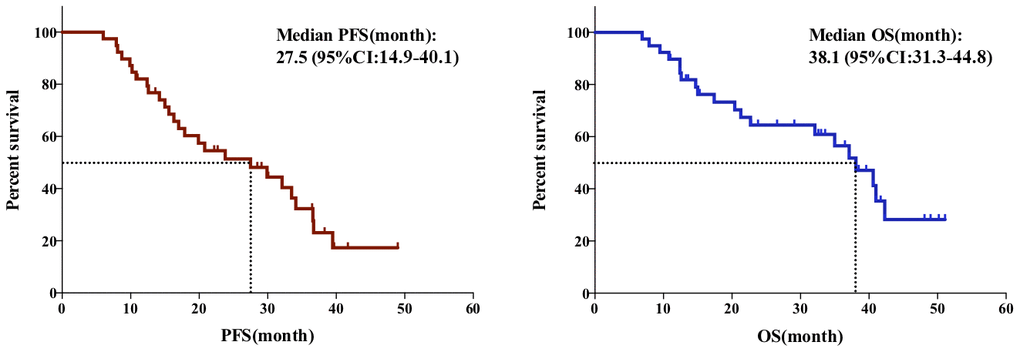
Figure 1. The PFS (Left) and OS (Right) of the whole cohort.
Univariate analysis showed a significant correlation between poor PFS and variables including SD after dCRT, combination of fistula, no adverse event, no absence of secondary hypertension or hand-foot syndrome (p<0.05). Upon inclusion of these variables in the Cox multivariate regression model, the multivariate analysis showed response after dCRT (HR = 3.663, 95%[CI] = 1.560 - 8.599), combination of fistula (HR = 5.799, 95%[CI] = 2.247-14.961), adverse events (HR = 0.274, 95%[CI] = 0.119 - 0.630), to be independent predictors of PFS in the whole cohort (Figure 2A–2C) (Table 4). Further, multivariate analysis showed SD after dCRT (HR= 5.858, 95%[CI]= 2.082-16.488), combination of fistula (HR= 10.193, 95%[CI]= 3.291 - 31.568), and no absence of proteinuria (HR= 0.108, 95%[CI]= 0.025 - 0.456), predicted worse prognosis in OS (Figure 2D, 2E) (Table 5). No significant between-group difference was found upon treatment with S1/capecitabine followed by apatinib and concurrent treatment with apatinib.
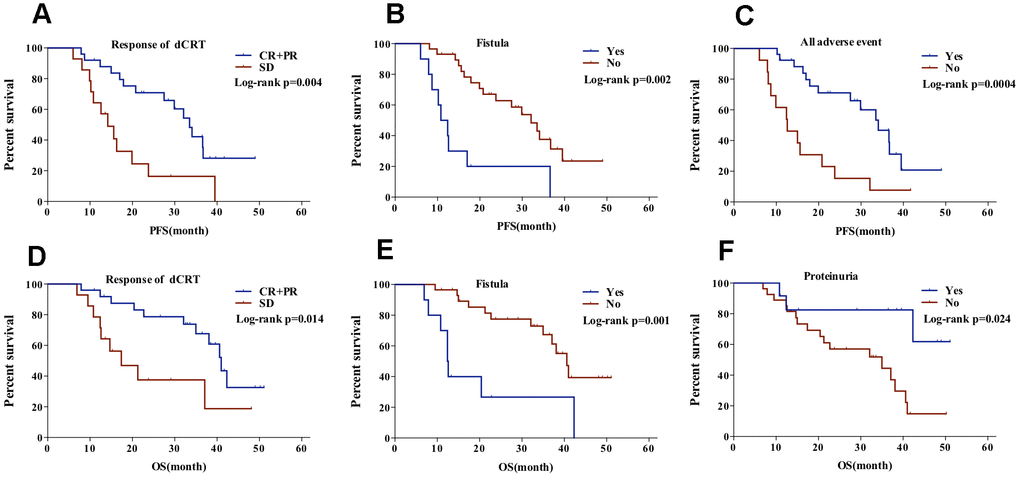
Figure 2. PFS of patients (A) with CR+PR vs SD after dCRT, (B) with vs without fistula, and (C) with vs without any adverse event; OS of patients with (D) CR+PR vs SD after dCRT, (E) with vs without fistula, and (F) with vs without proteinuria.
Table 4. Univariate and multivariate analysis of PFS.
| Variables | univariate analysis | multivariate analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR(95% CI) | p value | log-rank p | HR(95% CI) | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender (male vs female) | 0.577(0.169-1.965) | 0.379 | 0.373 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age(<60 vs ≥60) | 0.905(0.417-1.963) | 0.8 | 0.8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Length(<5 vs ≥5cm) | 1.752(0.758-4.051) | 0.19 | 0.184 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TNM stage (II vs III) | 2.824(0.664-12.003) | 0.16 | 0.142 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Concurrent Chemotherapy regimens | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single reagent | Reference | 0.105 | 0.086 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP | 0.330(0.097-1.130) | 0.077 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PF | 0.356(0.130-0.977) | 0.045 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiation dose (≤60 vs >60Gy) | 0.596(0.249-1.425) | 0.244 | 0.239 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Response (PR vs SD) | 3.221(1.448-7.165) | 0.004* | 0.003* | 3.663(1.560-8.599) | 0.003* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual disease sites | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary lesion only | reference | 0.779 | 0.778 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Regional lymph nodes only | 0.702(0.251-1.966) | 0.501 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary lesion combined with Regional lymph nodes | 0.898(0.340-2.367) | 0.827 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathological residual disease (Yes vs No) | 2.061(0.939-4.524) | 0.071 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fistula (Yes vs No) | 4.149(1.766-9.749) | 0.001* | 0.0004* | 5.799(2.247-14.961) | 0.0003* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| S1/capecitabine followed by apatinib vs concurrent with apatinib | 2.887(0.850-4.191) | 0.119 | 0.113 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| side effects related | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overall side effects (No vs Yes) | 0.294(0.134-0.644) | 0.002* | 0.001* | 0.274(0.119-0.630) | 0.002* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Secondary hypertension (No vs Yes) | 0.335(0.133-0.846) | 0.021* | 0.015* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Proteinuria (No vs Yes) | 0.425(0.167-1.080) | 0.072 | 0.065 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hand–foot syndrome (No vs Yes) | 0.368(0.146-0.928) | 0.034* | 0.028* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP: taxol and platinum; PF: platinum and fluorouracil; PR: partial response; SD: stable disease | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 5. Univariate and multivariate analysis of OS.
| Variables | univariate analysis | multivariate analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR(95% CI) | P value | log-rank p | HR(95% CI) | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender (male vs female) | 0.792(0.226-2.781) | 0.716 | 0.715 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age(<60 vs ≥60) | 1.060(0.440-2.558) | 0.896 | 0.896 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Length(<5 vs ≥5cm) | 2.301(0.830-6.376) | 0.109 | 0.099 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TNM stage (II vs III) | 2.564(0.583-11.265) | 0.213 | 0.197 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Concurrent Chemotherapy regimens | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single reagent | Reference | 0.583 | 0.573 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP | 0.506(0.124-2.066) | 0.343 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PF | 0.580(0.183-1.843) | 0.356 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiation dose (≤60 vs >60Gy) | 0.562(0.204-1.549) | 0.265 | 0.258 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Response (PR vs SD) | 2.844(1.145-7.062) | 0.024* | 0.019* | 5.858(2.082-16.488) | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Failure pattern | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary lesion only | Reference | 0.767 | 0.764 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Regional lymph nodes only | 0.655(0.210-2.050) | 0.468 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary lesion combined with Regional lymph nodes | 0.784(0.267-2.295) | 0.656 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pathological residual disease(Yes vs No) | 2.291(0.948-5.538) | 0.066 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fistula | 4.224(1.680-10.620) | 0.002* | 0.001* | 10.193(3.291-31.568) | 0.00004 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| S1/capecitabine followed by apatinib vs concurrent with apatinib | 1.318(0.528-3.290) | 0.555 | 0.553 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| side effects related | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overall side effects (No vs Yes) | 0.277(0.109-0.703) | 0.007* | 0.004* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Secondary hypertension (No vs Yes) | 0.475(0.178-1.268) | 0.475 | 0.129 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Proteinuria (No vs Yes) | 0.244(0.068-0.870) | 0.030* | 0.020* | 0.108(0.025-0.456) | 0.002 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hand–foot syndrome (No vs Yes) | 0.459(0.172-1.223) | .0.119 | 0.111 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP: taxol and platinum; PF: platinum and fluorouracil; PR: partial response; SD: stable disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
Despite dCRT being a common curative approach for unresectable locally advanced ESCC, only 15-53% of treated patients will achieve CR upon completion of dCRT [16, 17]. Survival of patients with the clinical non-CR disease after initial CRT was substantially poor compared to those with CR [18]. Recent data shows an overall 3-year PFS of around 45% in ESCC patients who received dCRT indicating that over half of treated patients will develop recurrent disease within three years [19]. Patients with clinical non-CR disease account for a major portion of recurrence cases, suggesting that early control of the persistent disease may lead to survival benefits [20]. However, improved survival achieved through consolidated chemotherapy in ESCC patients after dCRT remains controversial, though the inconsistencies reported may be due to the enrollment of patients with and without CR in these studies [21]. Further, it may suggest the need for consolidative or maintenance therapy only for patients with persistent disease.
Thus far, a consensus treatment approach has not been established for patients with residual lesions. Recently, the addition of individualized multimodal approaches such as salvage surgery, photodynamic therapy, and endoscopic mucosal resection after the local failure of dCRT have been reported to prolong patient survival [16, 22–25]. However, only a small subset of patients is eligible for such local treatments. Further, salvage surgery is associated with increased susceptibility to postoperative complications such as anastomotic leakage due to prior treatment with a relatively high dose of radiation [25]. Conventional treatment strategies in clinical practice include close follow-up and second-line chemotherapy is recommended upon confirmation of disease progression. Thus, intravenous systemic chemotherapy is frequently used to arrest disease recurrence and progression. However, patient compliance is generally poor due to the occurrence of high toxicity leading to early termination [6]. Oral drugs include the TKIs and chemotherapy agents are widely used as the substitute for intravenous infusion chemotherapy regimens, suggesting they are also good candidates as the maintenance therapy for those with residual disease after dCRT.
Fluorouracil is a standard chemotherapeutic agent for ESCC. There are now two commercially available oral fluorouracil agents — S-1 and capecitabine — with similar proven anticancer effects compared to intravenous 5-Fu [7, 8]. The safety and efficacy of chemoradiotherapy with concurrent S-1 and cisplatin for ESCC were explored in a phase I/II trial (JCOG0604), which showed a favorable 3-year OS rate of 61.9%, CR rate of 59.5% and, acceptable toxicity, comparable to conventional chemotherapy [26]. Similarly, another phase II study demonstrated that concurrent selective lymph node radiotherapy and S-1 with cisplatin were feasible and well-tolerated in patients with stage II–IVa ESCC [11]. Besides its application as a first-line treatment, S-1 combined with chemotherapy has also been used as a second-line treatment in ESCC [10, 27]. To further improve its advantages as an oral formulation and its convenience as a continuous delivery application, without the need for intravenous infusion compared with 5-Fu, emerging studies have been conducted by combining S-1 with TKIs as dual oral agents.
Apatinib is a small-molecule TKI that targets VEGFR-2, thereby inhibiting VEGF-mediated endothelial cell migration, which impairs tumor microvasculature and suppressing tumor growth [28]. Apatinib was first shown to significantly improve OS and PFS with limited toxicity when used as a later line therapy in advanced adenocarcinoma of the stomach or gastroesophageal junction in a randomized phase III trial [29]. It was then widely applied in gastric cancer and then expanded to the treatment of lung, sarcoma, and liver cancer [30]. The use of apatinib as a second-line treatment monotherapy for advanced ESCC achieved median PFS and OS of 3.5 and 7 months, respectively [13]. These findings were confirmed in a phase II study, which showed that the monotherapy achieved an OR of 7.7%, with median PFS and OS at 4.63 and 6.57 months, respectively [31]. Moreover, in vivo and in vitro studies have demonstrated that apatinib significantly increased the sensitivity to paclitaxel, cisplatin, and 5-Fu, suggesting that it is feasible to combine apatinib with other chemotherapeutic agents to yield a synergistic effect [32–34].
When combined with S-1, treatment of advanced gastric cancer with apatinib has been explored [35]. Zhao et al. first reported the use of this combination regimen as second-line treatment in 15 advanced ESCC patients who received apatinib (250-500 mg) plus S-1 until disease progression. The median PFS and OS were 6.23 and 8.83 months, respectively, which are longer than previously reported data of monotherapy, suggesting an improvement in the efficacy of tumor control with dual treatment [15]. The results of our retrospective analysis of 39 ESCC patients with residual disease after dCRT who received apatinib plus S-1/capecitabine showed a satisfactory survival with a median PFS of 27.5 (95%CI: 14.9-40.1) and OS of 38.1 (95%CI: 31.3-44.8) months. The reported median OS and OS rate at 3-years of those patients with local advanced ESCC who received dCRT varied from 9.0 to 41.0 months and 21 to 45% [36–38]. Similar to published studies, we found that the response after dCRT, as an independent factor, was correlated with the better prognosis of patients in the multivariate analysis. In those patients who achieved clinical CR or good response, the median OS was 46 months and the 3-years survival rate was 57%, which were significantly better than others [39]. The survival data reported in this study was comparable to the patients who had CR after dCRT, suggesting that maintenance therapy for those non-CR ESCC is a promising strategy to improve survival.
Secondary hypertension, hand-foot syndrome, and proteinuria were the most common adverse events associated with treatment. These largely overlapped with the toxicity profile of anti-angiogenic agents including apatinib, and consistent with previous reports, were grade 1 to 2 in severity and therefore, tolerable [40, 41]. Although one confirmed case showed grade 4 proteinuria, the patient had recovered rapidly upon the cessation of apatinib. In addition, there was no worsening in toxicity when apatinib was combined with S-1/capecitabine, which may reflect the differences in the toxicity spectrum between S-1/capecitabine and apatinib. Similar to other TKIs, toxicity related to apatinib was a predictive biomarker for treatment response and survival [42]. In our multivariate analysis, patients with an occurrence of adverse events related to apatinib showed significantly longer PFS compared to those with none. Moreover, proteinuria was also significantly correlated with improved OS. VEGF-TKI targets VEGFR2 and then decreased the release of nitric oxide from endothelial cells, leading to the constant contraction of arterial smooth muscle cells to induce hypertension [43]. These side effects mostly are caused by the sufficient action of VEGF-TKIs thus representing the ‘‘on-target’’ effect in normal tissues. This partially explained why there was a positive correlation between the occurrence of side effects and better tumor control. However, due to the limited number of enrolled patients, our conclusions must remain tentative.
Strengths and limitations
To the best of our knowledge, this is the first retrospective analysis to show the use of apatinib combined with S-1/capecitabine as the maintenance therapy for ESCC with residual disease after dCRT. Ongoing prospective clinical trials exploring the efficiency of apatinib alone or in combination with other agents for EC are listed in Table 6. Since apatinib and S-1/capecitabine are orally administered drugs, the convenience of its application offers a significant advantage over other regimens. Further, an improvement in patient compliance to oral therapy is expected since hospital admission or continuous intravenous infusion can be avoided and therefore achieve tumor control over a longer period. The small sample size and the retrospective nature of this study are significant limitations.
Table 6. Clinical trials of apatinib in EC.
| Agents | Other agents | Conditions | Phase | No. | Design | Endpoints | NCT ID | Status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Apatinib | Metastatic EC | 2 | 40 | Randomized; open-label | PFS | NCT02683655 | Unknown | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N/A | Metastatic EC | 2 | 29 | Single group; open-label | response; AEs; OS; PFS | NCT02544737 | Unknown | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Esophageal and Gastric Cancer | 2/3 | 30 | Single group; open-label | PFS; OS | NCT03285906 | Unknown | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Advanced EC | 2 | 50 | Single group; open-label | PFS; OS | NCT03542422 | Unknown | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Advanced EC | 2 | 60 | Single group; open-label | PFS; OS | NCT03170310 | Unknown | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrent and Metastatic EC | 2 | 40 | Single group; open-label | PFS; OS; response | NCT03274011 | Active, not recruiting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrent and Metastatic EC | 2 | 39 | Single group; open-label | PFS; OS; response | NCT03913182 | Recruiting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multiple Malignancies including EC | 4 | 38 | Single group; open-label | response; AEs; OS; PFS | NCT03384511 | Completed | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrent and Metastatic EC | 2 | 120 | Randomized; parallel; single-blind | PFS; OS; response | NCT03787251 | Not yet recruiting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EC | 2 | 43 | Single group; open-label | response; AEs; OS; PFS | NCT02976896 | Recruiting | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Irinotecan | Unresectable or Metastatic EC | 2 | 50 | Single group; open-label | response; AEs; OS; PFS | NCT03251417 | Recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EC | 1 | 9 | Single group; open-label | response; AEs; OS; PFS | NCT02645864 | Unknown | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Docetaxel | Advanced EC | 2 | 120 | Randomized;parallel Assignment | PFS; OS | NCT03193424 | Unknown | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Docetaxel, Nedaplatin, Endostar VS Docetaxel, Nedaplatin | EC | 2 | 186 | Randomized; parallel; single-blind | PFS; OS | NCT03649945 | Not yet recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fluorouracil and platinum | EC | 2 | 189 | Randomized; parallel | response; AEs; OS; PFS | NCT03224221 | Unknown | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Paclitaxel, Cisplatin+RT | EC | 2 | 40 | Single group; open-label | response; AEs; OS; DFS | NCT03857763 | Not yet recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| S-1+ RT | Refractory or Metastatic EC | 2 | 80 | Randomized; parallel; open-label | response; AEs; OS; DFS | NCT03320629 | Unknown | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SHR-1210 | Advanced EC | 2 | 45 | Single group; open-label | PFS; response | NCT03736863 | Not yet recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SHR-1210+ Docetaxel, Cisplatin+ RT | Local Advanced EC | NA | 20 | Single group; open-label | response; AEs; OS; PFS | NCT03671265 | Recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SHR-1210+ Irinotecan, Paclitaxel, Nedaplatin | Advanced EC | 2 | 45 | Non-Randomized; parallel; open-label | response; AEs; OS; PFS | NCT03603756 | Recruiting | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RT: radiotherapy; EC: esophageal carcinoma; AEs: adverse events; OS: overall survival; PFS: progression-free survival; DFS: disease-free survival. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Conclusions
In conclusion, our study suggested that the oral combination therapy of apatinib and S-1/capecitabine holds significant and promising efficacy with manageable toxicity for the treatment of ESCC in patients with residual disease after dCRT. Prospective clinical trials are warranted to further confirm the feasibility of this treatment regimen.
Materials and Methods
This study was approved by the Sun Yat-Sen University Cancer Center Human Research Ethical Committee. Informed consent was obtained from all enrolled patients.
Eligibility criteria
Patients diagnosed with ESCC and post-dCRT residual lesions were enrolled in this retrospective study. The inclusion criteria were (1) Histopathologically-confirmed ESCC; (2) Age ≥18 years; (3) Eastern Cooperative Oncology Group - Performance Status (ECOG-PS) scores from 0-2; (4) Local residual disease confirmed by endoscopy, ultrasonography, computed tomography (CT), physical examination and/or biopsy at three months after the completion of dCRT; (5) No distant metastasis; (6) Life expectancy ≥ 6 months.
Treatment regimen
Patients in this retrospective analysis were orally treated with S-1 twice daily at 40 mg (body surface area <1.25 m2) or 60 mg (body surface area ≥ 1.25 m2). In the event of shortage, unacceptable toxicity, or patient refusal of S-1, capecitabine was orally administered twice daily at 1.25g/m2. Treatment with S-1 or capecitabine treatment followed a four-week cycle consisting of three weeks of treatment followed by one-week rest. Patients were concurrently treated with apatinib once daily at 250 to 500 mg per four-week cycle. Patients who could not tolerate dual treatments at the beginning were treated initially with S-1/capecitabine and sequentially with apatinib after 1-2 cycle of S-1/capecitabine. Treatments were scheduled until the progressive disease was confirmed, due to unacceptable toxicity or patient refusal.
Response, toxicity, and survival
Patient’s response to treatment was assessed by CT scan and endoscopy at one or two months after initiating maintenance therapy, according to Response Evaluation Criteria in Solid Tumors 1.1 (RECIST 1.1) criteria. The ORR and DCR were calculated. During treatment, complete blood count, serum chemistry profile, and urine routine test were examined each month to monitor toxicity. Adverse events were assessed and graded into 0-V degrees according to the Common Terminology Criteria for Adverse Events version 3.0 (CTCAE 3.0). The duration from maintenance treatment to tumor progression or death (Progression-Free Survival; PFS), and to mortality or the last follow-up (Overall Survival; OS) were calculated.
Statistical analysis
The Kaplan–Meier curves with the log-rank test were used to analyze and compare the median PFS and OS. Multivariate analysis was performed using Cox regression to analyze the prognostic factors. The SPSS 26.0 and GraphPad Prism 5.0 were used for analyses. P <0.05 considered being statistically significant.
Author Contributions
All authors should have made substantial contributions to all of the following: (1) DMC, BQC, SPG, KHB, HLM, YHH, QQL, and YJZ contributed to the conception and design of the study. (2) DMC, BQC, QQL, and KHB contributed to the acquisition, analysis, and interpretation of data. (3) DMC, BQC, and YJZ drafted the article and submitted it. All authors revised and approved the final manuscript.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This work was supported by Guangdong Esophageal Cancer Institute Science and Technology Program (No.Q201807).
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019; 69:7–34. https://doi.org/10.3322/caac.21551 [PubMed]
- 2. Liang H, Fan JH, Qiao YL. Epidemiology, etiology, and prevention of esophageal squamous cell carcinoma in China. Cancer Biol Med. 2017; 14:33–41. https://doi.org/10.20892/j.issn.2095-3941.2016.0093 [PubMed]
- 3. Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Corvera C, Das P, Denlinger CS, Enzinger PC, Fanta P, Farjah F, Gerdes H, Gibson M, Glasgow RE, et al. Esophageal and esophagogastric junction cancers, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019; 17:855–83. https://doi.org/10.6004/jnccn.2019.0033 [PubMed]
- 4. Sudo K, Kato K, Kuwabara H, Sasaki Y, Takahashi N, Shoji H, Iwasa S, Honma Y, Okita NT, Takashima A, Hamaguchi T, Yamada Y, Ito Y, et al. Patterns of relapse after definitive chemoradiotherapy in stage II/III (Non-T4) esophageal squamous cell carcinoma. Oncology. 2018; 94:47–54. https://doi.org/10.1159/000480515 [PubMed]
- 5. Liw PX, Wen YW, Tsai CY, Chang HK, Tseng CK, Hung TM, Chao YK. Pretreatment clinical stage predicts locoregional recurrence in patients with esophageal cancer who achieved a complete clinical response to chemoradiotherapy. J Thorac Cardiovasc Surg. 2018; 155:2233–2242.e2. https://doi.org/10.1016/j.jtcvs.2017.12.082 [PubMed]
- 6. Osaka Y, Takagi Y, Hoshino S, Tachibana S, Tsuchida A, Aoki T. Combination chemotherapy with docetaxel and nedaplatin for recurrent esophageal cancer in an outpatient setting. Dis Esophagus. 2006; 19:473–76. https://doi.org/10.1111/j.1442-2050.2006.00614.x [PubMed]
- 7. Boku N, Yamamoto S, Fukuda H, Shirao K, Doi T, Sawaki A, Koizumi W, Saito H, Yamaguchi K, Takiuchi H, Nasu J, Ohtsu A, and Gastrointestinal Oncology Study Group of the Japan Clinical Oncology Group. Fluorouracil versus combination of irinotecan plus cisplatin versus S-1 in metastatic gastric cancer: a randomised phase 3 study. Lancet Oncol. 2009; 10:1063–69. https://doi.org/10.1016/S1470-2045(09)70259-1 [PubMed]
- 8. Shiozawa M, Sugano N, Tsuchida K, Morinaga S, Akaike M, Sugimasa Y. A phase I study of combination therapy with S-1 and irinotecan (CPT-11) in patients with advanced colorectal cancer. J Cancer Res Clin Oncol. 2009; 135:365–70. https://doi.org/10.1007/s00432-008-0480-5 [PubMed]
- 9. Rich T. Capecitabine and radiation therapy for advanced gastrointestinal Malignancies. Oncology (Williston Park). 2002; 16:27–30. [PubMed]
- 10. Nakamura T, Ota M, Narumiya K, Sato T, Shirai Y, Yamamoto M, Kuramochi H, Hayashi K. [Docetaxel plus S-1 as a second-line chemotherapy for metastasis or recurrence of esophageal cancer]. Gan To Kagaku Ryoho. 2012; 39:227–30. [PubMed]
- 11. Wang X, Liu X, Li D, Wang X, Huang W, Li B. Concurrent selective lymph node radiotherapy and S-1 plus cisplatin for esophageal squamous cell carcinoma: a phase II study. Ann Surg Oncol. 2019; 26:1886–92. https://doi.org/10.1245/s10434-019-07264-4 [PubMed]
- 12. Xue JM, Astère M, Zhong MX, Lin H, Shen J, Zhu YX. Efficacy and safety of apatinib treatment for gastric cancer, hepatocellular carcinoma and non-small cell lung cancer: a meta-analysis. Onco Targets Ther. 2018; 11:6119–28. https://doi.org/10.2147/OTT.S172717 [PubMed]
- 13. Li J, Wang L. Efficacy and safety of apatinib treatment for advanced esophageal squamous cell carcinoma. Onco Targets Ther. 2017; 10:3965–69. https://doi.org/10.2147/OTT.S132756 [PubMed]
- 14. Li YH, Zhou Y, Wang YW, Tong L, Jiang RX, Xiao L, Zhang GJ, Xing SS, Qian F, Feng JQ, Zhao YL, Wang JG, Wang XH. Comparison of apatinib and capecitabine (xeloda) with capecitabine (xeloda) in advanced triple-negative breast cancer as third-line therapy: a retrospective study. Medicine (Baltimore). 2018; 97:e12222. https://doi.org/10.1097/MD.0000000000012222 [PubMed]
- 15. Zhao J, Lei J, Yu J, Zhang C, Song X, Zhang N, Wang Y, Zhang S. Clinical efficacy and safety of apatinib combined with S-1 in advanced esophageal squamous cell carcinoma. Invest New Drugs. 2020; 38:500–06. https://doi.org/10.1007/s10637-019-00866-5 [PubMed]
- 16. Swisher SG, Moughan J, Komaki RU, Ajani JA, Wu TT, Hofstetter WL, Konski AA, Willett CG. Final results of NRG oncology RTOG 0246: an organ-preserving selective resection strategy in esophageal cancer patients treated with definitive chemoradiation. J Thorac Oncol. 2017; 12:368–74. https://doi.org/10.1016/j.jtho.2016.10.002 [PubMed]
- 17. Sasaki Y, Kato K. Chemoradiotherapy for esophageal squamous cell cancer. Jpn J Clin Oncol. 2016; 46:805–10. https://doi.org/10.1093/jjco/hyw082 [PubMed]
- 18. Berger AC, Farma J, Scott WJ, Freedman G, Weiner L, Cheng JD, Wang H, Goldberg M. Complete response to neoadjuvant chemoradiotherapy in esophageal carcinoma is associated with significantly improved survival. J Clin Oncol. 2005; 23:4330–37. https://doi.org/10.1200/JCO.2005.05.017 [PubMed]
- 19. Chen Y, Ye J, Zhu Z, Zhao W, Zhou J, Wu C, Tang H, Fan M, Li L, Lin Q, Xia Y, Li Y, Li J, et al. Comparing paclitaxel plus fluorouracil versus cisplatin plus fluorouracil in chemoradiotherapy for locally advanced esophageal squamous cell cancer: a randomized, multicenter, phase III clinical trial. J Clin Oncol. 2019; 37:1695–703. https://doi.org/10.1200/JCO.18.02122 [PubMed]
- 20. Chen M, Liu P, Chen Y, Chen Z, Shen M, Liu X, Li X, Lin Y, Yang R, Ni W, Zhou X, Zhang L, Tian Y, Chen J. Primary tumor regression patterns in esophageal squamous cell cancer treated with definitive chemoradiotherapy and implications for surveillance schemes. Cancer Manag Res. 2019; 11:3361–69. https://doi.org/10.2147/CMAR.S198524 [PubMed]
- 21. Adenis A, Castan F, Conroy T. Consolidation chemotherapy after definite concurrent chemoradiation in patients with non-operable esophageal cancer: is it useful? Radiother Oncol. 2018; 129:180–81. https://doi.org/10.1016/j.radonc.2017.12.018 [PubMed]
- 22. Hatogai K, Yano T, Kojima T, Onozawa M, Fujii S, Daiko H, Yoda Y, Hombu T, Doi T, Kaneko K, Ohtsu A. Local efficacy and survival outcome of salvage endoscopic therapy for local recurrent lesions after definitive chemoradiotherapy for esophageal cancer. Radiat Oncol. 2016; 11:31. https://doi.org/10.1186/s13014-016-0604-z [PubMed]
- 23. Yano T, Muto M, Minashi K, Ohtsu A, Yoshida S. Photodynamic therapy as salvage treatment for local failures after definitive chemoradiotherapy for esophageal cancer. Gastrointest Endosc. 2005; 62:31–36. https://doi.org/10.1016/s0016-5107(05)00545-6 [PubMed]
- 24. Taniyama Y, Sakurai T, Heishi T, Okamoto H, Sato C, Maruyama S, Onodera Y, Ishida H, Unno M, Kamei T. Different strategy of salvage esophagectomy between residual and recurrent esophageal cancer after definitive chemoradiotherapy. J Thorac Dis. 2018; 10:1554–62. https://doi.org/10.21037/jtd.2018.03.04 [PubMed]
- 25. Faiz Z, Dijksterhuis WP, Burgerhof JG, Muijs CT, Mul VE, Wijnhoven BP, Smit JK, Plukker JT. A meta-analysis on salvage surgery as a potentially curative procedure in patients with isolated local recurrent or persistent esophageal cancer after chemoradiotherapy. Eur J Surg Oncol. 2019; 45:931–40. https://doi.org/10.1016/j.ejso.2018.11.002 [PubMed]
- 26. Tahara M, Fuse N, Mizusawa J, Sato A, Nihei K, Kanato K, Kato K, Yamazaki K, Muro K, Takaishi H, Boku N, Ohtsu A. Phase I/II trial of chemoradiotherapy with concurrent S-1 and cisplatin for clinical stage II/III esophageal carcinoma (JCOG 0604). Cancer Sci. 2015; 106:1414–20. https://doi.org/10.1111/cas.12764 [PubMed]
- 27. Ter Veer E, Haj Mohammad N, van Valkenhoef G, Ngai LL, Mali RM, van Oijen MG, van Laarhoven HW. Second- and third-line systemic therapy in patients with advanced esophagogastric cancer: a systematic review of the literature. Cancer Metastasis Rev. 2016; 35:439–56. https://doi.org/10.1007/s10555-016-9632-2 [PubMed]
- 28. Li J, Zhao X, Chen L, Guo H, Lv F, Jia K, Yv K, Wang F, Li C, Qian J, Zheng C, Zuo Y. Safety and pharmacokinetics of novel selective vascular endothelial growth factor receptor-2 inhibitor YN968D1 in patients with advanced Malignancies. BMC Cancer. 2010; 10:529. https://doi.org/10.1186/1471-2407-10-529 [PubMed]
- 29. Li J, Qin S, Xu J, Xiong J, Wu C, Bai Y, Liu W, Tong J, Liu Y, Xu R, Wang Z, Wang Q, Ouyang X, et al. Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Apatinib in Patients With Chemotherapy-Refractory Advanced or Metastatic Adenocarcinoma of the Stomach or Gastroesophageal Junction. J Clin Oncol. 2016; 34:1448–54. https://doi.org/10.1200/JCO.2015.63.5995 [PubMed]
- 30. Zhao D, Hou H, Zhang X. Progress in the treatment of solid tumors with apatinib: a systematic review. Onco Targets Ther. 2018; 11:4137–47. https://doi.org/10.2147/OTT.S172305 [PubMed]
- 31. Yanwei L, Feng H, Ren P, Yue J, Zhang W, Tang P, Shang X, Pang Q, Liu D, Chen C, Pan Z, Tao YZ. Safety and efficacy of apatinib monotherapy for unresectable, metastatic esophageal cancer: a single-arm, open-label, phase II study. Oncologist. 2020; 25:e1464–72. https://doi.org/10.1634/theoncologist.2020-0310 [PubMed]
- 32. Xu Z, Hu C, Chen S, Zhang C, Yu J, Wang X, Lv H, Cheng X. Apatinib enhances chemosensitivity of gastric cancer to paclitaxel and 5-fluorouracil. Cancer Manag Res. 2019; 11:4905–15. https://doi.org/10.2147/CMAR.S196372 [PubMed]
- 33. Wei B, Wang Y, Wang J, Cai X, Xu L, Wu J, Wang Y, Liu W, Gu Y, Guo W, Xu Q. Apatinib suppresses tumor progression and enhances cisplatin sensitivity in esophageal cancer via the Akt/β-catenin pathway. Cancer Cell Int. 2020; 20:198. https://doi.org/10.1186/s12935-020-01290-z [PubMed]
- 34. Qiu H, Li J, Liu Q, Tang M, Wang Y. Apatinib, a novel tyrosine kinase inhibitor, suppresses tumor growth in cervical cancer and synergizes with paclitaxel. Cell Cycle. 2018; 17:1235–44. https://doi.org/10.1080/15384101.2018.1471315 [PubMed]
- 35. Liu Y, Zhou C, Zhang K, Feng Y, Zhang R. The combination of apatinib and S-1 for the treatment of advanced gastric cancer in China: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018; 97:e13259. https://doi.org/10.1097/MD.0000000000013259 [PubMed]
- 36. Du D, Song T, Liang X, Fang M, Wu S. Concurrent chemoradiotherapy with elective lymph node irradiation for esophageal cancer: a systemic review and pooled analysis of the literature. Dis Esophagus. 2017; 30:1–9. https://doi.org/10.1111/dote.12471 [PubMed]
- 37. Luo Y, Mao Q, Wang X, Yu J, Li M. Radiotherapy for esophageal carcinoma: dose, response and survival. Cancer Manag Res. 2017; 10:13–21. https://doi.org/10.2147/CMAR.S144687 [PubMed]
- 38. Cooper SL, Russo JK, Chin S. Definitive chemoradiotherapy for esophageal carcinoma. Surg Clin North Am. 2012; 92:1213–48. https://doi.org/10.1016/j.suc.2012.07.013 [PubMed]
- 39. Zhao Z, Zhang Y, Wang X, Geng X, Zhu L, Li M. Clinical response to chemoradiotherapy in esophageal carcinoma is associated with survival and benefit of consolidation chemotherapy. Cancer Med. 2020; 9:5881–88. https://doi.org/10.1002/cam4.3273 [PubMed]
- 40. Lan CY, Wang Y, Xiong Y, Li JD, Shen JX, Li YF, Zheng M, Zhang YN, Feng YL, Liu Q, Huang HQ, Huang X. Apatinib combined with oral etoposide in patients with platinum-resistant or platinum-refractory ovarian cancer (AEROC): a phase 2, single-arm, prospective study. Lancet Oncol. 2018; 19:1239–46. https://doi.org/10.1016/S1470-2045(18)30349-8 [PubMed]
- 41. Zhang H. Apatinib for molecular targeted therapy in tumor. Drug Des Devel Ther. 2015; 9:6075–81. https://doi.org/10.2147/DDDT.S97235 [PubMed]
- 42. Fan M, Zhang J, Wang Z, Wang B, Zhang Q, Zheng C, Li T, Ni C, Wu Z, Shao Z, Hu X. Phosphorylated VEGFR2 and hypertension: potential biomarkers to indicate VEGF-dependency of advanced breast cancer in anti-angiogenic therapy. Breast Cancer Res Treat. 2014; 143:141–51. https://doi.org/10.1007/s10549-013-2793-6 [PubMed]
- 43. Tang JR, Markham NE, Lin YJ, McMurtry IF, Maxey A, Kinsella JP, Abman SH. Inhaled nitric oxide attenuates pulmonary hypertension and improves lung growth in infant rats after neonatal treatment with a VEGF receptor inhibitor. Am J Physiol Lung Cell Mol Physiol. 2004; 287:L344–51. https://doi.org/10.1152/ajplung.00291.2003 [PubMed]