




Introduction
Atrial fibrillation (AF) affected the quality of life (QOL) of 2 million patients in the United States and increased the risk of stroke and mortality [1, 2]. Antiarrhythmic drug therapy (ADT) to control heart rate and rhythm was the mainstay of paroxysmal AF (PAF) treatment. Treatment guidelines for elderly patients with PAF aim to reduce the frequency and recurrence rate; ADT was recommended as the first line treatment of PAF [3]. Amiodarone was the most effective ADT for PAF, but it is associated with a limited curative effect and can lead to some serious side effects [4, 5]. Catheter ablation (CA), used after ADT failure in clinical therapy [6–9], is a minimally invasive procedure used to treat PAF and associated with side effects such as pulmonary vein stenosis, tamponade, fistula, etc. In some special cases, CA was used as the first-line treatment and can also be used concurrently with ADT [10]. The efficacy of CA was controversial in patients with AF who had received first-line ADT and varied among individuals [1, 6].
Studies have shown that the control rate of AF recurrence at 6 to 12 months is only about 46% [5, 9–11] and the patients often discontinue therapy due to side effects [2, 7, 8]. It has been confirmed that the first-line use of CA without ADT can achieve a 60% non-recurrence rate and reduced the recurrence rate of PAF compared with ADT [2, 5, 10], but this result has not been confirmed in the investigation of the accumulated burden of PAF to patients [11]. Moreover, most clinical studies investigated the short-term curative effects and side effects of CA or ADT and rarely explored long-term efficacy and side effects [2, 8–10].
Therefore, our meta-analysis analyzed clinical studies using CA and ADT for managing PAF in terms of short- and long-term clinical efficacy and QOL to find differences between CA and ADT, with the aim of providing evidence on the standard treatment of PAF in elderly patients.
Results
Included studies
The relevant RCTs published from January 2005 to June 2020 in the Cochrane Library, MEDLINE, PubMed, and EMBASE were 288, of which 87 were not RCTs, 53 reported persistent AF, 48 had no age data and 92 had no 3-month AF-free rate data (Figure 1). A total of 8 RCT studies [2, 5, 7–12] involving 1336 patients (718 underwent CA, CA group; 618 underwent ADT; ADT group) on CA and ADT for treating PAF were included (Table 1). All studies included AF-free rate data at the 3- and 6-month follow-up; 7 had AF-free rate data at the 9-month, 5 had AF-free rate data at the 12-month, and 3 had AF-free rate data at the 24-month follow-up. For QOL, meta-analysis was conducted on the physical component summary, mental component summary, symptom frequency and symptom severity data in the groups at 3 months and 12 months.
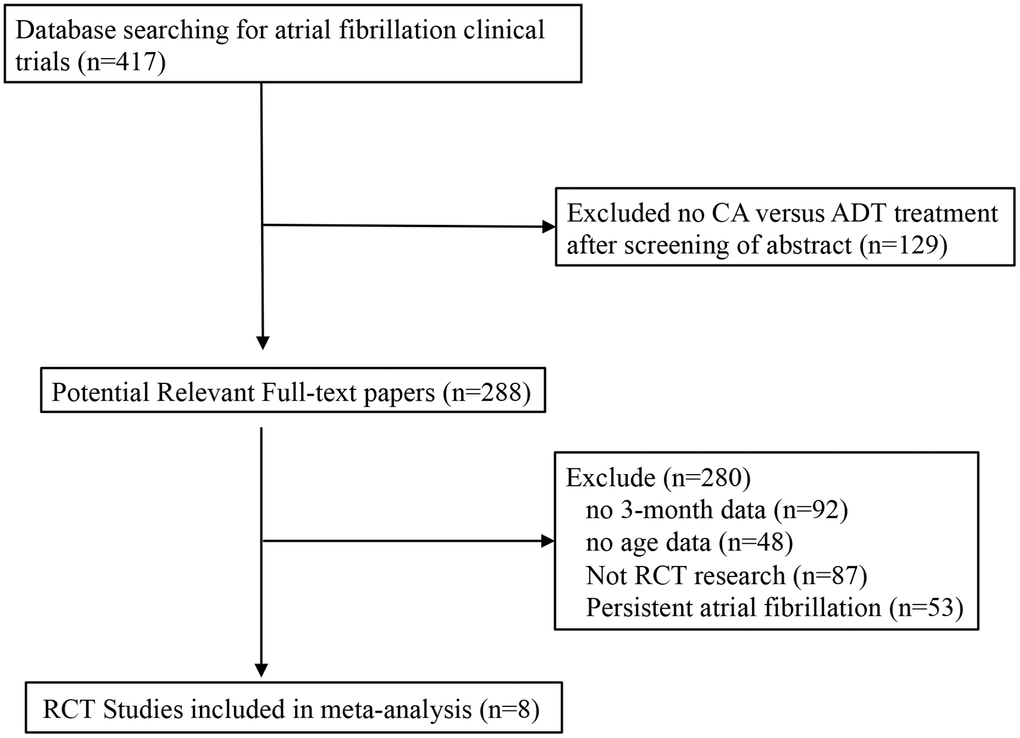
Figure 1. Flow diagram of studies selection process.
Table 1. Basic characteristics of the included studies.
| Study | Treatment | Patient number | Follow-up | 12-month AF free | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Carlos A. Morillo | PVI | 66 | 24 months | 73% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 61 | 65% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oussama M. Wazni | PVI | 33 | 12 months | 87% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 37 | 37% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pierre Jais | PVI | 112 | 12 months | 89% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 59 | 23% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jens Cosedis Nielsen | PVI | 146 | 24 months | 85% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 148 | 71% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Carlo Pappone | PVI | 99 | 12 months | 84.8% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 99 | 29.3% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| David J. Wilber | PVI | 106 | 9 months | none | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 61 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Evgeny Pokushalov | PVI | 77 | 36 months | 72.7% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 77 | 32.5% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Carina Blomstrom-Lundqvist | PVI | 79 | 48 months | 83.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ADT | 76 | 77.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviation: PVI, pulmonary vein isolation; ADT, antiarrhythmic drug; AF free, Atrial fibrillation-free. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Main outcomes
AF-free rate at 3 months
At the 3-month follow-up, 511 of the 651 patients in the CA group were AF-free and 379 of the 616 patients in the ADT group were AF-free. The random effects model showed a Z score of 1.73. Patients with PAF had similar outcomes in terms of AF occurrence (RR 1.32; 95% confidence interval [CI] 0.96-1.82; P = 0.08) (Figure 2).
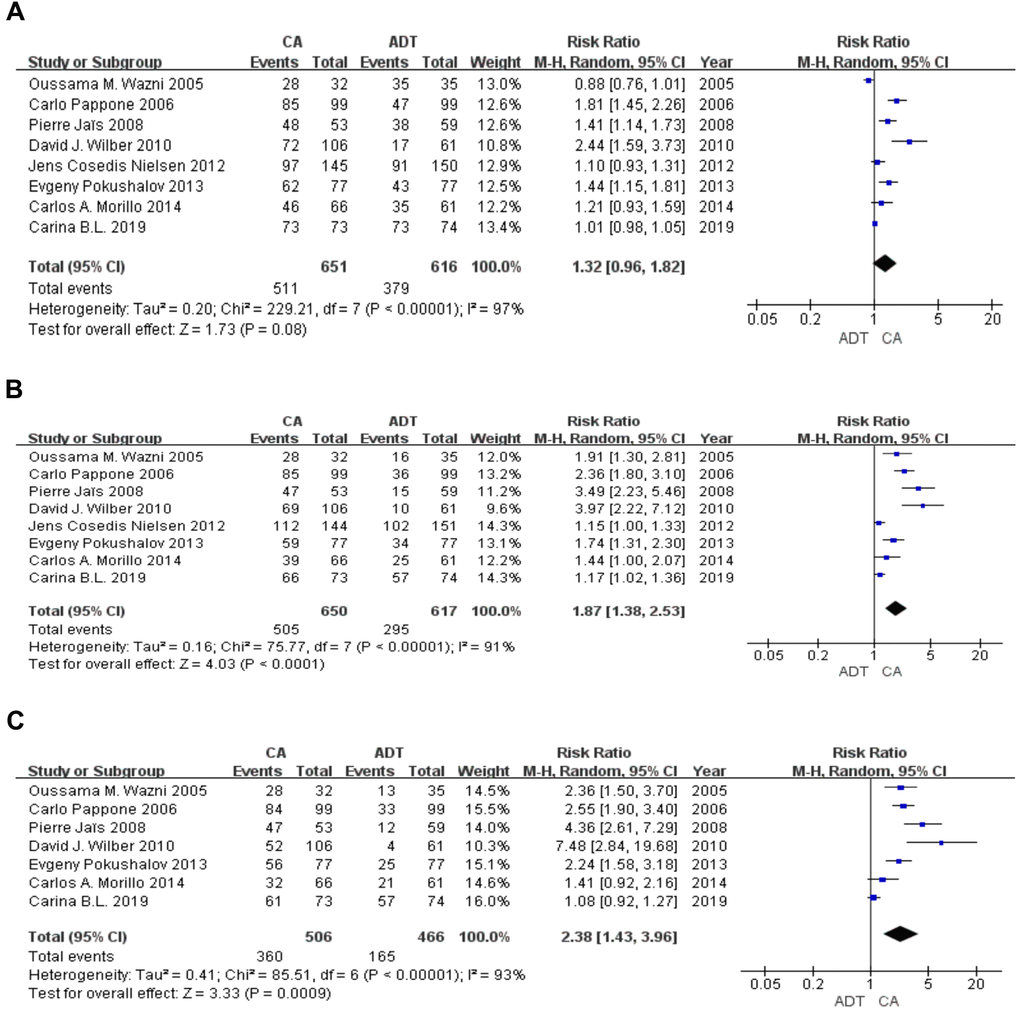
Figure 2. Forest plot of the AF-free rate in the short term. The AF-free rate was similar at 3 months (A) and significantly higher in the CA group than in the ADT group in 6 (B), 9 (C) months.
AF-free rate from 6 months to 9 months
At the 6-month follow-up (8 RCTs), 505 of the 650 patients in the CA group were AF-free and 295 of the 617 patients in the ADT group were AF-free. The random effects model showed a Z score of 4.03 (RR 1.87; 95% CI 1.38-2.53; P < 0.001). At the 9-month follow-up (7 RCTs), 360 of the 506 patients in the CA group were AF-free and 165 of the 466 patients in the ADT group were AF-free. The random effects model showed a Z score of 3.33 (RR 2.38; 95% CI 1.43-3.96; P < 0.001) (Figure 2).
AF-free rate at 12months and 24 months
At the 12-month follow-up (5 RCTs), 336 of the 436 patients in the CA group were AF-free and 188 of the 450 patients in the ADT group were AF-free. The random effects model showed a Z score of 2.83 (I2=93%; RR 2.21; 95% CI 1.28-3.84; P = 0.005). These results suggest that CA resulted in a higher AF-free rate during the mid-term follow-up than ADT. At the 24-month follow-up (3 RCTs), 142 of the 283 patients in the CA group were AF-free and 91 of the 293 patients in the ADT group were AF-free. The random effects model showed a Z score of 1.87 (I2 = 82%; RR 1.81; 95% CI 0.97-3.36; P = 0.06). In the long-term follow-up, the CA group showed a non-significant increase in the AF-free rate compared with the ADT group (Figure 3).
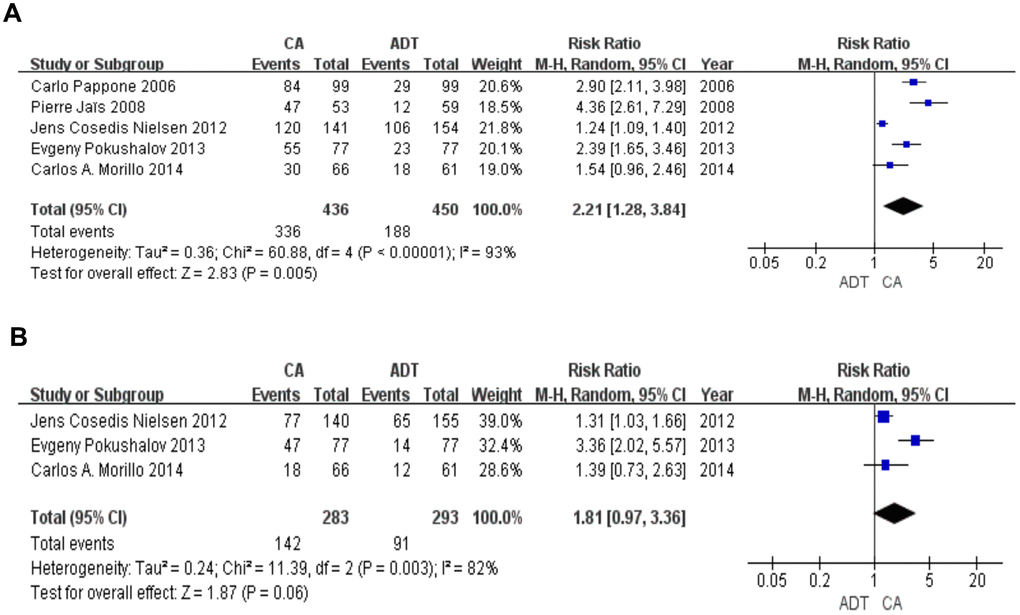
Figure 3. Forest plot of the AF-free rate in the long term. The AF-free rate was significantly higher in the CA group in 12 months (A). There was no statistical difference between the two groups in 24 months (B).
QOL
At the 3-month follow-up, QOL analysis was performed in 2 studies using the SF-36 General Health score. A total of 143 and 98 patients underwent CA and ADT, respectively, were included. In the mental component and physical component, the CA group scored significantly higher than the ADT group (RR 6.14; 95% CI 4.65-7.63; P < 0.001 and RR 5.37; 95% CI 4.01-6.73; P < 0.001, respectively). Symptom frequency scores were lower in the CA group (RR -8.7; 95% CI -14.37- -3.03; P = 0.003). There was no statistical difference in symptom severity evaluation scores between the groups (RR 8.83; 95% CI -26.84-44.50; P = 0.63). At the 12-months follow-up, QOL analysis was conducted in 2 studies using the SF-36 General Health score. A total of 202 and 205 patients underwent CA and ADT treatment. In terms of the mental component (RR 2.41; 95% CI 0.89-3.93; P = 0.002) and physical component (RR 3.32; 95% CI 1.81-4.83; P<0.001), the CA group scored higher than the ADT group.
Discussion
In this study, we found that the CA group had significantly higher AF-free rates in the early phase (6-12 months) than the ADT group. AF-free rates were also higher in the CA group than in the ADT group at the 24-month follow-up, though this difference was not significant. RCTs with longer follow-up durations of at least 2 years are recommended to verify the long-term prognosis of PAF.
In the CA group, QOL scores were higher than those in the ADT group after 3 months and 12 months of follow-up. These results suggest that in patients with PAF, primary CA can lead to better AF-free rates and QOL. Notably, it was recommended that after first-line CA failure, continuing second-line CA but not ADT resulted in higher AF-free rates. RCTs with long follow-up durations are needed to evaluate the long-term curative effect and side effects. Further studies are recommended to provide information on the predictors of the long-term prognosis of PAF. The most promising benefit reported by CA was the improvement in AF symptoms. In the early period of treatment at 3, 6, 9, and 12 months, CA reduced AF recurrence, improved the QOL, and shortened hospitalization time [1, 12]. Moreover, for some rare but important side effects, such as shock or bleeding, results were unstable, possibly due to the small sample size and short follow-up duration.
Our meta-analysis revealed that at 24 months, there was no statistically significant difference between the two treatments; therefore, evidence on the long-term benefits of CA and ADT in AF patients was limited. Most studies were not of sufficient duration (at least 2 years) to observe the long-term efficacy [2, 8–10], which is a problem that needs to be addressed in future RCTs. Moreover, the drug efficacy-cost ratio can be useful for the long-term use of ADT and short-term use of CA [13–15]. 14% of patients without recurrence of AF required second-line treatment after the 2-year follow-up, while 50% of patients relapsed in the second year after treatment with a single method [7, 13, 16]. A study [11] revealed that there was no statistically significant difference in the cumulative burden of PAF over the 2-year follow up; therefore, they recommended ADT but not CA in the early phase, which conformed to guidelines. Moreover, 36% of patients who used ADT as the first-line treatment would require second treatment with CA in the first year. A study [10] reported that ADT can lower the mortality rate and reduce side effects in the long-term. In the 12-month follow-up, 87% of patients who underwent CA were AF-free, while only 37% of those who underwent ADT were AF-free. Therefore, CA was 2.5 times more effective than ADT in controlling AF recurrence. In terms of cardiac structure remodeling, ADT had no effect compared to CA. However, death [17–19] was a risk during the entire CA procedure. Although the operational risk of CA was reduced, the reduction in mortality and stroke was rarely reported. In addition, the adverse effects of ADT, such as thyroid dysfunction, caused 23% of patients to discontinue treatment, in addition to the accumulation of more serious side effects over the long term [12, 17, 20, 21]. Although CA was superior to ADT in the first year, the long-term efficacy remains to be evaluated, which is key problem in all current RCT studies [2, 8–10].
The standard sequential therapy of CA or ADT is controversial. A study [9] included PAF patients who had failed first-line ADT. They found that CA improved symptoms, QOL, and exercise tolerance compared with ADT. They also revealed that only 23% of patients who underwent ADT showed improvement in AF symptoms even after amiodarone use during first-line ADT. The study was deficient in its small sample size, short follow-up time, and the safety of discontinuation of antiplatelet drugs in CA treatment remained to be explored. In Wilber’s research [8], CA was used after failure of first-line ADT in patients with AF symptoms. AF-free survival and control of QOL were higher after CA than after ADT. Importantly, if the response to ADT was poor in the early phase, amiodarone could only achieve 9% to 23% efficacy. The relative safety was also higher after CA, with only 6% of patients with PAF who underwent CA reporting major adverse events, including thromboembolic events, atrioesophageal fistula, cardiac perforation, phrenic nerve palsy, and death [4, 13, 22]. In the study by Pokushalov [7], after failure of first-line CA, 23% of patients who received second-line ADT progressed to persistent AF, compared with only 4% of those who receive second-line CA. After long-term observation, ADT was recommended, despite no improvement in the AF-free rate. Notably, the time of follow-up and the instruments used to evaluate AF influenced outcomes. After the 3-year follow-up, the AF-free rate in the CA group (58%) was significantly higher than that in the ADT group (12%). First-line CA was not recommended, which applied only after ADT treatment failure. Furthermore, after CA failure, secondary CA was more effective than ADT. However, partial studies included in the study did not have enough age data in detail to distinguish the elderly patients, although most of patients' age were older than 60 years old.
In conclusion, for elderly patients with PAF who underwent CA, a higher AF-free rate was obtained in the early stage. However, after 24 months, the difference in the AF-free rate was not statistically significant. Our meta-analysis revealed that after first-line CA or ADT failure, repeat CA but not ADT can result in a higher AF-free rate. RCTs are needed to evaluate the long-term curative effect and side effects. Furthermore, studies should be designed to discover new predictors for the prognosis of PAF following CA or ADT.
Materials and Methods
Search strategy
This meta-analysis examined the short- and long-term efficacy and safety of CA and ADT in terms of AF-free rates and QOL scores at 3-24 months. Search terms included “paroxysmal atrial fibrillation”, “catheter ablation”, “antiarrhythmic drug treatment” and "elderly patients" to collect all relevant randomized controlled trials (RCTs) published from January 2005 to June 2020 in the Cochrane Library, PubMed, and EMBASE.
Selection criteria and study selection
The inclusion criteria were as follows: clinical trials of PAF in which patients underwent CA and ADT, AF-free survival, and follow-up duration of more than 3 months, elderly patients (≥ 65 years old). The exclusion criteria were persistent AF, non-RCTs, no CA and ADT, no age data and no AF-free survival data. Data extraction was performed by two reviewers who independently checked for the quality and accuracy of the data. This involved identifying the disease as PAF, the CA and ADT groups, and the type of study; assessing study quality and clinical research data, the first recurrence of atrial tachyarrhythmia-free rates in 3, 6, 9, 12, and 24 months; In case of unclear or inconsistent factors, assessment and analysis were done by a third reviewer.
Data extraction and quality assessment
Using the AF-free survival data curve of 3 to 24 months, the AF-free survival rate was extracted at 3, 6, 9, 12 and 24 months. The physical component summary, mental component summary, symptom frequency, and symptom severity data in the Short Form (SF-36) General Health score were also extracted. The research used the PRISMA Checklist and Cochrane Reviewers’ Handbook to help improve reporting quality.
Statistical analysis
Review Manager software (version 5.2; Cochrane Collaboration, Oxford, UK) was used for meta-analysis. Heterogeneity was assessed by Cochrane χ2 statistic and I2 statistic. Low (I2 ≤ 25%), moderate (I2 > 25% and < 75%), or high (I2 ≥ 75%) heterogeneity was selected by a random effects model or fixed effects model. Efficacy results are presented in terms of risk ratio for AF-free survival rate and QOL score. All studies were assessed for publication bias using a funnel plot and Egger's test [23]. Two-tailed P values < 0.05 were considered statistically significant.
Abbreviations
ADT: antiarrhythmic drug therapy; CA: catheter ablation; PAF: paroxysmal atrial fibrillation; SF-36: short form health score-36; RR: risk ratio; CI: confidence interval; QOL: quality of life; RCT: randomized controlled trial.
Author Contributions
Yinan Sun and Lu Wang designed the study; Lu Wang managed the study; Yinan Sun and Lu Wang extracted the data; Yinan Sun performed the analyses; Yinan Sun and Lu Wang interpreted the evidence and wrote the manuscript; Lu Wang and Xiaoyun Yang revised the article. All authors agreed to be accountable for the work.
Acknowledgments
We thank all members of our study team for their hard work.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study was supported by the Tongji Hospital Fund (No. 2019YJJA14).
References
- 1. Packer DL, Mark DB, Robb RA, Monahan KH, Bahnson TD, Poole JE, Noseworthy PA, Rosenberg YD, Jeffries N, Mitchell LB, Flaker GC, Pokushalov E, Romanov A, et al, and CABANA Investigators. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019; 321:1261–74. https://doi.org/10.1001/jama.2019.0693 [PubMed]
- 2. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005; 293:2634–40. https://doi.org/10.1001/jama.293.21.2634 [PubMed]
- 3. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD, and Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002; 347:1825–33. https://doi.org/10.1056/NEJMoa021328 [PubMed]
- 4. Wang M, Cai S, Sun L, Zhao Q, Feng W. Safety and efficacy of early radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation complicated with amiodarone-induced thyrotoxicosis. Cardiol J. 2016; 23:416–21. https://doi.org/10.5603/CJ.a2016.0029 [PubMed]
- 5. Morillo CA, Verma A, Connolly SJ, Kuck KH, Nair GM, Champagne J, Sterns LD, Beresh H, Healey JS, Natale A, and RAAFT-2 Investigators. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a randomized trial. JAMA. 2014; 311:692–700. https://doi.org/10.1001/jama.2014.467 [PubMed]
- 6. Stabile G, Bertaglia E, Senatore G, De Simone A, Zoppo F, Donnici G, Turco P, Pascotto P, Fazzari M, Vitale DF. Catheter ablation treatment in patients with drug-refractory atrial fibrillation: a prospective, multi-centre, randomized, controlled study (catheter ablation for the cure of atrial fibrillation study). Eur Heart J. 2006; 27:216–21. https://doi.org/10.1093/eurheartj/ehi583 [PubMed]
- 7. Pokushalov E, Romanov A, De Melis M, Artyomenko S, Baranova V, Losik D, Bairamova S, Karaskov A, Mittal S, Steinberg JS. Progression of atrial fibrillation after a failed initial ablation procedure in patients with paroxysmal atrial fibrillation: a randomized comparison of drug therapy versus reablation. Circ Arrhythm Electrophysiol. 2013; 6:754–60. https://doi.org/10.1161/CIRCEP.113.000495 [PubMed]
- 8. Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V, Augello G, Reynolds MR, et al, and ThermoCool AF Trial Investigators. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010; 303:333–40. https://doi.org/10.1001/jama.2009.2029 [PubMed]
- 9. Jaïs P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clémenty J, Haïssaguerre M. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation. 2008; 118:2498–505. https://doi.org/10.1161/CIRCULATIONAHA.108.772582 [PubMed]
- 10. Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, et al. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF study. J Am Coll Cardiol. 2006; 48:2340–47. https://doi.org/10.1016/j.jacc.2006.08.037 [PubMed]
- 11. Cosedis Nielsen J, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Kongstad O, Pehrson S, Englund A, Hartikainen J, Mortensen LS, Hansen PS. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med. 2012; 367:1587–95. https://doi.org/10.1056/NEJMoa1113566 [PubMed]
- 12. Blomström-Lundqvist C, Gizurarson S, Schwieler J, Jensen SM, Bergfeldt L, Kennebäck G, Rubulis A, Malmborg H, Raatikainen P, Lönnerholm S, Höglund N, Mörtsell D. Effect of catheter ablation vs antiarrhythmic medication on quality of life in patients with atrial fibrillation: the CAPTAF randomized clinical trial. JAMA. 2019; 321:1059–68. https://doi.org/10.1001/jama.2019.0335 [PubMed]
- 13. De Potter T, Van Herendael H, Balasubramaniam R, Wright M, Agarwal SC, Sanders P, Khaykin Y, Latcu DG, Maury P, Pani A, Hayes J, Kalman J, Nery P, Duncan E. Safety and long-term effectiveness of paroxysmal atrial fibrillation ablation with a contact force-sensing catheter: real-world experience from a prospective, multicentre observational cohort registry. Europace. 2018; 20:f410–18. https://doi.org/10.1093/europace/eux290 [PubMed]
- 14. Takigawa M, Takahashi A, Kuwahara T, Okubo K, Takahashi Y, Watari Y, Nakashima E, Nakajima J, Yamao K, Takagi K, Tanaka Y, Fujino T, Kimura S, et al. Long-term outcome after catheter ablation of paroxysmal atrial fibrillation: impact of different atrial fibrillation foci. Int J Cardiol. 2017; 227:407–12. https://doi.org/10.1016/j.ijcard.2016.11.028 [PubMed]
- 15. Kumar S, Michaud GF. Catheter ablation for paroxysmal atrial fibrillation: time to focus more on trigger ablation? Circ Arrhythm Electrophysiol. 2016; 9:e004129. https://doi.org/10.1161/CIRCEP.116.004129 [PubMed]
- 16. Kettering K, Yim DH, Benz A, Gramley F. Catheter ablation of paroxysmal atrial fibrillation: circumferential pulmonary vein ablation: success rates with and without exclusion of areas adjacent to the esophagus. Clin Res Cardiol. 2017; 106:743–51. https://doi.org/10.1007/s00392-017-1118-x [PubMed]
- 17. Buist TJ, Adiyaman A, Beukema RJ, Smit JJ, Delnoy PP, Hemels ME, Sie HT, Ramdat Misier AR, Elvan A. Quality of life after catheter and minimally invasive surgical ablation of paroxysmal and early persistent atrial fibrillation: results from the SCALAF trial. Clin Res Cardiol. 2020; 109:215–24. https://doi.org/10.1007/s00392-019-01504-z [PubMed]
- 18. Shimamoto K, Miura F, Shimatani Y, Nishioka K, Inoue I. Pulmonary vein volume predicts the outcome of radiofrequency catheter ablation of paroxysmal atrial fibrillation. PLoS One. 2018; 13:e0201199. https://doi.org/10.1371/journal.pone.0201199 [PubMed]
- 19. Grieco D, Palamà Z, Borrelli A, De Ruvo E, Sciarra L, Scarà A, Goanta E, Calabrese V, Pozzilli P, Di Sciascio G, Calò L. Diabetes mellitus and atrial remodelling in patients with paroxysmal atrial fibrillation: role of electroanatomical mapping and catheter ablation. Diab Vasc Dis Res. 2018; 15:185–95. https://doi.org/10.1177/1479164117752492 [PubMed]
- 20. Wang Y, Xu Y, Ling Z, Chen W, Su L, Du H, Xiao P, Liu Z, Yin Y. Radiofrequency catheter ablation for paroxysmal atrial fibrillation: outcomes during a 3-year follow-up period. J Int Med Res. 2019; 47:1636–48. https://doi.org/10.1177/0300060519828522 [PubMed]
- 21. Chinitz LA, Melby DP, Marchlinski FE, Delaughter C, Fishel RS, Monir G, Patel AM, Gibson DN, Athill CA, Ming Boo L, Stagg R, Natale A. Safety and efficiency of porous-tip contact-force catheter for drug-refractory symptomatic paroxysmal atrial fibrillation ablation: results from the SMART SF trial. Europace. 2018; 20:f392–f400. https://doi.org/10.1093/europace/eux264 [PubMed]
- 22. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. 2005; 111:1100–05. https://doi.org/10.1161/01.CIR.0000157153.30978.67 [PubMed]
- 23. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34. https://doi.org/10.1136/bmj.315.7109.629 [PubMed]