



Introduction
Among various cancers, Lung cancer was the most incident and lethal malignant tumor worldwide [1]. Lung cancer could be split into two categories: small cell lung cancer (SCLC, 15%) and NSCLC (85%) [2]. Although the efficacy of treatment for advanced NSCLC remains poor, the prognosis of NSCLC increased gradually during recent years because of the ICIs [3–6]. ICIs have shown convincing clinical benefits, significantly prolonging the survival of advanced NSCLC patients. However, the response rate of NSCLC with ICIs is only about 20%, indicating that most NSCLC patients failed to respond to ICIs [7]. In clinical application, it is the greatest challenge to be found potential biomarkers to predict the efficacy of ICIs treatment and find the appropriate population. Therefore, it is extremely important to estimate biomarkers to identify advanced NSCLC patients who may respond to ICIs.
At present, there are some biomarkers related to ICIs that have been approved by many clinical trials, including PD-L1 expression, TMB, and MSI-H [8, 9]. Most clinical trials have shown increased response rates and prognosis in NSCLC with higher PD-L1 expression, but enrichment of responses is incomplete [9, 10]. Only PD-L1 expression is insufficient to meet the accuracy requirements of clinical application in NSCLC. Moreover, there is still a lack of standardization and consistency in PD-L1 detection methods. Nowadays, TMB has been regarded as an independent predictive biomarker of response to ICIs in many cancers, including NSCLC [11–13]. For most cancers, high TMB is related to improved survival in patients with ICIs treatment, but there has not been an internationally accepted definition of high TMB at present [14]. Moreover, several potential biomarkers have been reported in numerous studies, including tumor-infiltrating lymphocytes, gut microbiota, tumor driver gene mutation, and so on [15, 16]. Besides that, some clinical indicators of advanced NSCLC patients can also be used to predict the prognosis of immunotherapy. ICIs have been significantly less successful in never-smokers, including EGFR-mutated, ALK-rearranged, and other rarer oncogenic drivers of NSCLC [17, 18]. With the increasing routine of NGS in clinical practice, it is essential to integrate various clinical indicators and genome data to develop a prognostic nomogram for predicting the clinical outcomes (including PFS and OS) in patients receiving ICIs.
In this study, genomic and clinical data of advanced NSCLC treated with ICIs were downloaded from cBioPortal [12, 13, 19, 20]. Subsequently, we compared the top 20 gene alterations between the DCB and NDB groups. The correlation between the gene mutation and TIICs and TMB was investigated by TCGA cohort. Finally, two novel nomograms based on the clinicopathological features and mutational data were built to predict the PFS and OS in advanced NSCLC with ICIs.
Materials and Methods
Data download
Three ICIs cohorts of advanced NSCLC with immunotherapy were obtained from cBioPortal. The first cohort (MSK, J Clin Oncol 2018) consisted of targeted NGS of 240 advanced NSCLC with anti-PD-(L)1 monotherapy or in combination with anti–CTLA-4 [19]. The second cohort (MSK, Science 2015) collected genomic and survival data of 16 advanced NSCLC with anti-PD-1 monotherapy [12]. The third cohort (MSKCC, Nat Genet 2019) consisted of 350 advanced NSCLC patients with anti-PD-(L)1 as monotherapy or in combination [13]. The efficacy of immunotherapy was assessed by RECIST version 1.1. Moreover, DCB was defined as CR/PR/SD that lasted > 6 months, and NDB was defined as PD or SD that lasted ≤ 6 months [21]. PFS was defined as the time from the initiation of immunotherapy to disease progression or death. OS was defined as the time from the initiation of immunotherapy to date of death or last follow-up. PD-L1 negative, weak, and strong were defined as the PD-L1 expression < 0, 50 > PD-L1 expression ≥ 1, and PD-L1 expression ≥ 50, respectively. The first and second ICIs cohorts contained PFS of advanced NSCLC, and the third cohort contained OS data. All clinical studies reported the assessment of TMB. Besides that, we conducted a comprehensive analysis of gene mutations and survival data of LUAD and LUSC cohorts from the TCGA database. cBioPortal data were shown in Supplementary Table 1.
Construction of nomogram
Survival analyses were conducted using the Kaplan-Meier plot method and selected clinical variables to develop a novel nomogram. Based on the patient’s clinical data and other information, nomograms can predict the likelihood of an event, including PFS, OS, and recurrence. In this work, the construction of the nomogram was based on clinicopathological information and mutational data. The “rms” package, which stands for Regression Modeling Strategies, is a collection of functions that facilitates and simplifies regression modeling, testing, estimation, validation, plotting, prediction, and presentation by incorporating enhanced model design attributes. The “rms” package serves as a valuable tool for assisting and streamlining the modeling process. And the R package rms was used to construct the nomogram. And the predictive accuracy and discriminative value of nomogram mainly included the concordance index (C-index), calibration curve, and ROC curve.
Bioinformatic analysis
GO is a common technique for studying the biological function of genetic data, which mainly includes biological process, cellular component, and molecular function [22]. KEGG database collects genomic, chemical, and systematic functional information [23]. In this study, GO and KEGG enrichment analyses were performed to top 20 mutation gene functional annotations using the R package clusterProfiler.
The gene mutation, gene expression, and clinical data of LUAD and LUSC were obtained from TCGA database. The TMB score was further calculated for each sample. According to the comparison between single gene mutation group and wild group, the different degree of whole genes was obtained, which was performed by the gene set enrichment analysis (GSEA). In addition, the relative abundance of TIICs in NSCLC was determined by converting the genes expression into the fraction of immune cells.
Verification of the prognostic significance of gene
External validation of the prognostic significance of gene was performed by another ICIs cohort (MSK, Cancer Cell 2018). This cohort consisted of 75 NSCLC with anti-PD-1 combination with anti–CTLA-4 [20].
Statistical analyses
In this work, GraphPad Prism 9.0 and R 4.2.2 were used for statistical analyses. One-way Student’s t tests were used to determine statistical significance. Survival analyses were performed using the Kaplan-Meier plot method and compared using the log-rank test. And P-value< 0.05 indicating statistically significant.
Availability of data and materials
All data included in this study are available including cBioPortal of Cancer Genomics ([MSK, J Clin Oncol 2018], [MSK, Science 2015], [MSKCC, Nat Genet 2019], [MSK, Cancer Cell 2018]) and TCGA database.
Results
Gene alterations associated with DCB
The top 20 gene alterations in DCB group include TP53, KRAS, KEAP1, PTPRT, PTPRD, STK11, MLL3, FAT1, SMARCA4, EPHA5, EPHA3, TERT, NF1, MGA, ERBB4, ATRX, ARID1A, PIK3CG, PIK3C2G, PGR (Figure 1A). We also examined those gene alterations in NDB group (Figure 1B). TMB (P = 0.0009) and PFS (P < 0.0001) were higher in DCB than NDB (Figure 1C). In addition, there are some clinicopathological variables were closely related to the PFS of ICIs including TMB (P = 0.0101, HR = 1.419 (1.081 – 1.862)), PD-L1 expression (P = 0.0062, HR = 1.799 (1.139 – 2.842)), line of treatment (P = 0.0058, HR = 1.574 (1.171 – 2.116)), smoking status (P = 0.0102, HR = 1.529 (1.045 –2.239)), and treatment type (P = 0.0009, HR = 1.969 (1.407 – 2.754)) (Figure 1D–1H). Moreover, treatment type (P value = 0.0093, HR = 1.913 (1.173 – 3.119)) was significantly related to the OS in advanced NSCLC patients with ICIs treatment (Figure 1I). And patient characteristics with NDB and DCB groups were shown in Table 1.
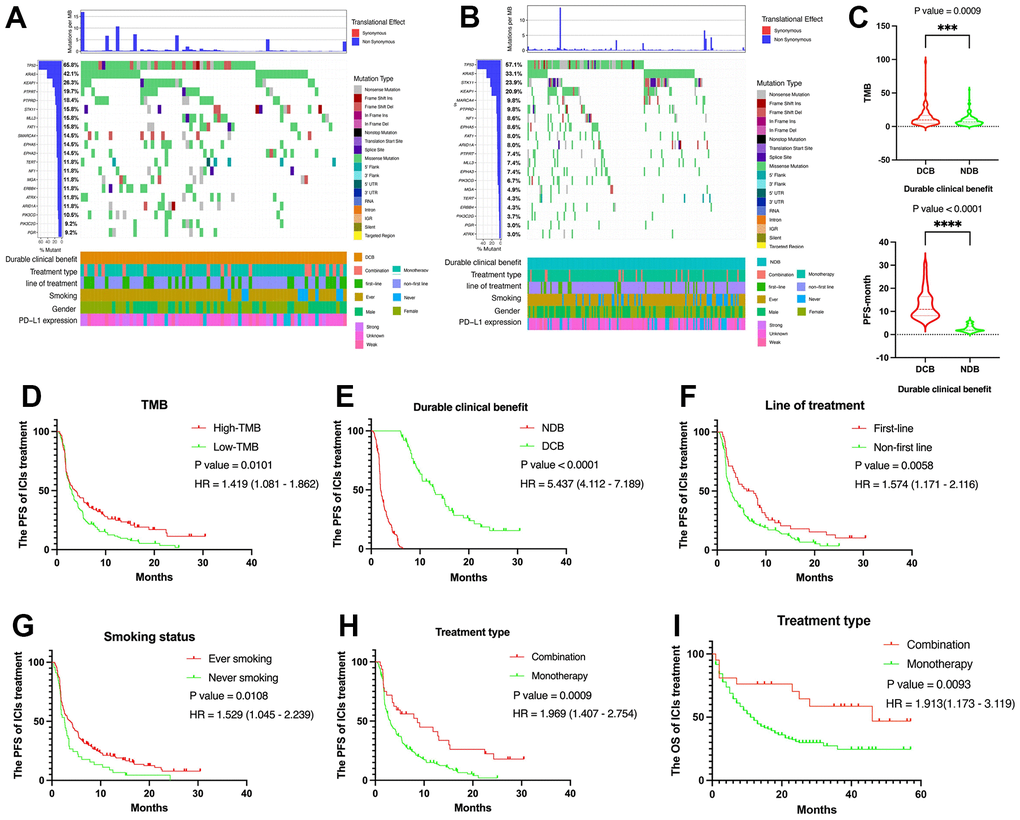
Figure 1. Summary of genomic landscape and clinical features associated with response or non-response in NSCLC with immunotherapy. (A, B) OncoPrint that has top 20 gene alterations in DCB group and NDB group. (C) TMB level and PFS were higher in DCB group than NDB group. (D) The Kaplan-Meier plot for NSCLC PFS based on TMB. (E) The Kaplan-Meier plot for NSCLC PFS based on PD-L1 expression. (F) The Kaplan-Meier plot for NSCLC PFS based on treatment line. (G) The Kaplan-Meier plot for NSCLC PFS based on smoking status. (H) The Kaplan-Meier plot for NSCLC PFS based on treatment type. (I) The Kaplan-Meier plot for NSCLC OS based on treatment type.
Table 1. NSCLC patient characteristics of cBioPortal with ICIs in DCB and NDB group.
| Clinical characteristics | NDB group | DCB group |
| Total cases | 167 | 76 |
| Gender | ||
| Female | 82 (49.1%) | 42 (55.2%) |
| Male | 85 (50.9%) | 34 (44.7%) |
| Age | ||
| <65 | 77 (46.1%) | 44 (57.9%) |
| >=65 | 90 (53.9%) | 32 (42.1%) |
| Smoking | ||
| Ever | 131 (78.4%) | 67 (88.2%) |
| Never | 36 (21.6%) | 9 (11.8%) |
| Treatment type | ||
| Monotherapy | 151 (90.4%) | 53 (69.7%) |
| Combination | 16 (9.6%) | 16 (21.1%) |
| Line of treatment | ||
| First-line | 25 (15.0%) | 27 (35.5%) |
| Non-first line | 142 (85.0%) | 49 (64.5%) |
| PD-L1 expression | ||
| Negative | 35 (20.9%) | 9 (11.8%) |
| Weak | 19 (11.4%) | 9 (11.8%) |
| Strong | 8 (4.8%) | 13 (17.1%) |
| Unknown | 105 (62.9%) | 45 (59.3%) |
| TMB | ||
| High | 74 (44.3%) | 49 (64.5%) |
| Low | 93 (55.7%) | 27 (35.5%) |
Enrichment analysis
The results of GO analysis suggested that the significant enrichment of the top 20 genes was mainly associated with cellular response to chemical stimulus, anatomical structure morphogenesis, cell development, and nervous system development (Figure 2A). In addition, three pathways were particularly enriched including PI3K-Akt signaling pathway, MAPK signaling pathway, and Longevity regulating pathway (Figure 2B). These pathways are all associated with tumor development and progression.
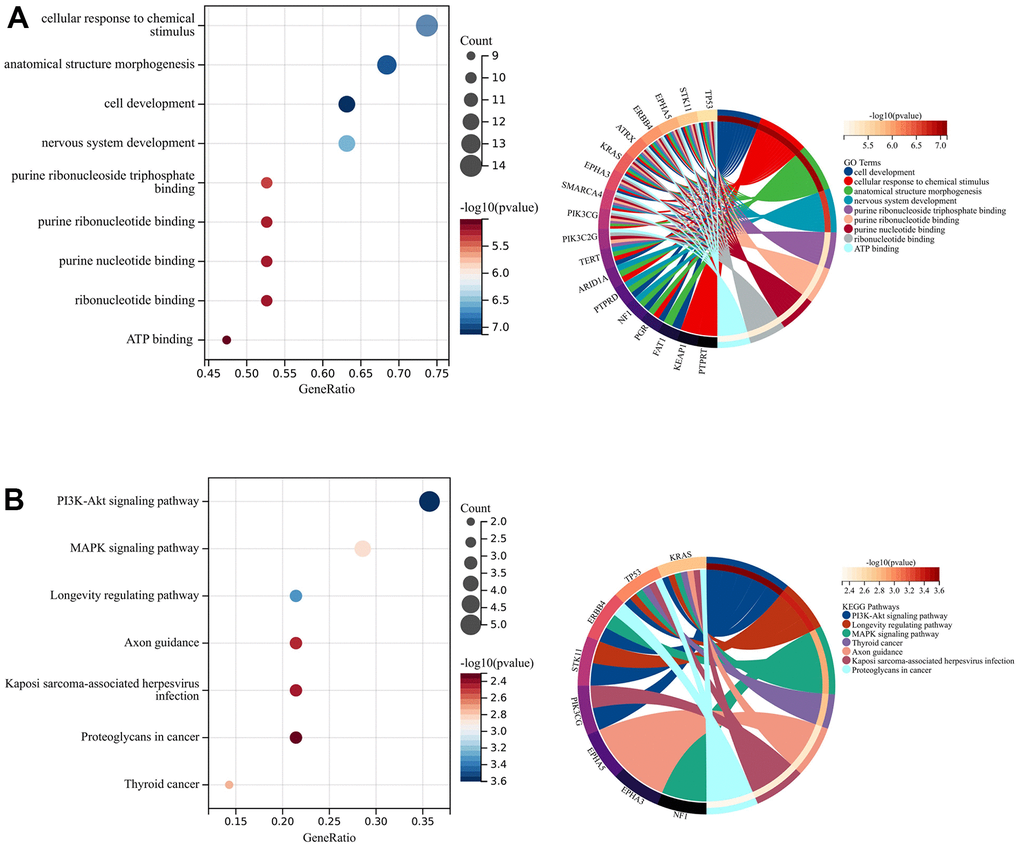
Figure 2. Enrichment analysis and PPI network construction. (A) GO analysis. (B) KEGG analysis.
Identification of survival related gene
Based on gene mutation and survival data, we selected the survival related gene from top 20 alterations in DCB group by the Kaplan-Meier plot method. ATRX, PTPRD, and PTPRT were closely related to PFS of NSCLC with immunotherapy in the first cohort (MSK, J Clin Oncol 2018) and the second cohort (MSK, Science 2015). Next, we analyzed the mutation status of ATRX, PTPRD, and PTPRT in the third cohort (MSKCC, Nat Genet 2019) (Figure 3A). Mutation frequencies of ATRX, PTPRD, and PTPRT were 5.4%, 13.4%, and 11.4%, respectively. Only PTPRD mutation was significantly related to the PFS and OS in advanced NSCLC with immunotherapy (Figure 3B). There was no significant difference in OS between ATRX and PTPRT mutations (Figure 3C, 3D). In addition, there was no significant difference in survival between ATRX, PTPRD, and PTPRT mutations in TCGA cohort (Supplementary Figure 1A–1C). The mutation status of ATRX, PTPRD, and PTPRT were both closely associated with higher TMB values (Figure 3E–3G). Moreover, the ATRX, PTPRD, and PTPRT mutation was related to higher TMB value in TCGA (Supplementary Figure 1D–1F).
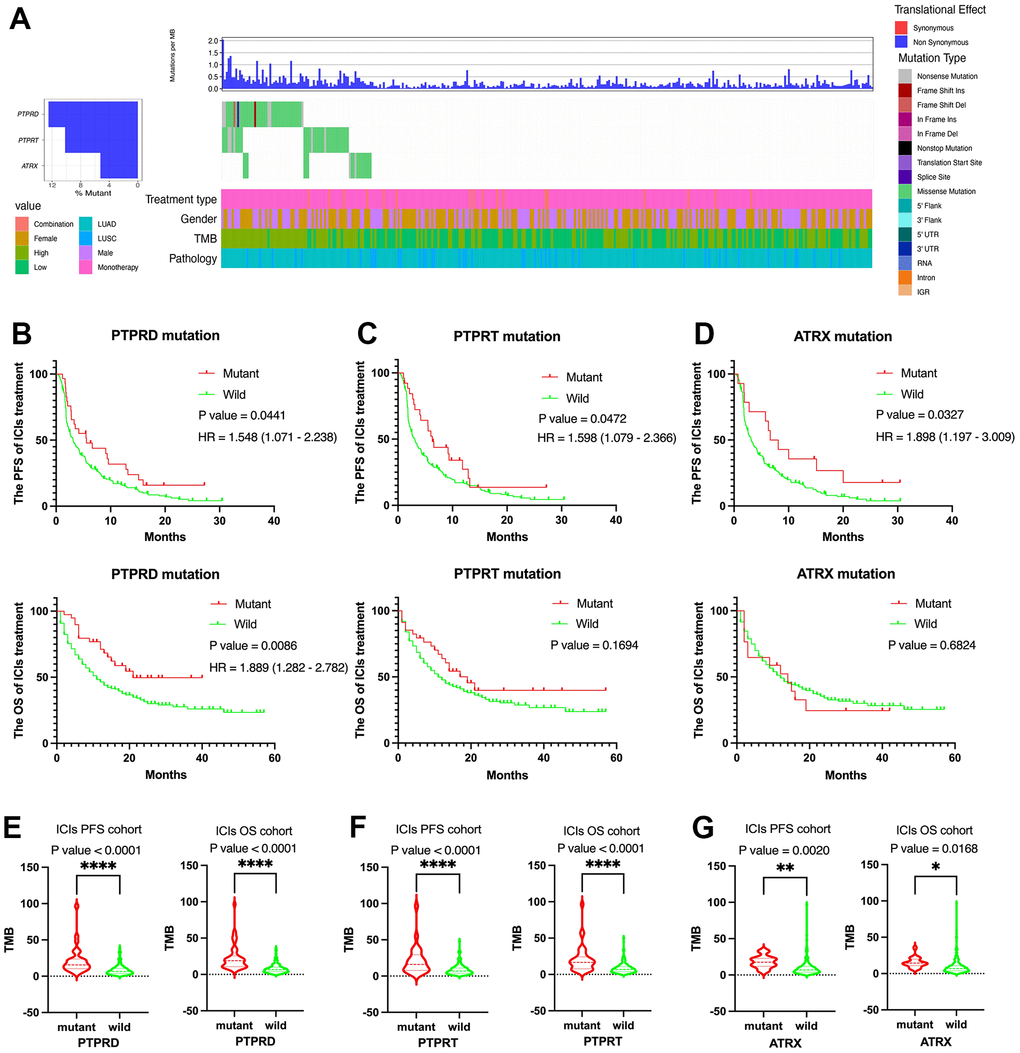
Figure 3. Clinical and molecular features of ATRX, PTPRD, and PTPRT in advanced NSCLC with ICIs treatment. (A) The prevalence of ATRX, PTPRD, and PTPRT mutations in the third cohort (MSKCC, Nat Genet 2019). (B) PTPRD was related to the PFS and OS. (C) PTPRT was related to the PFS. (D) ATRX was related to the PFS. (E–G) ATRX, PTPRD, and PTPRT mutations were closely related to higher TMB value.
Development of nomogram for the prognosis of immunotherapy
Survival analyses were performed using the Kaplan-Meier plot method and selected clinical variables to develop a novel nomogram. TMB (P value = 0.00101), PD-L1 expression (P value = 0.0062), line of treatment (P value = 0.0058), smoking status (P value = 0.00108), treatment type (P value = 0.0009) and PTPRD (P value = 0.0441) were significantly related to the PFS in advanced NSCLC patients with ICIs treatment (Figures 1D–1H, 3B). Based on these variables, we established a systematic nomogram to predict 6-month, and 1-year PFS for advanced NSCLC with ICIs (Figure 4A). The C-index of this nomogram was 0.680 (95% CI 0.617 to 0.742). The same, treatment type (P value = 0.0093) and PTPRD (P value = 0.0086) were significantly related to the OS in advanced NSCLC patients with ICIs treatment (Figures 1I, 3B). The survival probabilities for NSCLC patients with ICIs treatment at 1-year, and 3-year OS were predicted using a nomogram that was constructed based on these variables (Figure 4B). The C-index of this nomogram was 0.658 (95% CI 0.555 to 0.762). The calibration plot demonstrated great predictive performance of our two nomograms (Figure 4C, 4D). In addition, the ROC curve also showed a good ability of our two nomograms to predict 6-month PFS (AUC = 0.76), 1-year PFS (AUC =0.88), 1-year OS (AUC = 0.60), and 3-year OS (AUC = 0.76) of advanced NSCLC patients with immunotherapy (Figure 4E, 4F). Based on our nomograms, clinical physicians could obtain the total point based on all variable points, and then evaluate PFS and OS of each advanced NSCLC with immunotherapy.
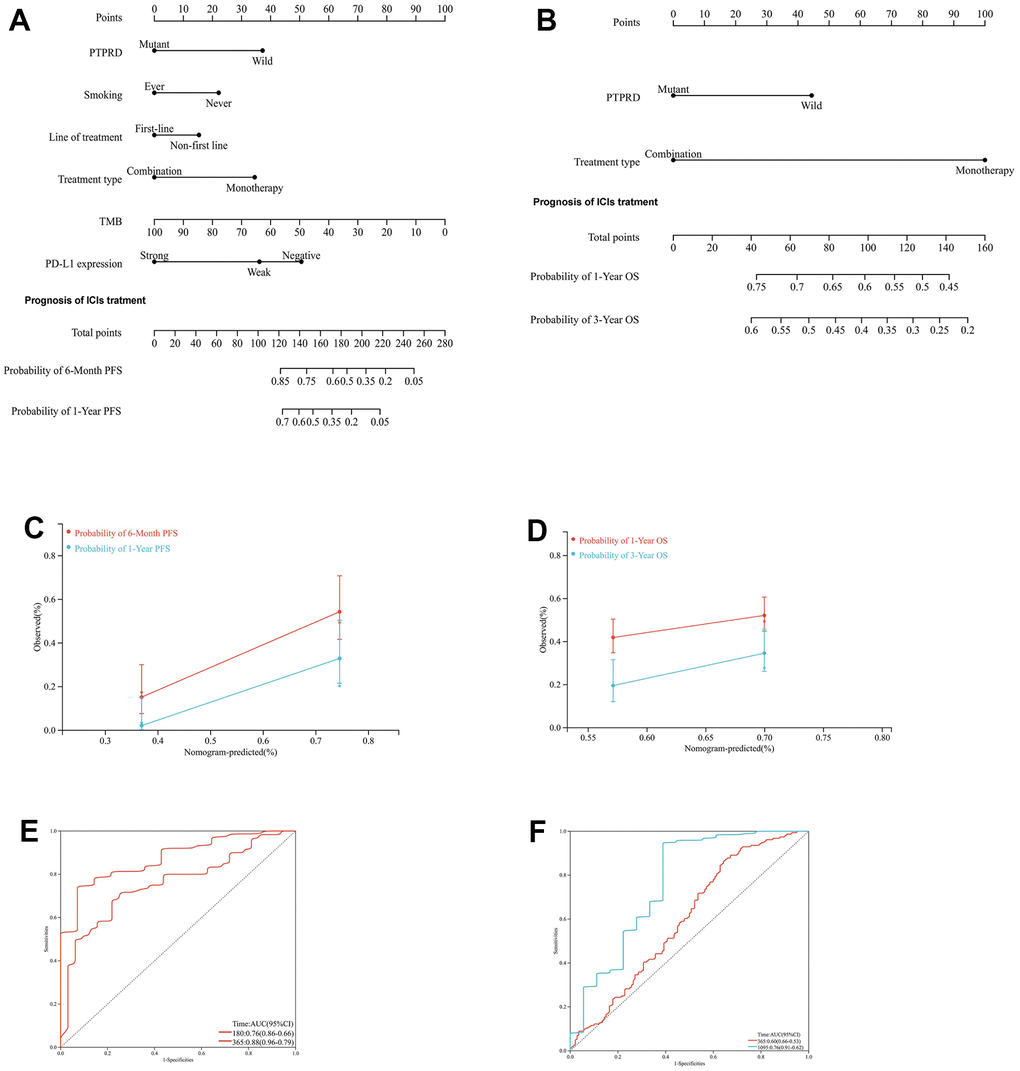
Figure 4. Development of nomograms for the PFS and OS of NSCLC with ICIs. (A) Systematic nomogram to predict the 6-month and 1-year PFS. (B) Systematic nomogram to predict the 1-year and 3-year OS. (C) The calibration plot for the chance of surviving 6-month and 1-year PFS. (D) The calibration plot for the chance of surviving 1-year and 3-year OS. (E) The ROC curve for the chance of 6-month and 1-year PFS. (F) The ROC curve for the chance of 6-month and 1-year PFS.
The role of PTPRD mutation in TIICs and GSEA
The GSEA enrichment analysis performed with TCGA-LUAD cohort showed that riboflavin metabolism, RNA degradation, cell cycle, mismatch repair, and homologous recombination were significantly enriched in PTPRD mutation samples (Figure 5A). In TCGA-LUSC cohort, autoimmune thyroid disease, glycosphingolipid biosynthesis ganglio series, other glycan degradation, bile acid biosynthesis, and regulation of autophagy were significantly abundant in PTPRD mutation samples (Figure 5B).
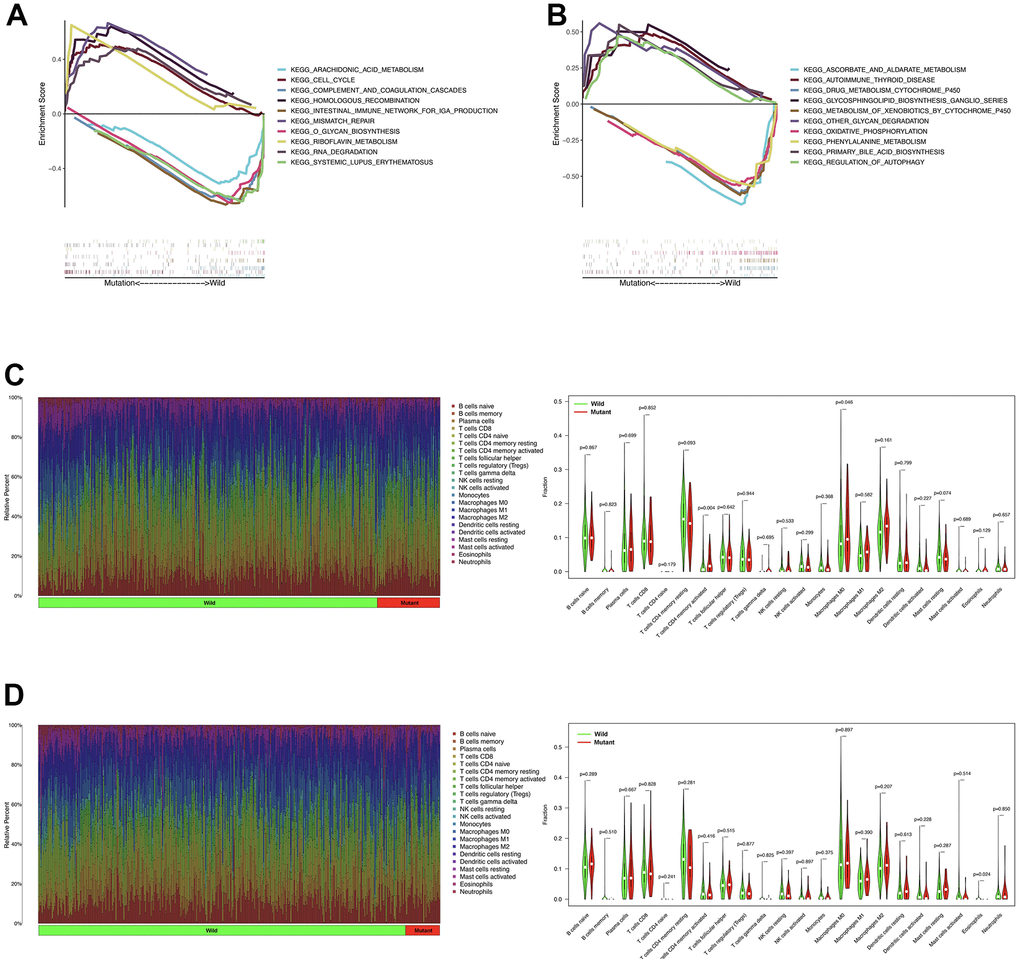
Figure 5. The role of PTPRD mutation in GSEA and TIICs. (A) GSEA analysis of PTPRD mutation in LUAD. (B) GSEA analysis of PTPRD mutation in LUSC. (C) The relationship between the mutation status of PTPRD and immune cells in LUAD. (D) The relationship between the mutation status of PTPRD and immune cells in LUSC.
We also evaluated the relationship between PTPRD mutation and TIICs in NSCLC. In TCGA-LUAD cohort, activated memory CD4 T cells, and M0 macrophages were more enriched in PTPRD mutant sample (Figure 5C). As for LUSC group, eosinophils were more abundant in PTPRD mutation sample (Figure 5D). The mutation of PTPRD may change the tumor microenvironment (TME), leading to the change of sensitivity to immunotherapy in NSCLC.
Verification of the prognostic value of PTPRD mutation in immunotherapy
We further explored the prognostic value of PTPRD mutation in another ICIs cohort (MSK, Cancer Cell 2018) as an independent external validation. Similarly, mutation frequency of PTPRD was 12% (Figure 6A). The same, PTPRD mutation was significantly related to the prognosis of LUAD with ICIs (P = 0.0196, HR = 2.675 (1.377 – 5.196)) (Figure 6B). PTPRD mutation was closely related to higher TMB value in NSCLC with ICIs (Figure 6C). Mutation frequency of PTPRD was 18.4% in DCB group (Figure 1A). However, mutation frequency of PTPRD was only 9.8% in NDB group (Figure 1B). According to the research above, we reasonably deduced that the mutation PTPRD can be used as a potential biomarker for the sensitivity to ICIs and prognosis of advanced NSCLC.
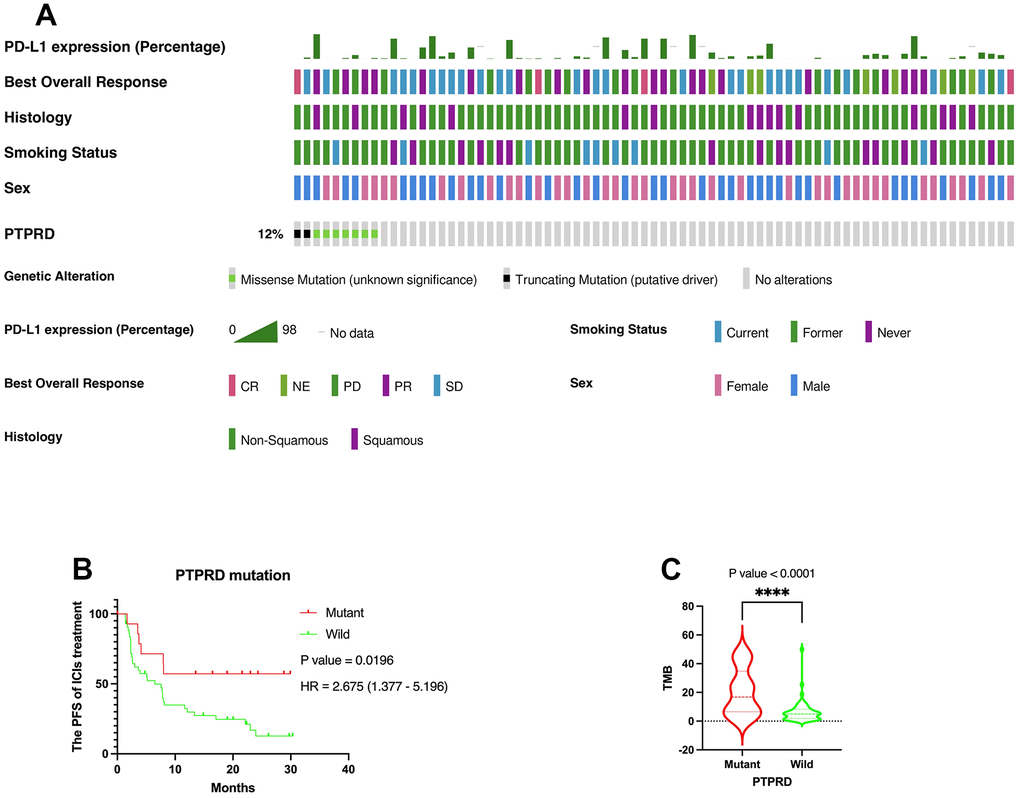
Figure 6. Verification of the prognostic value of PTPRD in immunotherapy. (A) Genomic landscape and clinical feature of PTPRD mutations in another ICIs cohort (MSK, Cancer Cell 2018). (B) The mutation of PTPRD was closely related to prognosis of LUAD with ICIs treatment. (C) PTPRD mutation was closely related to higher TMB in NSCLC.
Discussion
At present, PD-L1 expression or TMB alone did not demonstrate a satisfactory ability to select advanced NSCLC patients who are likely to respond to ICIs. Apart from the expression of PD-L1 and TMB, there are some specific gene mutations including KRAS/TP53, STK11, EGFR, EPHA, and NOTCH, that are related to efficacy of ICIs by regulating the tumor microenvironment and served as potential biomarkers to predict the clinical benefits of immunotherapy [24–27]. Sun et al. found that ARID1A mutation could serve as predictive biomarkers for the prognosis of ICIs [28]. Besides that, some studies show ERBB4 mutation and FGFR4 mutation could serve as a potential biomarker for the prognosis of NSCLC with ICIs treatment [29, 30]. With the increasing routine of NGS in clinical practice, it is essential to explore predictors factors of response to immunotherapy. At the same time, it is important to integrate these prognostic factors to establish a novel systematic nomogram to improve clinical prediction ability in NSCLC with ICIs treatment.
PTPRD is a member of protein tyrosine phosphatases, which negatively regulate tyrosine phosphorylation [31]. It has been reported that PTPRD has a tumor suppressor function, and mutation of PTPRD may promote tumor growth [32]. A high frequency of gene deletions of PTPRD occurs in a variety of cancers [33, 34]. And other mechanisms that may contribute to PTPRD inactivation include point mutations and promoter region hypermethylation [35, 36]. A study found that PTPRD inactivation promotes tumor metastasis by induced CXCL8 in gastric cancer [37]. Recently, a study analyzed the data of 1745 NSCLC and elucidated the landscape of interaction effects among common co-mutations on the efficacy of ICIs [38]. Particularly, KRAS mutation remarkably interacted with its co-occurring mutations in TP53, STK11, PTPRD, RBM10, and ATM in non-squamous NSCLC. In addition, Shang et al. found that PTPRD and PTPRT mutations may be a biomarker for predicting immunotherapy in pan-cancer, but the role of PTPRD mutation in NSCLC has not been analyzed separately [39]. Li et al. suggested that PTPRD/PTPRT mutation was significantly associated with better progression-free survival (PFS) in three independent cohorts. The median PFS for PTPRD/PTPRT mutant-type vs. wild-type NSCLC patients were not reached vs. 6.3 months (Rizvi2015, HR = 0.16; 95% CI, 0.02-1.17; P=0.03), 24.0 vs. 5.4 months (Hellmann2018, HR, 0.49; 95% CI, 0.26-0.94; P=0.03), 5.6 vs. 3.0 months (Rizvi2018, HR = 0.64; 95% CI, 0.44-0.92; P=0.01) and 6.8 vs. 3.5 months (Pooled cohort, HR, 0.54; 95% CI, 0.39-0.73; P<0.0001) respectively [40]. Sun et al. demonstrated that tissue or circulating tumor DNA PTPRD mutation is a prognostic biomarker predicting prognosis of anti-PD-(L)1 monotherapy in non-squamous NSCLC patients [41]. However, the above study failed to predict OS in validation cohort, and squamous NSCLC were not included in the study. There is still a lack of sufficient literature to support the clinical prognostic significance of ICIs treatment in NSCLC patients who harbor PTPRD mutations. The underlying mechanisms of PTPRD mutation that regulate immune-related pathways in NSCLC remain unknown. According to these studies, we further explored the significance of PTPRD mutations in predicting the clinical outcome (PFS and OS) of advanced NSCLC with immunotherapy.
In this study, mutation frequencies of PTPRD in DCB group, NDB group, the third cohort (MSKCC, Nat Genet 2019), and the last cohort (MSK, Cancer Cell 2018) were 18.4%, 9.8%, 13.4%, and 12%, respectively. The Kaplan–Meier survival curves showed the mutation of PTPRD was associated with the PFS (P = 0.0441, HR = 1.548 (1.071 – 2.238)) and OS (P = 0.0086, HR = 1.889 (1.282 – 2.782)) in NSCLC with ICIs treatment. The prognostic value of PTPRD mutation was validated in the last ICIs cohort as an independent external validation (P = 0.0196, HR = 2.675 (1.377 – 5.196)). Besides, the PTPRD mutation was closely associated with higher TMB values in all ICIs cohort and TCGA cohort (P < 0.0001). Therefore, we reasonably deduced that the mutation PTPRD can be used as a potential biomarker for the sensitivity to ICIs treatment and prognosis of advanced NSCLC.
To explain why PTPRD mutations were associated with favorable ICIs prognosis, we evaluated the role of PTPRD mutation in GSEA and immune infiltration. The GSEA enrichment analysis showed that PTPRD mutation samples were mainly associated with riboflavin metabolism, RNA degradation, cell cycle, and mismatch repair in LUAD, and glycosphingolipid biosynthesis ganglio series, other glycan degradation, bile acid biosynthesis, and regulation of autophagy in LUSC, respectively. Besides that, we found that activated memory CD4 T cells, M0 macrophages, and eosinophils were more enriched in PTPRD mutant sample. Some studies revealed that eosinophils were closely associated with clinical outcomes in patients with ICIs treatment [42–44]. The mutation of PTPRD may influence CD4+ T cell infiltration via its phosphatase activity, and promote the occurrence of “hot” TME with enhanced anti-tumor immunity in advanced NSCLC patients.
Moreover, NSCLC patient’s clinical variables and genomic data that we included were screened by the Kaplan-Meier plot method. TMB, PD-L1 expression, line of treatment, smoking status, treatment type, and PTPRD mutant were significantly related to the PFS in advanced NSCLC patients with ICIs treatment. Besides that, treatment type and PTPRD mutant were significantly related to the OS in advanced NSCLC patients with ICIs treatment. According to the above results, we constructed two novel systematic nomograms that are based on the patient’s clinicopathological parameters and genome data to predict the prognosis for advanced NSCLC with ICIs. Based on our novel nomograms, clinicians can obtain the total point based on all variable points for each patient and can then predict the 6-month PFS, 1-year PFS, 1-year OS, and 3-year OS of advanced NSCLC patients with immunotherapy. Our novel nomograms can be used to assess the PFS and OS of NSCLC patients ICIs and formulate the appropriate type of treatment and follow-up time before immunotherapy.
The existing literature suggested that the mechanism of PTPRD mutation in NSCLC with ICIs still needs to be further explored. This study is the first to use the large database to establish two systematic nomograms for predicting the PFS and OS of advanced NSCLC patients with ICIs treatment, which undoubtedly provides a new clinical strategy for advanced NSCLC patients. This work is the first to illustrate the role of PTPRD mutations as a potential biomarker for the sensitivity to ICIs treatment and prognosis of advanced NSCLC. PTPRD can be used as a potential biomarker in regulating the TME and associating with the PFS and OS in advanced NSCLC with immunotherapy. Nevertheless, there remains some limitations in our work. First, this work employed four ICIs cohorts from the cBioPortal database. Due to the utilization of different platforms and detection depths, four cohorts may exhibit potential heterogeneity. Second, clinical information, response data, and genome data of NSCLC with ICIs were downloaded from four public datasets, some specific patients’ information and clinicopathological variables were unclear or not available. Third, four ICIs cohorts used different treatment types, such as immunotherapy monotherapy or combination with anti-CTLA-4, resulting in a certain degree of research heterogeneity. In addition, the mechanism of PTPRD affecting TME and immunotherapy in NSCLC needs further experiments to explore.
Conclusions
To conclude, our study demonstrated that PTPRD mutation could serve as a prognostic biomarker predicting the PFS and OS in advanced NSCLC treated ICIs. PTPRD mutation is strongly associated with high TMB levels and immune infiltration and enhanced anti-tumor microenvironment. Our systematic nomograms showed great potential value in clinical application to predict the PFS and OS in advanced NSCLC with immunotherapy.
Author Contributions
Chaohui Leng and Li Wang conceived and designed the study. Li Wang and Zhixuan Ren performed the analysis. Li Wang wrote the paper. Chaohui Leng reviewed and edited the manuscript. All authors read and approved the manuscript.
Acknowledgments
This study is thankful for Miss Xiong Sisi’s help and support.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
No funding was provided for this study.
References
- 1. Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, Jemal A, Kramer JL, Siegel RL. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019; 69:363–85. https://doi.org/10.3322/caac.21565 [PubMed]
- 2. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018; 553:446–54. https://doi.org/10.1038/nature25183 [PubMed]
- 3. Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho BC, Turna HZ, Castro G
Jr , Srimuninnimit V, Laktionov KK, Bondarenko I, Kubota K, Lubiniecki GM, Zhang J, et al, and KEYNOTE-042 Investigators. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019; 393:1819–30. https://doi.org/10.1016/S0140-6736(18)32409-7 [PubMed] - 4. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O’Brien M, Rao S, Hotta K, et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50. J Clin Oncol. 2021; 39:2339–49. https://doi.org/10.1200/JCO.21.00174 [PubMed]
- 5. Gadgeel S, Rodríguez-Abreu D, Speranza G, Esteban E, Felip E, Dómine M, Hui R, Hochmair MJ, Clingan P, Powell SF, Cheng SY, Bischoff HG, Peled N, et al. Updated Analysis From KEYNOTE-189: Pembrolizumab or Placebo Plus Pemetrexed and Platinum for Previously Untreated Metastatic Nonsquamous Non-Small-Cell Lung Cancer. J Clin Oncol. 2020; 38:1505–17. https://doi.org/10.1200/JCO.19.03136 [PubMed]
- 6. Novello S, Kowalski DM, Luft A, Gümüş M, Vicente D, Mazières J, Rodríguez-Cid J, Tafreshi A, Cheng Y, Lee KH, Golf A, Sugawara S, Robinson AG, et al. Pembrolizumab Plus Chemotherapy in Squamous Non-Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study. J Clin Oncol. 2023; 41:1999–2006. https://doi.org/10.1200/JCO.22.01990 [PubMed]
- 7. Park YJ, Kuen DS, Chung Y. Future prospects of immune checkpoint blockade in cancer: from response prediction to overcoming resistance. Exp Mol Med. 2018; 50:1–13. https://doi.org/10.1038/s12276-018-0130-1 [PubMed]
- 8. Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, Lu S, Kemberling H, Wilt C, Luber BS, Wong F, Azad NS, Rucki AA, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017; 357:409–13. https://doi.org/10.1126/science.aan6733 [PubMed]
- 9. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O’Brien M, Rao S, Hotta K, et al, and KEYNOTE-024 Investigators. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016; 375:1823–33. https://doi.org/10.1056/NEJMoa1606774 [PubMed]
- 10. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L, Carcereny E, Ahn MJ, Felip E, et al, and KEYNOTE-001 Investigators. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015; 372:2018–28. https://doi.org/10.1056/NEJMoa1501824 [PubMed]
- 11. Goodman AM, Kato S, Bazhenova L, Patel SP, Frampton GM, Miller V, Stephens PJ, Daniels GA, Kurzrock R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol Cancer Ther. 2017; 16:2598–608. https://doi.org/10.1158/1535-7163.MCT-17-0386 [PubMed]
- 12. Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, Lee W, Yuan J, Wong P, Ho TS, Miller ML, Rekhtman N, Moreira AL, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015; 348:124–8. https://doi.org/10.1126/science.aaa1348 [PubMed]
- 13. Samstein RM, Lee CH, Shoushtari AN, Hellmann MD, Shen R, Janjigian YY, Barron DA, Zehir A, Jordan EJ, Omuro A, Kaley TJ, Kendall SM, Motzer RJ, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet. 2019; 51:202–6. https://doi.org/10.1038/s41588-018-0312-8 [PubMed]
- 14. Jardim DL, Goodman A, de Melo Gagliato D, Kurzrock R. The Challenges of Tumor Mutational Burden as an Immunotherapy Biomarker. Cancer Cell. 2021; 39:154–73. https://doi.org/10.1016/j.ccell.2020.10.001 [PubMed]
- 15. Wang L, Zhao D, Qin K, Rehman FU, Zhang X. Effect and biomarker of Nivolumab for non-small-cell lung cancer. Biomed Pharmacother. 2019; 117:109199. https://doi.org/10.1016/j.biopha.2019.109199 [PubMed]
- 16. Huang J, Liu D, Wang Y, Liu L, Li J, Yuan J, Jiang Z, Jiang Z, Hsiao WW, Liu H, Khan I, Xie Y, Wu J, et al. Ginseng polysaccharides alter the gut microbiota and kynurenine/tryptophan ratio, potentiating the antitumour effect of antiprogrammed cell death 1/programmed cell death ligand 1 (anti-PD-1/PD-L1) immunotherapy. Gut. 2022; 71:734–45. https://doi.org/10.1136/gutjnl-2020-321031 [PubMed]
- 17. Chan TA, Yarchoan M, Jaffee E, Swanton C, Quezada SA, Stenzinger A, Peters S. Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann Oncol. 2019; 30:44–56. https://doi.org/10.1093/annonc/mdy495 [PubMed]
- 18. Dafni U, Tsourti Z, Vervita K, Peters S. Immune checkpoint inhibitors, alone or in combination with chemotherapy, as first-line treatment for advanced non-small cell lung cancer. A systematic review and network meta-analysis. Lung Cancer. 2019; 134:127–40. https://doi.org/10.1016/j.lungcan.2019.05.029 [PubMed]
- 19. Rizvi H, Sanchez-Vega F, La K, Chatila W, Jonsson P, Halpenny D, Plodkowski A, Long N, Sauter JL, Rekhtman N, Hollmann T, Schalper KA, Gainor JF, et al. Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients With Non-Small-Cell Lung Cancer Profiled With Targeted Next-Generation Sequencing. J Clin Oncol. 2018; 36:633–41. https://doi.org/10.1200/JCO.2017.75.3384 [PubMed]
- 20. Hellmann MD, Nathanson T, Rizvi H, Creelan BC, Sanchez-Vega F, Ahuja A, Ni A, Novik JB, Mangarin LM, Abu-Akeel M, Liu C, Sauter JL, Rekhtman N, et al. Genomic Features of Response to Combination Immunotherapy in Patients with Advanced Non-Small-Cell Lung Cancer. Cancer Cell. 2018; 33:843–52.e4. https://doi.org/10.1016/j.ccell.2018.03.018 [PubMed]
- 21. Kuhl CK, Alparslan Y, Schmoee J, Sequeira B, Keulers A, Brümmendorf TH, Keil S. Validity of RECIST Version 1.1 for Response Assessment in Metastatic Cancer: A Prospective, Multireader Study. Radiology. 2019; 290:349–56. https://doi.org/10.1148/radiol.2018180648 [PubMed]
- 22. Ashburner M, Ball CA, Blake JA, Botstein D, Butler H, Cherry JM, Davis AP, Dolinski K, Dwight SS, Eppig JT, Harris MA, Hill DP, Issel-Tarver L, et al. Gene ontology: tool for the unification of biology. The Gene Ontology Consortium. Nat Genet. 2000; 25:25–9. https://doi.org/10.1038/75556 [PubMed]
- 23. Kanehisa M, Sato Y, Kawashima M, Furumichi M, Tanabe M. KEGG as a reference resource for gene and protein annotation. Nucleic Acids Res. 2016; 44:D457–62. https://doi.org/10.1093/nar/gkv1070 [PubMed]
- 24. Dong ZY, Zhong WZ, Zhang XC, Su J, Xie Z, Liu SY, Tu HY, Chen HJ, Sun YL, Zhou Q, Yang JJ, Yang XN, Lin JX, et al. Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma. Clin Cancer Res. 2017; 23:3012–24. https://doi.org/10.1158/1078-0432.CCR-16-2554 [PubMed]
- 25. Biton J, Mansuet-Lupo A, Pécuchet N, Alifano M, Ouakrim H, Arrondeau J, Boudou-Rouquette P, Goldwasser F, Leroy K, Goc J, Wislez M, Germain C, Laurent-Puig P, et al. TP53, STK11, and EGFR Mutations Predict Tumor Immune Profile and the Response to Anti-PD-1 in Lung Adenocarcinoma. Clin Cancer Res. 2018; 24:5710–23. https://doi.org/10.1158/1078-0432.CCR-18-0163 [PubMed]
- 26. Bai H, Duan J, Li C, Xie W, Fang W, Xu Y, Wang G, Wan R, Sun J, Xu J, Wang X, Fei K, Zhao Z, et al. EPHA mutation as a predictor of immunotherapeutic efficacy in lung adenocarcinoma. J Immunother Cancer. 2020; 8:e001315. https://doi.org/10.1136/jitc-2020-001315 [PubMed]
- 27. Zhang K, Hong X, Song Z, Xu Y, Li C, Wang G, Zhang Y, Zhao X, Zhao Z, Zhao J, Huang M, Huang D, Qi C, et al. Identification of Deleterious NOTCH Mutation as Novel Predictor to Efficacious Immunotherapy in NSCLC. Clin Cancer Res. 2020; 26:3649–61. https://doi.org/10.1158/1078-0432.CCR-19-3976 [PubMed]
- 28. Sun D, Tian L, Zhu Y, Wo Y, Liu Q, Liu S, Li H, Hou H. Subunits of ARID1 serve as novel biomarkers for the sensitivity to immune checkpoint inhibitors and prognosis of advanced non-small cell lung cancer. Mol Med. 2020; 26:78. https://doi.org/10.1186/s10020-020-00208-9 [PubMed]
- 29. Hu X, Xu H, Xue Q, Wen R, Jiao W, Tian K. The role of ERBB4 mutations in the prognosis of advanced non-small cell lung cancer treated with immune checkpoint inhibitors. Mol Med. 2021; 27:126. https://doi.org/10.1186/s10020-021-00387-z [PubMed]
- 30. Wang L, Ren Z, Yu B, Tang J. Development of nomogram based on immune-related gene FGFR4 for advanced non-small cell lung cancer patients with sensitivity to immune checkpoint inhibitors. J Transl Med. 2021; 19:22. https://doi.org/10.1186/s12967-020-02679-0 [PubMed]
- 31. Meehan M, Parthasarathi L, Moran N, Jefferies CA, Foley N, Lazzari E, Murphy D, Ryan J, Ortiz B, Fabius AW, Chan TA, Stallings RL. Protein tyrosine phosphatase receptor delta acts as a neuroblastoma tumor suppressor by destabilizing the aurora kinase A oncogene. Mol Cancer. 2012; 11:6. https://doi.org/10.1186/1476-4598-11-6 [PubMed]
- 32. Peyser ND, Du Y, Li H, Lui V, Xiao X, Chan TA, Grandis JR. Loss-of-Function PTPRD Mutations Lead to Increased STAT3 Activation and Sensitivity to STAT3 Inhibition in Head and Neck Cancer. PLoS One. 2015; 10:e0135750. https://doi.org/10.1371/journal.pone.0135750 [PubMed]
- 33. Giefing M, Zemke N, Brauze D, Kostrzewska-Poczekaj M, Luczak M, Szaumkessel M, Pelinska K, Kiwerska K, Tönnies H, Grenman R, Figlerowicz M, Siebert R, Szyfter K, Jarmuz M. High resolution ArrayCGH and expression profiling identifies PTPRD and PCDH17/PCH68 as tumor suppressor gene candidates in laryngeal squamous cell carcinoma. Genes Chromosomes Cancer. 2011; 50:154–66. https://doi.org/10.1002/gcc.20840 [PubMed]
- 34. Stark M, Hayward N. Genome-wide loss of heterozygosity and copy number analysis in melanoma using high-density single-nucleotide polymorphism arrays. Cancer Res. 2007; 67:2632–42. https://doi.org/10.1158/0008-5472.CAN-06-4152 [PubMed]
- 35. Veeriah S, Brennan C, Meng S, Singh B, Fagin JA, Solit DB, Paty PB, Rohle D, Vivanco I, Chmielecki J, Pao W, Ladanyi M, Gerald WL, et al. The tyrosine phosphatase PTPRD is a tumor suppressor that is frequently inactivated and mutated in glioblastoma and other human cancers. Proc Natl Acad Sci USA. 2009; 106:9435–40. https://doi.org/10.1073/pnas.0900571106 [PubMed]
- 36. Kohno T, Otsuka A, Girard L, Sato M, Iwakawa R, Ogiwara H, Sanchez-Cespedes M, Minna JD, Yokota J. A catalog of genes homozygously deleted in human lung cancer and the candidacy of PTPRD as a tumor suppressor gene. Genes Chromosomes Cancer. 2010; 49:342–52. https://doi.org/10.1002/gcc.20746 [PubMed]
- 37. Bae WJ, Ahn JM, Byeon HE, Kim S, Lee D. PTPRD-inactivation-induced CXCL8 promotes angiogenesis and metastasis in gastric cancer and is inhibited by metformin. J Exp Clin Cancer Res. 2019; 38:484. https://doi.org/10.1186/s13046-019-1469-4 [PubMed]
- 38. Zhang F, Wang J, Xu Y, Cai S, Li T, Wang G, Li C, Zhao L, Hu Y. Co-occurring genomic alterations and immunotherapy efficacy in NSCLC. NPJ Precis Oncol. 2022; 6:4. https://doi.org/10.1038/s41698-021-00243-7 [PubMed]
- 39. Shang X, Zhang W, Zhang X, Yu M, Liu J, Cheng Y, Cheng B. PTPRD/PTPRT mutation as a predictive biomarker of immune checkpoint inhibitors across multiple cancer types. Front Immunol. 2022; 13:991091. https://doi.org/10.3389/fimmu.2022.991091 [PubMed]
- 40. Wang X, Wu B, Yan Z, Wang G, Chen S, Zeng J, Tao F, Xu B, Ke H, Li M. Association of PTPRD/PTPRT Mutation With Better Clinical Outcomes in NSCLC Patients Treated With Immune Checkpoint Blockades. Front Oncol. 2021; 11:650122. https://doi.org/10.3389/fonc.2021.650122 [PubMed]
- 41. Sun Y, Duan J, Fang W, Wang Z, Du X, Wang X, Li C, Cai S, Zhao J, Li S, Zhang L, Bai H, Wang J. Identification and validation of tissue or ctDNA PTPRD phosphatase domain deleterious mutations as prognostic and predictive biomarkers for immune checkpoint inhibitors in non-squamous NSCLC. BMC Med. 2021; 19:239. https://doi.org/10.1186/s12916-021-02075-5 [PubMed]
- 42. Mota JM, Teo MY, Whiting K, Li HA, Regazzi AM, Lee CH, Funt SA, Bajorin D, Ostrovnaya I, Iyer G, Rosenberg JE. Pretreatment Eosinophil Counts in Patients With Advanced or Metastatic Urothelial Carcinoma Treated With Anti-PD-1/PD-L1 Checkpoint Inhibitors. J Immunother. 2021; 44:248–53. https://doi.org/10.1097/CJI.0000000000000372 [PubMed]
- 43. Yoshida T, Ohe C, Ikeda J, Atsumi N, Ohsugi H, Sugi M, Higasa K, Saito R, Tsuta K, Matsuda T, Kinoshita H. Eosinophilic features in clear cell renal cell carcinoma correlate with outcomes of immune checkpoint and angiogenesis blockade. J Immunother Cancer. 2021; 9:e002922. https://doi.org/10.1136/jitc-2021-002922 [PubMed]
- 44. Chu X, Zhao J, Zhou J, Zhou F, Jiang T, Jiang S, Sun X, You X, Wu F, Ren S, Zhou C, Su C. Association of baseline peripheral-blood eosinophil count with immune checkpoint inhibitor-related pneumonitis and clinical outcomes in patients with non-small cell lung cancer receiving immune checkpoint inhibitors. Lung Cancer. 2020; 150:76–82. https://doi.org/10.1016/j.lungcan.2020.08.015 [PubMed]