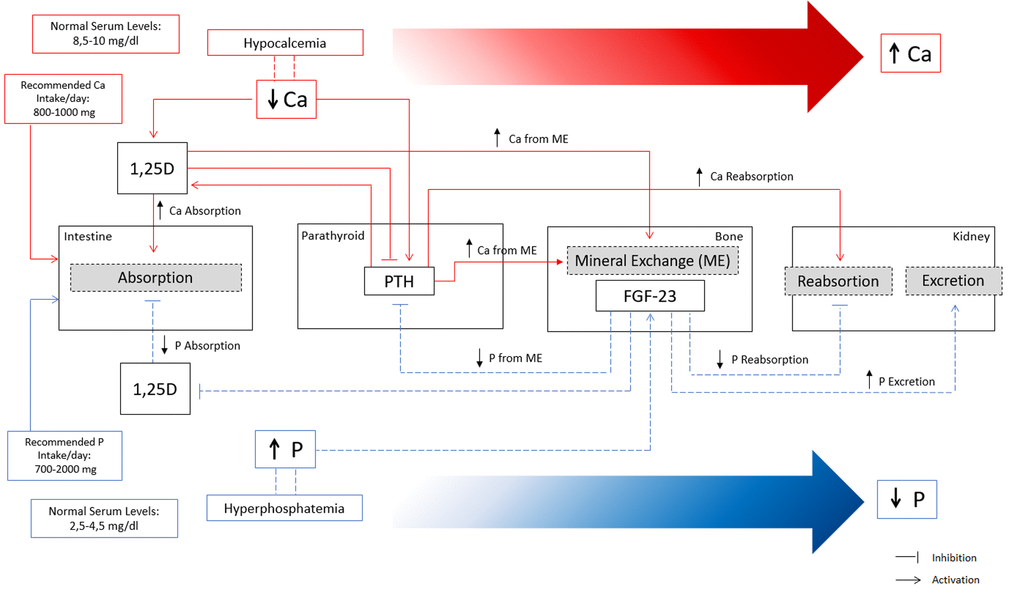
Figure 1.Overview of calcium (Ca) and phosphate (P) homeostatic regulation. Red lines represent the main mechanisms of Ca regulation in a situation of hypocalcemia. Decreased Ca levels in serum increase 1,25D and PTH. Increased levels of 1,25D increase Ca absorption at the intestine and stimulate mineral exchange in bone increasing Ca efflux. Increased PTH stimulate mineral exchange in bone increasing Ca efflux, and increase Ca reabsorption in the kidney. Indirectly, high levels of PTH stimulate 1,25D with consequent increase in Ca absorption. Overall, the concerted action of PTH and 1,25D lead to increased serum Ca levels until the normal range by increasing Ca reabsorption at the intestine, increasing Ca from mineral exchange in bone, and increasing Ca reabsorption in the kidneys. Blue lines represent the main mechanisms of P regulation in a situation of hyperphosphatemia. High levels of serum P increase FGF-23 production in bone, which exerts several effects to promote a decrease in serum P. FGF-23 decreases P reabsorption and increases P excretion in the kidneys, and indirectly decreases P absorption at the intestine and P efflux from bone mineral exchange, through the inhibition of 1,25D and PTH.