Evaluation of the clinical significance of long non-coding RNA MALAT1 genetic variants in human lung adenocarcinoma
Abstract
Lung adenocarcinoma (LUAD) is the most frequent histological subtype of lung cancer, which is the most common malignant tumor and the main cause of cancer-related mortality globally. Recent reports revealed that long non-coding RNA (lncRNA) of metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) plays a crucial role in tumorigenesis and metastasis development in lung cancer. However, the contribution of MALAT1 genetic variants to the development of LUAD is unclear, especially in epidermal growth factor receptor (EGFR) mutation status. In this study, 272 LADC patients with different EGFR status were recruited to dissect the allelic discrimination of the MALAT1 polymorphisms at rs3200401, rs619586, and rs1194338. The findings of the study showed that MALAT1 polymorphisms rs3200401, rs619586, and rs1194338 were not associated to LUAD susceptibility; however, rs3200401 polymorphisms was significantly correlated to EGFR wild-type status and tumor stages in LUAD patients in dominant model (p=0.016). Further analyses using the datasets from The Cancer Genome Atlas (TCGA) revealed that lower MALAT1 mRNA levels were associated with the advanced stage, and lymph node metastasis in LADC patients. In conclusion, our results showed that MALAT1 rs3200401 polymorphisms dramatically raised the probability of LUAD development.
Introduction
The most common cause of cancer-related death globally and a lethal malignancy, is lung cancer [1]. Non-small cell lung cancer (NSCLC) is the most often seen histological subtype of lung cancer and is largely divided into squamous cell carcinoma (LUSC) and adenocarcinoma (LUAD) [2]. Among them, LUAD accounts for about 40% of all lung cancer patients [3]. The prognosis for LUAD is still disappointing, with a 5-year survival rate of less than 20%, despite recent advancements in cancer therapeutic treatments, such as surgical resection, immunotherapy, chemotherapy, and radiation [4]. Nevertheless, once distant metastases have developed, LUAD cannot be treated surgically [5]. Consequently, based on the developing concept of precision medicine, the development of molecular pathology diagnostic technologies and tailored therapy have considerably increased the overall survival of LUAD patients [6]. Key genes involved in carcinogenesis might be thought of as therapeutic targets in precision medicine. Mutations in the epidermal growth factor receptor EGFR is one often reported molecule that is employed in the diagnosis of disease and as therapeutic targets in NSCLC [7, 8]. Curing individuals with LUAD remains difficult despite the positive clinical outcomes of molecularly targeted treatments. Thus, further research is required for the development of lung cancer treatments, particularly to identify relevant potential genetic markers [9–11].
Non-coding RNAs (ncRNAs) are further divided into two categories according to the length, less than 200 bp (Small non-coding RNAs; sncRNAs) and greater than 200 bp (Long non-coding RNAs; lncRNAs), respectively [12]. Accumulating evidence has shown that long non-coding RNAs, which have been identified as oncogenes or tumor suppressors, play crucial roles in biological processes and are involved in tumorigenesis processes, including uncontrolled proliferation, escape cell death and tumor metastasis [13–16]. Metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) lncRNA, which was initially identified as an oncogene in a study of NSCLC, is situated at 11q13 [17]. Since its discovery, MALAT1 has contributed significantly to the progression, metastasis, drug resistance, and treatment of the cancer, as well as its clinical importance in predicting the tumor metastasis of early stage, particularly lung cancer [17, 18]. Subsequently, overexpression of MALAT1 was also found to be involved in tumor cell proliferation, migration, invasion and apoptosis in various cancers. In addition, increased expression level of MALAT1 can also be used as a potential biomarker for tumor diagnosis and prognosis, including liver, colorectal, pancreatic, papillary thyroid, renal cancers and gastrointestinal diffuse large B-cell lymphoma [19–24].
Many single nucleotide polymorphisms (SNPs) are linked to several cancers, according to genome-wide association studies (GWAS) [25, 26]. Recent studies have shown that genetic variations, such as those prevalent universally present in lncRNA genes, may directly or indirectly affect lncRNA expression levels in multiple ways to regulate tumor development [27, 28]. Previous studies have reported that the MALAT1 polymorphisms were associated with cancer development, carcinogenesis and prognosis in various cancers such as hepatocellular carcinoma [29], cervical cancer [30], oral squamous cell carcinoma [31], and prostate cancer [32]. However, only a small number of researches have looked into the connection between MALAT1 SNPs and lung cancer [33, 34]. The link between genetic variations and somatic mutations in the development of cancer has recently been studied. In NSCLC, for instance, it was discovered that SNPs were associated with EGFR mutation susceptibility [11, 35]. Furthermore, the coexistence of MALAT1 SNPs with various EGFR mutation statuses remains unclear for the clinicopathological features of LUAD. In this study, a case-control study was conducted on the Taiwanese population to explore the relationship between MALAT1 polymorphisms and susceptibility, and to explore the correlation between MALAT1 SNPs and EGFR phenotypes and their impact on clinicopathological characteristics, aiming to reveal potential genetic markers affecting EGFR mutation status and prognosis in LUAD patients.
Results
A total of 272 LADC patients were included in this study, and Table 1 summarizes the characteristics of EGFR wild-type and EGFR mutation subjects recruited. The EGFR wild-type and EGFR mutation samples were split into two groups. There were 163 patients with EGFR mutation (57 males and 106 females; mean age, 65.71 + 13.50 years) compared to 109 patients (66 males and 43 females; mean age, 65.10 + 13.40 years) with the EGFR wild-type. The EGFR mutation were significantly associated with gender (p<0.001), cigarette smoking status (p<0.001), and cell differentiation (p<0.001) in relation to the clinical characteristics of these individuals. Age, tumor stage, tumor T status, clinical stage, lymph node status and distant metastasis were all similar, with no discernible differences.
Table 1. Demographics and clinical characteristics of 272 patients in lung adenocarcinoma with EGFR mutation status.
| Variable | EGFR wild type
(N=109) n (%) | EGFR mutation
(N=163) n (%) | p-value |
| Age | | | |
| Mean + SD | 65.10 + 13.40 | 65.71 + 13.50 | p=0.714 |
| Gender | | | |
| Male | 66 (60.6%) | 57 (35.0%) | p<0.001 |
| Female | 43 (39.4%) | 106 (65.0%) | |
| Cigarette smoking status | | | |
| Never-smoker | 49 (45.0%) | 127 (77.9%) | p<0.001 |
| Ever-smoker | 60 (55.0%) | 36 (22.1%) | |
| stage | | | |
| I+II | 25 (22.9%) | 46 (28.2%) | p=0.331 |
| III+IV | 84 (77.1%) | 117 (71.8%) | |
| Tumor T status | | | |
| T1+T2 | 58 (53.2%) | 104 (63.8%) | p=0.081 |
| T3+T4 | 51 (46.8%) | 59 (36.2%) | |
| Lymph node status | | | |
| Negative | 28 (25.7%) | 53 (32.5%) | p=0.228 |
| Positive | 81 (74.3%) | 110 (67.5%) | |
| Distant Metastasis | | | |
| Negative | 52 (47.7%) | 78 (47.9%) | p=0.981 |
| Positive | 57 (52.3%) | 85 (52.1%) | |
| Cell differentiation | | | |
| Well | 8 (7.3%) | 19 (11.7%) | p<0.001 |
| Moderately | 78 (71.6%) | 135 (82.8%) | |
| Poorly | 23 (21.1%) | 9 (5.5%) | |
| Data with categories: N (%); Continuous variables: mean standard deviation (SD); The comparisons between the EGFR wild-type and EGFR mutation in LUAD were assessed using the Mann-Whitney U-test or Fisher’s exact test; Statistics were considered significant at p-values less than 0.05. |
The genotype frequencies of all three SNPs (rs3200401, rs619586, and rs1194338) carrying EGFR wild-type or EGFR mutation were initially examined in LADC patients to evaluate any potential associations between MALAT1 SNPs and the likelihood of the risk of developing EGFR mutation. The highest frequencies of these SNPs of MALAT1 were homozygous for CC (rs3200401), AA (rs619586) and CC (rs1194338), respectively, in both EGFR wild-type or EGFR mutation groups. Statistical data demonstrated that there was no correlation between MALAT1 SNPs and EGFR mutation (Table 2).
Table 2. Distribution frequency of MALAT1 genotypes of patients with lung adenocarcinoma and multiple logistic regression analysis of EGFR mutation association.
| Genotypes | EGFR wild type (N=109) | EGFR mutation (N=163) | AOR (95% CI) | p-value |
| rs3200401 | | | | |
| CC | 70 (64.2%) | 112 (68.7%) | 1.000 (reference) | |
| CT | 35 (32.1%) | 45 (27.6%) | 0.897 (0.507-1.588) | p=0.710 |
| TT | 4 (3.7%) | 6 (3.7%) | 0.900 (0.227-3.568) | p=0.881 |
| CT+TT | 39 (35.8%) | 51 (31.3%) | 0.947 (0.720-1.247) | p=0.699 |
| rs619586 | | | | |
| AA | 93 (85.3%) | 140 (85.9%) | 1.000 (reference) | |
| AG | 15 (13.8%) | 23 (14.1%) | 1.005 (0.476-2.123) | p=0.990 |
| GG | 1 (0.9%) | 0 (0.0%) | --- | --- |
| AG+GG | 16 (14.7%) | 23 (14.1%) | 0.959 (0.664-1.384) | p=0.822 |
| rs1194338 | | | | |
| CC | 43 (39.4%) | 73 (44.8%) | 1.000 (reference) | |
| CA | 47 (43.1%) | 68 (41.7%) | 0.898 (0.512-1.576) | p=0.708 |
| AA | 19 (17.5%) | 22 (13.5%) | 0.765 (0.354-1.650) | p=0.494 |
| CA+AA | 66 (60.6%) | 90 (55.2%) | 0.928 (0.714-1.206) | p=0.575 |
| The AORs with 95% CIs were estimated by multiple logistic regression models after controlling for genotypes. AOR, adjusted odds ratio; CI, confidence interval. |
Next, to further investigate the associations with MALAT1 genotypes for the dominant model (CC versus CT+TT) (rs3200401) in all LADC patients of clinicopathologic characteristics such as tumor stages, tumor T status, lymph node status, distant metastasis and cell differentiation. Statistical analysis showed no association between MALAT1 SNPs (rs3200401) and all LADC patients (Table 3). As shown in Table 4, the rs3200401 dominant model (CC versus CT+TT) was significantly associated with MALAT1 genotypes and EGFR wild-type at tumor stages (p=0.016), but not associated with tumor T status, lymph node status, distant metastasis and cell differentiation (Table 4).
Table 3. MALAT1 rs3200401 genotype distribution and clinicopathologic characteristics of lung adenocarcinoma patients.
| Variable | ALL (N=272) |
| CC (N=182) | CT + TT (N=90) | OR (95% CI) | p-value |
| stages | | | | |
| I+II | 43 (23.6%) | 28 (31.1%) | 1.00 | p=0.186 |
| III+IV | 139 (76.4%) | 62 (68.9%) | 0.685 (0.390-1.202) | |
| Tumor T status | | | | |
| T1+T2 | 105 (57.7%) | 57 (63.3%) | 1.00 | p=0.372 |
| T3+T4 | 77 (42.3%) | 33 (36.7%) | 0.789 (0.469-1.328) | |
| Lymph node status | | | | |
| Negative | 53 (29.1%) | 28 (31.1%) | 1.00 | p=0.736 |
| Positive | 129 (70.9%) | 62 (68.9%) | 0.910 (0.525-1.575) | |
| Distant metastasis | | | | |
| Negative | 87 (47.8%) | 43 (47.8%) | 1.00 | p=0.997 |
| Positive | 95 (52.2%) | 47 (52.2%) | 1.001 (0.604-1.660) | |
| Cell differentiation | | | | |
| Well/Moderately | 162 (89.0%) | 78 (86.7%) | 1.00 | p=0.572 |
| Poorly | 20 (11.0%) | 12 (13.3%) | 1.246 (0.580-2.678) | |
| The AORs with 95% CIs were estimated by multiple logistic regression models after controlling for variable. AOR, adjusted odds ratio; CI, confidence interval. |
Table 4. MALAT1 rs3200401 genotype distribution and clinicopathologic characteristics of EGFR wild type lung adenocarcinoma patients.
| Variable | EGFR wild type (N=109) |
| CC (N=70) | CT + TT (N=39) | OR (95% CI) | p-value |
| stages | | | | |
| I+II | 11 (15.7%) | 14 (35.9%) | 1.00 | p=0.016 |
| III+IV | 59 (84.3%) | 25 (64.1%) | 0.333 (0.133-0.834) | |
| Tumor T status | | | | |
| T1+T2 | 35 (50.0%) | 23 (59.0%) | 1.00 | p=0.368 |
| T3+T4 | 35 (50.0%) | 16 (41.0%) | 0.696 (0.315-1.535) | |
| Lymph node status | | | | |
| Negative | 16 (22.9%) | 12 (30.8%) | 1.00 | p=0.365 |
| Positive | 54 (77.1%) | 27 (69.2%) | 0.667 (0.277-1.607) | |
| Distant metastasis | | | | |
| Negative | 32 (45.7%) | 20 (51.3%) | 1.00 | p=0.577 |
| Positive | 38 (54.3%) | 19 (48.7%) | 0.800 (0.365-1.753) | |
| Cell differentiation | | | | |
| Well/Moderately | 55 (78.6%) | 31 (79.5%) | 1.00 | p=0.911 |
| Poorly | 15 (21.4%) | 8 (20.5%) | 0.946 (0.361-2.482) | |
| The AORs with 95% CIs were estimated by multiple logistic regression models after controlling for variable. AOR, adjusted odds ratio; CI, confidence interval. |
Further studies utilizing open-access datasets were carried out to determine the clinical significance of the MALAT1 expression in light of the genetic link between MALAT1 and LADC that was discovered. In The Cancer Genome Atlas (TCGA) dataset, we discovered that larger cases of tumors with LADC had lower MALAT1 mRNA expression levels at pathologic stage (all LADC patients: p=0.0226; EGFR wild-type patients: p=0.0159) (Figure 1A), and lymph node metastasis (all LADC patients: p=0.0003; EGFR wild-type patients: p=0.0018) (Figure 1B) in all LADC (Total) or EGFR wild-type, respectively. Moreover, LADC had lower MALAT1 mRNA expression levels at large tumor T status (p=0.0116) in all LADC patients (Figure 2A). To elucidate the prognostic role of MALAT1 in patients with LADC, the 5 years survival rates were estimated using Kaplan-Meier survival curves from all LADC (Total), EGFR wild-type and EGFR mutation, respectively. The log-rank test further confirmed that patients with low expression of MALAT1 had a significantly worse prognosis than patients with high expression of EGFR wild-type in LADC patients (Figure 2B).
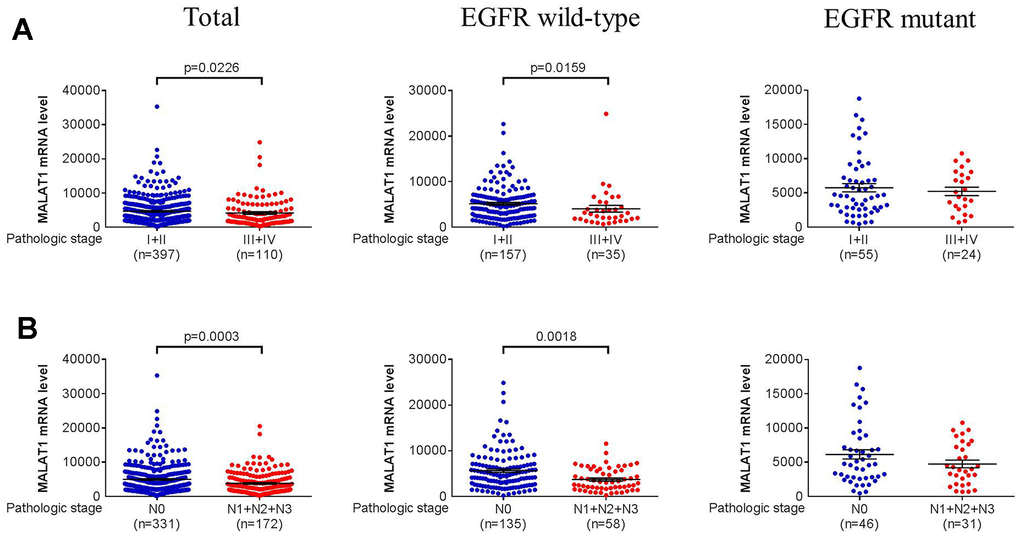
Figure 1. Pathologic stage and lymph node metastases in LADC were correlated with MALAT1 mRNA expression levels. (A, B) From the TCGA database, correlations between lower MALAT1 mRNA expression and pathologic stage or lymph node metastasis of total, EGFR wild-type and EGFR mutant in LADC. A p-value <0.05 was regarded as statistically significant using Student’s t-test.
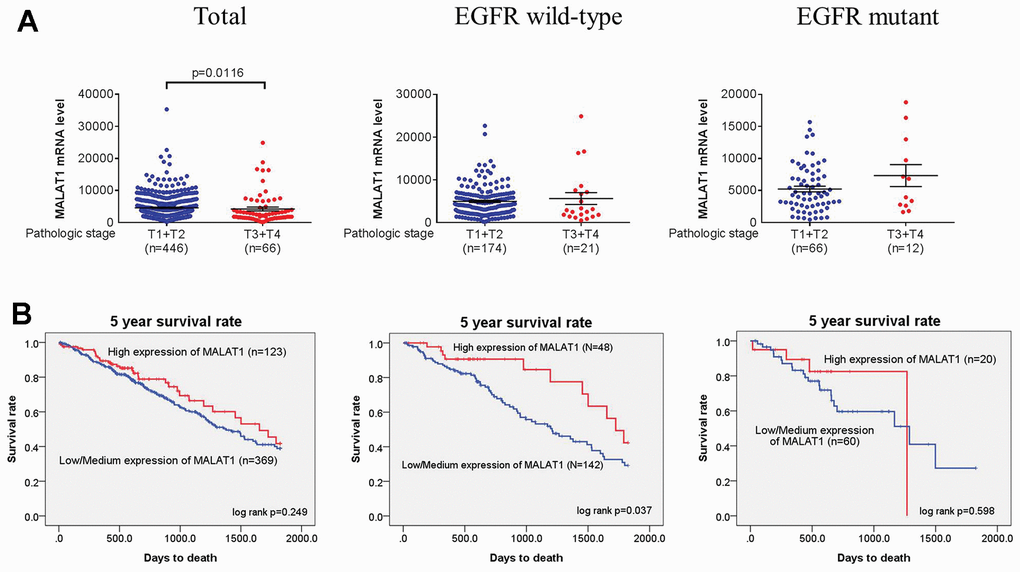
Figure 2. Tumor T status in LADC was correlated with MALAT1 mRNA expression levels or 5 years survival rates. (A, B) From the TCGA database, correlations between lower MALAT1 mRNA expression or 5 years survival rates and tumor T status of total, EGFR wild-type and EGFR mutant in LADC. A p-value <0.05 was regarded as statistically significant using Student’s t-test or log-rank test.
Discussion
MALAT1 lncRNA has recently been discovered to have a significant part in an expanding spectrum of illnesses and their progressions, including diabetes and its related complications [36, 37], inflammatory disorders such as Coronavirus disease 2019 (COVID-19) [38, 39], and sepsis, in addition to its well-known function in the progression of cancers [40, 41]. A pleiotropic role for MALAT1 in controlling gene expression and signaling pathways under different pathophysiological situations is suggested by the fact that it is ubiquitously linked with genomes in the areas crucial for transcriptional regulation as well as RNA processing [42]. As a result of its abundance and abnormal expression, MALAT1 lncRNA plays a critical role in the development of several malignancies, including lung cancer colorectal cancer, and bladder cancer [19, 43, 44]. According to reports, elevated MALAT1 expression is associated with a poor prognosis, tumor development, metastasis, chemoresistance, and tumor radioresistance [19, 45, 46].
According to evidence, structural changes caused by genetic variations in lncRNA may affect how it expresses or functions, which might participate in tumor development [47]. In recent years, studies have also revealed that genetic polymorphisms of MALAT1 have susceptibility to cancers [31, 32, 40]. In our study, the cohort of LUAD demographics and fundamental traits were comparable to those of previous Asian cohort [48, 49]; these cohort also showed that LUAD patients with an EGFR mutation were more likely to be female, never-smokers, and to have better cell differentiation than the EGFR wild-type group. The absence of smoking was linked to the development of LUAD, whereas EGFR mutations were more common among never-smoker (Table 1). Nevertheless, two researches showed that the MALAT1 SNPs (rs619586; A/G) dramatically decreased the risk of lung cancer, and the SNPs (rs3200401; CT) was linked to the susceptibility to NSCLC and lung squamous cell carcinoma (LSCC) in Chinese population [33, 34]. Moreover, previous study showed that the rs3200401C allele of the MALAT1 polymorphism could be a protective factor for cervical cancer development [50]. According to our findings, this is the first study to investigate relationships between MALAT1 SNPs (rs3200401, rs619586, and rs1194338) and the presence of EGFR mutations as well as clinicopathologic characteristics at a Taiwanese population in LUAD (Table 2). We provide a novel discovery that LUAD patients with tumor stages harboring MALAT1 (rs3200401; CC and CT+TT) heterozygotes had a significantly associated with EGFR wild-type (Table 4), but not in all LADC patients (Table 3).
The ability of certain lncRNAs to act as tumor suppressors or oncogenes, which are critical in the regulation of cell growth, division, and differentiation, has been demonstrated in earlier studies. These lncRNAs also employ multiple mechanisms to regulate cancer status, and the expression of lncRNAs may contribute to cancer initiation and progression [34]. MALAT1 was shown to be an abundant nuclear-enriched transcript that is expressed in healthy organs such the pancreas, lung, and nervous system. Elevated MALAT1 highly expression has been detected in lung cancer, endometrial stromal sarcoma, hepatocellular carcinoma, tongue squamous cell carcinoma, breast cancer and pancreatic cancer [34, 51, 52]. A study finds that lncRNA-MALAT1 is involved in NSCLC progression by targeting miR-202 [53]. Additionally, MALAT1 has also been used as a biomarker for lung cancer metastasis using a loss-of-function model demonstrates that MALAT1 has an active role in regulating gene expression that is responsible for preventing lung cancer metastasis [43]. High expression of MALAT1 promoted the progression of NSCLC through the extracellular signal-regulated kinase 1/2 (ERK)/mitogen-activated protein kinase (MAPK) signaling pathway [54].
In our study, we further investigated that clinical significance of the mRNA expression in light of the genetic link between MALAT1 and pathologic stage at EGFR wild-type and EGFR mutation in LADC. Lower expression mRNA levels of MALAT1 were associated with pathologic stage (Figure 1A) and lymph node metastasis (Figure 1B) and tumor T status in all LADC or EGFR wild-type. Intriguingly, the TCGA study revealed that patients with LADC who had low expression of MALAT1 had a considerably poorer prognosis than those who had high expression of EGFR wild-type (Figure 2B). Nevertheless, previous studies have shown that MALAT1 functions as an oncogene in cancer [55, 56]; however, our data suggest that MALAT1 may have a tumor suppressor function in lung cancer cells which is consistent with previous result [33, 57].
While interpreting our findings, it is important to consider the present study of limitations. In this study, the sample size of patients was still insufficient which may have limited statistical impact on the accuracy and precision of the results and a larger independent cohort was required to further confirm the influence of MALAT1 SNPs on EGFR mutation susceptibility and LUAD development. In addition, this study is limited to the Taiwanese population and other ethnic groups still need to be compared with the current results. Additionally, the relationship between MALAT1 genetic variations and its level of expression in LUAD cannot be supported by our research. Consequently, it is necessary to collect both mRNA and DNA from the same sample and to further confirm this issue in future research.
In summary, our results provide evidence that in Taiwanese population, the polymorphisms rs3200401 in MALAT1 was associated with the risk and low expression of MALAT1 had a significantly worse prognosis of EGFR wild-type in LUAD. It will need further research to confirm or disprove the findings of this preliminary investigation.
Materials and Methods
Study subjects and sample collection
A total of 272 patients with lung adenocarcinoma were recruited for the present study, either with or without an EGFR mutation. For each patient, the medical records were consulted to determine their age, gender, cigarette smoking status, tumor stage, tumor T status, lymph node status, distant metastasis and cell differentiation. Clinical staging was determined using the TNM staging approach according to the seventh edition of the American Joint Committee on Cancer (AJCC) Staging Manual for each patient. After gaining the fully informed permission of all participants, the study proposal was approved by the Institutional Review Board (IRB) at Chung Shan Medical University Hospital (IRB No. CS1-20144).
Genomic MALAT1 SNPs detected from peripheral blood in LUAD patients
Genomic DNA was extracted using a QIAamp DNA blood micro kit from peripheral blood samples of the research participants (Qiagen, Valencia, CA, USA). The allelic discrimination of these three MALAT1 SNPs including rs3200401 (assay ID: C_3246069_10), rs619586 (assay ID: C_1060479_10), and rs1194338 (assay ID: C_11661801_10) was evaluated by utilizing the TaqMan SNP Genotyping Assay by using the ABI StepOnePlusTM Real-Time PCR System (Applied Biosystems, Foster City, CA, USA). ABI SDS version 3.0 software was used to compute the allelic frequency [9, 29].
Statistical analysis
The multiple logistic regression methods were used to calculate the genotype with LUAD risk correlation while controlling for relevant variables. The multiple logistic regression models were used to evaluate adjusted odds ratios (AORs) and 95% confidence intervals (CIs). Using the Mann-Whitney U test or Fisher’s exact test, significant differences in demographic data between EGFR mutation and EGFR wild-type controls were assessed in LUAD patients. For the potential association between MALAT1 expression and clinical status of LUAD, we use the data of lung adenocarcinoma obtained from The Cancer Genome Atlas (TCGA) to analyze this issue [58]. Furthermore, the cumulative survival rates were determined using the log-rank test, and the Student’s t-test was used to compare the MALAT1 expression levels. The analyses were performed using Statistical Product and Service Solutions (SPSS, version 17) (SPSS, Inc., Chicago, IL, USA). A p-value <0.05 was regarded as statistically significant.
Data availability statement
The data used to support the findings of the present study are available from the corresponding author upon request.
Author Contributions
SHL, JWL, PJY and SFY conceived and designed this study. SHL, WTH, YEC and SFY performed the experiments. SHL and SFY analyzed the data. TCS, TJT, and YJT helped discuss the results. SHL, JWL, PJY and SFY drafted and edited the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank the Human Biobank of Chung Shan Medical University Hospital, Taichung, Taiwan for specimen preparation.
Conflicts of Interest
The authors declare that there are no conflicts of interest.
Ethical Statement and Consent
The study was approved by the Institutional Review Board (IRB) at Chung Shan Medical University Hospital (IRB No. CS1-20144). Informed permission of all participants was obtained.
Funding
No funding was provided for this study.
References
-
1.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71:209–49. https://doi.org/10.3322/caac.21660 [PubMed]
-
2.
Travis WD. Pathology of lung cancer. Clin Chest Med. 2011; 32:669–92. https://doi.org/10.1016/j.ccm.2011.08.005 [PubMed]
-
3.
Shi J, Hua X, Zhu B, Ravichandran S, Wang M, Nguyen C, Brodie SA, Palleschi A, Alloisio M, Pariscenti G, Jones K, Zhou W, Bouk AJ, et al. Somatic Genomics and Clinical Features of Lung Adenocarcinoma: A Retrospective Study. PLoS Med. 2016; 13:e1002162. https://doi.org/10.1371/journal.pmed.1002162 [PubMed]
-
4.
Hao CC, Xu CY, Zhao XY, Luo JN, Wang G, Zhao LH, Ge X, Ge XF. Up-regulation of VANGL1 by IGF2BPs and miR-29b-3p attenuates the detrimental effect of irradiation on lung adenocarcinoma. J Exp Clin Cancer Res. 2020; 39:256. https://doi.org/10.1186/s13046-020-01772-y [PubMed]
-
5.
Yu Y, Wang Z, Zheng Q, Li J. FAM72 serves as a biomarker of poor prognosis in human lung adenocarcinoma. Aging (Albany NY). 2021; 13:8155–76. https://doi.org/10.18632/aging.202625 [PubMed]
-
6.
Moreira AL, Eng J. Personalized therapy for lung cancer. Chest. 2014; 146:1649–57. https://doi.org/10.1378/chest.14-0713 [PubMed]
-
7.
Tanaka T, Matsuoka M, Sutani A, Gemma A, Maemondo M, Inoue A, Okinaga S, Nagashima M, Oizumi S, Uematsu K, Nagai Y, Moriyama G, Miyazawa H, et al. Frequency of and variables associated with the EGFR mutation and its subtypes. Int J Cancer. 2010; 126:651–5. https://doi.org/10.1002/ijc.24746 [PubMed]
-
8.
Jin CY, Du L, Nuerlan AH, Wang XL, Yang YW, Guo R. High expression of RRM2 as an independent predictive factor of poor prognosis in patients with lung adenocarcinoma. Aging (Albany NY). 2020; 13:3518–35. https://doi.org/10.18632/aging.202292 [PubMed]
-
9.
Chang JH, Lai TC, Yang PJ, Shih PC, Yang YC, Lee KL, Liu TC, Tsao TC, Yang SF, Chien MH. Associations of TIMP-3 Genetic Polymorphisms with EGFR Statuses and Cancer Clinicopathologic Development in Lung Adenocarcinoma Patients. Int J Mol Sci. 2020; 21:8023. https://doi.org/10.3390/ijms21218023 [PubMed]
-
10.
Lin CH, Yang PJ, Lin SH, Yeh KT, Tsao TC, Chen YE, Lin SH, Yang SF. Association between EGFR Gene Mutation and Antioxidant Gene Polymorphism of Non-Small-Cell Lung Cancer. Diagnostics (Basel). 2020; 10:692. https://doi.org/10.3390/diagnostics10090692 [PubMed]
-
11.
Wu YL, Chien MH, Chou YE, Chang JH, Liu TC, Tsao TC, Chou MC, Yang SF. Association of EGFR mutations and HMGB1 genetic polymorphisms in lung adenocarcinoma patients. J Cancer. 2019; 10:2907–14. https://doi.org/10.7150/jca.31125 [PubMed]
-
12.
Sana J, Faltejskova P, Svoboda M, Slaby O. Novel classes of non-coding RNAs and cancer. J Transl Med. 2012; 10:103. https://doi.org/10.1186/1479-5876-10-103 [PubMed]
-
13.
Arun G, Diermeier SD, Spector DL. Therapeutic Targeting of Long Non-Coding RNAs in Cancer. Trends Mol Med. 2018; 24:257–77. https://doi.org/10.1016/j.molmed.2018.01.001 [PubMed]
-
14.
Su SC, Yeh CM, Lin CW, Hsieh YH, Chuang CY, Tang CH, Lee YC, Yang SF. A novel melatonin-regulated lncRNA suppresses TPA-induced oral cancer cell motility through replenishing PRUNE2 expression. J Pineal Res. 2021; 71:e12760. https://doi.org/10.1111/jpi.12760 [PubMed]
-
15.
Yeh JC, Chen YT, Chou YE, Su SC, Chang LC, Chen YL, Lin CW, Yang SF. Interactive effects of CDKN2B-AS1 gene polymorphism and habitual risk factors on oral cancer. J Cell Mol Med. 2023; 27:3395–403. https://doi.org/10.1111/jcmm.17966 [PubMed]
-
16.
Su SC, Hsieh MJ, Lin CW, Chuang CY, Liu YF, Yeh CM, Yang SF. Impact of HOTAIR Gene Polymorphism and Environmental Risk on Oral Cancer. J Dent Res. 2018; 97:717–24. https://doi.org/10.1177/0022034517749451 [PubMed]
-
17.
Ji P, Diederichs S, Wang W, Böing S, Metzger R, Schneider PM, Tidow N, Brandt B, Buerger H, Bulk E, Thomas M, Berdel WE, Serve H, Müller-Tidow C. MALAT-1, a novel noncoding RNA, and thymosin beta4 predict metastasis and survival in early-stage non-small cell lung cancer. Oncogene. 2003; 22:8031–41. https://doi.org/10.1038/sj.onc.1206928 [PubMed]
-
18.
Shen L, Chen L, Wang Y, Jiang X, Xia H, Zhuang Z. Long noncoding RNA MALAT1 promotes brain metastasis by inducing epithelial-mesenchymal transition in lung cancer. J Neurooncol. 2015; 121:101–8. https://doi.org/10.1007/s11060-014-1613-0 [PubMed]
-
19.
Zheng HT, Shi DB, Wang YW, Li XX, Xu Y, Tripathi P, Gu WL, Cai GX, Cai SJ. High expression of lncRNA MALAT1 suggests a biomarker of poor prognosis in colorectal cancer. Int J Clin Exp Pathol. 2014; 7:3174–81. [PubMed]
-
20.
Pang EJ, Yang R, Fu XB, Liu YF. Overexpression of long non-coding RNA MALAT1 is correlated with clinical progression and unfavorable prognosis in pancreatic cancer. Tumour Biol. 2015; 36:2403–7. https://doi.org/10.1007/s13277-014-2850-8 [PubMed]
-
21.
Zhang HM, Yang FQ, Chen SJ, Che J, Zheng JH. Upregulation of long non-coding RNA MALAT1 correlates with tumor progression and poor prognosis in clear cell renal cell carcinoma. Tumour Biol. 2015; 36:2947–55. https://doi.org/10.1007/s13277-014-2925-6 [PubMed]
-
22.
Liu J, Dong H, Yang Y, Qian Y, Liu J, Li Z, Guan H, Chen Z, Li C, Zhang K, Zhang Q, Cao W, Lv J. Upregulation of long noncoding RNA MALAT1 in papillary thyroid cancer and its diagnostic value. Future Oncol. 2018; 14:3015–22. https://doi.org/10.2217/fon-2018-0416 [PubMed]
-
23.
Liao X, Chen J, Luo D, Luo B, Huang W, Xie W. Prognostic value of long non-coding RNA MALAT1 in hepatocellular carcinoma: A study based on multi-omics analysis and RT-PCR validation. Pathol Oncol Res. 2023; 28:1610808. https://doi.org/10.3389/pore.2022.1610808 [PubMed]
-
24.
Qian Z, Chen L, Wang X, Kan Y, Wang Y, Yu Y, Wang X, Zhao Z, Yang H, Ge P, Ding T, Zhai Q, Zhao H. Increased MALAT1 expression predicts poor prognosis in primary gastrointestinal diffuse large B-cell lymphoma. Clin Exp Med. 2022; 22:183–91. https://doi.org/10.1007/s10238-021-00748-2 [PubMed]
-
25.
Bowden SJ, Bodinier B, Kalliala I, Zuber V, Vuckovic D, Doulgeraki T, Whitaker MD, Wielscher M, Cartwright R, Tsilidis KK, Bennett P, Jarvelin MR, Flanagan JM, et al, and FinnGen consortium. Genetic variation in cervical preinvasive and invasive disease: a genome-wide association study. Lancet Oncol. 2021; 22:548–57. https://doi.org/10.1016/S1470-2045(21)00028-0 [PubMed]
-
26.
Bau DT, Liu TY, Tsai CW, Chang WS, Gu J, Yang JS, Shih LC, Tsai FJ. A Genome-Wide Association Study Identified Novel Genetic Susceptibility Loci for Oral Cancer in Taiwan. Int J Mol Sci. 2023; 24:2789. https://doi.org/10.3390/ijms24032789 [PubMed]
-
27.
Lv Z, Xu Q, Yuan Y. A systematic review and meta-analysis of the association between long non-coding RNA polymorphisms and cancer risk. Mutat Res Rev Mutat Res. 2017; 771:1–14. https://doi.org/10.1016/j.mrrev.2016.10.002 [PubMed]
-
28.
Su SC, Reiter RJ, Hsiao HY, Chung WH, Yang SF. Functional Interaction between Melatonin Signaling and Noncoding RNAs. Trends Endocrinol Metab. 2018; 29:435–45. https://doi.org/10.1016/j.tem.2018.03.008 [PubMed]
-
29.
Yuan LT, Chang JH, Lee HL, Yang YC, Su SC, Lin CL, Yang SF, Chien MH. Genetic Variants of lncRNA MALAT1 Exert Diverse Impacts on the Risk and Clinicopathologic Characteristics of Patients with Hepatocellular Carcinoma. J Clin Med. 2019; 8:1406. https://doi.org/10.3390/jcm8091406 [PubMed]
-
30.
Sun YH, Chou YH, Tsai HY, Hsiao YH, Lee CY, Yang SF, Ting KH, Wang PH. Impact of Genetic Variants of Long Noncoding RNA Metastasis-Associated Lung Adenocarcinoma Transcript 1 on Uterine Cervical Cancer. J Cancer. 2022; 13:2150–8. https://doi.org/10.7150/jca.70730 [PubMed]
-
31.
Ding YF, Wen YC, Chuang CY, Lin CW, Yang YC, Liu YF, Chang WM, Chang LC, Yang SF, Chien MH. Combined Impacts of Genetic Variants of Long Non-Coding RNA MALAT1 and the Environmental Carcinogen on the Susceptibility to and Progression of Oral Squamous Cell Carcinoma. Front Oncol. 2021; 11:684941. https://doi.org/10.3389/fonc.2021.684941 [PubMed]
-
32.
Hu JC, Wang SS, Chou YE, Chiu KY, Li JR, Chen CS, Hung SC, Yang CK, Ou YC, Cheng CL, Lin CY, Yang SF. Associations between LncRNA MALAT1 Polymorphisms and Lymph Node Metastasis in Prostate Cancer. Diagnostics (Basel). 2021; 11:1692. https://doi.org/10.3390/diagnostics11091692 [PubMed]
-
33.
Tong G, Tong W, He R, Cui Z, Li S, Zhou B, Yin Z. MALAT1 Polymorphisms and Lung Cancer Susceptibility in a Chinese Northeast Han Population. Int J Med Sci. 2022; 19:1300–6. https://doi.org/10.7150/ijms.73026 [PubMed]
-
34.
Chen M, Cai D, Gu H, Yang J, Fan L. MALAT1 rs619586 A/G polymorphisms are associated with decreased risk of lung cancer. Medicine (Baltimore). 2021; 100:e23716. https://doi.org/10.1097/MD.0000000000023716 [PubMed]
-
35.
Wei R, Cao L, Pu H, Wang H, Zheng Y, Niu X, Weng X, Zhang H, Favus M, Zhang L, Jia W, Zeng Y, Amos CI, et al. TERT Polymorphism rs2736100-C Is Associated with EGFR Mutation-Positive Non-Small Cell Lung Cancer. Clin Cancer Res. 2015; 21:5173–80. https://doi.org/10.1158/1078-0432.CCR-15-0009 [PubMed]
-
36.
Chen J, Ke S, Zhong L, Wu J, Tseng A, Morpurgo B, Golovko A, Wang G, Cai JJ, Ma X, Li D, Tian Y. Long noncoding RNA MALAT1 regulates generation of reactive oxygen species and the insulin responses in male mice. Biochem Pharmacol. 2018; 152:94–103. https://doi.org/10.1016/j.bcp.2018.03.019 [PubMed]
-
37.
Chen J, Tang S, Ke S, Cai JJ, Osorio D, Golovko A, Morpurgo B, Guo S, Sun Y, Winkle M, Calin GA, Tian Y. Ablation of long noncoding RNA MALAT1 activates antioxidant pathway and alleviates sepsis in mice. Redox Biol. 2022; 54:102377. https://doi.org/10.1016/j.redox.2022.102377 [PubMed]
-
38.
Rodrigues AC, Adamoski D, Genelhould G, Zhen F, Yamaguto GE, Araujo-Souza PS, Nogueira MB, Raboni SM, Bonatto AC, Gradia DF, Carvalho de Oliveira J. NEAT1 and MALAT1 are highly expressed in saliva and nasopharyngeal swab samples of COVID-19 patients. Mol Oral Microbiol. 2021; 36:291–4. https://doi.org/10.1111/omi.12351 [PubMed]
-
39.
Huang K, Wang C, Vagts C, Raguveer V, Finn PW, Perkins DL. Long non-coding RNAs (lncRNAs) NEAT1 and MALAT1 are differentially expressed in severe COVID-19 patients: An integrated single-cell analysis. PLoS One. 2022; 17:e0261242. https://doi.org/10.1371/journal.pone.0261242 [PubMed]
-
40.
Cao L, Yan G, Yu S, Li F, Su Z, Hou X, Xiao J, Tian T. Associations of MALAT1 and its functional single nucleotide polymorphisms with cancer. Pathol Res Pract. 2022; 236:153988. https://doi.org/10.1016/j.prp.2022.153988 [PubMed]
-
41.
Hou J, Zhang G, Wang X, Wang Y, Wang K. Functions and mechanisms of lncRNA MALAT1 in cancer chemotherapy resistance. Biomark Res. 2023; 11:23. https://doi.org/10.1186/s40364-023-00467-8 [PubMed]
-
42.
Engreitz JM, Sirokman K, McDonel P, Shishkin AA, Surka C, Russell P, Grossman SR, Chow AY, Guttman M, Lander ES. RNA-RNA interactions enable specific targeting of noncoding RNAs to nascent Pre-mRNAs and chromatin sites. Cell. 2014; 159:188–99. https://doi.org/10.1016/j.cell.2014.08.018 [PubMed]
-
43.
Gutschner T, Hämmerle M, Eissmann M, Hsu J, Kim Y, Hung G, Revenko A, Arun G, Stentrup M, Gross M, Zörnig M, MacLeod AR, Spector DL, Diederichs S. The noncoding RNA MALAT1 is a critical regulator of the metastasis phenotype of lung cancer cells. Cancer Res. 2013; 73:1180–9. https://doi.org/10.1158/0008-5472.CAN-12-2850 [PubMed]
-
44.
Fan Y, Shen B, Tan M, Mu X, Qin Y, Zhang F, Liu Y. TGF-β-induced upregulation of malat1 promotes bladder cancer metastasis by associating with suz12. Clin Cancer Res. 2014; 20:1531–41. https://doi.org/10.1158/1078-0432.CCR-13-1455 [PubMed]
-
45.
Liu JH, Chen G, Dang YW, Li CJ, Luo DZ. Expression and prognostic significance of lncRNA MALAT1 in pancreatic cancer tissues. Asian Pac J Cancer Prev. 2014; 15:2971–7. https://doi.org/10.7314/apjcp.2014.15.7.2971 [PubMed]
-
46.
Shen W, Yu Q, Pu Y, Xing C. Upregulation of Long Noncoding RNA MALAT1 in Colorectal Cancer Promotes Radioresistance and Aggressive Malignance. Int J Gen Med. 2022; 15:8365–80. https://doi.org/10.2147/IJGM.S393270 [PubMed]
-
47.
Schmitt AM, Chang HY. Long Noncoding RNAs in Cancer Pathways. Cancer Cell. 2016; 29:452–63. https://doi.org/10.1016/j.ccell.2016.03.010 [PubMed]
-
48.
Lee KL, Lai TC, Wang YC, Shih PC, Yang YC, Tsao TC, Liu TC, Wen YC, Chang LC, Yang SF, Chien MH. Potential Impacts of Interleukin-17A Promoter Polymorphisms on the EGFR Mutation Status and Progression of Non-Small Cell Lung Cancer in Taiwan. Genes (Basel). 2021; 12:427. https://doi.org/10.3390/genes12030427 [PubMed]
-
49.
Hsieh MH, Wu YL, Tsao TC, Huang YW, Lin JC, Lee CY, Hsieh MJ, Yang SF. Impact of LncRNA GAS5 Genetic Variants and the Epidermal Growth Factor Receptor Phenotypes on the Clinicopathological Characteristics of Lung Adenocarcinoma Patients. Int J Environ Res Public Health. 2022; 19:9971. https://doi.org/10.3390/ijerph19169971 [PubMed]
-
50.
Yao Y, Liang Y, Dong X, Liu S, Zhang S, Liu W, Li Y, Shi L, Yan Z, Yao Y. Association of Long Non-Coding RNAs (lncRNAs) ANRIL and MALAT1 Polymorphism with Cervical Cancer. Pharmgenomics Pers Med. 2022; 15:359–75. https://doi.org/10.2147/PGPM.S358453 [PubMed]
-
51.
Hauptman N, Glavač D. Long non-coding RNA in cancer. Int J Mol Sci. 2013; 14:4655–69. https://doi.org/10.3390/ijms14034655 [PubMed]
-
52.
Hussein AA, Forouzanfar T, Bloemena E, de Visscher J, Brakenhoff RH, Leemans CR, Helder MN. A review of the most promising biomarkers for early diagnosis and prognosis prediction of tongue squamous cell carcinoma. Br J Cancer. 2018; 119:724–36. https://doi.org/10.1038/s41416-018-0233-4 [PubMed]
-
53.
Tiansheng G, Junming H, Xiaoyun W, Peixi C, Shaoshan D, Qianping C. lncRNA Metastasis-Associated Lung Adenocarcinoma Transcript 1 Promotes Proliferation and Invasion of Non-Small Cell Lung Cancer Cells via Down-Regulating miR-202 Expression. Cell J. 2020; 22:375–85. https://doi.org/10.22074/cellj.2020.6837 [PubMed]
-
54.
Liu C, Li H, Jia J, Ruan X, Liu Y, Zhang X. High Metastasis-Associated Lung Adenocarcinoma Transcript 1 (MALAT1) Expression Promotes Proliferation, Migration, and Invasion of Non-Small Cell Lung Cancer via ERK/Mitogen-Activated Protein Kinase (MAPK) Signaling Pathway. Med Sci Monit. 2019; 25:5143–9. https://doi.org/10.12659/MSM.913308 [PubMed]
-
55.
Fu S, Wang Y, Li H, Chen L, Liu Q. Regulatory Networks of LncRNA MALAT-1 in Cancer. Cancer Manag Res. 2020; 12:10181–98. https://doi.org/10.2147/CMAR.S276022 [PubMed]
-
56.
Li ZX, Zhu QN, Zhang HB, Hu Y, Wang G, Zhu YS. MALAT1: a potential biomarker in cancer. Cancer Manag Res. 2018; 10:6757–68. https://doi.org/10.2147/CMAR.S169406 [PubMed]
-
57.
Guo L, Zhang X, Pan H, Li Y, Wang J, Li L, Dong Y, Du X, Chen J, Guo F. Prognostic and immunological significance of metastasis associated lung adenocarcinoma transcript 1 among different kinds of cancers. Bioengineered. 2021; 12:4247–58. https://doi.org/10.1080/21655979.2021.1955511 [PubMed]
-
58.
Tung MC, Wen YC, Wang SS, Lin YW, Liu YC, Yang SF, Chien MH. Dopamine receptor D2 genetic variations is associated with the risk and clinicopathological variables of urothelial cell carcinoma in a Taiwanese population. Int J Med Sci. 2018; 15:1187–93. https://doi.org/10.7150/ijms.26895 [PubMed]