



Introduction
The aldehyde dehydrogenase (ALDH) superfamily, encoded by ALDH genes, is crucial for metabolizing physiological and pathophysiological aldehydes [1]. ALDH polymorphisms or mutations reduce the activities of ALDH and increase acetaldehyde, which is toxic, mutagenic, and carcinogenic. Acetaldehyde also results in deoxyribonucleic acid (DNA) adducts, inhibited DNA repair, and DNA methylation [2]. As many as 19 ALDH genes have been identified within the human genome, and several diseases have been proven to be associated with ALDH mutations [3]. However, the role of individual ALDH genes in cancer development and prognosis has been a subject of controversial discussion.
ALDH 7 family member A1 (ALDH7A1), a member of the ALDH superfamily, is the enzyme encoded by ALDH7A1 [4]. Several studies have proven the relationship between ALDH7A1 mutations and pyridoxine-dependent seizures in children [5]. ALDH7A1 dysfunctions have also been associated with other disorders, such as osteoporosis and Huntington’s disease, as well as with the mechanism of intracellular transport [6–9]. However, the role of ALDH7A1 in cancer development and prognosis has remained unclear. The roles of the different ALDH7A1 polymorphisms may vary, moreover, on account of different allele mutations and cancer types [10, 11].
Oral cancer, a subgroup of head and neck squamous cell carcinoma (HNSCC), is the sixth most common cancer globally and the fourth most common cancer in Taiwanese men [12, 13]. Although several innovative treatments that are effective in prolonging survival have been developed and approved [14, 15], over 50% of patients using those treatment agents still progressed to recurrent metastatic status, and only 20%–30% of them experienced long-term survival [16, 17]. With the development of next-generation sequencing, applying genetic information to cancer risk prediction, diagnosis, and treatment has become more feasible [18–20]. The role of genetic polymorphism in cancer development and progression is also critical.
In this study, we enrolled patients diagnosed as having oral cancer and healthy controls as participants. The ALDH7A1 single-nucleotide polymorphisms (SNPs) of these participants were retrospectively tested. The effects of ALDH7A1 polymorphism were compared for all participants, those who habitually chewed betel quid, and those who did not chew betel quid. Furthermore, published databases, such as Genotype-Tissue Expression (GTEx) Portal and The Cancer Genome Atlas (TCGA), were used to validate our results. Oral cancer tissues and five oral cancer cell lines (SCC-14, SAS, CA9-22, HSC-3, and OECM-1) were used to investigate the correlations of ALDH7A1 rs13182402 polymorphisms and ALDH7A1 expression levels. Based on this study, we discovered the impact and functions of ALDH7A1 polymorphism in oral cancer.
Results
Baseline characteristics
A total of 1332 patients with oral cancer and 1191 healthy controls were enrolled. All the participants were male. No major age difference between the patients and healthy controls was observed (P = 0.920). Due to the observational study, patients with oral cancer were significantly more likely to smoke cigarettes, drink alcohol, and chew betel quid than the healthy controls were (all P < 0.001). The basic characteristics of the participants are presented in Table 1.
Table 1. Basic characteristics of the patients with oral cancer and healthy controls.
| Variable | Patients (N = 1332) | Controls (N = 1191) | P value |
| Age (yrs) | P = 0.476 | ||
| ≧55 | 705 (52.9%) | 628 (52.7%) | |
| <55 | 627 (47.1%) | 563 (47.3%) | |
| Cigarette smoking | P < 0.001* | ||
| Yes | 1124 (84.4%) | 632 (53.1%) | |
| No | 208 (15.6%) | 559 (46.9%) | |
| Alcohol drinking | P < 0.001* | ||
| Yes | 635 (47.7%) | 236 (19.8%) | |
| No | 697 (52.3%) | 955 (80.2%) | |
| Betel quid chewing | P < 0.001* | ||
| Yes | 994 (74.6%) | 199 (16.7%) | |
| No | 338 (25.4%) | 992 (83.3%) | |
| Pathologic staging | |||
| I + II | 622 (46.7%) | ||
| III + IV | 710 (53.3%) | ||
| Pathologic T staging | |||
| T1 + T2 | 667 (50.1%) | ||
| T3 + T4 | 665 (49.9%) | ||
| Pathologic N staging | |||
| N0 | 876 (65.8%) | ||
| N+ | 456 (34.2%) | ||
| Pathologic M staging | |||
| M0 | 1322 (99.2%) | ||
| M1 | 10 (0.8%) | ||
| Histological differentiation | |||
| Well | 186 (14.0%) | ||
| Moderate to poor | 1146 (86.0%) |
ALDH7A1 SNPs
Two ALDH7A1 SNPs, namely rs13182402 and rs12659017, were sequenced for all participants. Both SNPs are located on chromosome 5. The allele frequencies of the SNPs for the East Asian population are 5.75% and 70.4%, respectively, as reported by the 1000 Genomes Project. The clinical significance of these two SNPs is not reported in ClinVar (Table 2).
Table 2. Detailed information of ALDH7A1 SNPs from dbSNP.
| dbSNP | rs13182402 | rs12659017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Organism | Homo sapiens | Homo sapiens | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Position1 | chr5:126582456 | chr5:126652483 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nucleotide change | A>G | G>A | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Variation type | SNV | SNV | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Minor allele frequency2 | G = 0.0575 | A = 0.7044 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gene consequence | Intron variant | None | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical significance | Not reported in ClinVar | Not reported in ClinVar | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1GRCh38.p12. 2Minor allele frequency using the East Asian population from 1000 Genomes. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Influence of ALDH7A1 SNPs in oral cancer development
The incidences of ALDH7A1 rs13182402 and rs12659017 polymorphism between the patients with oral cancer and healthy controls were comparable. For the AORs, which were because of different basic characteristics and adjusted by age, smoke cigarettes, drink alcohol, and chew betel quid, also showed that cancer development risk between these two groups was no different. In Taiwan, oral cancer is the largest subgroup of HNSCC, and more than 80% of patients with oral cancer habitually chew betel quid [21, 22]. Betel quid chewing significantly contributes to the development of oral cancer [23–25]. Thus, the analysis classified participants into categories of alcohol drinkers and betel quid chewers. As shown in Table 3, no significant differences were observed between oral cancer patients with ALDH7A1 rs13182402 and rs12659017 and those with the wild-type (WT) gene. Moreover, no associations were observed in the alcohol drinker or betel quid chewer (Table 3).
Table 3. Odds ratios (OR) and 95% confidence interval (CI) of oral cancer associated with ALDH7A1 genotypic frequencies.
| Variable | Patients (N, %) | Controls (N, %) | OR (95% CI) | AOR (95% CI)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| All (both Betel quid chewer and non-betel quid chewer) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N = 1332 | N = 1191 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs13182402 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 1161 (87.2%) | 1063 (89.3%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 166 (12.5%) | 125 (10.5%) | 1.216 (0.950–1.556) | 1.177 (0.868–1.597) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 5 (0.4%) | 3 (0.3%) | 1.526 (0.364–6.401) | 1.600 (0.293–8.725) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 171 (12.8%) | 128 (10.7%) | 1.223 (0.959–1.561) | 1.188 (0.879–1.605) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs12659017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 698 (52.4%) | 611 (51.3%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 534 (40.1%) | 490 (41.1%) | 0.954 (0.810–1.124) | 1.058 (0.863–1.296) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 100 (7.5%) | 90 (7.6%) | 0.973 (0.431–1.319) | 0.919 (0.634–1.333) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 634 (47.6%) | 580 (48.7%) | 0.957 (0.818–1.119) | 1.033 (0.851–1.253) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcohol drinker | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N = 635 | N = 236 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs13182402 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 560 (88.2%) | 205 (86.9%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 73 (11.5%) | 30 (12.7%) | 0.891 (0.566–1.403) | 0.822 (0.481–1.406) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 2 (0.3%) | 1 (0.4%) | 0.732 (0.066–8.117) | 0.757 (0.046–12.557) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 75 (11.8%) | 31 (13.1%) | 0.886 (0.566–1.386) | 0.821 (0.484–1.391) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs12659017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 332 (52.3%) | 122 (51.7%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 256 (40.3%) | 93 (39.4%) | 1.012 (0.738–1.386) | 1.154 (0.798–1.670) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 47 (7.4%) | 21 (8.9%) | 0.822 (0.472–1.432) | 0.812 (0.426–1.548) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 303 (47.7%) | 114 (48.3%) | 0.977 (0.724–1.317) | 1.086 (0.765–1.542) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Betel quid chewer | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N = 994 | N = 199 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs13182402 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 868 (87.3%) | 174 (87.4%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 123 (12.4%) | 24 (12.1%) | 1.027 (0.664–1.638) | 1.024 (0.641–1.638) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 3 (0.3%) | 1 (0.5%) | 0.601 (0.062–5.815) | 0.608 (0.062–5.936) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 126 (12.7%) | 25 (12.6%) | 1.010 (0.638–1.599) | 1.007 (0.635–1.597) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| rs12659017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AA | 524 (52.7%) | 114 (57.3%) | 1.000 (reference) | 1.000 (reference) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG | 394 (39.6%) | 66 (33.2%) | 1.299 (0.934–1.807) | 1.289 (0.925–1.796) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GG | 76 (7.7%) | 19 (9.5%) | 0.870 (0.506–1.496) | 0.866 (0.502–1.494) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AG+GG | 470 (47.3%) | 85 (42.7%) | 1.203 (0.885–1.636) | 1.195 (0.878–1.628) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aAdjusted for the effects of age, cigarette smoking, alcohol drinking, and betel quid chewer. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Prognostic effect of ALDH7A1 SNPs in oral cancer
The prognostic influence of ALDH7A1 SNPs in oral cancer was also analyzed. Among the patients with and without ALDH7A1 rs13182402 and rs12659017 polymorphism, no differences in pathologic staging, tumor size, lymph node metastasis, distant metastasis, or histologic differentiation were observed (Tables 4 and 5). Among the patients who habitually used betel quid, however, those with ALDH7A1 rs13182402 polymorphism had less pathologic nodal metastasis than did those with the normal allele type (AG + GG vs. AA, 24.6% vs. 34.6%, P = 0.016; Table 4). After adjustment for other factors, ALDH7A1 rs13182402 represented an independent favorable prognostic factor for nodal metastasis (OR [95% confidence interval (CI)] = 0.596 [0.382–0.929], P = 0.022; Table 6).
Table 4. The distributions of demographical characteristics of ALDH7A1 rs13182402 allele mutation in oral cancer.
| Variable | Total (N = 1332) | Alcohol drinker (N = 635) | Betel Quid Chewers (N = 994) | ||||||
| AA (N = 1161) | AG+GG (N = 171) | P value | AA (N = 560) | AG+GG (N = 75) | P value | AA (N = 868) | AG+GG (N = 126) | P value | |
| Stage | |||||||||
| Stage I + II | 544 (46.9%) | 78 (45.6%) | 0.413 | 260(46.4%) | 32(42.7%) | 0.313 | 408 (47.0%) | 62 (49.2%) | 0.356 |
| Stage III + IV | 617 (53.1%) | 93 (54.4%) | 300(53.6%) | 43(57.3%) | 460 (53.0%) | 64 (50.8%) | |||
| T staging | |||||||||
| T1/2 | 591(50.9%) | 570 (49.1%) | 0.067 | 295(52.7%) | 37(49.3%) | 0.336 | 446 (51.4%) | 60 (47.6%) | 0.244 |
| T3/4 | 570 (49.1%) | 95 (55.6%) | 265(47.3%) | 38(50.7%) | 422 (48.6%) | 66 (52.4%) | |||
| N staging | |||||||||
| N0 | 758 (65.3%) | 118 (69.0%) | 0.193 | 201(62.7%) | 28(37.3%) | 0.45 | 568 (65.4%) | 95 (75.4%) | 0.016 |
| N+ | 403 (34.7%) | 53 (31.0%) | 359(64.1%) | 47(62.7%) | 300 (34.6%) | 31 (24.6%) | |||
| Metastasis | |||||||||
| M0 | 1152 (99.2%) | 170 (99.4%) | 0.626 | 554(98.9%) | 74(98.7%) | 0.587 | 861 (99.2%) | 126 (100.0%) | 0.386 |
| M1 | 9 (0.8%) | 1 (0.6%) | 6(1.1%) | 1(1.3%) | 7 (0.8%) | 0 (0.0%) | |||
| Cell differentiated | |||||||||
| Well | 161 (13.9%) | 25 (14.6%) | 0.433 | 80(14.3%) | 11(14.7%) | 0.522 | 131 (15.1%) | 20 (15.9%) | 0.453 |
| Moderate or poor | 1000 (86.1%) | 146 (85.4%) | 480(85.7%) | 64(85.3%) | 737 (84.9%) | 106 (84.1%) | |||
Table 5. The distributions of demographical characteristics of ALDH7A1 rs12659017 allele mutation in oral cancer.
| Variable | Total (N = 1332) | Alcohol drinker (N = 635) | Betel Quid Chewers (N = 994) | ||||||
| AA (N = 698) | AG+GG (N = 634) | P value | AA (N = 332) | AG+GG (N = 303) | P value | AA (N = 524) | AG+GG (N = 470) | P value | |
| Stage | |||||||||
| Stage I + II | 342 (49.0%) | 280 (44.2%) | 0.044 | 154 (46.4%) | 138 (45.5%) | 0.447 | 256 (48.9%) | 214 (45.5%) | 0.163 |
| Stage III + IV | 356 (51.0%) | 354 (55.8%) | 178 (53.6%) | 165 (54.5%) | 268 (51.1%) | 256 (54.5%) | |||
| T staging | |||||||||
| T1/2 | 364 (52.1%) | 303 (47.8%) | 0.063 | 174 (52.4%) | 158 (52.1%) | 0.505 | 276 (52.7%) | 230 (48.9%) | 0.133 |
| T3/4 | 334 (47.9%) | 331 (52.2%) | 158 (47.6%) | 145 (47.9%) | 248 (47.3%) | 240 (51.1%) | |||
| N staging | |||||||||
| N+ | 233 (33.4%) | 223 (35.2%) | 0.264 | 209 (63.0%) | 197 (65.0%) | 0.323 | 179 (34.2%) | 152 (32.3%) | 0.295 |
| N0 | 465 (66.6%) | 411 (64.8%) | 123 (37.0%) | 106 (35.0%) | 345 (65.8%) | 318 (67.7%) | |||
| Metastasis | |||||||||
| M0 | 693 (99.3%) | 629 (99.2%) | 0.563 | 328 (98.8%) | 300 (99.0%) | 0.55 | 521 (99.4%) | 466 (99.1%) | 0.441 |
| M1 | 5 (0.7%) | 5 (0.8%) | 4 (1.2%) | 3 (1.0%) | 3 (0.6%) | 4 (0.9%) | |||
| Cell differentiated | |||||||||
| Well | 99 (14.2%) | 87 (13.7%) | 0.436 | 46 (13.9%) | 45 (14.9%) | 0.403 | 76 (14.5%) | 75 (16.0%) | 0.291 |
| Moderate or poor | 599 (85.8%) | 547 (86.3%) | 286 (86.1%) | 258 (85.1%) | 448 (85.5%) | 395 (84.0%) | |||
Table 6. Univariate and multivariate logistic regression for neck lymph node metastasis in oral cancer patients with betel quid chewing.
| Variable | Univariate | Multivariate | ||
| P value | OR (95% CI) | P value | OR (95% CI) | |
| Age (yrs) | ||||
| ≥ 55 vs. <55 | 0.069 | 0.783 (0.601–1.020) | ||
| Tumor T status | ||||
| T3/4 vs. T1/2 | <0.001 | 2.864 (2.174–3.772) | <0.001 | 3.100 (2.337–4.113) |
| Metastasis | ||||
| M1 vs. M0 | 0.021 | 12.222 (1.465–101.938) | 0.01 | 18.165 (2.024–162.999) |
| Cell differentiation | ||||
| Moderately or poorly differentiated vs. well differentiated | <0.001 | 2.465 (1.597–3.804) | <0.001 | 2.877 (1.829–4.524) |
| rs13182402 | ||||
| AG+GG vs. AA | 0.028 | 0.618 (0.402–0.949) | 0.022 | 0.596 (0.382–0.929) |
| rs12659017 | ||||
| AG+GG vs. AA | 0.543 | 0.921 (0.707–1.200) | ||
ALDH7A1 allele mutation with higher mRNA Expression
To support our findings, some published databases were used to validate our results. In the GTEx database, which has 54 enrolled non-diseased normal tissue sites covering nearly 1000 individuals, ALDH7A1 expression in the rs13182402 mutation expression (AG + GG) was higher in upper aerodigestive (esophagus) mucosa, whole blood, and the musculoskeletal system compared with the ALDH7A1 allele normal type (AA) (all P < 0.001; Figure 1A–1C). Furthermore, to realize correlation between the mRNA level of ALDH7A1 and rs13182402 polymorphism, quantitative real time-PCR (qPCR) were used to analyze ALDH7A1 mRNA level in cancer tissue of 30 oral cancer patients. We found that oral cancer patient who carry allele mutation (AG) of rs13182402 polymorphism have significantly higher mRNA levels of ALDH7A1 compare to AA genotype (Figure 1D). Taken together, these results demonstrated that ALDH7A1 allele mutation (rs13182402) was associated with higher ALDH7A1 expression than the ALDH7A1 SNP wild type was.
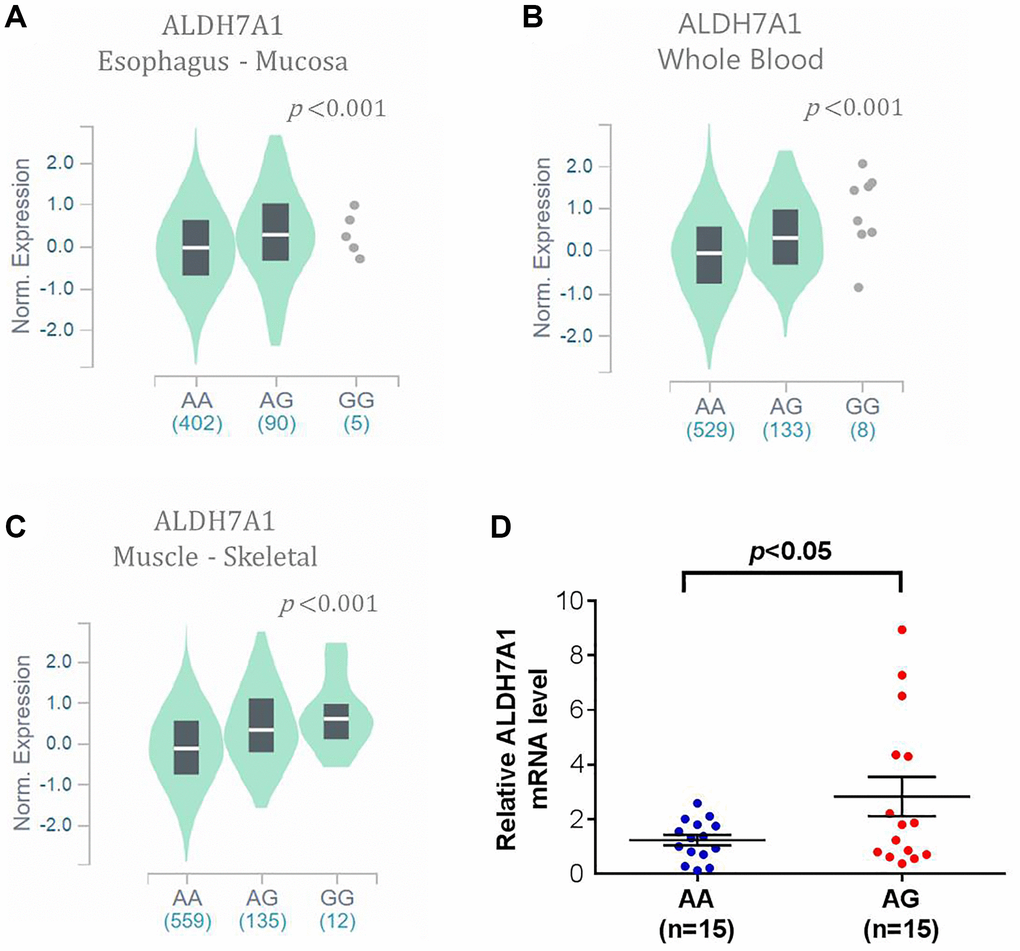
Figure 1. The validated results of ALDH7A1 expression by Genotype-Tissue Expression (GTEx) Portal (https://www.gtexportal.org/home/). (A–C) In GTEx, which enrolled 54 non-diseased tissue sites across nearly 1000 individuals, violin plots of ALDH7A1 rs13182402 mutation was associated with higher ALDH7A1 expression level in upper aerodigestive (esophagus) mucosa, whole blood, and musculoskeletal system than those of ALDH7A1 allele normal type (P < 0.001, < 0.001, < 0.001, respectively). (D) ALDH7A1 mRNA expression in cancer tissue of 30 oral cancer patients was analyzed by quantitative real time-PCR assay.
Relationship between ALDH7A1 expression and clinical outcomes
ALDH7A1 expression was lower in tumor tissues than in normal and adjacent normal tissues from the TCGA database (both P < 0.001; Figure 2A and 2B). Within the tumor tissues, ALDH7A1 expression levels were also lower for patients with nodal metastasis than for those without (P < 0.0257; Figure 2C). The patients could be divided into ALDH7A1-high- and ALDH7A1-low-expression groups. Because approximately 10% (12.8%, 171 out of 1332) of the patients with oral cancer had ALDH7A1 allele mutation (rs13182402), one-tenth of the patients with the highest ALDH7A1 expression in the TCGA database were classified as the high-ALDH7A1 group, and the others were classified as the low-ALDH7A1 group. The basic characteristics of these two groups are shown in Table 7. The high-ALDH7A1 group tended to have better clinical outcomes than the low-ALDH7A1 group did (5-year progression-free survival, 58.7% vs. 48.0%, P = 0.048; 5-year overall survival, 49.0% vs. 47.4%, P = 0.412) (Table 7, Figure 2D and 2E). These results indirectly demonstrate that patients with oral cancer and ALDH7A1 rs13182402 mutation have higher ALDH7A1 expression than others do, which might result in less nodal metastasis and better prognostic outcomes.
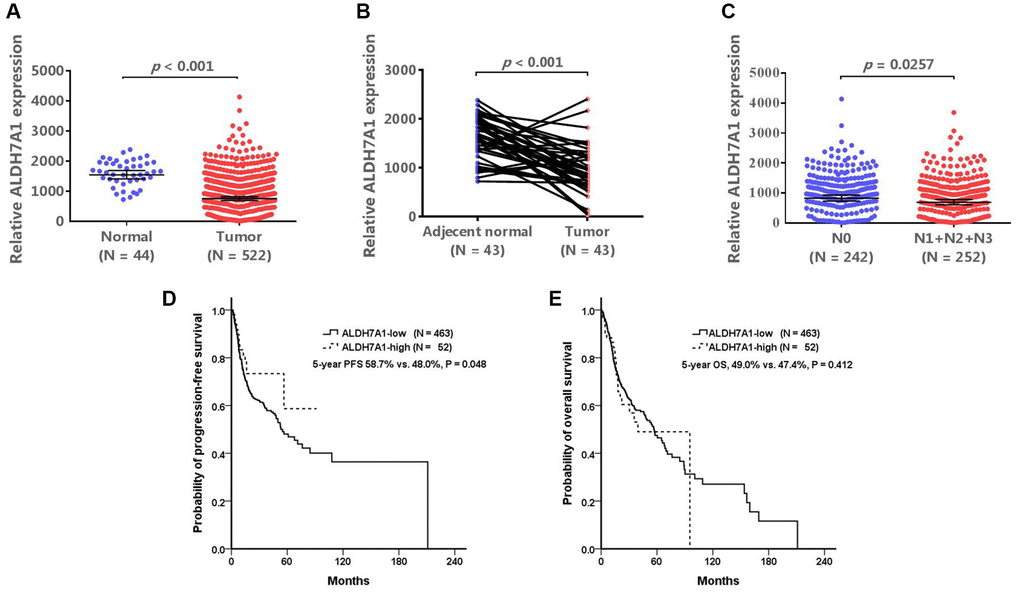
Figure 2. The validated results of ALDH7A1 expression. The Cancer Genome Atlas (TCGA) database (https://www.cbioportal.org/) was used to validate our results. (A, B) In TCGA database, ALDH7A1 expression levels were lower in tumor tissues than those in normal and adjacent normal tissues (P < 0.001, and < 0.001, respectively). ALDH7A1 expression levels were also lower for patients with nodal metastasis than those without nodal metastasis (P < 0.0257) (C). If the patients were divided into ALDH7A1 -high and –low groups, the high-ALDH7A1 group tended to have better clinical outcomes than the low-ALDH7A1 group did (5-year progression-free survival, 58.7% vs. 48.0%, P = 0.048; 5-year overall survival, 49.0% vs. 47.4%, P = 0.412) (D and E).
Table 7. Basic characteristics of high- and low- ALDH7A1 expression patients diagnosed HNSCC from the TCGA database.
| Variable | High ALDH7A1 (N = 52) | Low ALDH7A1 (N = 463) | P value |
| Age (yrs) | |||
| ≧55 | 44 (69.7%) | 322 (69.7%) | 0.015 |
| <55 | 8 (15.4%) | 141 (30.3%) | |
| Pathologic staging | |||
| I + II | 12 (23.1%) | 89 (19.2%) | 0.759 |
| III + IV | 34 (65.4%) | 310 (67.0%) | |
| Unknown | 6 (11.5%) | 64 (13.8%) | |
| Pathologic T staging | |||
| T1 + T2 | 20 (38.5%) | 163 (35.2%) | 0.897 |
| T3 + T4 | 26 (50.0%) | 244 (52.7%) | |
| Unknown | 6 (11.5%) | 56 (12.1%) | |
| Pathologic N staging | |||
| N0 | 21 (40.4%) | 153 (33.0%) | 0.527 |
| N+ | 21 (40.4%) | 221 (47.7%) | |
| Unknown | 10 (19.2%) | 89 (19.2%) | |
| Pathologic M staging | |||
| M0 | 15 (28.8%) | 168 (36.3%) | 0.531 |
| M1 | 0 (0.0%) | 1 (0.2%) | |
| Unknown | 37 (71.2%) | 294 (63.5%) | |
| Histological differentiation | |||
| Well | 8 (15.4%) | 54 (11.7%) | 0.76 |
| Moderate | 28 (53.8%) | 273 (59.0%) | |
| Poor | 13 (25.0%) | 110 (23.8%) | |
| Undifferentiated | 0 (0.0%) | 7 (1.5%) | |
| Unknown | 3 (5.8%) | 19 (4.1%) | |
| 5-year progression free survival | 58.70% | 48.00% | 0.048 |
| 5-year overall survival | 49.00% | 47.40% | 0.412 |
Functional analysis of ALDH7A1 expression in oral cancer cell lines
To further investigate correlations of ALDH7A1 rs13182402 polymorphisms with ALDH7A1 expression levels in oral cancer, we examined rs13182402 genotypes of five oral cancer cell lines (SCC-14, SAS, CA9-22, HSC-3, and OECM-1) and found that SAS cells carried the GG genotype of rs13182402 compared to SCC-14, CA9-22, HSC-3 and OECM-1 cells which carried the AA genotype (Figure 3A, upper panel). Moreover, we detected ALDH7A1 expression by quantitative real time-PCR analysis. Among these oral cancer cell lines, we observed that SAS cells expressed higher ALDH7A1 levels than SCC-14, CA9-22, HSC-3 and OECM-1 cells (Figure 3A, lower panel). Furthermore, SAS cell lines also expressed higher migratory potential than SCC-14, CA9-22, HSC-3 and OECM-1 cells by using Boyden chamber migration assays (Figure 3B).
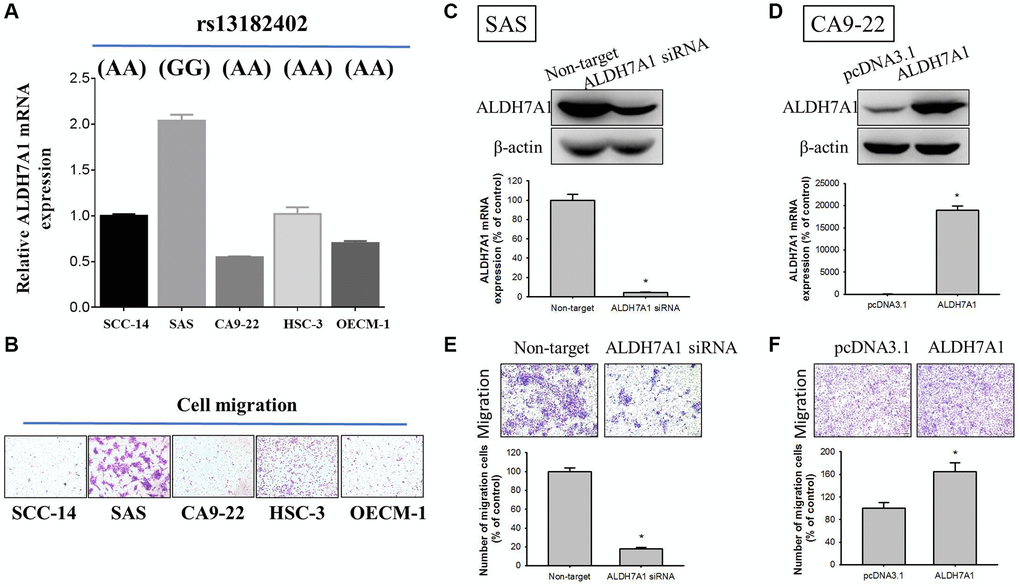
Figure 3. Correlations of ALDH7A1 rs13182402 genotypes with ALDH7A1 mRNA levels in five oral cancer cell lines. (A) Upper panel, ALDH7A1 rs13182402 genotypes in oral cancer cell lines (SCC-14, SAS, CA9-22, HSC-3, and OECM-1) were detected by a TaqMan SNP Genotyping Assay. Lower panel, mRNA level of ALDH7A1 was detected by quantitative real time-PCR analysis. (B) The migratory ability in oral cancer cell lines (SCC-14, SAS, CA9-22, HSC-3, and OECM-1) was detected by Boyden chamber migration assays. (C) Western blot analysis and real time-PCR assay for ALDH7A1 protein and mRNA expressions of SAS cells after siRNA directly against the ALDH7A1 expression were conducted. (D) Western blot analysis and real time-PCR assay for ALDH7A1 protein and mRNA expressions of CA9-22 cells after transfection with vectors containing a constitutively active ALDH7A1 cDNA were conducted. (E and F) Boyden chamber migration assays for cell migratory ability in SAS cells and CA9-22 cells were conducted.
To determine the whether ALDH7A1 influences cellular migration, siRNA directly against the ALDH7A1 expression for SAS cells and transfection with pcDNA vector for overexpression of ALDH7A1 for CA9-22 cells was employed. We confirmed knockdown and overexpression of ALDH7A1 protein and mRNA levels through Western blotting and real time-PCR in SAS and CA9-22 cells, respectively (Figure 3C and 3D). Moreover, by using Boyden chamber migration assays, the results showed that using ALDH7A1 knockdown significantly repressed migratory potential in SAS cells (Figure 3E), whereas overexpression of ALDH7A1 significantly enhanced those potentials in CA9-22 cells (Figure 3F).
Discussion
A total of 2523 participants (1332 patients with oral cancer and 1191 healthy controls) were enrolled in this study. ALDH7A1 polymorphisms did not influence the risk of oral cancer for all participants, alcoholic drinkers, or betel quid chewers. However, ALDH7A1 rs13182402 represented an independent favorable prognostic factor for nodal lymph node metastasis in patients with oral cancer who chewed betel quid. Databases used in validation also indicated that the expression of ALDH7A1 rs13182402 allele mutations was higher in upper aerodigestive (esophagus) mucosa, whole blood, and the musculoskeletal system than the expression of the ALDH7A1 normal type was. ALDH7A1 expression in tumor cells and in patients with advanced cancer status was lower than that in normal tissue and in patients with early-stage disease. Patients with HNSCC who had high ALDH7A1 expression also tended to have superior progression-free survival outcomes compared with those having low ALDH7A1 expression. Future research to further validate these findings is warranted.
Allele frequency of ALDH7A1 rs13182402 in the East Asian population is low. However, some points supported us to pay attention to ALDH7A1 polymorphisms. First, based on the concept of precision medicine, although the incidences of certain genetic alterations were low, the possibility of treatment opinion for these few patients still existed, such as tropomyosin receptor kinase (TRK) inhibitors for the patients with TRK fusion genes, and anaplastic lymphoma kinase (ALK) inhibitor for the patients with ALK-mutant non-small cell lung cancer [26, 27]. Drug development for these small populations was still worth looking forward to. Besides, according to the TCGA database, the patients with high-ALDH7A1 expression tend to have superior outcomes in progression-free survival than those with low-ALDH7A1. The critical issue was how to divide the patients into the high- and low- expression group. Advanced in vivo validations were warranted to identify the cutoff level, which might be helpful to expand the effective population. Finally, several studies reported the importance of ALDH isoenzymes in cancers [2, 13, 28, 29], and ALDH7A1 is a member of the ALDH superfamily. Based on this study, the results provided us with a better understanding of the roles of ALDH in oral cancer, especially ALDH7A1 polymorphism.
Acetaldehyde, a metabolite from ethanol, is metabolized to acetate by ALDH, a process that results in DNA adducts, inhibited DNA repair, and DNA methylation [2]. Several studies have discussed the interaction between ALDH and cancer, especially within the Asian population [2, 13]. Some authors reported that ALDH genes play a role in the maintenance and differentiation of cancer stem cells [30], and others contended that high ALDH expression in cancer stem cells is associated with graver prognostic outcomes [31]. However, the functions of individual ALDH isoenzymes, such as ALDH7A1, have not been clearly ascertained. Wang et al. [10] revealed that ALDH7A1 rs13182402 allele mutation reduces the development of esophageal squamous cell carcinoma (OR [95% CI] = 0.79 [0.67–0.93], P = 0.003). However, Lu et al. [11] suggested that ALDH7A1 rs12659017 mutation advances colorectal cancer (OR [95% CI], 1.09 [1.06–1.12], P < 0.001). The different alleles on the same gene lead to potentially different influences on cancer development. In our study, both ALDH7A1 rs13182402 and rs12659017 were not discovered to constitute risk factors for oral cancer development.
Conversely, the prognostic role of ALDH7A1 in cancer is equivocal. Giacalone et al. [32] demonstrated that in non-small-cell lung cancer, patients with higher ALDH7A1 expression on an immunohistochemical stain experienced lower recurrence-free survival than those with lower ALDH7A1 expression did. Rose et al. [33] also reported that higher ALDH7A1 expression was associated with human nodular melanoma, a melanoma subtype with a higher recurrence rate than that of superficial spreading melanoma. However, high ALDH7A1 expression can play an opposite role in other cancer types. Hoogen et al. [34] revealed that in prostate cancer, ALDH7A1 knockdown reduces intrabone growth and inhibits experimentally induced bone metastasis. Moreover, Busso-Lopes et al. [35] found that low expression of ALDH7A1 in extracellular vesicles from metastatic lymph nodes is correlated with reduced survival in oral cancer patients. Other prognosis-related mechanisms, such as the activity of peroxisome proliferator-activated receptors and DNA methylation, have also been shown to be influenced by ALDH7A1 expression [36–38]. Thus, the influence of ALDH7A1 on prognosis should be evaluated for individual cancer types.
The expression of ALDH7A1 might varies remarkably among different tissues from the published database, such as the GTEx database and TCGA database. In our study, ALDH7A1 rs13182402 allele mutation, which was detected from the whole-blood genomic DNA, was an independent favorable prognostic factor for nodal metastasis in oral cancer. In the GTEx database, this allele mutation was validated in different non-diseased tissue sites and associated with higher ALDH7A1 expression than the normal type in blood. Moreover, oral cancer patient who carry allele mutation (AG) of rs13182402 polymorphism have significantly higher mRNA levels of ALDH7A1 compare to AA genotype. Similarly, in tumor tissue, the high-ALDH7A1 group tended to have better progression-free survival outcomes than the low-ALDH7A1 group did, validated by the TCGA database. And conversely, ALDH7A1 expression in advanced status (patients with nodal metastasis) was lower than that in early status (patients without nodal metastasis). The result supported that ALDH7A1 rs13182402 allele mutation, detected from the whole-blood genomic DNA, was associated with high ALDH7A1 expression and favorable outcomes. Besides, based on our previous study, which indicated that lower ALDH7A1 expression was associated with increased cell proliferation, DNA synthesis, and decreased apoptosis [39], several aspects warrant discussion. First, different allele mutations might result in different functions. Patients with HNSCC and mutant ALDH7A1 (missense mutation, c.1168 G > C, rs121912707) had lower ALDH7A1 expression than those carrying ALDH7A1 wild-type [39], but in the current study, ALDH7A1 rs13182402 mutation led to increased ALDH7A1 expression. Because of the complexity of genotype-phenotype interactions and the fact that the mechanisms of epistatic interaction for different alleles of the same gene are largely unknown [40], future in vitro studies of individual alleles are warranted.
Betel (areca) nut, which has areca alkaloids including arecoline, arecaidine, guvacoline, and guvacine, was found to be implicated in carcinogenesis [41]. However, areca nut, the major component of betel quid, is also considered to lead to angiogenesis and cancer metastasis. Ji et al. [42] suggested that betel nut promotes massive inflammation that supports the proliferation of transforming cells. Subsequently, the vascular endothelial growth factor signaling pathway and angiogenesis are activated, causing cell growth and subsequent metastasis. Several studies have also reported that habitual betel quid chewing is associated with metabolic disorders [43–45]. However, in the TCGA database, low ALDH7A1 expression was correlated with disorders of the metabolic-associated signaling pathways, and the cancer metastasis mechanism might arise through cancer metabolism because of ALDH7A1 mutations [37, 39]. Nevertheless, few studies have discussed the interaction among betel quid chewing, ALDH7A1 expression, and cancer metastasis. Future studies investigating this as well as a potential link with cancer metabolism are warranted.
Several limitations were present in this study. Although less information provided the interactions between the loci and survival outcomes in our cohort, some published databases, such as the TCGA database, indirectly remedied the impact of ALDH7A1 expression on clinical outcomes. In Taiwan, tobacco, alcohol, and betel quid chewing were reported significantly in the development of oral cancer, several studies also mentioned the impact of obesity on cancer development and prognosis. This factor would also be included in our future studies [46–48]. Advanced studies, included individual allele mutations and clinical outcomes which were corresponded to the training and validation cohorts, should be warranted in the future. Furthermore, more detailed allele information of the patients enrolled in TCGA was unavailable. Moreover, due to the complex epistatic interaction between different alleles of the same gene [40], determining whether gain or loss of function occurred in each ALDH7A1 allele is problematic. Although patients with oral cancer who had lower ALDH7A1 expression had poorer prognoses than those with higher expression did, individual allele functions should be validated in vitro. Finally, few studies have discussed the interaction between betel quid chewing, ALDH7A1 expression, and cancer metastasis. Thus, more experiments in this area are also necessary.
In conclusion, this study reported that ALDH7A1 SNPs, detected from the whole-blood genomic DNA, did not affect the risk of oral cancer. But ALDH7A1 rs13182402 mutation was an independent favorable prognostic factor for neck lymph node metastasis in the patients who used betel quid. In addition, the published database showed that ALDH7A1 rs13182402 mutation in whole blood coexisted with high ALDH7A1 expression. And patients with higher ALDH7A1 expression seemed to have superior prognoses than those with lower expression do. It hinted ALDH7A1 rs13182402 mutation, associated with high ALDH7A1 expression, might be a favorable prognostic factor for patients with oral cancer. Future validations in vitro and in vivo are warranted.
Materials and Methods
Study subjects
Patients diagnosed as having oral cancer at Chung Shan Medical University Hospital and Changhua Christian Hospital between 2007 and 2019 were enrolled into the case group. Moreover, healthy participants without a cancer history were enrolled from Taiwan Biobank as a control group. For the case group, all patients included were pathological diagnostic oral cancer. In Taiwan, because more than 90% of oral cancer patients were male [13, 49], females were excluded due to a rare population. The patients who were no pathological diagnosis, cytologic diagnosis only, and second primary malignancies were also excluded. Healthy participants were included between 30- to 70-year-old and had normal mental capacity. The participants who were female or diagnosed with malignancies were excluded. Clinical information, including age, pathologic staging, and any habits of chewing betel quid, smoking cigarettes, or drinking alcohol, was collected according to the medical records. All patients were staged according to the American Joint Committee on Cancer’s staging system (seventh edition) [50]. This study was approved by the Institutional Review Board of Chung Shan Medical University Hospital (CSMUH No: CS15125 and CS1-21151).
Oral cancer cell lines and culture
The human SAS, CA9-22 and HSC-3 cell lines were purchased from and validated by the Japanese Collection of Research Bioresources Cell Bank (JCRB, Osaka, Japan). SCC-14 cells lines were purchased from were obtained from Cell Lines Service (CLS; Eppelheim, Germany). The OECM-1 cell line derived from a male Taiwanese patient [51] was maintained in RPMI-1640 medium with 10% FBS. All cells were cultured and maintained at 37°C in a 5% CO2 and 95% air atmosphere.
DNA extraction and genotyping
Whole-blood specimens were collected and placed in sterile tubes containing ethylene diamine tetraacetic acid. These specimens were immediately centrifuged and then stored at −80°C. Genomic DNA was extracted from peripheral blood leukocytes by using QIAamp DNA blood mini kits (Qiagen, Valencia, CA, USA) according to previously described publication [52, 53] and then dissolved the extracts into pH 7.8 TE buffer (10 mM trisaminomethane and 1 mM ethylene diamine tetraacetic acid; pH 7.8) and then quantified by measuring the optical density at 260 nm. The final product was stored at −20°C and used as a template for polymerase chain reaction. Two ALDH7A1 genetic polymorphism rs13182402 and rs12659017 were detected in previous study and International HapMap Project database [7]. Moreover, ALDH7A1 rs13182402 and rs12659017 polymorphism were reported significantly in malignant diseases, such as esophageal squamous cell carcinoma, osteoporosis, and colorectal cancer [7, 10, 11]. But the roles of ALDH7A1 polymorphisms in oral cancer were unknown. Therefore, we chose these two candidate loci in our study. Assessment of allelic discrimination for ALDH7A1 rs13182402 (assay IDs: C__31889488_10) and rs12659017 (assay IDs: C_32255284_10) SNPs was performed using a TaqMan assay with an Applied Biosystems StepOne Real-Time Polymerase Chain Reaction System (Applied Biosystems, Foster City, CA, USA). The results were further analyzed using SDS version 3.0. The details of DNA extraction and genotyping were published in our previous study [54].
RNA preparation and quantitative real-time PCR
Total RNA was isolated from oral cancer cell lines and oral cancer tissues using RNeasy Mini Kit (Qiagen, Valencia, CA, USA) according to previously described [55, 56]. Quantitative real-time PCR analysis was performed using TaqMan one-step PCR Master Mix (Applied Biosystems) as previously described [57].
Cell migration assay
Five oral cancer cell lines (SCC-14, SAS, CA9-22, HSC-3, and OECM-1) cell migration was evaluated as described previously [58–61]. Briefly, after 48-hours treatment with siRNA or other manipulations, migration responses of SAS cell or other cell lines were assessed in a Boyden chamber assay with cell culture inserts of diameter 6.5-mm and pore size 8 μm (Neuro Probe) at 24-hours incubation.
Published databases for validation
In this study, several published databases were used to validate our results. dbSNP, a public-domain archive housing a broad collection of simple genetic polymorphisms, includes the sequence context and frequency of the polymorphism [62]. GTEx Portal, a comprehensive public resource for studying tissue-specific gene expression and regulation, provides gene expression, quantitative trait loci, and histology images for nearly 1000 individuals registered at 54 non-diseased tissue sites [63]. TCGA database was downloaded from cBioPortal, an open-access resource providing more than 5000 tumor samples from 20 cancer studies [64].
Statistical analysis
The correlations between the clinicopathological parameters were analyzed by using the Chi-square test. And Hardy Weinberg test was done to detect the population representation of genotypes of the two loci. The adjusted odds ratio (AOR)-with 95% CIs of the association between genotype frequency and oral cancer risk and clinical pathological characteristics—were measured using multiple logistic regression models after controlling for covariates. The variables with P values of <0.05 in univariate analyses were enrolled into the multivariate analysis. SPSS (version 21.0, SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Author Contributions
HJL, CWL and SFY contributed to the concept and design, drafted the manuscript, and critically revised the manuscript; HJL, CYC, MKC, KML and SFY contributed to collect the sample and data. CWS, WEY, CMY and CHT contributed to perform the experiments, and analyzed the data. All authors read and agreed to the published version of the manuscript.
Acknowledgments
We would like to thank the Human Biobank of Chung Shan Medical University Hospital for providing the biological specimen and related clinical data for our research.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This study was supported by research grants from the Chung Shan Medical University Hospital, Taiwan (CSH-2020-D-009) to Hsueh-Ju Lu.
References
- 1. Jackson B, Brocker C, Thompson DC, Black W, Vasiliou K, Nebert DW, Vasiliou V. Update on the aldehyde dehydrogenase gene (ALDH) superfamily. Hum Genomics. 2011; 5:283–303. https://doi.org/10.1186/1479-7364-5-4-283 [PubMed]
- 2. Seitz HK, Stickel F. Acetaldehyde as an underestimated risk factor for cancer development: role of genetics in ethanol metabolism. Genes Nutr. 2010; 5:121–8. https://doi.org/10.1007/s12263-009-0154-1 [PubMed]
- 3. Marchitti SA, Brocker C, Stagos D, Vasiliou V. Non-P450 aldehyde oxidizing enzymes: the aldehyde dehydrogenase superfamily. Expert Opin Drug Metab Toxicol. 2008; 4:697–720. https://doi.org/10.1517/17425255.4.6.697 [PubMed]
- 4. Skvorak AB, Robertson NG, Yin Y, Weremowicz S, Her H, Bieber FR, Beisel KW, Lynch ED, Beier DR, Morton CC. An ancient conserved gene expressed in the human inner ear: identification, expression analysis, and chromosomal mapping of human and mouse antiquitin (ATQ1). Genomics. 1997; 46:191–9. https://doi.org/10.1006/geno.1997.5026 [PubMed]
- 5. Mills PB, Struys E, Jakobs C, Plecko B, Baxter P, Baumgartner M, Willemsen MA, Omran H, Tacke U, Uhlenberg B, Weschke B, Clayton PT. Mutations in antiquitin in individuals with pyridoxine-dependent seizures. Nat Med. 2006; 12:307–9. https://doi.org/10.1038/nm1366 [PubMed]
- 6. Chan CL, Wong JW, Wong CP, Chan MK, Fong WP. Human antiquitin: structural and functional studies. Chem Biol Interact. 2011; 191:165–70. https://doi.org/10.1016/j.cbi.2010.12.019 [PubMed]
- 7. Guo Y, Tan LJ, Lei SF, Yang TL, Chen XD, Zhang F, Chen Y, Pan F, Yan H, Liu X, Tian Q, Zhang ZX, Zhou Q, et al. Genome-wide association study identifies ALDH7A1 as a novel susceptibility gene for osteoporosis. PLoS Genet. 2010; 6:e1000806. https://doi.org/10.1371/journal.pgen.1000806 [PubMed]
- 8. Sorolla MA, Rodríguez-Colman MJ, Vall-Llaura N, Vived C, Fernández-Nogales M, Lucas JJ, Ferrer I, Cabiscol E. Impaired PLP-dependent metabolism in brain samples from Huntington disease patients and transgenic R6/1 mice. Metab Brain Dis. 2016; 31:579–86. https://doi.org/10.1007/s11011-015-9777-7 [PubMed]
- 9. Yang JS, Hsu JW, Park SY, Lee SY, Li J, Bai M, Alves C, Tseng W, Michelet X, Ho IC, Hsu VW. ALDH7A1 inhibits the intracellular transport pathways during hypoxia and starvation to promote cellular energy homeostasis. Nat Commun. 2019; 10:4068. https://doi.org/10.1038/s41467-019-11932-0 [PubMed]
- 10. Wang H, Tong L, Wei J, Pan W, Li L, Ge Y, Zhou L, Yuan Q, Zhou C, Yang M. The ALDH7A1 genetic polymorphisms contribute to development of esophageal squamous cell carcinoma. Tumour Biol. 2014; 35:12665–70. https://doi.org/10.1007/s13277-014-2590-9 [PubMed]
- 11. Lu Y, Kweon SS, Tanikawa C, Jia WH, Xiang YB, Cai Q, Zeng C, Schmit SL, Shin A, Matsuo K, Jee SH, Kim DH, Kim J, et al. Large-Scale Genome-Wide Association Study of East Asians Identifies Loci Associated With Risk for Colorectal Cancer. Gastroenterology. 2019; 156:1455–66. https://doi.org/10.1053/j.gastro.2018.11.066 [PubMed]
- 12. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020; 70:7–30. https://doi.org/10.3322/caac.21590 [PubMed]
- 13. Koyanagi YN, Ito H, Oze I, Hosono S, Tanaka H, Abe T, Shimizu Y, Hasegawa Y, Matsuo K. Development of a prediction model and estimation of cumulative risk for upper aerodigestive tract cancer on the basis of the aldehyde dehydrogenase 2 genotype and alcohol consumption in a Japanese population. Eur J Cancer Prev. 2017; 26:38–47. https://doi.org/10.1097/CEJ.0000000000000222 [PubMed]
- 14. Ferris RL, Blumenschein G
Jr , Fayette J, Guigay J, Colevas AD, Licitra L, Harrington K, Kasper S, Vokes EE, Even C, Worden F, Saba NF, Iglesias Docampo LC, et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N Engl J Med. 2016; 375:1856–67. https://doi.org/10.1056/NEJMoa1602252 [PubMed] - 15. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G
Jr , Psyrri A, Basté N, Neupane P, Bratland Å, Fuereder T, Hughes BGM, Mesía R, et al, and KEYNOTE-048 Investigators. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019; 394:1915–28. https://doi.org/10.1016/S0140-6736(19)32591-7 [PubMed] - 16. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre JL, Greiner RH, Giralt J, Maingon P, Rolland F, Bolla M, Cognetti F, Bourhis J, Kirkpatrick A, van Glabbeke M, and European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004; 350:1945–52. https://doi.org/10.1056/NEJMoa032641 [PubMed]
- 17. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, Kish JA, Kim HE, Cmelak AJ, Rotman M, Machtay M, Ensley JF, Chao KS, et al, and Radiation Therapy Oncology Group 9501/Intergroup. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004; 350:1937–44. https://doi.org/10.1056/NEJMoa032646 [PubMed]
- 18. Kamps R, Brandão RD, Bosch BJ, Paulussen AD, Xanthoulea S, Blok MJ, Romano A. Next-Generation Sequencing in Oncology: Genetic Diagnosis, Risk Prediction and Cancer Classification. Int J Mol Sci. 2017; 18:308. https://doi.org/10.3390/ijms18020308 [PubMed]
- 19. Meldrum C, Doyle MA, Tothill RW. Next-generation sequencing for cancer diagnostics: a practical perspective. Clin Biochem Rev. 2011; 32:177–95. [PubMed]
- 20. Gagan J, Van Allen EM. Next-generation sequencing to guide cancer therapy. Genome Med. 2015; 7:80. https://doi.org/10.1186/s13073-015-0203-x [PubMed]
- 21. Su SC, Chang LC, Lin CW, Chen MK, Yu CP, Chung WH, Yang SF. Mutational signatures and mutagenic impacts associated with betel quid chewing in oral squamous cell carcinoma. Hum Genet. 2019; 138:1379–89. https://doi.org/10.1007/s00439-019-02083-9 [PubMed]
- 22. Yang SF, Lin CW, Chuang CY, Lee YC, Chung WH, Lai HC, Chang LC, Su SC. Host Genetic Associations with Salivary Microbiome in Oral Cancer. J Dent Res. 2022; 101:590–8. https://doi.org/10.1177/00220345211051967 [PubMed]
- 23. Su SC, Hsieh MJ, Lin CW, Chuang CY, Liu YF, Yeh CM, Yang SF. Impact of HOTAIR Gene Polymorphism and Environmental Risk on Oral Cancer. J Dent Res. 2018; 97:717–24. https://doi.org/10.1177/0022034517749451 [PubMed]
- 24. Su SC, Lin CW, Liu YF, Fan WL, Chen MK, Yu CP, Yang WE, Su CW, Chuang CY, Li WH, Chung WH, Yang SF. Exome Sequencing of Oral Squamous Cell Carcinoma Reveals Molecular Subgroups and Novel Therapeutic Opportunities. Theranostics. 2017; 7:1088–99. https://doi.org/10.7150/thno.18551 [PubMed]
- 25. Yang SF, Huang HD, Fan WL, Jong YJ, Chen MK, Huang CN, Chuang CY, Kuo YL, Chung WH, Su SC. Compositional and functional variations of oral microbiota associated with the mutational changes in oral cancer. Oral Oncol. 2018; 77:1–8. https://doi.org/10.1016/j.oraloncology.2017.12.005 [PubMed]
- 26. Drilon A, Laetsch TW, Kummar S, DuBois SG, Lassen UN, Demetri GD, Nathenson M, Doebele RC, Farago AF, Pappo AS, Turpin B, Dowlati A, Brose MS, et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N Engl J Med. 2018; 378:731–9. https://doi.org/10.1056/NEJMoa1714448 [PubMed]
- 27. Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó L, Ahn MJ, De Pas T, Besse B, Solomon BJ, Blackhall F, Wu YL, Thomas M, O'Byrne KJ, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013; 368:2385–94. https://doi.org/10.1056/NEJMoa1214886 [PubMed]
- 28. Januchowski R, Wojtowicz K, Zabel M. The role of aldehyde dehydrogenase (ALDH) in cancer drug resistance. Biomed Pharmacother. 2013; 67:669–80. https://doi.org/10.1016/j.biopha.2013.04.005 [PubMed]
- 29. Marcato P, Dean CA, Giacomantonio CA, Lee PW. Aldehyde dehydrogenase: its role as a cancer stem cell marker comes down to the specific isoform. Cell Cycle. 2011; 10:1378–84. https://doi.org/10.4161/cc.10.9.15486 [PubMed]
- 30. Clark DW, Palle K. Aldehyde dehydrogenases in cancer stem cells: potential as therapeutic targets. Ann Transl Med. 2016; 4:518. https://doi.org/10.21037/atm.2016.11.82 [PubMed]
- 31. Pors K, Moreb JS. Aldehyde dehydrogenases in cancer: an opportunity for biomarker and drug development? Drug Discov Today. 2014; 19:1953–63. https://doi.org/10.1016/j.drudis.2014.09.009 [PubMed]
- 32. Giacalone NJ, Den RB, Eisenberg R, Chen H, Olson SJ, Massion PP, Carbone DP, Lu B. ALDH7A1 expression is associated with recurrence in patients with surgically resected non-small-cell lung carcinoma. Future Oncol. 2013; 9:737–45. https://doi.org/10.2217/fon.13.19 [PubMed]
- 33. Rose AE, Poliseno L, Wang J, Clark M, Pearlman A, Wang G, Vega Y Saenz de Miera EC, Medicherla R, Christos PJ, Shapiro R, Pavlick A, Darvishian F, Zavadil J, et al. Integrative genomics identifies molecular alterations that challenge the linear model of melanoma progression. Cancer Res. 2011; 71:2561–71. https://doi.org/10.1158/0008-5472.CAN-10-2958 [PubMed]
- 34. van den Hoogen C, van der Horst G, Cheung H, Buijs JT, Pelger RC, van der Pluijm G. The aldehyde dehydrogenase enzyme 7A1 is functionally involved in prostate cancer bone metastasis. Clin Exp Metastasis. 2011; 28:615–25. https://doi.org/10.1007/s10585-011-9395-7 [PubMed]
- 35. Busso-Lopes AF, Carnielli CM, Winck FV, Patroni FMS, Oliveira AK, Granato DC, E Costa RAP, Domingues RR, Pauletti BA, Riaño-Pachón DM, Aricetti J, Caldana C, Graner E, et al. A Reductionist Approach Using Primary and Metastatic Cell-Derived Extracellular Vesicles Reveals Hub Proteins Associated with Oral Cancer Prognosis. Mol Cell Proteomics. 2021; 20:100118. https://doi.org/10.1016/j.mcpro.2021.100118 [PubMed]
- 36. Pommergaard HC, Preuss Hasselby J, Linno Willemoe G, Ralbovska A, Arendtsen Rostved A, Rasmussen A, Aagaard Schultz N, Hillingsø J, Nørgaard Larsen P, Kugler JM. Peroxisome proliferator-activated receptor activity correlates with poor survival in patients resected for hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2021; 28:327–35. https://doi.org/10.1002/jhbp.745 [PubMed]
- 37. Andrejeva D, Kugler JM, Nguyen HT, Malmendal A, Holm ML, Toft BG, Loya AC, Cohen SM. Metabolic control of PPAR activity by aldehyde dehydrogenase regulates invasive cell behavior and predicts survival in hepatocellular and renal clear cell carcinoma. BMC Cancer. 2018; 18:1180. https://doi.org/10.1186/s12885-018-5061-7 [PubMed]
- 38. Hata A, Nakajima T, Matsusaka K, Fukuyo M, Morimoto J, Yamamoto T, Sakairi Y, Rahmutulla B, Ota S, Wada H, Suzuki H, Matsubara H, Yoshino I, Kaneda A. A low DNA methylation epigenotype in lung squamous cell carcinoma and its association with idiopathic pulmonary fibrosis and poorer prognosis. Int J Cancer. 2020; 146:388–99. https://doi.org/10.1002/ijc.32532 [PubMed]
- 39. Lu HJ, Hsieh CC, Yeh CC, Yeh YC, Wu CC, Wang FS, Lai JM, Yang MH, Wang CH, Huang CF, Chang PM. Clinical, pathophysiologic, and genomic analysis of the outcomes of primary head and neck malignancy after pulmonary metastasectomy. Sci Rep. 2019; 9:12913. https://doi.org/10.1038/s41598-019-49212-y [PubMed]
- 40. Xu L, Barker B, Gu Z. Dynamic epistasis for different alleles of the same gene. Proc Natl Acad Sci U S A. 2012; 109:10420–5. https://doi.org/10.1073/pnas.1121507109 [PubMed]
- 41. Lin YS, Jen YM, Wang BB, Lee JC, Kang BH. Epidemiology of oral cavity cancer in taiwan with emphasis on the role of betel nut chewing. ORL J Otorhinolaryngol Relat Spec. 2005; 67:230–6. https://doi.org/10.1159/000089214 [PubMed]
- 42. Ji WT, Chuang YC, Chen HP, Lee CC, Chen JY, Yang SR, Chen JH, Wang CJ, Chen HR. Areca nut extracts exert different effects in oral cancer cells depending on serum concentration: A clue to the various oral alterations in betel quid chewers. Toxicol Rep. 2014; 1:1087–95. https://doi.org/10.1016/j.toxrep.2014.10.018 [PubMed]
- 43. Lee BJ, Chan MY, Hsiao HY, Chang CH, Hsu LP, Lin PT. Relationship of Oxidative Stress, Inflammation, and the Risk of Metabolic Syndrome in Patients with Oral Cancer. Oxid Med Cell Longev. 2018; 2018:9303094. https://doi.org/10.1155/2018/9303094 [PubMed]
- 44. Shafique K, Zafar M, Ahmed Z, Khan NA, Mughal MA, Imtiaz F. Areca nut chewing and metabolic syndrome: evidence of a harmful relationship. Nutr J. 2013; 12:67. https://doi.org/10.1186/1475-2891-12-67 [PubMed]
- 45. Yamada T, Hara K, Kadowaki T. Chewing betel quid and the risk of metabolic disease, cardiovascular disease, and all-cause mortality: a meta-analysis. PLoS One. 2013; 8:e70679. https://doi.org/10.1371/journal.pone.0070679 [PubMed]
- 46. Lee YA, Li S, Chen Y, Li Q, Chen CJ, Hsu WL, Lou PJ, Zhu C, Pan J, Shen H, Ma H, Cai L, He B, et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck. 2019; 41:92–102. https://doi.org/10.1002/hed.25383 [PubMed]
- 47. Iyengar NM, Kochhar A, Morris PG, Morris LG, Zhou XK, Ghossein RA, Pino A, Fury MG, Pfister DG, Patel SG, Boyle JO, Hudis CA, Dannenberg AJ. Impact of obesity on the survival of patients with early-stage squamous cell carcinoma of the oral tongue. Cancer. 2014; 120:983–91. https://doi.org/10.1002/cncr.28532 [PubMed]
- 48. Scully T, Ettela A, LeRoith D, Gallagher EJ. Obesity, Type 2 Diabetes, and Cancer Risk. Front Oncol. 2021; 10:615375. https://doi.org/10.3389/fonc.2020.615375 [PubMed]
- 49. Lu HJ, Tseng SW, Peng CY, Tseng HC, Hsin CH, Chen HL, Huang WS, Wu MF, Yang MH, Chang PM. Predictors of early progression after curative resection followed by platinum-based adjuvant chemoradiotherapy in oral cavity squamous cell carcinoma. Postgrad Med. 2021; 133:377–84. https://doi.org/10.1080/00325481.2020.1809869 [PubMed]
- 50. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010; 17:1471–4. https://doi.org/10.1245/s10434-010-0985-4 [PubMed]
- 51. Yang CY, Meng CL. Regulation of PG synthase by EGF and PDGF in human oral, breast, stomach, and fibrosarcoma cancer cell lines. J Dent Res. 1994; 73:1407–15. https://doi.org/10.1177/00220345940730080301 [PubMed]
- 52. Chung TT, Pan MS, Kuo CL, Wong RH, Lin CW, Chen MK, Yang SF. Impact of RECK gene polymorphisms and environmental factors on oral cancer susceptibility and clinicopathologic characteristics in Taiwan. Carcinogenesis. 2011; 32:1063–8. https://doi.org/10.1093/carcin/bgr083 [PubMed]
- 53. Hsiao PC, Chen MK, Su SC, Ueng KC, Chen YC, Hsieh YH, Liu YF, Tsai HT, Yang SF. Hypoxia inducible factor-1alpha gene polymorphism G1790A and its interaction with tobacco and alcohol consumptions increase susceptibility to hepatocellular carcinoma. J Surg Oncol. 2010; 102:163–9. https://doi.org/10.1002/jso.21539 [PubMed]
- 54. Chou CH, Chang CY, Lu HJ, Hsin MC, Chen MK, Huang HC, Yeh CM, Lin CW, Yang SF. IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer. Int J Mol Sci. 2020; 21:5662. https://doi.org/10.3390/ijms21165662 [PubMed]
- 55. Su CW, Chang YC, Chien MH, Hsieh YH, Chen MK, Lin CW, Yang SF. Loss of TIMP3 by promoter methylation of Sp1 binding site promotes oral cancer metastasis. Cell Death Dis. 2019; 10:793. https://doi.org/10.1038/s41419-019-2016-0 [PubMed]
- 56. Su SC, Chang LC, Huang HD, Peng CY, Chuang CY, Chen YT, Lu MY, Chiu YW, Chen PY, Yang SF. Oral microbial dysbiosis and its performance in predicting oral cancer. Carcinogenesis. 2021; 42:127–35. https://doi.org/10.1093/carcin/bgaa062 [PubMed]
- 57. Hsin MC, Hsieh YH, Wang PH, Ko JL, Hsin IL, Yang SF. Hispolon suppresses metastasis via autophagic degradation of cathepsin S in cervical cancer cells. Cell Death Dis. 2017; 8:e3089. https://doi.org/10.1038/cddis.2017.459 [PubMed]
- 58. Su SC, Yeh CM, Lin CW, Hsieh YH, Chuang CY, Tang CH, Lee YC, Yang SF. A novel melatonin-regulated lncRNA suppresses TPA-induced oral cancer cell motility through replenishing PRUNE2 expression. J Pineal Res. 2021; 71:e12760. https://doi.org/10.1111/jpi.12760 [PubMed]
- 59. Chu YH, Su CW, Hsieh YS, Chen PN, Lin CW, Yang SF. Carbonic Anhydrase III Promotes Cell Migration and Epithelial-Mesenchymal Transition in Oral Squamous Cell Carcinoma. Cells. 2020; 9:E704. https://doi.org/10.3390/cells9030704 [PubMed]
- 60. Yang WE, Ho YC, Tang CM, Hsieh YS, Chen PN, Lai CT, Yang SF, Lin CW. Duchesnea indica extract attenuates oral cancer cells metastatic potential through the inhibition of the matrix metalloproteinase-2 activity by down-regulating the MEK/ERK pathway. Phytomedicine. 2019; 63:152960. https://doi.org/10.1016/j.phymed.2019.152960 [PubMed]
- 61. Yeh CM, Hsieh MJ, Yang JS, Yang SF, Chuang YT, Su SC, Liang MY, Chen MK, Lin CW. Geraniin inhibits oral cancer cell migration by suppressing matrix metalloproteinase-2 activation through the FAK/Src and ERK pathways. Environ Toxicol. 2019; 34:1085–93. https://doi.org/10.1002/tox.22809 [PubMed]
- 62. Sherry ST, Ward MH, Kholodov M, Baker J, Phan L, Smigielski EM, Sirotkin K. dbSNP: the NCBI database of genetic variation. Nucleic Acids Res. 2001; 29:308–11. https://doi.org/10.1093/nar/29.1.308 [PubMed]
- 63. Carithers LJ, Moore HM. The Genotype-Tissue Expression (GTEx) Project. Biopreserv Biobank. 2015; 13:307–8. https://doi.org/10.1089/bio.2015.29031.hmm [PubMed]
- 64. Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E, Antipin Y, Reva B, Goldberg AP, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012; 2:401–4. https://doi.org/10.1158/2159-8290.CD-12-0095 [PubMed]