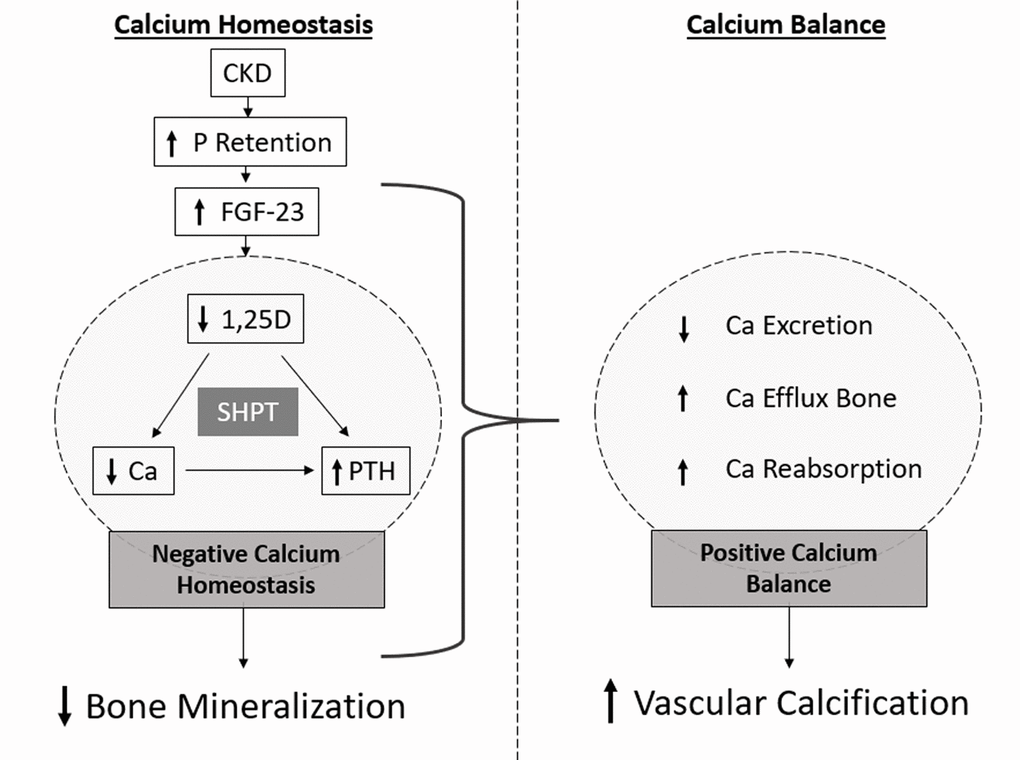
Figure 2.Schematic representation of the mineralization paradox in CKD. As kidney functional declines, P retention occurs and FGF-23 highly increases, with consequent decrease in 1,25D levels. Dysregulated levels of 1,25D lead to increased levels of PTH and decreased levels of serum Ca. Low levels of serum Ca maintained by low 1,25D, constantly stimulate PTH production, often resulting in secondary hyperparathyroidism (SHPT) and bone resorption leading to decreased bone mineralization. However, increased Ca efflux from bone, and increased Ca reabsorption and decreased excretion in the kidneys originate a positive Ca balance, correlated with increased vascular calcification.