



Introduction
Digestive system tumor is a heterogeneous group of complex diseases affecting different organs, and the vast majority of it is malignancies [1, 2]. Digestive system tumor is the common cause of cancer deaths [3, 4]. According to World Health Organization (WHO) classification of tumors, digestive system tumors include esophageal cancer, gastric cancer, small intestine cancer, hepatocellular carcinoma, gallbladder cancer, biliary tract cancer, pancreatic cancer and colorectal cancer. Although some studies have reported drugs or components with therapeutic potential for gastrointestinal cancer, such as allicin and curcumin [2, 5]. However, due to the challenge for clinical translation of current studies and the strong aggressiveness and metastatic ability of digestive system tumors, early diagnosis and surgery are crucial for reducing the mortality and prolonging the survival time of patients with digestive system tumors [5–7]. Therefore, the identification of new potential diagnostic and prognostic tumor biomarker is helpful for the early prevention and treatment of digestive system tumors.
Non-coding RNAs including long non-coding RNAs (lncRNAs), circular RNAs (circRNAs), and microRNAs (miRNAs) are responsible for the regulation of many cells signaling pathways [8]. Moreover, there are several studies suggesting that circRNAs, lncRNAs and miRNAs are epigenetic regulators with prognostic and therapeutic effects in digestive system tumors [9–11]. LncRNAs are defined as nonprotein-coding RNAs with lengths exceeding 200 nucleotides [12, 13]. Recent studies on formation and functional mechanisms of lncRNAs have shown that lncRNAs play a key role in regulating chromatin dynamics, gene expression and maintaining biological processes [14–16]. More and more evidences indicate that the dysregulation of lncRNA expression is closely related to the development of several human diseases, such as diabetes, sepsis, stroke, autoimmune diseases and cancer [8, 17–21]. Studies on tumors have shown that lncRNAs are involved in the pathogenesis of digestive system tumors through the regulation of autophagy [1]. Therefore, lncRNAs can be used as biomarkers and therapeutic targets for cancers.
Highly up-regulated in liver cancer (HULC) is located on the chromosome 6p24.3 and approximately 500nt in length [22]. In 2007, it was first reported to be significantly up-regulated in hepatocellular carcinoma, then, increasing studies have verified that it is dysregulated in various tumors such as pancreatic cancer, breast cancer and bladder cancer [23–26]. Recently, studies have shown that HULC is overexpressed in digestive system tumors to promote tumor development [24, 27, 28]. Therefore, we believe that high expression of lncRNA HULC in patients with digestive system tumors tend to have a poor prognosis.
Meta-analysis is an analytical method that could aggregate different studies to address deficiencies caused by small sample sizes and certain human errors. Although there have been studies evaluating the prognostic value of HULC in digestive system tumors through subgroup analysis [29]. In recent years, there have been several newly-published in this field. We conducted an updated and comprehensive meta-analysis of all published studies to provide more reliable evidence to evaluate the association between HULC and the prognosis and clinicopathological features in patients with digestive system tumors.
Materials and Methods
Literature retrieval strategies and selection criteria
Articles for inclusion in this meta-analysis were searched in PubMed, Web of Science and Embase, up to February 2021. The keywords used in our literature search contained (“HULC” or “lncRNA HULC”) and (“colorectal” or “gastric” or “esophageal” or “small intestine” or “hepatocellular carcinoma” or “gallbladder” or “biliary tract” or “pancreatic” or “liver” or “colon” or “rectal”). The inclusion and exclusion of the literatures were independently identified by two researchers.
Inclusion and exclusion criteria
Inclusion criteria
(1) The expression of lncRNA HULC in tumor tissues, serum and plasma of patients was measured; (2) According to the expression levels of HULC, patients were divided into high expression group and low expression group; (3) All patients suffered from digestive system tumors; (4) Studies were to investigate the role of HULC in digestive system tumors; (5) Survival information of patients, such as overall survival (OS), disease-free survival rate (DFS), progression-free survival rate (PFS), was provided; (6) The odds ratio (OR) or hazard ratio (HR), and the corresponding 95% confidence interval (CI) could be calculated; (6) If there were repeated studies, the latest literature was included.
Exclusion criteria
(1) The study subjects were non-human; (2) Case reports, comments, reviews, letters and conference reports; (3) Non-English research; (4) Studies with insufficient clinical data; (5) Duplicate data or research.
Quality assessment and data extraction
The quality assessment and data extraction of the eligible studies were conducted by two researchers independently. A third researcher was used to resolve disagreements in eligibility, data extraction, or quality assessment. The Cochrane Non-Randomized Studies Methods Group recommended the use of the Newcastle-Ottawa Scale (NOS) to assess the quality of eligible studies (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) [30]. Publications with scores ≥ 6 were included in this meta-analysis.
The following data were extracted: (1) The first author and year of publication; (2) Tumor types and detection methods; (3) demographic characteristics, including sample size, region, age, gender and follow-up time; (4) clinical characteristics of patients, including number of tumors, TNM stage, differentiation, lymph node metastasis (LNM) and distant metastasis (DM); (5) HR with 95% CI for OS, DFS and PFS. If only Kaplan-Meier survival curves were available, the Engauge Digitizer v11.1 software could be used to obtain the available data to calculate the HR and the corresponding 95% CI [31].
Data mining from the TCGA and GTEx data set
RNA-seq data and OS data for HULC in The Cancer Genome Atlas (TCGA) and The Genotype-Tissue Expression (GTEx) were extracted from GEPIA2 (http://gepia2.cancer-pku.cn/#index) [32]. The median cutoff was chosen to divide the patients into two groups of high and low, and plot a Kaplan–Meier curve. p < 0.05 was considered to be of prognostic value.
Statistical analysis
Stata SE14.0 software was used for statistical analysis in this meta-analysis. Heterogeneity among all included studies was assessed by I2 statistics and Q test. I2 > 50%, P < 0.05 indicated that the heterogeneity was statistically significant. Random-effects model should be applied to improve statistical stability. I2 < 50%, P > 0.05 indicated no statistical significance in heterogeneity, so the fixed-effects model was used. Data extracted from Kaplan-Meier survival curves and univariate analysis data were used for pooled analysis. The relationship between the expression level of HULC and the prognosis of patients with digestive system tumors was determined by HR and the corresponding 95% CI. Also, the relationship between clinicopathological characteristics and HULC was assessed by OR and 95% CI. We used subgroup analysis to analyze the sources of heterogeneity. Sensitivity analysis was used to assess the robustness of the meta-analysis. The Egger’s test was used to evaluate the potential publication bias. HR > 1 indicated a poor prognosis. P value was calculated by two-tailed test, P < 0.05 suggested statistically significant difference.
Results
Characteristics of eligible publications
Figure 1 showed the process of literature selection. After excluding duplicate studies, a total of 138 studies were obtained from PubMed, Web of Science and Embase. 83 research articles were excluded based on their titles and abstracts. After carefully reviewing the contents of the remaining 55 studies, a total of 14 articles met the inclusion criteria of this meta-analysis [24, 28, 33–44]. These studies were published between 2014 and 2020. There were 6 different kinds of digestive system tumors, including pancreatic cancer (PC, n=2), hepatocellular carcinoma (HCC, n=5), gastric cancer (GC, n=3) and colorectal cancer (CRC, n =4), in which CRC included colon cancer (CC, n=1) and colon adenocarcinoma (CA, n=1).
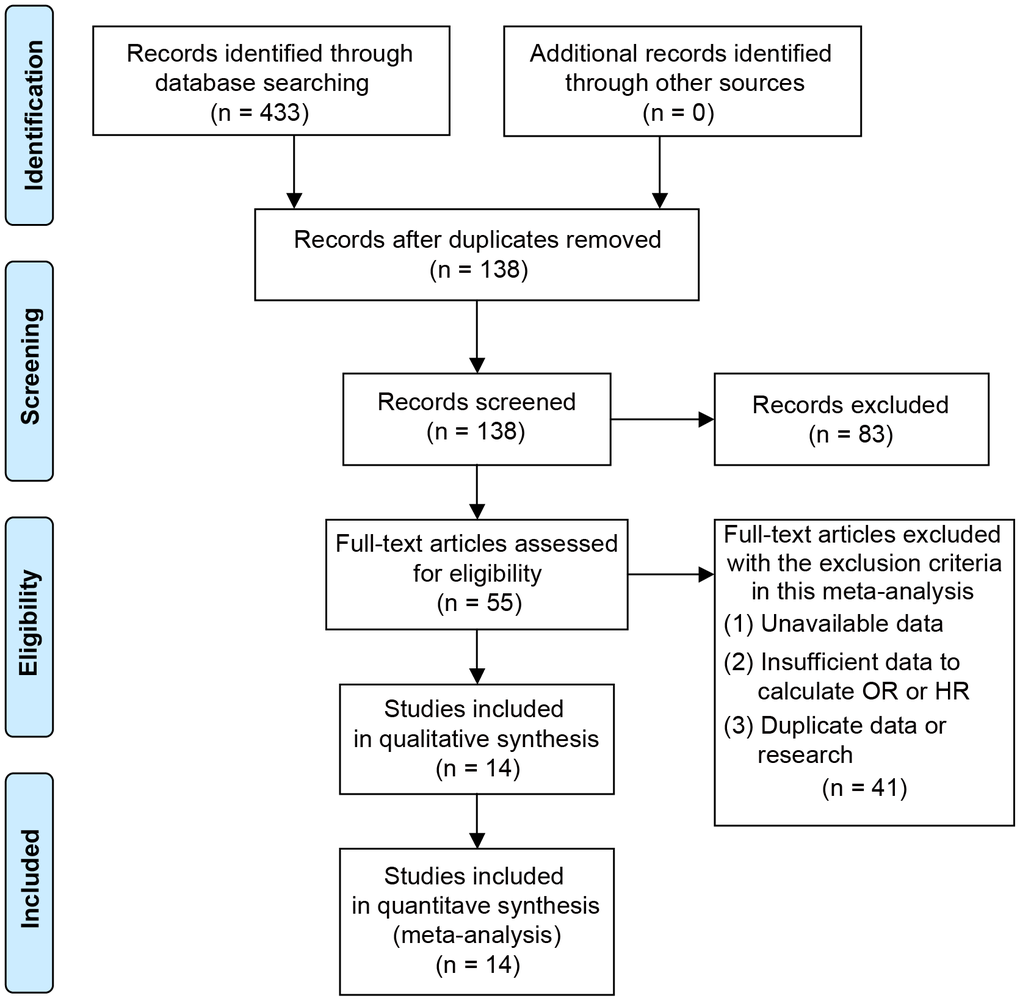
Figure 1. Flowchart for the process of search, selection and exclusion of studies.
Table 1 summarized the main characteristics of all eligible studies in this meta-analysis. Four different regions were included in these 14 studies, China (n=11), Japan (n=1), South Korea (n=1) and Germany (n=1). A total of 1312 patients were included in this study. The sample size was a minimum of 30 and a maximum of 304. There were 5 studies with a sample size exceeding 100. In 13 studies, the HULC expression levels were determined through quantitative real-time polymerase chain reaction (qRT-PCR). In 1 study, beadchip was used to detect the HULC expression. Nine studies reported the relationship between the expression level of HULC and the clinicopathological characteristics of patients, such as age, gender, tumor size, TNM stage and tumor differentiation. The NOS scores of all included studies were ≥ 6.
Table 1. Basic characteristics of all qualified studies.
| Study | Region | Cancer | Sample size | Gender | Specimen | Method | Survival analysis | Outcome | Cut-off | Follow-up (months) | NOS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| F | M | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peng et al. 2014 | China | PC | 304 | 136 | 168 | tissue | qRT-PCR | Multivariate/Univariable | OS | mean | 36 | 8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yang et al. 2015 | Korea | HCC | 240 | tissue | beadchip | Multivariate/Univariable | OS/DFS | median | 120 | 9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Li et al. 2015 | China | HCC | 66 | 13 | 53 | plasma | qRT-PCR | median | 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Li et al. 2016 | China | HCC | 38 | 9 | 29 | tissue | qRT-PCR | Kaplan-Meier curve | OS | mean | 60 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jin et al. 2016 | China | GC | 100 | 35 | 65 | serum | qRT-PCR | Kaplan-Meier curve | OS | median | 36 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yang et al. 2016 | China | CRC | 35 | tissue | qRT-PCR | Kaplan-Meier curve | OS | mean | 120 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Zhang et al. 2016 | China | GC | 42 | plasma | qRT-PCR | Kaplan-Meier curve | OS | mean | 60 | 8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sonohara et al. 2017 | Japan | HCC | 158 | 26 | 132 | tissue | qRT-PCR | Kaplan-Meier curve | OS/RFS | mean | 120 | 8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Zhang et al. 2018 | China | CA | 50 | 27 | 23 | tissue | qRT-PCR | median | 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dong et al. 2019 | China | CC | 67 | 28 | 39 | tissue | qRT-PCR | Kaplan-Meier curve | OS | mean | 60 | 7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oehme et al. 2019 | Germany | CRC | 52 | 19 | 33 | serum exosome | qRT-PCR | Kaplan-Meier curve | OS | median | 100 | 6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cao et al. 2019 | China | HCC | 30 | 21 | 9 | tissue, serum exosome | qRT-PCR | mean | 6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liu et al. 2020 | China | GC | 116 | 40 | 76 | tissue | qRT-PCR | median | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ou et al. 2020 | China | PC | 60 | 17 | 43 | serum | qRT-PCR | Multivariate/Univariable | OS | median | 60 | 9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PC, pancreatic cancer; HCC, hepatocellular carcinoma; GC, gastric cancer; CRC, colorectal cancer; CC, colon cancer; CA, colon adenocarcinoma; F, female; M, male; OS, overall survival; DFS, disease-free survival; RFS, recurrence-free survival. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The relationship between the expression of lncRNA HULC and OS
There were 10 studies, including 1050 patients with digestive system tumors, reported the correlation between HULC and OS. Due to the significant heterogeneity, a random-effects model was applied to calculate the pooled HR and the corresponding 95% CI (I2 = 88.5%, P < 0.05). The results indicated that the OS of patients with up-regulated HULC expression had a worse prognosis than that of those with low HULC expression (HR = 1.83, 95% CI: 1.01-3.30, P = 0.045) (Figure 2A).
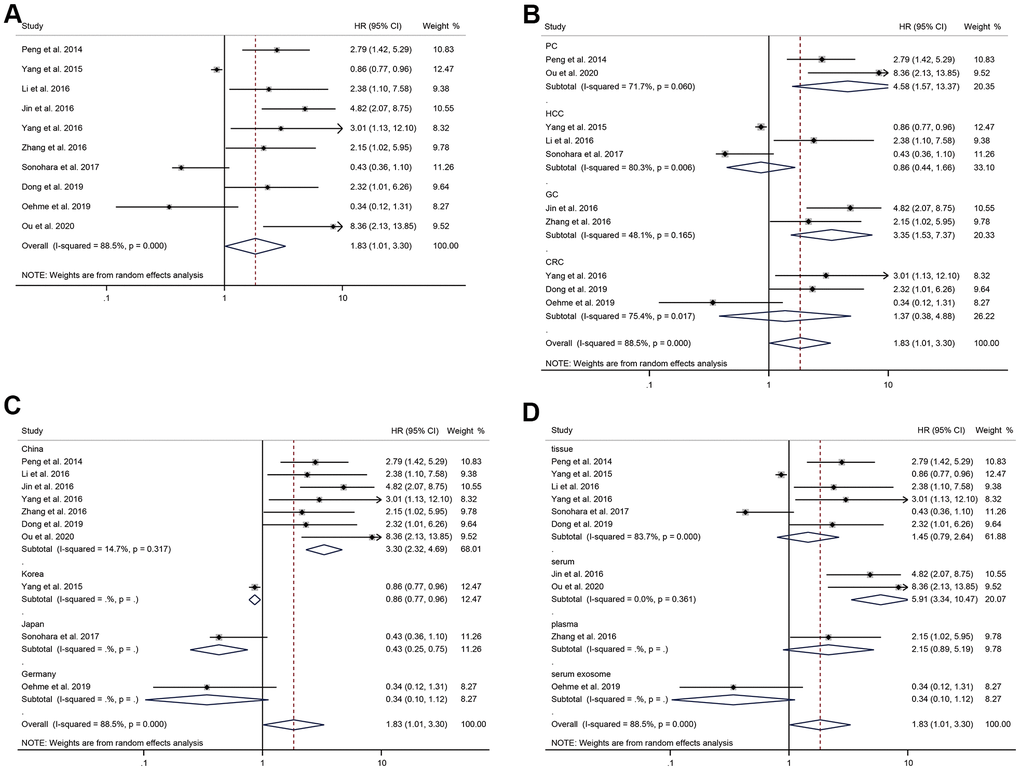
Figure 2. The correlation analysis between HULC expression level and OS. (A) Forest plot of the correlation between HULC expression level and OS in patients with digestive system tumors. (B) Subgroup analysis of HRs of OS according to the cancer type. (C) Subgroup analysis of HRs of OS according to the regions. (D) Subgroup analysis of HRs of OS according to the specimens.
In term of cancer type, high expression of HULC was significantly related to poor survival prognosis in PC (HR = 4.58, 95%CI: 1.57-13.37, P = 0.005) with significant heterogeneity (I2 = 71.7%, P = 0.060), and in GC (HR = 3.35, 95%CI: 1.53-7.37, P = 0.003) with no significant heterogeneity (I2 = 48.1%, P = 0.165) (Figure 2B). There was no significant correlation between HULC expression level and prognosis in HCC (HR = 0.86, 95%CI: 0.44-1.66, P = 0.65) with significant heterogeneity (I2 = 80.3%, P = 0.006), and in CRC (HR = 1.37, 95%CI: 0.38-4.88, P = 0.63) with significant heterogeneity (I2 = 75.4%, P = 0.017). According to subgroup analyses stratified by regions, the four geographic locations presented inconsistent results. In China, higher HULC expression level was related to poor prognosis (HR = 3.30, 95%CI: 2.32-4.69, P < 0.001) with no significant heterogeneity (I2 = 14.7%, P = 0.32). However, it was associated with favorable prognosis in Japan (HR = 0.43, 95%CI: 0.25-0.75, P = 0.003) and Korea (HR = 0.86, 95%CI: 0.77-0.96, P = 0.007). In Germany, the association between HULC expression level and prognosis of digestive system tumors was not statistically significant (HR =0.34, 95%CI: 0.10-1.12, P = 0.077) (Figure 2C). When the studies were stratified by specimens, we found that the result of serum was statistically significant (HR = 5.91, 95%CI: 3.34-10.47, P < 0.001) with significant heterogeneity (I2 = 0.0%, P = 0.361); nevertheless, the significant association was not found in tissue (HR = 1.45, 95%CI: 0.79-2.64, P = 0.23) with significant heterogeneity (I2 = 83.7%, P < 0.001), plasma (HR = 2.15, 95%CI: 0.89-5.19, P = 0.089) or serum exosomes (HR = 0.34, 95%CI: 0.10-1.12, P = 0.077) (Figure 2D). The above results suggested that cancer type and region were the sources of heterogeneity in this meta-analysis.
Sensitivity analysis observed whether the pooled results were affected by eliminating each study in turn. Figure 3 showed the results of sensitivity analysis, which suggested that the results were reliable.
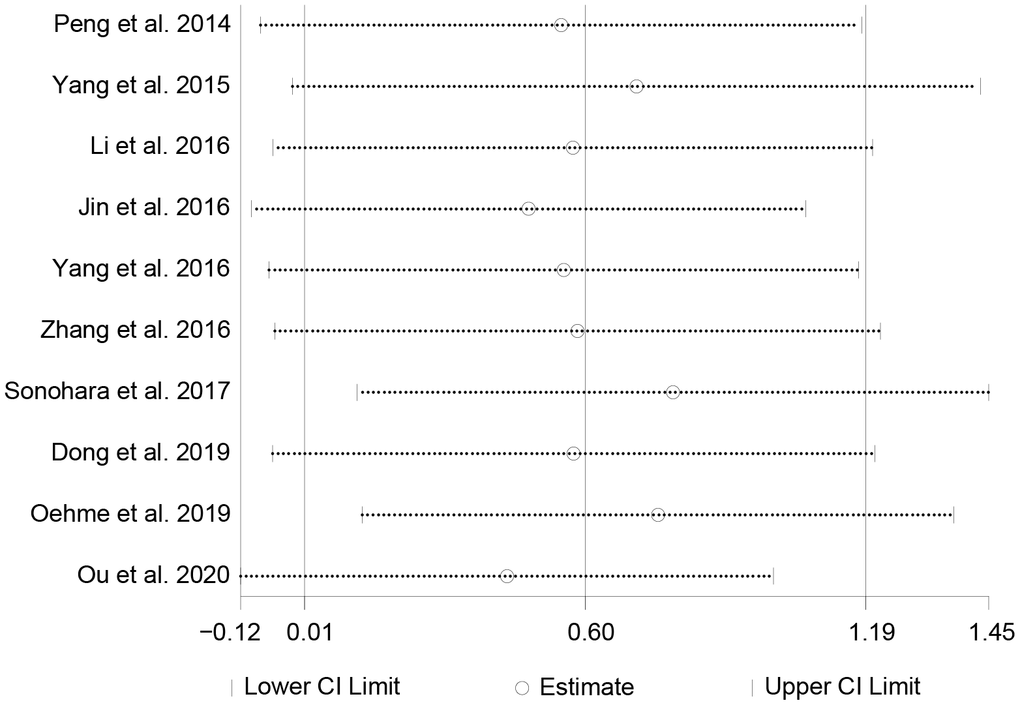
Figure 3. The sensitivity analysis on the correlation between HULC expression level and OS.
The relationship between the expression of HULC and tumor size, number, TNM stage, differentiation
There were 6 and 3 studies respectively reporting the tumor size and number of tumors in patients with digestive system tumors. The pooled results showed that the expression level of HULC was not correlated to tumor size (OR = 1.74, 95%CI: 0.68-4.48, P = 0.25) or number of tumors (OR = 0.71, 95%CI: 0.47-1.09, P = 0.11) (Figure 4A, 4B). A random-effects model was used to analyze the relationship between HULC expression and TNM stage (I2 = 63.5%, P = 0.008). The pooled OR was 2.51 (95%CI: 1.36-4.62, P = 0.003), suggesting a significant correlation between the expression of HULC and TNM stage (Figure 4C). Thus, overexpression of HULC could easily increase the risk of high-stage tumors. Eight of included studies reported the differentiation of tumors. Since there was no significant heterogeneity, we used a fixed-effects model (I2 = 0.0%, P = 0.488) to analyze the data of tumor differentiation. The results suggested that the increased expression of HULC was significantly related to the poor differentiation of the digestive system tumors (OR = 1.38, 95% CI: 1.02-1.87, P = 0.035) (Figure 4D).
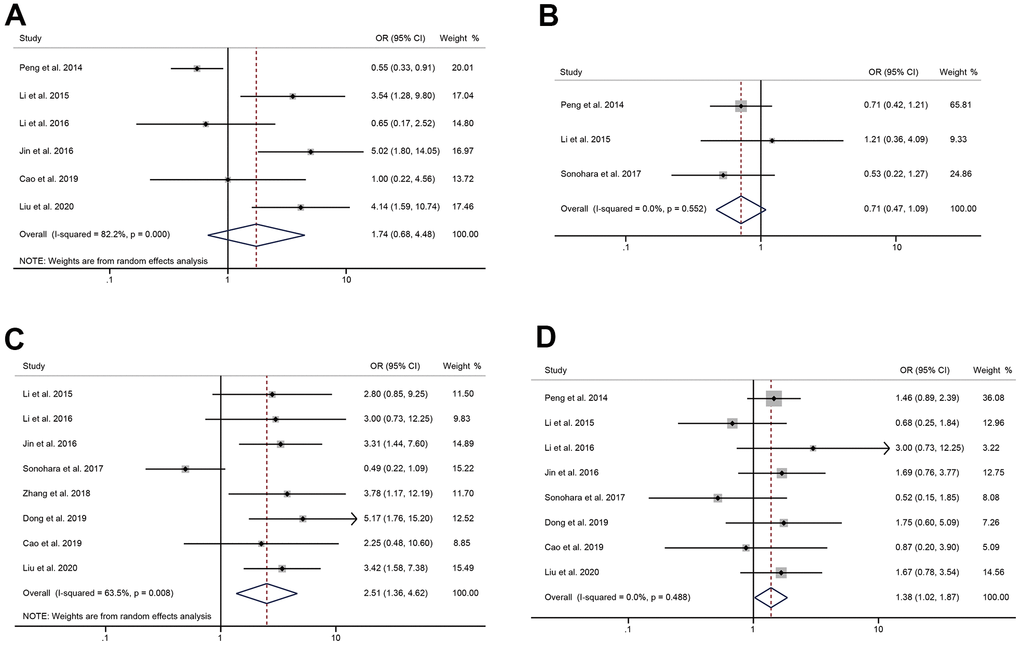
Figure 4. The correlation between HULC expression level and tumor characteristics. (A) The forest plot of ORs for the correlation between HULC expression and tumor size in patients with digestive system tumors; (B) The forest plot of ORs for the correlation between HULC expression and number of tumors in patients with digestive system tumors; (C) The forest plot of ORs for the correlation between HULC expression and TNM stage in patients with digestive system tumors; (D) The forest plot of ORs for the correlation between HULC expression and differentiation in patients with digestive system tumors.
The relationship between the expression of HULC and LNM, DM
A total of 6 qualified literatures reported the occurrence of LNM in patients with digestive system tumors. Since no significant heterogeneity was found, we adopted a fixed-effects model (I2 = 26.9%, P = 0.233). The pooled result indicated that cancer patients with high HULC expression had higher risk of LNM than those with low HULC expression (OR = 4.93, 95% CI: 3.47-6.99, P < 0.001) (Figure 5A). I2 = 73.1%, P = 0.011 suggested significant heterogeneity, so a random-effects model was used for the pooled analysis of DM. We found that high HULC expression was not significantly correlated with the DM of tumors (OR = 3.18, 95% CI: 0.69-14.57, P = 0.14) (Figure 5B).
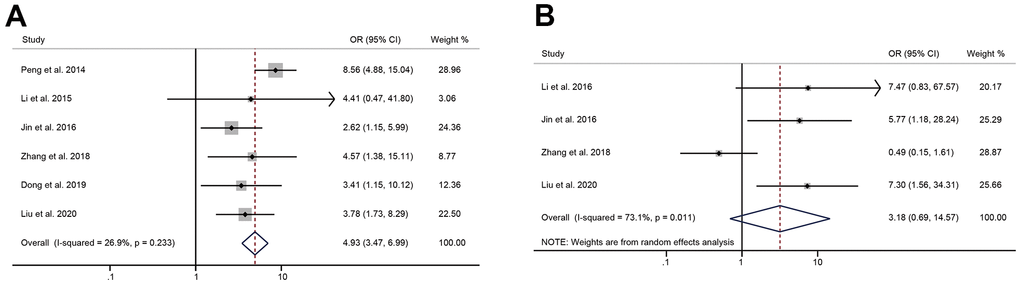
Figure 5. The correlation between HULC expression level and metastasis. (A) The forest plot of ORs for the correlation between HULC expression and lymphatic node metastasis in patients with digestive system tumors; (B) The forest plot of ORs for the correlation between HULC expression and distant metastasis in patients with digestive system tumors.
The relationship between the expression of HULC and patients’ age, gender
In 5 studies (1 on pancreatic cancer, 2 on hepatocellular carcinoma, and 2 on gastric cancer), the high expression of HULC was not significantly related to the age of patients (OR = 0.78, 95% CI: 0.55-1.10, P = 0.16) (Figure 6A). The gender of patients was mentioned in 9 qualified studies. Since the heterogeneity was not significant, we used a fixed-effects model (I2 = 0.0%, P = 0.867). The pooled OR was 1.01 (95% CI: 0.75-1.35, P = 0.95), indicating that the overexpression of HULC was not significantly associated with the gender of patients (Figure 6B).
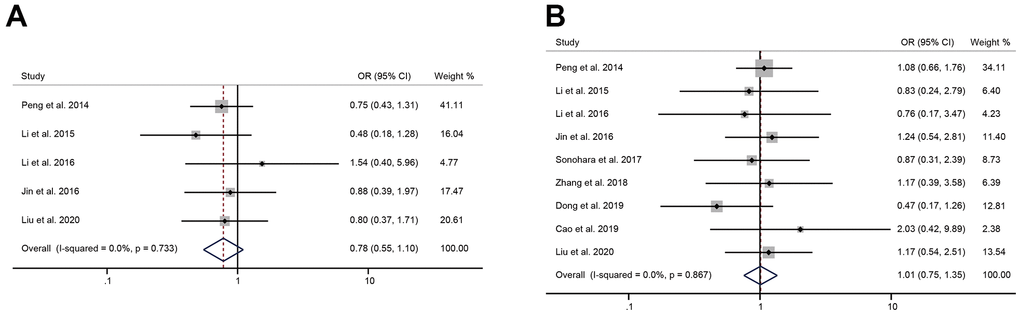
Figure 6. The correlation between HULC expression level and the patient’s age, gender. (A) The forest plot of ORs for the correlation between HULC expression and age in patients with digestive system tumors; (B) The forest plot of ORs for the correlation between HULC expression and gender in patients with digestive system tumors.
Assessment of publication bias
To assess the publication bias in the current study, we performed an Egger’s linear regression test. The Egger’s test and linear regression plot was shown in Figure 7. Moreover, there was no statistically significant publication bias in OS (P = 0.059), age (P = 0.61), gender (P = 0.72), tumor size (P = 0.25), TNM stage (P = 0.25), differentiation (P = 0.51), number of tumors (P = 0.77), LNM (P = 0.33) and DM (P = 0.19).
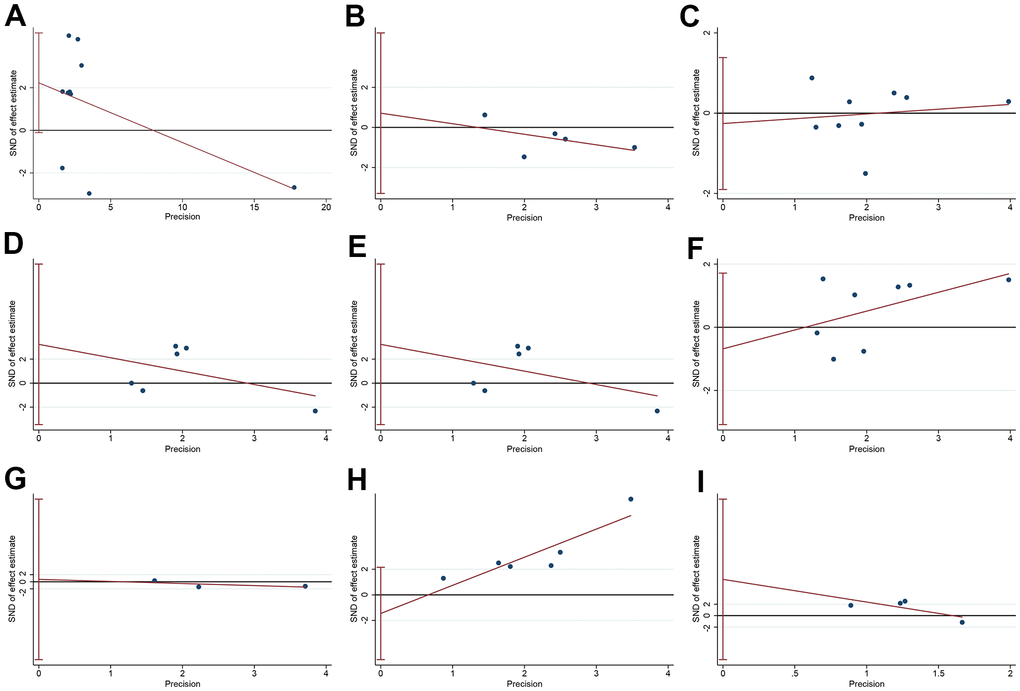
Figure 7. The publication bias of HULC-related research. (A) The Egger’s test and linear regression plot for the publication bias of OS; (B) The Egger’s test and linear regression plot for the publication bias of age; (C) The Egger’s test and linear regression plot for the publication bias of gender; (D) The Egger’s test and linear regression plot for the publication bias of tumor size; (E) The Egger’s test and linear regression plot for the publication bias of TNM stage; (F) The Egger’s test and linear regression plot for the publication bias of differentiation; (G) The Egger’s test and linear regression plot for the publication bias of number of tumors; (H) The Egger’s test and linear regression plot for the publication bias of lymphatic node metastasis; (I) The Egger’s test and linear regression plot for the publication bias of distant metastasis.
Results in TCGA and GTEx data set
The prognostic value of HULC was further verified by retrieving the clinical data from TCGA and GTEX data set. We finally retrieved 5 GI cancers, including cholangiocarcinoma (CHOL), colon adenocarcinoma (COAD), esophageal carcinoma (ESCA), liver hepatocellular carcinoma (LIHC) and rectum adenocarcinoma (READ) (Figure 8). Unexpectedly, the high expression of HULC was negatively correlated with OS time in CHOL, while HULC expression was not significantly correlated with OS time in other cancers. Moreover, CHOL was a kind of GI cancers not included in our meta-analysis.
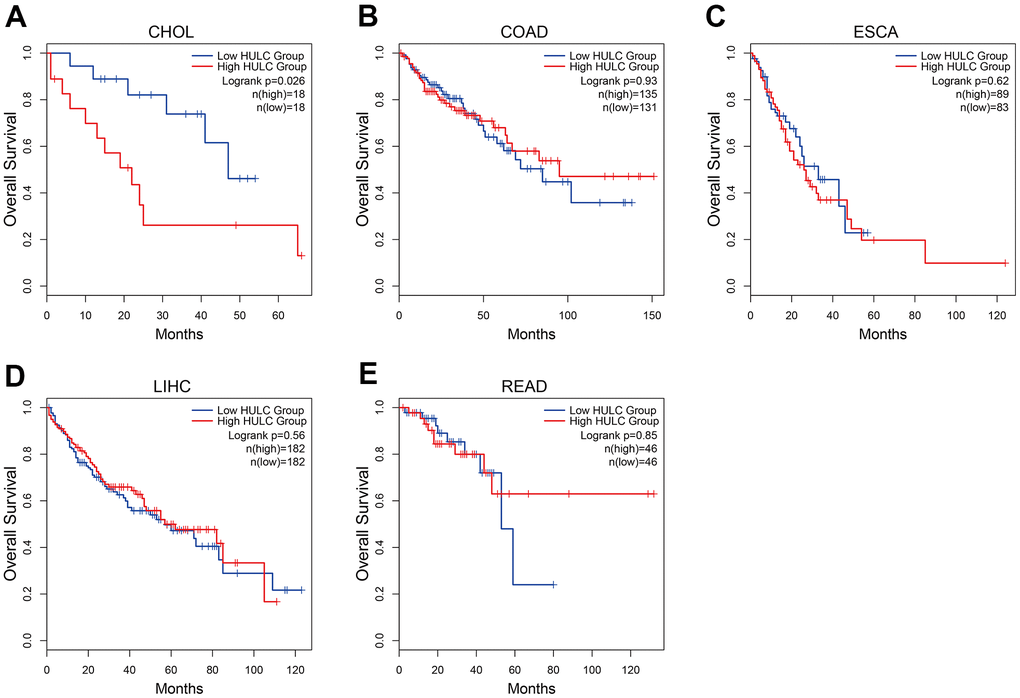
Figure 8. Kaplan–Meier curves showing the prognostic value of HULC in TCGA and GTEx data set. (A) The Kaplan–Meier curve of CHOL; (B) The Kaplan–Meier curve of COAD; (C) The Kaplan–Meier curve of ESCA; (D) The Kaplan–Meier curve of LIHC; (E) The Kaplan–Meier curve of READ. CHOL: cholangiocarcinoma; COAD: colon adenocarcinoma; ESCA: esophageal carcinoma; LIHC: liver hepatocellular carcinoma; READ: rectum adenocarcinoma.
Discussion
Because lncRNA can regulate gene expression through epigenetic modification, transcription and post-transcriptional translation, lncRNAs have key functions in various diseases [45]. It has been found that lncRNAs are critical for angiogenesis and neuroprotection. Therefore, lncRNAs were considered as therapeutic, diagnostic and prognostic tools in cerebrovascular diseases, including stroke [17]. Recently, lncRNA has been proved to be a key factor in tumorigenesis, and it can involve in cancer by regulating tumor cell proliferation, migration and DNA stability [46]. In gynecological cancer, lncRNA is considered as a biomarker or therapeutic target [20]. LncRNAs such as MALAT1, XIST and NORAD have been proven to be biomarkers for human tumor prognosis [47–49]. Also, some studies have shown that HULC expression is dysregulated in digestive system tumors [37, 39, 50]. Therefore, we believe that HULC can be used as a new potential diagnostic and prognostic tumor biomarker for digestive system tumors.
We conducted this meta-analysis to verify the correlation between HULC expression level and survival prognosis of patients with digestive system tumors. A total of 14 studies involving 1312 patients were included. The pooled results suggested that high expression level of HULC had a significant correlation with poor survival prognosis in patients with digestive system tumors. Sensitivity analysis showed that our analysis was robust. We found that high expression level of HULC could increase the risk of high TNM stage, poor differentiation, and LNM. HULC expression level was not associated with age, gender, tumor size, number of tumors, or DM. The results of subgroup analysis suggested that cancer type and region were the sources of heterogeneity in this meta-analysis. There was no significant publication bias among all included studies. These results suggested that HULC may be a candidate oncogene for digestive system tumors. The up-regulated of HULC could be used as a novel predictor of poor prognosis in patients with digestive system tumors.
Since most studies prefer to report positive results rather than negative results. We performed a further verification for prognostic value of HULC in patients with digestive system tumors. By analyzing TCGA and GTEX data set, we found unexpected results. The high expression of HULC was negatively correlated with OS time in CHOL, while HULC expression was not significantly correlated with OS time in other cancers. This finding deserves further investigation.
According to previous reports, HULC can exert oncogenic effect through different mechanisms. Many cancer researchers have made great efforts to explore the functional mechanism of lncRNA HULC on the occurrence and development of various cancers. YB-1 is a multifunctional protein that participates in cellular functions, such as transcription regulation, mRNA splicing and translation regulation [51, 52]. It has been reported that HULC can promote the phosphorylation of YB-1 protein to activate the translation of silent oncogenes, so as to promote the occurrence of hepatocellular carcinoma [53]. The “Warburg effect” refers to the reprogramming of glucose metabolism from oxidative phosphorylation to aerobic glycolysis, which is one of the hallmarks of tumor cells [54]. Wang et al. have found that HULC can enhance the binding of LDHA and PKM2 to FGFR1, resulting in increased phosphorylation of these two enzymes and consequently promoting glycolysis [55]. Non-coding RNAs (ncRNAs) can transfer information from their donor cells to recipient cells through exosomes to play a role in cell-to-cell communication [56]. Circulating extracellular vesicle-encapsulated HULC showed good predictive performance in distinguishing pancreatic ductal adenocarcinoma (PDAC) [57]. Takahashi et al. 2020 et al. reported that miR-622 encapsulated by exosomes can inhibit epithelial-mesenchymal transition (EMT) by targeting HULC to inhibit the invasion and migration of pancreatic ductal adenocarcinoma cells [58]. Autophagy is recognized an intracellular regulatory process [10]. There is evidence that autophagy plays an important role in both progression and suppression of digestive system tumors [1, 10]. Thus, HULC can not only increase the expression of P62 by reducing mature miR-15a, but also increase autophagy by increasing Sirt1-dependent LC3II to promote the development of hepatocellular carcinoma [59]. STAT3, a transcription factor involved in immune response, inflammation and tumorigenesis, has been found to be critical for compensatory liver regeneration and chemically-induced HCC development [60]. Liu et al. indicated that HULC can elevate HBx, which co-activated the STAT3 to stimulate the miR-539 promoter, and then down regulated APOBEC3B to activate HBV in HBV-related hepatocellular carcinoma [61]. The expression of HULC and endothelial cell specific molecule 1 (ESM-1) in glioma tissue is positively correlated with microvessel density and hierarchical dependence. Thus, the pro-angiogenic activity mechanism of HULC may be achieved by regulating ESM-1 through the PI3K/ Akt/ mTOR signal transduction pathway [62].
We found several meta-analyses evaluating the correlation between HULC expression level and prognosis. However, there is some difference between our study and the previous meta-analyses. First, the inclusion criteria are different. The previously meta-analyses evaluated the correlation between HULC expression and survival prognosis of cancer patients. These meta-analyses included various cancers. However, our study only included patients with digestive system tumors. A meta-analysis by Li et al. has no restrictions on the language of the publications [63]. Secondly, the number of eligible studies is increased significantly. The publications related to digestive system tumors included in the previous meta-analyses was 4-6, while we included 14 studies reporting digestive system tumors [29, 63–66]. Third, previous studies do not evaluate the correlation between HULC expression levels and tumor differentiation. Our meta-analysis confirms the association between HULC expression levels and survival prognosis in patients with digestive system tumors, and adds the analysis of tumor size, number of tumors, differentiation, age and gender of patients. Finally, although most of the studies were from China, this meta-analysis also included studies from South Korea, Japan and Germany.
However, this study still has some obvious limitations. First, Due to the complexity of digestive cancer types, the mechanism of HULC may be different among digestive system tumors. Then, there was no uniform cut-off value to define high HULC expression and low HULC expression. All included studies divided patients into high HULC expression group and low HULC expression group by mean or median. Third, the limited number of eligible studies and data in the analyses, leading to low statistical power and incomplete results. The HR and 95% CI extracted from the Kaplan-Meier curve were far less reliable than the values directly provided by original studies. Since the extracted HR and 95%CI could be affected by the subjective factors, it may lead to deviations of calculation. Next, the heterogeneity could not be completely improved, though the results of sensitivity analysis showed that our results were relatively robust. Finally, most of the included studies were from China, and the rest came from South Korea, Japan, and Germany. This limited the results of the study by region and ethnicity. Therefore, the results of this meta-analysis should be treated with caution for other ethnic groups.
In conclusion, this meta-analysis confirms that patients with up-regulated HULC may cause poorer clinical outcomes. Our results also show that the high expression level of HULC in serum and plasma was related to poor survival prognosis. HULC, especially from serum and plasma, can be used as a new potential predictor of the prognosis of patients with digestive system tumors. High expression of HULC increases the risk of high tumor stage, poor differentiation, and LNM in digestive system tumors. In view of the limitations mentioned above, it is necessary to conduct a more carefully designed study with diverse ethnic groups and large sample sizes to confirm the results of this meta-analysis and determine the predictive value of HULC in the prognosis of digestive system tumors.
Ethics approval and consent to participate
Ethical approval was not needed because this is a meta-analysis.
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
PC: pancreatic cancer; HCC: hepatocellular carcinoma; GC: gastric cancer; CRC: colorectal cancer; CC: colon cancer; CA: colon adenocarcinoma; OS: overall survival; DFS: disease-free survival; RFS: recurrence-free survival; HR: hazard ratio; CI: confidence interval; OR: odds ratio; TNM: tumor node metastasis; LNM: lymph node metastasis; DM: distant metastasis; WHO: World Health Organization; lncRNA: Long non-coding RNA; circRNA: circular RNA; miRNA: microRNA; HULC: Highly up-regulated in liver cancer; qRT-PCR: quantitative real-time polymerase chain reaction; CHOL: cholangiocarcinoma; COAD: colon adenocarcinoma; ESCA: esophageal carcinoma; LIHC: liver hepatocellular carcinoma; READ: rectum adenocarcinoma; MALAT1: metastasis-associated lung adenocarcinoma transcript 1; XIST: X-inactive specific transcript; NORAD: non-coding RNA activated by DNA damage; YB-1: Y-box binding protein 1; LDHA: lactate dehydrogenase A; PKM2: pyruvate kinase M2; FGFR1: fibroblast growth factor receptor type 1; EMT: epithelial-mesenchymal transition; P62: sequestosome 1; LC3II: microtubule-associated protein 1 light chain 3 alpha; VEGF: vascular endothelial growth factor; ESM-1: endothelial cell specific molecule 1; PI3K: phosphatidylinositol 3-kinase; Akt: protein kinase B; mTOR: mammalian target of rapamycin.
Author Contributions
LD, WR, WN, YYQ: Critical revision of the manuscript; LD, WR, WN, YYQ: Substantial contribution to the conception and design of the work, manuscript drafting; LD, WR, WN, YYQ: Acquisition, analysis, and interpretation of the data; LD, WR, WN, YYQ: Revising the manuscript critically, final approval of the version to be published. All authors have read and approved the final manuscript.
Conflicts of Interest
All the authors declare that they have no conflicts of interest.
References
- 1. Shafabakhsh R, Arianfar F, Vosough M, Mirzaei HR, Mahjoubin-Tehran M, Khanbabaei H, Kowsari H, Shojaie L, Azar ME, Hamblin MR, Mirzaei H. Autophagy and gastrointestinal cancers: the behind the scenes role of long non-coding RNAs in initiation, progression, and treatment resistance. Cancer Gene Ther. 2021; 28:1229–55. https://doi.org/10.1038/s41417-020-00272-7 [PubMed]
- 2. Sarvizadeh M, Hasanpour O, Naderi Ghale-Noie Z, Mollazadeh S, Rezaei M, Pourghadamyari H, Masoud Khooy M, Aschner M, Khan H, Rezaei N, Shojaie L, Mirzaei H. Allicin and Digestive System Cancers: From Chemical Structure to Its Therapeutic Opportunities. Front Oncol. 2021; 11:650256. https://doi.org/10.3389/fonc.2021.650256 [PubMed]
- 3. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019; 69:7–34. https://doi.org/10.3322/caac.21551 [PubMed]
- 4. Feng RM, Zong YN, Cao SM, Xu RH. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun (Lond). 2019; 39:22. https://doi.org/10.1186/s40880-019-0368-6 [PubMed]
- 5. Ashrafizadeh M, Zarrabi A, Hashemipour M, Vosough M, Najafi M, Shahinozzaman M, Hushmandi K, Khan H, Mirzaei H. Sensing the scent of death: modulation of microRNAs by Curcumin in gastrointestinal cancers. Pharmacol Res. 2020; 160:105199. https://doi.org/10.1016/j.phrs.2020.105199 [PubMed]
- 6. Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, Stein KD, Alteri R, Jemal A. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016; 66:271–89. https://doi.org/10.3322/caac.21349 [PubMed]
- 7. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87–108. https://doi.org/10.3322/caac.21262 [PubMed]
- 8. Hashemian SM, Pourhanifeh MH, Fadaei S, Velayati AA, Mirzaei H, Hamblin MR. Non-coding RNAs and Exosomes: Their Role in the Pathogenesis of Sepsis. Mol Ther Nucleic Acids. 2020; 21:51–74. https://doi.org/10.1016/j.omtn.2020.05.012 [PubMed]
- 9. Ahluwalia P, Kolhe R, Gahlay GK. The clinical relevance of gene expression based prognostic signatures in colorectal cancer. Biochim Biophys Acta Rev Cancer. 2021; 1875:188513. https://doi.org/10.1016/j.bbcan.2021.188513 [PubMed]
- 10. Pourhanifeh MH, Vosough M, Mahjoubin-Tehran M, Hashemipour M, Nejati M, Abbasi-Kolli M, Sahebkar A, Mirzaei H. Autophagy-related microRNAs: possible regulatory roles and therapeutic potential in and gastrointestinal cancers. Pharmacol Res. 2020; 161:105133. https://doi.org/10.1016/j.phrs.2020.105133 [PubMed]
- 11. Naeli P, Pourhanifeh MH, Karimzadeh MR, Shabaninejad Z, Movahedpour A, Tarrahimofrad H, Mirzaei HR, Bafrani HH, Savardashtaki A, Mirzaei H, Hamblin MR. Circular RNAs and gastrointestinal cancers: epigenetic regulators with a prognostic and therapeutic role. Crit Rev Oncol Hematol. 2020; 145:102854. https://doi.org/10.1016/j.critrevonc.2019.102854 [PubMed]
- 12. Guo CJ, Zhang W, Gershwin ME. Long noncoding RNA lncKdm2b: A critical player in the maintenance of group 3 innate lymphoid cells. Cell Mol Immunol. 2018; 15:5–7. https://doi.org/10.1038/cmi.2017.55 [PubMed]
- 13. Ponting CP, Oliver PL, Reik W. Evolution and functions of long noncoding RNAs. Cell. 2009; 136:629–41. https://doi.org/10.1016/j.cell.2009.02.006 [PubMed]
- 14. Bhan A, Soleimani M, Mandal SS, Long Noncoding RN. Long Noncoding RNA and Cancer: A New Paradigm. Cancer Res. 2017; 77:3965–81. https://doi.org/10.1158/0008-5472.CAN-16-2634 [PubMed]
- 15. Bhan A, Mandal SS. LncRNA HOTAIR: A master regulator of chromatin dynamics and cancer. Biochim Biophys Acta. 2015; 1856:151–64. https://doi.org/10.1016/j.bbcan.2015.07.001 [PubMed]
- 16. Wapinski O, Chang HY. Long noncoding RNAs and human disease. Trends Cell Biol. 2011; 21:354–61. https://doi.org/10.1016/j.tcb.2011.04.001 [PubMed]
- 17. Mahjoubin-Tehran M, Rezaei S, Jesmani A, Birang N, Morshedi K, Khanbabaei H, Khan H, Piranviseh A, Nejati M, Aschner M, Mirzaei H. New epigenetic players in stroke pathogenesis: from non-coding RNAs to exosomal non-coding RNAs. Biomed Pharmacother. 2021; 140:111753. https://doi.org/10.1016/j.biopha.2021.111753 [PubMed]
- 18. Morán I, Akerman I, van de Bunt M, Xie R, Benazra M, Nammo T, Arnes L, Nakić N, García-Hurtado J, Rodríguez-Seguí S, Pasquali L, Sauty-Colace C, Beucher A, et al. Human β cell transcriptome analysis uncovers lncRNAs that are tissue-specific, dynamically regulated, and abnormally expressed in type 2 diabetes. Cell Metab. 2012; 16:435–48. https://doi.org/10.1016/j.cmet.2012.08.010 [PubMed]
- 19. Kogo R, Shimamura T, Mimori K, Kawahara K, Imoto S, Sudo T, Tanaka F, Shibata K, Suzuki A, Komune S, Miyano S, Mori M. Long noncoding RNA HOTAIR regulates polycomb-dependent chromatin modification and is associated with poor prognosis in colorectal cancers. Cancer Res. 2011; 71:6320–6. https://doi.org/10.1158/0008-5472.CAN-11-1021 [PubMed]
- 20. Rahimian N, Razavi ZS, Aslanbeigi F, Mirkhabbaz AM, Piroozmand H, Shahrzad MK, Hamblin MR, Mirzaei H. Non-coding RNAs related to angiogenesis in gynecological cancer. Gynecol Oncol. 2021; 161:896–912. https://doi.org/10.1016/j.ygyno.2021.03.020 [PubMed]
- 21. Hashemipour M, Boroumand H, Mollazadeh S, Tajiknia V, Nourollahzadeh Z, Rohani Borj M, Pourghadamyari H, Rahimian N, Hamblin MR, Mirzaei H. Exosomal microRNAs and exosomal long non-coding RNAs in gynecologic cancers. Gynecol Oncol. 2021; 161:314–27. https://doi.org/10.1016/j.ygyno.2021.02.004 [PubMed]
- 22. Yu X, Zheng H, Chan MT, Wu WK. HULC: an oncogenic long non-coding RNA in human cancer. J Cell Mol Med. 2017; 21:410–7. https://doi.org/10.1111/jcmm.12956 [PubMed]
- 23. Gavgani RR, Babaei E, Hosseinpourfeizi MA, Fakhrjou A, Montazeri V. Study of long non-coding RNA highly upregulated in liver cancer (HULC) in breast cancer: A clinical and in vitro investigation. Indian J Med Res. 2020; 152:244–53. https://doi.org/10.4103/ijmr.IJMR_1823_18 [PubMed]
- 24. Ou ZL, Luo Z, Lu YB. Long non-coding RNA HULC as a diagnostic and prognostic marker of pancreatic cancer. World J Gastroenterol. 2019; 25:6728–42. https://doi.org/10.3748/wjg.v25.i46.6728 [PubMed]
- 25. Wang J, Ma W, Liu Y. Long non-coding RNA HULC promotes bladder cancer cells proliferation but inhibits apoptosis via regulation of ZIC2 and PI3K/AKT signaling pathway. Cancer Biomark. 2017; 20:425–34. https://doi.org/10.3233/CBM-170188 [PubMed]
- 26. Panzitt K, Tschernatsch MM, Guelly C, Moustafa T, Stradner M, Strohmaier HM, Buck CR, Denk H, Schroeder R, Trauner M, Zatloukal K. Characterization of HULC, a novel gene with striking up-regulation in hepatocellular carcinoma, as noncoding RNA. Gastroenterology. 2007; 132:330–42. https://doi.org/10.1053/j.gastro.2006.08.026 [PubMed]
- 27. Abdi E, Latifi-Navid S, Abdi F, Taherian-Esfahani Z. Emerging circulating MiRNAs and LncRNAs in upper gastrointestinal cancers. Expert Rev Mol Diagn. 2020; 20:1121–38. https://doi.org/10.1080/14737159.2020.1842199 [PubMed]
- 28. Dong Y, Wei MH, Lu JG, Bi CY. Long non-coding RNA HULC interacts with miR-613 to regulate colon cancer growth and metastasis through targeting RTKN. Biomed Pharmacother. 2019; 109:2035–42. https://doi.org/10.1016/j.biopha.2018.08.017 [PubMed]
- 29. Ding Y, Sun C, Li J, Hu L, Li M, Liu J, Pu L, Xiong S. The Significance of Long Non-coding RNA HULC in Predicting Prognosis and Metastasis of Cancers: a Meta-Analysis. Pathol Oncol Res. 2019; 25:311–8. https://doi.org/10.1007/s12253-017-0351-y [PubMed]
- 30. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25:603–5. https://doi.org/10.1007/s10654-010-9491-z [PubMed]
- 31. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007; 8:16. https://doi.org/10.1186/1745-6215-8-16 [PubMed]
- 32. Tang Z, Kang B, Li C, Chen T, Zhang Z. GEPIA2: an enhanced web server for large-scale expression profiling and interactive analysis. Nucleic Acids Res. 2019; 47:W556–60. https://doi.org/10.1093/nar/gkz430 [PubMed]
- 33. Liu T, Liu Y, Wei C, Yang Z, Chang W, Zhang X. LncRNA HULC promotes the progression of gastric cancer by regulating miR-9-5p/MYH9 axis. Biomed Pharmacother. 2020; 121:109607. https://doi.org/10.1016/j.biopha.2019.109607 [PubMed]
- 34. Oehme F, Krahl S, Gyorffy B, Muessle B, Rao V, Greif H, Ziegler N, Lin K, Thepkaysone ML, Polster H, Tonn T, Schneider M, Weitz J, et al. Low level of exosomal long non-coding RNA HOTTIP is a prognostic biomarker in colorectal cancer. RNA Biol. 2019; 16:1339–45. https://doi.org/10.1080/15476286.2019.1637697 [PubMed]
- 35. Cao SQ, Zheng H, Sun BC, Wang ZL, Liu T, Guo DH, Shen ZY. Long non-coding RNA highly up-regulated in liver cancer promotes exosome secretion. World J Gastroenterol. 2019; 25:5283–99. https://doi.org/10.3748/wjg.v25.i35.5283 [PubMed]
- 36. Zhang Z, Qian W, Wang S, Ji D, Wang Q, Li J, Peng W, Gu J, Hu T, Ji B, Zhang Y, Wang S, Sun Y. Analysis of lncRNA-Associated ceRNA Network Reveals Potential lncRNA Biomarkers in Human Colon Adenocarcinoma. Cell Physiol Biochem. 2018; 49:1778–91. https://doi.org/10.1159/000493623 [PubMed]
- 37. Sonohara F, Inokawa Y, Hayashi M, Yamada S, Sugimoto H, Fujii T, Kodera Y, Nomoto S. Prognostic Value of Long Non-Coding RNA HULC and MALAT1 Following the Curative Resection of Hepatocellular Carcinoma. Sci Rep. 2017; 7:16142. https://doi.org/10.1038/s41598-017-16260-1 [PubMed]
- 38. Zhang Y, Song X, Wang X, Hu J, Jiang L. Silencing of LncRNA HULC Enhances Chemotherapy Induced Apoptosis in Human Gastric Cancer. J Med Biochem. 2016; 35:137–43. https://doi.org/10.1515/jomb-2015-0016 [PubMed]
- 39. Yang XJ, Huang CQ, Peng CW, Hou JX, Liu JY. Long noncoding RNA HULC promotes colorectal carcinoma progression through epigenetically repressing NKD2 expression. Gene. 2016; 592:172–8. https://doi.org/10.1016/j.gene.2016.08.002 [PubMed]
- 40. Li SP, Xu HX, Yu Y, He JD, Wang Z, Xu YJ, Wang CY, Zhang HM, Zhang RX, Zhang JJ, Yao Z, Shen ZY. LncRNA HULC enhances epithelial-mesenchymal transition to promote tumorigenesis and metastasis of hepatocellular carcinoma via the miR-200a-3p/ZEB1 signaling pathway. Oncotarget. 2016; 7:42431–46. https://doi.org/10.18632/oncotarget.9883 [PubMed]
- 41. Jin C, Shi W, Wang F, Shen X, Qi J, Cong H, Yuan J, Shi L, Zhu B, Luo X, Zhang Y, Ju S. Long non-coding RNA HULC as a novel serum biomarker for diagnosis and prognosis prediction of gastric cancer. Oncotarget. 2016; 7:51763–72. https://doi.org/10.18632/oncotarget.10107 [PubMed]
- 42. Yang Z, Lu Y, Xu Q, Tang B, Park CK, Chen X. HULC and H19 Played Different Roles in Overall and Disease-Free Survival from Hepatocellular Carcinoma after Curative Hepatectomy: A Preliminary Analysis from Gene Expression Omnibus. Dis Markers. 2015; 2015:191029. https://doi.org/10.1155/2015/191029 [PubMed]
- 43. Li J, Wang X, Tang J, Jiang R, Zhang W, Ji J, Sun B. HULC and Linc00152 Act as Novel Biomarkers in Predicting Diagnosis of Hepatocellular Carcinoma. Cell Physiol Biochem. 2015; 37:687–96. https://doi.org/10.1159/000430387 [PubMed]
- 44. Peng W, Gao W, Feng J. Long noncoding RNA HULC is a novel biomarker of poor prognosis in patients with pancreatic cancer. Med Oncol. 2014; 31:346. https://doi.org/10.1007/s12032-014-0346-4 [PubMed]
- 45. Lou W, Ding B, Fu P. Pseudogene-Derived lncRNAs and Their miRNA Sponging Mechanism in Human Cancer. Front Cell Dev Biol. 2020; 8:85. https://doi.org/10.3389/fcell.2020.00085 [PubMed]
- 46. Rathinasamy B, Velmurugan BK. Role of lncRNAs in the cancer development and progression and their regulation by various phytochemicals. Biomed Pharmacother. 2018; 102:242–8. https://doi.org/10.1016/j.biopha.2018.03.077 [PubMed]
- 47. Ye T, Ye Z. LncRNA NORAD as a Novel Predictor of Lymph Node Metastasis and Prognosis in Solid Tumors: A Systematic Review and Meta-Analysis. Technol Cancer Res Treat. 2020; 19:1533033820963586. https://doi.org/10.1177/1533033820963586 [PubMed]
- 48. Deng C, Hu X, Wu K, Tan J, Yang C. Long non-coding RNA XIST predicting advanced clinical parameters in cancer: A Meta-Analysis and case series study in a single institution. Oncol Lett. 2019; 18:2192–202. https://doi.org/10.3892/ol.2019.10592 [PubMed]
- 49. Wei Y, Niu B. Role of MALAT1 as a Prognostic Factor for Survival in Various Cancers: A Systematic Review of the Literature with Meta-Analysis. Dis Markers. 2015; 2015:164635. https://doi.org/10.1155/2015/164635 [PubMed]
- 50. Wang WT, Ye H, Wei PP, Han BW, He B, Chen ZH, Chen YQ. LncRNAs H19 and HULC, activated by oxidative stress, promote cell migration and invasion in cholangiocarcinoma through a ceRNA manner. J Hematol Oncol. 2016; 9:117. https://doi.org/10.1186/s13045-016-0348-0 [PubMed]
- 51. Lyabin DN, Eliseeva IA, Ovchinnikov LP. YB-1 protein: functions and regulation. Wiley Interdiscip Rev RNA. 2014; 5:95–110. https://doi.org/10.1002/wrna.1200 [PubMed]
- 52. Wolffe AP. Structural and functional properties of the evolutionarily ancient Y-box family of nucleic acid binding proteins. BioEssays. 1994; 16:245–51. https://doi.org/10.1002/bies.950160407 [PubMed]
- 53. Li D, Liu X, Zhou J, Hu J, Zhang D, Liu J, Qiao Y, Zhan Q. Long noncoding RNA HULC modulates the phosphorylation of YB-1 through serving as a scaffold of extracellular signal-regulated kinase and YB-1 to enhance hepatocarcinogenesis. Hepatology. 2017; 65:1612–27. https://doi.org/10.1002/hep.29010 [PubMed]
- 54. Mirzaei H, Hamblin MR. Regulation of Glycolysis by Non-coding RNAs in Cancer: Switching on the Warburg Effect. Mol Ther Oncolytics. 2020; 19:218–39. https://doi.org/10.1016/j.omto.2020.10.003 [PubMed]
- 55. Wang C, Li Y, Yan S, Wang H, Shao X, Xiao M, Yang B, Qin G, Kong R, Chen R, Zhang N. Interactome analysis reveals that lncRNA HULC promotes aerobic glycolysis through LDHA and PKM2. Nat Commun. 2020; 11:3162. https://doi.org/10.1038/s41467-020-16966-3 [PubMed]
- 56. Tkach M, Théry C. Communication by Extracellular Vesicles: Where We Are and Where We Need to Go. Cell. 2016; 164:1226–32. https://doi.org/10.1016/j.cell.2016.01.043 [PubMed]
- 57. Takahashi K, Ota Y, Kogure T, Suzuki Y, Iwamoto H, Yamakita K, Kitano Y, Fujii S, Haneda M, Patel T, Ota T. Circulating extracellular vesicle-encapsulated HULC is a potential biomarker for human pancreatic cancer. Cancer Sci. 2020; 111:98–111. https://doi.org/10.1111/cas.14232 [PubMed]
- 58. Takahashi K, Koyama K, Ota Y, Iwamoto H, Yamakita K, Fujii S, Kitano Y. The Interaction Between Long Non-coding RNA HULC and MicroRNA-622 via Transfer by Extracellular Vesicles Regulates Cell Invasion and Migration in Human Pancreatic Cancer. Front Oncol. 2020; 10:1013. https://doi.org/10.3389/fonc.2020.01013 [PubMed]
- 59. Xin X, Wu M, Meng Q, Wang C, Lu Y, Yang Y, Li X, Zheng Q, Pu H, Gui X, Li T, Li J, Jia S, Lu D. Long noncoding RNA HULC accelerates liver cancer by inhibiting PTEN via autophagy cooperation to miR15a. Mol Cancer. 2018; 17:94. https://doi.org/10.1186/s12943-018-0843-8 [PubMed]
- 60. He G, Karin M. NF-κB and STAT3 - key players in liver inflammation and cancer. Cell Res. 2011; 21:159–68. https://doi.org/10.1038/cr.2010.183 [PubMed]
- 61. Liu Y, Feng J, Sun M, Yang G, Yuan H, Wang Y, Bu Y, Zhao M, Zhang S, Zhang X. Long non-coding RNA HULC activates HBV by modulating HBx/STAT3/miR-539/APOBEC3B signaling in HBV-related hepatocellular carcinoma. Cancer Lett. 2019; 454:158–70. https://doi.org/10.1016/j.canlet.2019.04.008 [PubMed]
- 62. Zhu Y, Zhang X, Qi L, Cai Y, Yang P, Xuan G, Jiang Y. HULC long noncoding RNA silencing suppresses angiogenesis by regulating ESM-1 via the PI3K/Akt/mTOR signaling pathway in human gliomas. Oncotarget. 2016; 7:14429–40. https://doi.org/10.18632/oncotarget.7418 [PubMed]
- 63. Li Y, Liu YH, Chen X, Zhu YJ, Zhang HB, Li Y, Bai JP, Liu LR, Qu YC, Qu X. Effect of long non-coding RNA highly up-regulated in liver cancer (HULC) on the prognosis of cancer: a meta-analysis. Oncotarget. 2017; 8:83246–50. https://doi.org/10.18632/oncotarget.18452 [PubMed]
- 64. Fan YH, Wu MJ, Jiang Y, Ye M, Lu SG, Wu L, Zhu XG. Long non-coding RNA HULC as a potential prognostic biomarker in human cancers: a meta-analysis. Oncotarget. 2017; 8:21410–7. https://doi.org/10.18632/oncotarget.15247 [PubMed]
- 65. Chen X, Lun L, Hou H, Tian R, Zhang H, Zhang Y. The Value of lncRNA HULC as a Prognostic Factor for Survival of Cancer Outcome: A Meta-Analysis. Cell Physiol Biochem. 2017; 41:1424–34. https://doi.org/10.1159/000468005 [PubMed]
- 66. Wang Y, Huang Y, Xiang P, Tian W. LncRNA expression and implication in osteosarcoma: a systematic review and meta-analysis. Onco Targets Ther. 2017; 10:5355–61. https://doi.org/10.2147/OTT.S149889 [PubMed]