



Introduction
Prostate cancer is the most prevalent cancer in men in Western societies [1]. Although the majority of prostate cancers behave in an indolent manner, a small subset is highly aggressive and requires extensive treatment [2]. Established preoperative prognostic parameters are limited to Gleason grade and tumor extent on biopsies, serum prostate-specific antigen (PSA), levels and clinical stage. These parameters are statistically strong, but not sufficient to enable optimal treatment decisions in every patient. It is, thus, hoped that a better understanding of disease biology will eventually lead to the identification of clinically applicable molecular markers that enable a more reliable prediction of prostate cancer aggressiveness.
Rho-associated coiled-coil containing kinase 1 (ROCK1) belongs to the family of so-called AGC kinases comprising more than 60 evolutionary related serin/threonine protein kinases including important anti-cancer targets such as AKT, p70S6 kinase, or GSK-3ß [3]. ROCK1 is a critical regulator of the shape and motility of mammalian cells by acting on the cytoskeleton. ROCK1 indirectly controls polymerization and depolymerization of actin filaments through activation of its downstream targets LIM kinase and cofilin and promotes contraction of actin fibers through phosphorylation of myosin light chains [3]. Besides its impact on cell motility, ROCK1 has also been implicated in cell growth and cell-cell adhesion. Earlier work has demonstrated that ROCK1 can stimulate PTEN activity [4], inhibit premature centriole separation during cytokinesis [5], antagonize insulin-like growths factor signaling, and facilitate disruption of E-cadherin dependent cell-cell contacts [6]. Two homologs have been identified, ROCK1 and ROCK2, which are encoded by distinct genes [3] but show a high amino acid sequence similarity especially in the kinase domain [7]. Particularly ROCK1 appears to be relevant in many human cancer types, as immunohistochemistry studies reported associations between adverse tumor features and increased ROCK1 protein levels in breast [8], colorectal [9], and gastric cancers [10] as well as in osteosarcomas [11]. Moreover, ROCK1 is a putative drug target as ROCK1 inhibitors are currently tested in clinical trials on advanced solid cancers (e.g. NCT01585701).
ROCK1 may be also implicated in prostate cancer biology. ROCK1 is androgen responsive [12], inhibits apoptosis [13] and promotes cell motility and proliferation [14] in prostate cancer cells. Genetic variants of RhoA and ROCK1 genes have been suggested as susceptibility factors for prostate cancer development [15]. One recent study on 56 prostate cancers and adjacent normal tissue reported a higher level of ROCK1 protein expression in tumor glands as compared to normal tissues [16]. To better understand the potential clinical impact of ROCK1 protein expression in prostate cancer we took advantage of our large prognosis tissue microarray (TMA) with its attached database on clinical, pathological and molecular data and studied patterns of ROCK1 expression in more than 12 000 prostate cancer patients by immunohistochemistry.
Results
A total of 10 613/12 427 (85.4%) tumor samples were interpretable in our TMA analysis. Reasons for non-informative cases included lack of tissue samples or absence of unequivocal cancer tissue in the TMA spot in 1814/12 427 (14.6%) tumors.
ROCK1 expression in normal and cancerous prostate tissues
Normal prostate glands showed weak cytoplasmic staining of luminal and basal cells. In cancers, at least weak ROCK1 staining was found in 92% of the cases, and was considered weak in 22%, moderate in 53%, and strong in 18% of tumors (Table 1). Samples with adjacent normal and cancerous glands revealed that staining was typically stronger in cancer cells as compared to normal prostate glands. Representative images of ROCK1 immunostainings in normal and cancerous glands are shown in Figure 1.
Table 1. Association between ROCK1 staining and prostate cancer phenotype in all cancers.
| Parameter | ROCK1 (%) | |||||
| N | Negative | Weak | Moderate | Strong | P | |
| All cancers | 10 613 | 8.0 | 21.5 | 52.6 | 17.9 | |
| Tumor stage | <0.0001 | |||||
| pT2 | 6893 | 8.9 | 22.6 | 53.5 | 15.1 | |
| pT3a | 2335 | 6.9 | 19.8 | 52.3 | 21.0 | |
| pT3b-pT4 | 1340 | 5.1 | 19.0 | 48.7 | 27.2 | |
| Gleason grade | <0.0001 | |||||
| ≤3+3 | 2336 | 12.6 | 29.5 | 50.2 | 7.7 | |
| 3+4 | 5830 | 7.1 | 20.0 | 54.8 | 18.1 | |
| 3+4 Tertiary 5 | 383 | 6.3 | 18.8 | 55.4 | 19.6 | |
| 4+3 | 1099 | 5.2 | 18.4 | 48.9 | 27.6 | |
| 4+3 Tertiary 5 | 609 | 3.9 | 15.8 | 52.1 | 28.2 | |
| ≥4+4 | 521 | 5.2 | 17.3 | 48.9 | 28.6 | |
| Quantitative Gleason grade | <0.0001 | |||||
| ≤3+3 | 2336 | 12.6 | 29.5 | 50.2 | 7.7 | |
| 3+4 ≤5% | 1545 | 8.1 | 22.5 | 54.6 | 14.9 | |
| 3+4 6–10% | 1514 | 7.7 | 19.9 | 55.7 | 16.7 | |
| 3+4 11–20% | 1251 | 7.1 | 18.1 | 54.4 | 20.4 | |
| 3+4 21–30% | 681 | 5.3 | 17.2 | 55.4 | 22.2 | |
| 3+4 31–49% | 536 | 5.6 | 20.7 | 50.6 | 23.1 | |
| 3+4 Tertiary 5 | 383 | 6.3 | 18.8 | 55.4 | 19.6 | |
| 4+3 50–60% | 462 | 5.6 | 20.1 | 50.2 | 24.0 | |
| 4+3 61–100% | 609 | 3.9 | 15.8 | 52.1 | 28.2 | |
| 4+3 Tertiary 5 | 513 | 4.7 | 16.0 | 47.0 | 32.4 | |
| ≥4+4 | 521 | 5.2 | 17.3 | 48.9 | 28.6 | |
| Lymph node metastasis | <0.0001 | |||||
| N0 | 5963 | 7.1 | 19.3 | 53.1 | 20.5 | |
| N+ | 607 | 4.9 | 16.3 | 48.8 | 30.0 | |
| Preoperative PSA level (ng/ml) | 0.0111 | |||||
| <4 | 1324 | 6.1 | 21.2 | 53.9 | 18.8 | |
| 4–10 | 6348 | 7.8 | 21.0 | 53.3 | 17.9 | |
| 10–20 | 2106 | 9.4 | 22.9 | 50.6 | 17.0 | |
| >20 | 720 | 8.8 | 22.2 | 49.7 | 19.3 | |
| Surgical margin | <0.0001 | |||||
| Negative | 8463 | 8.0 | 21.7 | 53.3 | 17.0 | |
| Positive | 1959 | 7.8 | 21.4 | 49.4 | 21.4 | |
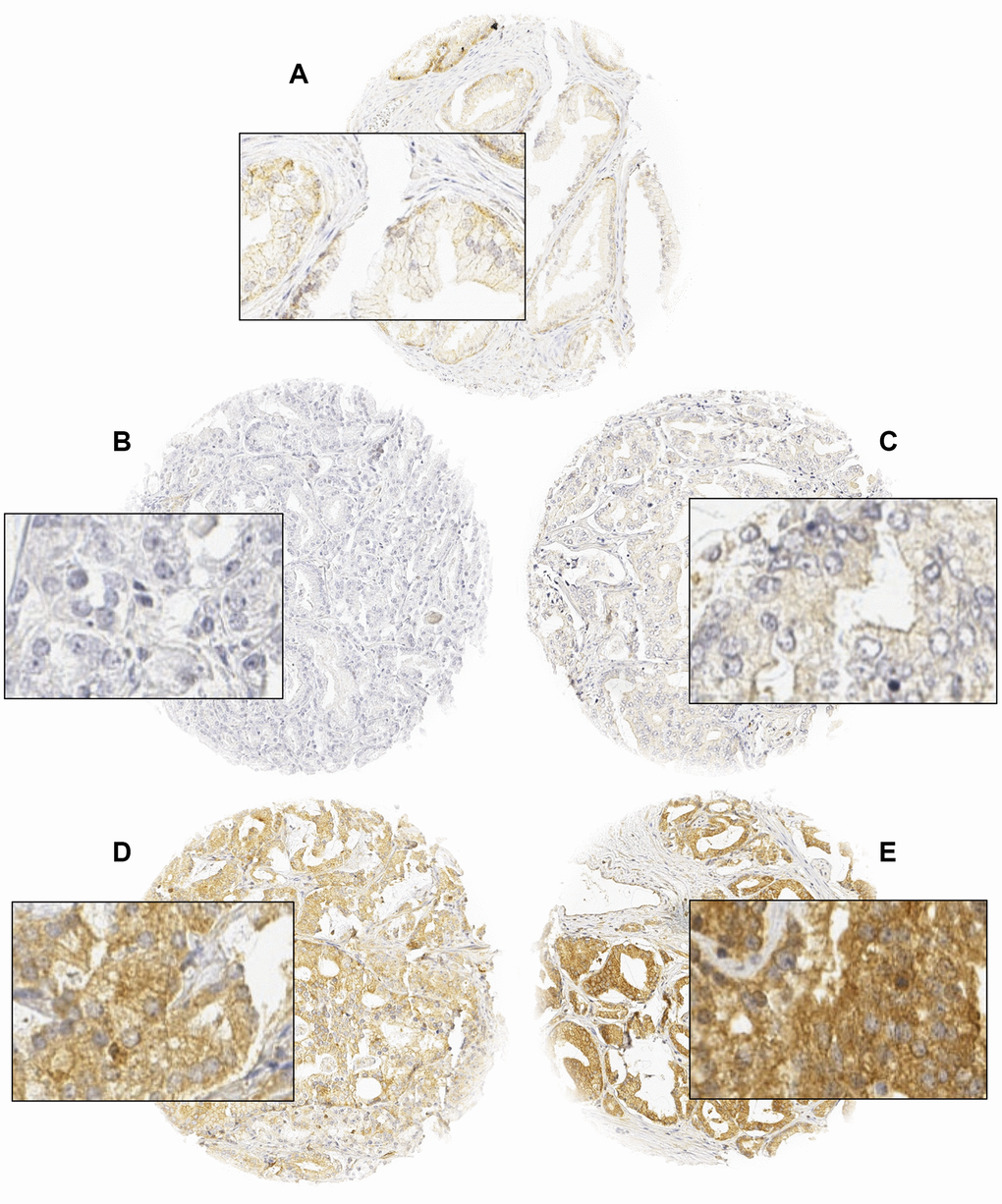
Figure 1. Representative images of normal (A) and cancerous glands (B–E) with negative (B), weak (C), moderate (D), and strong (E) ROCK1 staining. Spot size is 600 μm at 100 / 400x of originals.
TMPRSS2:ERG fusion status and ERG protein expression
Data on both ERG FISH and IHC were available from 5,976 cancers, and a concordant result (ERG IHC positive and break by FISH or ERG IHC negative and missing break by FISH) was found in more than 95% of the examined cancers. Increased ROCK1 expression was associated with TMPRSS2:ERG fusion positive prostate cancers (Supplementary Figure 1). For example, moderate to strong ROCK1 staining was seen in 63% of ERG IHC negative, but in 82% of ERG IHC positive cancers.
Tumor phenotype and PSA recurrence
Increased ROCK1 expression was significantly associated with advanced tumor stage, high classical and quantitative Gleason grade, positive nodal stage, positive surgical margin (p<0.0001 each), and high preoperative PSA level (p=0.0111; Table 1). For example, strong ROCK1 expression was found in 27.2% of pT3b-pT4 tumors and 30% of nodal-positive cancers, but only in 15% of pT2 cancers and 20% of nodal-negative cancers (p<0.0001 each). Most of these associations held also true in subset analyses of ERG negative or ERG positive cancers (Supplementary Table 1 and 2). Follow-up data were available for 9,590 patients with interpretable ROCK1 immunostaining. ROCK1 expression was associated with early PSA recurrence and (Figure 2A). This also hold true for the subsets of ERG-fusion negative and positive cancers (Figures 2B–2C) as well as in the subset of PTEN deleted (Figure 2D) and PTEN wild type cancers (p<0.0001, data not shown). To compare the prognostic impact of ROCK1 expression and the Gleason grade, further subset analyses were performed in cancers with identical classical and quantitative Gleason grade (Supplementary Figure 2). It showed that ROCK1 staining lacked significant prognostic impact in any group defined by classical or quantitative Gleason grade.
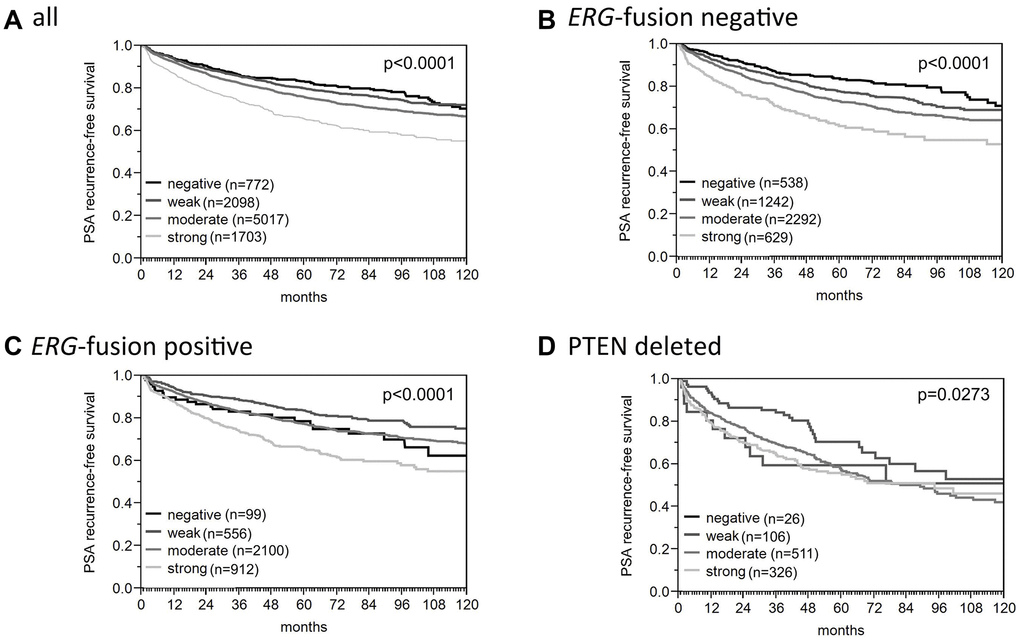
Figure 2. Association between ROCK1 expression and biochemical recurrence in (A) all cancers, (B) ERG-fusion negative cancers, (C) ERG-fusion positive cancers, (D) PTEN deleted cancers.
Association to patient age
ROCK1 upregulation was weakly linked to higher patient age when all tumors were jointly analyzed. The fraction of cancers with strong ROCK1 positivity increased from 13.4% in patients aged below 50 years to 20.5% in elderly patients (>70 years, p<0.0001). A subset analysis of revealed that this association was solely driven by cancers harboring TMPRSS2:ERG fusions (12.7% – 34.0%, p<0.0001) but was absent in fusion negative tumors (12.5% – 12.4%, p=0.4249). All data are summarized in Supplementary Table 3.
Multivariate analysis
Four different multivariate analyses were performed to evaluate the clinical relevance of ROCK1 expression in different scenarios (Supplementary Table 4). Scenario 1 evaluated all postoperatively available parameters including pT, pN, surgical margin status, preoperative PSA value and Gleason grade obtained on the prostatectomy specimen. In scenario 2, all postoperatively available parameters except pN were included. The rationale for this approach was that the indication and extent of lymph node dissection is not standardized in the surgical therapy of prostate cancer and may introduce a bias towards high-grade cancers. Two additional scenarios were to model the preoperative situation as much as possible. Scenario 3 included ROCK1 expression, preoperative PSA, clinical tumor stage (cT stage) and Gleason grade obtained on the prostatectomy specimen. Since postoperative determination of a tumor’s Gleason grade is “better” than the preoperatively determined Gleason grade (subjected to sampling errors and consequently under grading in more than one third of cases [17]) this parameter was replaced by the preoperative Gleason grade obtained on the original biopsy in Scenario 4. ROCK1 expression provided significant prognostic value beyond the established parameters in all of the described scenarios, particularly in the preclinical scenario 4. This also held true for the subgroups of ERG negative and ERG positive cancers. The cox proportional hazard ratio of PSA recurrence-free survival for patients with strong versus negative ROCK1 expression was in univariate analysis a moderate 2.04 (Supplementary Table 5).
Androgen receptor
To estimate the impact of AR on ROCK1 expression, we used AR expression data from a previous study [18], Data on both ROCK1 and AR were available from 6994 cancers. There was a strong positive association between AR expression and ROCK1 expression in all cancers as well as in subsets of ERG negative and ERG positive cancers (Figure 3).
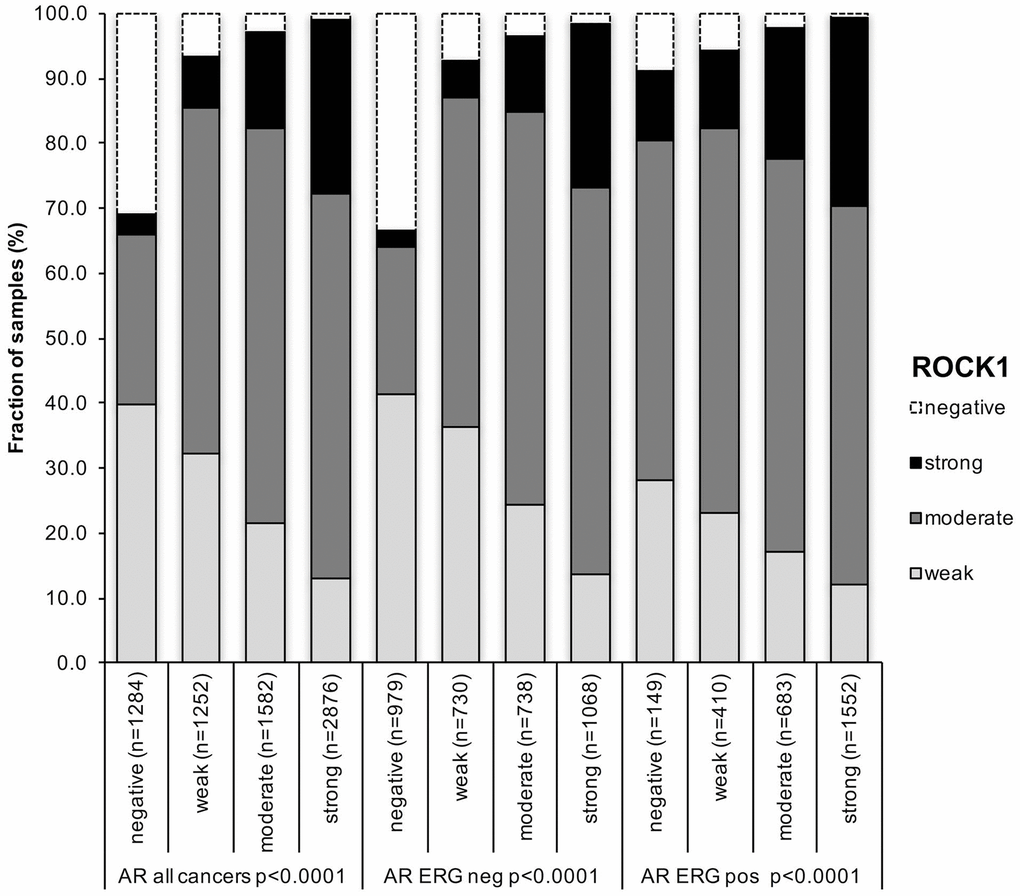
Figure 3. Association between positive ROCK1 staining and androgen-receptor (AR) status in all cancer, ERG fusion negative and ERG fusion positive cancers.
Association with cell proliferation
ROCK1 was significantly associated with increased cell proliferation as measured by Ki67-LI in all cancers (p<0.0001). The average Ki67-LI increased from 1.62±0.12 in cancers lacking ROCK1 expression to 2.28±0.07 (weak), 2.93±0.05 (moderate) and to 3.72±0.08 in cancers with strong ROCK1 expression (Table 2). This association held also true in tumor subsets with identical Gleason score.
Table 2. Association between ROCK1 expression and Ki67-labeling index in all cancers.
| Subset | ROCK1 | N | Ki67-LI* | P | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| All | Negative | 506 | 1.3±0.12 | p<0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weak | 1391 | 2.3±0.07 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate | 3279 | 2.9±0.05 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Strong | 1044 | 3.7±0.08 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gleason ≤3+4 | Negative | 448 | 1.2±0.11 | p<0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weak | 1167 | 2.1±0.07 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate | 2666 | 2.8±0.04 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Strong | 737 | 3.3±0.08 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gleason ≥4+3 | Negative | 55 | 1.9±0.50 | p<0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weak | 215 | 3.0±0.26 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate | 598 | 3.7±0.15 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Strong | 299 | 4.7±0.22 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PTEN normal | Negative | 165 | 1.8±0.21 | p<0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weak | 726 | 2.5±0.10 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate | 1808 | 3.1±0.06 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Strong | 540 | 3.8±0.12 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PTEN deletion | Negative | 17 | 3.1±0.70 | p=0.1086 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Weak | 78 | 3.1±0.33 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate | 376 | 3.6±0.15 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Strong | 214 | 3.9±0.20 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| * Mean ± standard error of the mean | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Chromosomal deletions
For PTEN, 6q15, 5q21 and 3p13, there was a tendency towards a higher level of ROCK1 immunostaining if deletions were present (Figure 4). This became particularly clear in ERG negative cancers (p<0.05 for all deletions; Figure 4B). In ERG positive cancers, this association reached statistical significance only for PTEN (p<0.0001; Figure 4C).
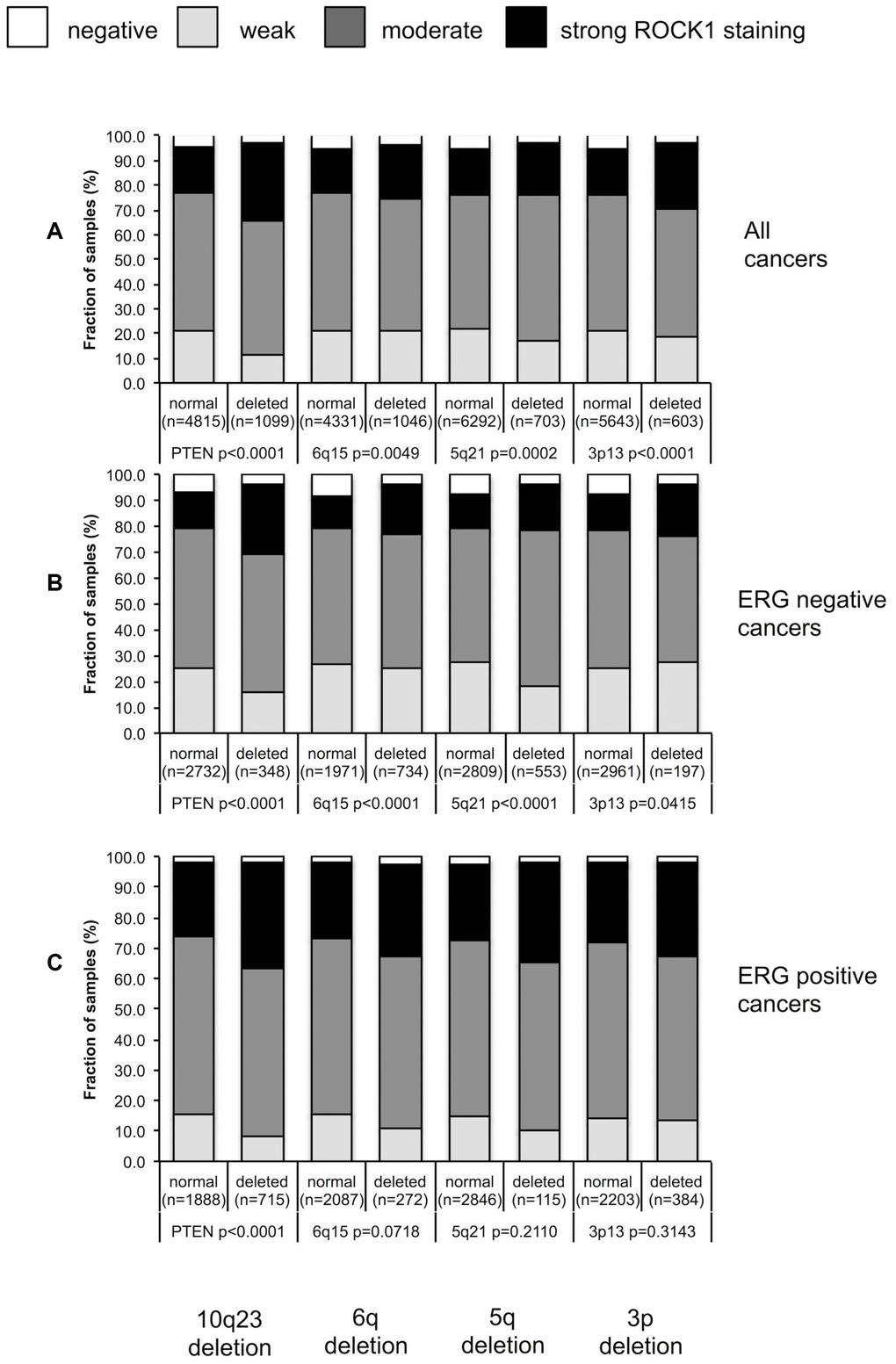
Figure 4. Association between ROCK1 staining and 10q23 (PTEN), 5q21 (CHD1), 6q15 (MAP3K7), 3p13 (FOXP1) deletions in (A) all cancers, (B) ERG negative cancers and (C) in ERG positive cancers.
Discussion
The results of this study demonstrate that overexpression of ROCK1 is associated with adverse tumor features and early biochemical recurrence in prostate cancer.
That ROCK1 staining was generally higher in cancers than in tumor adjacent normal prostatic tissue argues for a role of ROCK1 up regulation in prostate cancer development. Positive ROCK1 staining was seen in more than 90% of our 10,613 interpretable cancers, including 22% cancers with weak, 53% cancers with moderate and 18% with strong staining. Higher ROCK1 levels in cancer, than in normal epithelium was also described in an immunohistochemistry study by Kroiss et al. [16] reporting 100% positive staining in 56 cancers, including 14% cancers with low, 57% with moderate, and 29% with strong staining. The slightly higher fraction of cancers with strong staining in the study by Kroiss et al. is mostly likely due to the use of a different antibodies (Genetex GTX113266, rabbit polyclonal) and staining protocols.
The association with unfavorable tumor phenotype and poor clinical outcome in our patients argues for a role of ROCK1 overexpression in prostate cancer progression. While comparable immunohistochemistry data on the prognostic role of ROCK1 expression in prostate cancer are lacking, analysis of mRNA expression data from 85 prostate cancers from Taylor et al. [19] (raw data via GEO GSE21032) confirmed ROCK1 up-regulation in 21 recurrent (average mRNA expression level: 8.3) as compared to disease-free cancers (average 8.1, p=0.0263). A clinically relevant role of ROCK1 overexpression in prostate cancer is also consistent with reports from several other cancer types, where high ROCK1 expression was associated with tumor aggressiveness [8–10]. Schmidt et al. reported immunohistochemically detectable expression of ROCK’s upstream regulator RhoA to occur in >90% of prostate cancers and described a link between high level RhoA expression to large tumor size and poor prognosis [20]. Increased cancer aggressiveness in case of ROCK1 and/or RhoA overexpression fits very well with the known role of the Rho/Rock signaling pathway as a regulator of the actin cytoskeleton dynamics, and therefore, of various critical tumor-relevant processes such as cell motility, growth, dell division and cell survival. In vitro- and in vivo-studies with ROCK1 inhibitors suggest that ROCK1 activation increases motility, invasiveness and metastasis through accelerated actin filament remodeling and/or through indirect effects on the stiffness of the extracellular matrix, for example in mouse models of breast cancer bone metastasis [21], in ovarian cancer cells [22], and in lung cancer cells [23]. A role for tumor cell proliferation and angiogenesis is also assumed based on the anti-proliferative and anti-angiogenic effects of ROCK1 inhibition in lung cancer cells [24]. Moreover, ROCK1 has been shown to activate proliferation-promoting oncogenes such as c-myc by direct phosphorylation in breast cancer [21] and in prostate cancer [14]. An anti-apoptotic effect of ROCK1 has been reported in bladder cancer [25] and leukemia [26], and it was demonstrated that ROCK1 can disrupt the apoptotic-signaling cascade through inhibitory binding to Erk1/2 kinase [26].
The molecular database attached to our TMA allowed us to compare ROCK1 expression with other important molecular alterations occurring in prostate cancer. More than half of all prostate cancers, particularly those of young patients, harbor fusions connecting the androgen-regulated TMPRSS2 gene with the transcription factor ERG [18, 27]. These fusions result in an androgen-dependent overexpression of ERG [28] eventually leading to an altered expression of more than 1,600 genes in prostate epithelial cells [29]. The significant up-regulation of ROCK1 in cancers harboring the TMPRSS2:ERG fusion fits with an earlier report describing increased expression of ROCK’s upstream regulator Rho guanine diphosphate dissociation inhibitor beta (ARHGDIB) in ERG positive prostate cancers [30]. Of note, ARHGDIB up-regulation has also been reported from breast cancers [31] where it promotes invasiveness [32]. Interestingly, we found that ROCK1 up-regulation was linked to higher patient age exclusively in cancers harboring the ERG fusion, suggesting that the consequences of ERG fusion may vary with age. The positive association between AR and ROCK1 expression further supports recent work suggesting a regulatory loop involving both proteins. Two studies demonstrate that Rho/ROCK signaling activity is increased in response to androgen stimulation [20], while the androgen-regulated micro-RNA-135a controls ROCK1 expression [16].
Genomic deletions at various chromosomal loci represent the second most frequent type of genetic alterations next to TMPRSS2:ERG fusions. The significant association between high ROCK1 expression and several important deletions fits with earlier studies showing that perturbations in the actin filament homeostasis, which can occur as a consequence of ROCK1 deregulation [33], promote the development of general genetic instability including double strand breakage and deletions. In human pluripotent stem cells, which often acquire chromosomal aberrations in culture, replicative stress, defective chromosome condensation and aneuploidy had been associated with altered levels of actin cytoskeletal genes [34]. Those associations between ROCK1 and most deletions were less common in ERG positive than in ERG negative cancers may be due to the different microenvironment in ERG positive cells. Alternatively, this may be due to experimental issues caused by the general ROCK1 up-regulation in ERG positive cancers. In cancers with a higher average expression, the distinction of subtle expression differences may become more difficult in bright field immunohistochemistry. The particularly strong association between ROCK1 expression and PTEN deletions is likely to be due to the known PTEN/ROCK1 interaction. ROCK1 has been shown to modify PTEN activity in several studies, although with conflicting results describing either activation [4] or down-regulation of PTEN [35]. The data of this study suggest that ROCK1 expression may represent a potentially clinically useful prognostic marker in prostate cancer. Of note, the independent prognostic role of ROCK1 expression was even retained if the strongest established prognostic parameters were included, such as pT and pN stage, which are not available at the moment when therapeutic decisions are taken. Moreover, ROCK1 expression had a prognostic impact in all analyzed molecularly defined subgroups. This included cancers harboring deletions of the PTEN tumor suppressor, which belongs to the strongest molecular prognostic markers identified in prostate cancer as to yet [36]. That ROCK1 expression lacked prognostic impact in cancers defined by a comparable classical or quantitative Gleason grade demonstrates how difficult it is for a molecular marker to compete with classical histomorphological features. The potential for ROCK1 expression analysis is not compromised by the fact that ROCK1 expression analysis was not better than Gleason grading. Although Gleason grading is a very powerful statistical parameter, it suffers from notorious interobserver heterogeneity, which is in the range of 40% [37]. Accordingly, there is not only a need for better predictors of prostate cancer aggressiveness but also for more reproducible ones. Molecular analysis including one or more molecular parameters may, thus, help to improve standardization of prognosis assessment in the future.
Several drugs targeting ROCK1 are available. Y27632 [38] and Fasudil [39] are selective ROCK inhibitors, which target the ATP-dependent kinase domain of both isoforms ROCK1 and ROCK2. Fasudil is in clinical use in China and Japan in the treatment of cerebral vasospasm [40], pulmonary hypertension [41] and neurodegenerative memory loss [42]. Several studies suggest that it might be also useful for treating cancers [24, 43, 44]. Most recently, two studies found that Fasudil inhibits migration of breast, fibrosarcoma and laryngeal cancer cells [45, 46]. AT13148, a multi-AGC kinase inhibitor targeting ROCK and also various other serin/threonine protein kinases demonstrated potent cytotoxic and anti-proliferative activities in cell lines of human melanomas, gliomas, and various other cancers [47, 48]. AT13148 showed significant antitumor actions also in mouse models of human xenograft pancreatic cancers, where the compound reduced subcutaneous tumor growth and blocked invasion of healthy pancreatic tissue [49]. These promising results lead to the recruitment of patients with advanced solid cancers who are refractory to conventional therapy for a phase I clinical study (NCT01585701). The data from our study suggest a high importance of ROCK1 for prostate cancer biology. This may encourage future work on the effect of ROCK inhibitors in prostate cancer.
Conclusions
In summary, the results of our study demonstrate that up-regulation of ROCK1 is common in prostate cancer and is associated with tumor aggressiveness and poor prognosis. Anti-cancer drugs specifically targeting ROCK1 may thus be particularly efficient in prostate cancer. Moreover, ROCK1 measurement, either alone or in combination might be of clinical utility in prostate cancer.
Materials and Methods
Patients
Radical prostatectomy specimens were from patients, who had been operated between 1992 and 2012 at the Department of Urology and the Martini Clinics at the University Medical Center Hamburg-Eppendorf (Supplementary Table 6). Follow-up was available for a total of 11 613 patients (median 49 months; range: 1 to 276 months). PSA levels were measured following surgery and PSA recurrence was defined as the time point when postoperative PSA was at least 0.2 ng/ml and increasing at subsequent measurements. In addition to the classical Gleason categories, “quantitative” Gleason grading was performed as described before [50]. In brief, for every prostatectomy specimen, the percentages of Gleason 4 patterns in cancerous tissues were estimated during the regular process of pathologic interpretation. The TMA was produced with one 0.6mm core taken from a cancer containing tissue block from each patient. Each TMA block also contained various control tissues, including normal prostate tissue. The TMA is annotated with results on ERG expression, ERG break apart FISH analysis [51] and deletion status of 5q21 (CHD1) [52], 6q15 (MAP3K7) [53], PTEN (10q23) [54], 3p13 (FOXP1) [55], Ki67 labeling index (Ki67-LI) data), and androgen receptor (AR) expression [56]. The usage of archived diagnostic leftover tissues for manufacturing of tissue microarrays and their analysis for research purposes as well as patient data analysis has been approved by local laws (HmbKHG, §12a) and by the local ethics committee (Ethics commission Hamburg, WF-049/09). All work has been carried out in compliance with the Helsinki Declaration.
Immunohistochemistry
Freshly cut TMA sections were stained in one day and in one experiment. Slides were deparaffinized and exposed to heat-induced antigen retrieval for 5 minutes at 121°C in pH 7,8 Tris-EDTA-citrate buffer. Anti- ROCK1 immunohistochemical staining was performed with the rabbit monoclonal antibody clone EP786Y (Abcam ab45171, Cambridge, UK, 1:4050) for 60 min at 37°C. To confirm specificity of clone EP786Y, we partly repeated the staining using a more recent ROCK1 antidody that had been validated in ROCK1 knock-out cell lines (Abcam ab134181, clone EPR683Y). The identical staining pattern that was observed with both antibodies is compatible with specificity for the ROCK1 protein (Supplementary figure 3). ROCK1 staining was typically cytoplasmic and slightly nuclear. As no significant heterogeneity in ROCK1 staining was seen in TMA spots, the precentage of positive cells was not considered. Instead, the overall staining intensity (0, 1+, 2+, and 3+) of cancer cells was recorded for each tissue spot. Only one trained person analyzed all tissue spots manually. We do not regard this as a limitation of our study. We have earlier demonstrated that manual and automated image analysis of large scale TMAs yield comparable results [57] and that possible misdiagnosis of individual tissue spots (e.g. false classification of tumor and normal tissue) does not significantly impact the overall study outcome [58].
Statistics
Contingency tables and the chi²-test were performed to search for associations between molecular parameters and tumor phenotype. Kaplan-Meier curves were tested by the log-rank test to detect significant differences between groups. Cox proportional hazards regression analysis was applied to test the statistical independence and significance between pathological, molecular and clinical variables. All calculations were done with JMP 12 (SAS Institute Inc., NC, USA).
Author Contributions
SS, AH, BH, FB, DH, MCT, SM, TSC; AML participated in the study conception, design, case selection and experiments. EB, CF, SW, HH, AH,MG and TS carried out the data collection. RS, GS; AH, performed the experiment of this study. JRI and RS, GS, CHM performed the data analysis and writing of the manuscript. All the authors read and approved the final manuscript.
Acknowledgments
We thank Christina Möller-Koop, Sünje Seekamp and Inge Brandt for excellent technical assistance.
Conflicts of Interest
There are no conflicts of interest to declare.
Funding
The German Federal Ministry of Education and Research (BMBF), project ICGC_II FKZ 101KU1505B to GS, supported this work.
References
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 2. Wilt TJ, Brawer MK, Jones KM, Barry MJ, Aronson WJ, Fox S, Gingrich JR, Wei JT, Gilhooly P, Grob BM, Nsouli I, Iyer P, Cartagena R, et al, and Prostate Cancer Intervention versus Observation Trial (PIVOT) Study Group. Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med. 2012; 367:203–13. https://doi.org/10.1056/NEJMoa1113162 [PubMed]
- 3. Pearce LR, Komander D, Alessi DR. The nuts and bolts of AGC protein kinases. Nat Rev Mol Cell Biol. 2010; 11:9–22. https://doi.org/10.1038/nrm2822 [PubMed]
- 4. Li Z, Dong X, Wang Z, Liu W, Deng N, Ding Y, Tang L, Hla T, Zeng R, Li L, Wu D. Regulation of PTEN by Rho small GTPases. Nat Cell Biol. 2005; 7:399–404. https://doi.org/10.1038/ncb1236 [PubMed]
- 5. Yasui Y, Amano M, Nagata K, Inagaki N, Nakamura H, Saya H, Kaibuchi K, Inagaki M. Roles of Rho-associated kinase in cytokinesis; mutations in Rho-associated kinase phosphorylation sites impair cytokinetic segregation of glial filaments. J Cell Biol. 1998; 143:1249–58. https://doi.org/10.1083/jcb.143.5.1249 [PubMed]
- 6. Riento K, Ridley AJ. Rocks: multifunctional kinases in cell behaviour. Nat Rev Mol Cell Biol. 2003; 4:446–56. https://doi.org/10.1038/nrm1128 [PubMed]
- 7. Nakagawa O, Fujisawa K, Ishizaki T, Saito Y, Nakao K, Narumiya S. ROCK-I and ROCK-II, two isoforms of Rho-associated coiled-coil forming protein serine/threonine kinase in mice. FEBS Lett. 1996; 392:189–93. https://doi.org/10.1016/0014-5793(96)00811-3 [PubMed]
- 8. Bottino J, Gelaleti GB, Maschio LB, Jardim-Perassi BV, de Campos Zuccari DA. Immunoexpression of ROCK-1 and MMP-9 as prognostic markers in breast cancer. Acta Histochem. 2014; 116:1367–73. https://doi.org/10.1016/j.acthis.2014.08.009 [PubMed]
- 9. Li J, Bharadwaj SS, Guzman G, Vishnubhotla R, Glover SC. ROCK I Has More Accurate Prognostic Value than MET in Predicting Patient Survival in Colorectal Cancer. Anticancer Res. 2015; 35:3267–73. [PubMed]
- 10. Wu YJ, Tang Y, Li ZF, Li Z, Zhao Y, Wu ZJ, Su Q. Expression and significance of Rac1, Pak1 and Rock1 in gastric carcinoma. Asia Pac J Clin Oncol. 2014; 10:e33–39. https://doi.org/10.1111/ajco.12052 [PubMed]
- 11. Cai H, Lin L, Cai H, Tang M, Wang Z. Combined microRNA-340 and ROCK1 mRNA profiling predicts tumor progression and prognosis in pediatric osteosarcoma. Int J Mol Sci. 2014; 15:560–73. https://doi.org/10.3390/ijms15010560 [PubMed]
- 12. Wen S, Shang Z, Zhu S, Chang C, Niu Y. Androgen receptor enhances entosis, a non-apoptotic cell death, through modulation of Rho/ROCK pathway in prostate cancer cells. Prostate. 2013; 73:1306–15. https://doi.org/10.1002/pros.22676 [PubMed]
- 13. Xu B, Huang Y, Niu X, Tao T, Jiang L, Tong N, Chen S, Liu N, Zhu W, Chen M. Hsa-miR-146a-5p modulates androgen-independent prostate cancer cells apoptosis by targeting ROCK1. Prostate. 2015; 75:1896–903. https://doi.org/10.1002/pros.23068 [PubMed]
- 14. Zhang C, Zhang S, Zhang Z, He J, Xu Y, Liu S. ROCK has a crucial role in regulating prostate tumor growth through interaction with c-Myc. Oncogene. 2014; 33:5582–91. https://doi.org/10.1038/onc.2013.505 [PubMed]
- 15. Liu K, Li X, Wang J, Wang Y, Dong H, Li J. Genetic variants in RhoA and ROCK1 genes are associated with the development, progression and prognosis of prostate cancer. Oncotarget. 2017; 8:19298–309. https://doi.org/10.18632/oncotarget.15197 [PubMed]
- 16. Kroiss A, Vincent S, Decaussin-Petrucci M, Meugnier E, Viallet J, Ruffion A, Chalmel F, Samarut J, Allioli N. Androgen-regulated microRNA-135a decreases prostate cancer cell migration and invasion through downregulating ROCK1 and ROCK2. Oncogene. 2015; 34:2846–55. https://doi.org/10.1038/onc.2014.222 [PubMed]
- 17. Epstein JI, Feng Z, Trock BJ, Pierorazio PM. Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur Urol. 2012; 61:1019–24. https://doi.org/10.1016/j.eururo.2012.01.050 [PubMed]
- 18. Weischenfeldt J, Simon R, Feuerbach L, Schlangen K, Weichenhan D, Minner S, Wuttig D, Warnatz HJ, Stehr H, Rausch T, Jäger N, Gu L, Bogatyrova O, et al. Integrative genomic analyses reveal an androgen-driven somatic alteration landscape in early-onset prostate cancer. Cancer Cell. 2013; 23:159–70. https://doi.org/10.1016/j.ccr.2013.01.002 [PubMed]
- 19. Taylor BS, Schultz N, Hieronymus H, Gopalan A, Xiao Y, Carver BS, Arora VK, Kaushik P, Cerami E, Reva B, Antipin Y, Mitsiades N, Landers T, et al. Integrative genomic profiling of human prostate cancer. Cancer Cell. 2010; 18:11–22. https://doi.org/10.1016/j.ccr.2010.05.026 [PubMed]
- 20. Schmidt LJ, Duncan K, Yadav N, Regan KM, Verone AR, Lohse CM, Pop EA, Attwood K, Wilding G, Mohler JL, Sebo TJ, Tindall DJ, Heemers HV. RhoA as a mediator of clinically relevant androgen action in prostate cancer cells. Mol Endocrinol. 2012; 26:716–35. https://doi.org/10.1210/me.2011-1130 [PubMed]
- 21. Liu S, Goldstein RH, Scepansky EM, Rosenblatt M. Inhibition of rho-associated kinase signaling prevents breast cancer metastasis to human bone. Cancer Res. 2009; 69:8742–51. https://doi.org/10.1158/0008-5472.CAN-09-1541 [PubMed]
- 22. Ogata S, Morishige K, Sawada K, Hashimoto K, Mabuchi S, Kawase C, Ooyagi C, Sakata M, Kimura T. Fasudil inhibits lysophosphatidic acid-induced invasiveness of human ovarian cancer cells. Int J Gynecol Cancer. 2009; 19:1473–80. https://doi.org/10.1111/IGC.0b013e3181c03909 [PubMed]
- 23. Zhu F, Zhang Z, Wu G, Li Z, Zhang R, Ren J, Nong L. Rho kinase inhibitor fasudil suppresses migration and invasion though down-regulating the expression of VEGF in lung cancer cell line A549. Med Oncol. 2011; 28:565–71. https://doi.org/10.1007/s12032-010-9468-5 [PubMed]
- 24. Yang X, Zhang Y, Wang S, Shi W. Effect of fasudil on growth, adhesion, invasion, and migration of 95D lung carcinoma cells in vitro. Can J Physiol Pharmacol. 2010; 88:874–79. https://doi.org/10.1139/Y10-047 [PubMed]
- 25. Abe H, Kamai T, Hayashi K, Anzai N, Shirataki H, Mizuno T, Yamaguchi Y, Masuda A, Yuki H, Betsunoh H, Yashi M, Fukabori Y, Yoshida K. The Rho-kinase inhibitor HA-1077 suppresses proliferation/migration and induces apoptosis of urothelial cancer cells. BMC Cancer. 2014; 14:412. https://doi.org/10.1186/1471-2407-14-412 [PubMed]
- 26. Li F, Jiang Q, Shi KJ, Luo H, Yang Y, Xu CM. RhoA modulates functional and physical interaction between ROCK1 and Erk1/2 in selenite-induced apoptosis of leukaemia cells. Cell Death Dis. 2013; 4:e708. https://doi.org/10.1038/cddis.2013.243 [PubMed]
- 27. Tomlins SA, Rhodes DR, Perner S, Dhanasekaran SM, Mehra R, Sun XW, Varambally S, Cao X, Tchinda J, Kuefer R, Lee C, Montie JE, Shah RB, et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science. 2005; 310:644–48. https://doi.org/10.1126/science.1117679 [PubMed]
- 28. Clark JP, Cooper CS. ETS gene fusions in prostate cancer. Nat Rev Urol. 2009; 6:429–39. https://doi.org/10.1038/nrurol.2009.127 [PubMed]
- 29. Brase JC, Johannes M, Mannsperger H, Fälth M, Metzger J, Kacprzyk LA, Andrasiuk T, Gade S, Meister M, Sirma H, Sauter G, Simon R, Schlomm T, et al. TMPRSS2-ERG -specific transcriptional modulation is associated with prostate cancer biomarkers and TGF-β signaling. BMC Cancer. 2011; 11:507. https://doi.org/10.1186/1471-2407-11-507 [PubMed]
- 30. Barwick BG, Abramovitz M, Kodani M, Moreno CS, Nam R, Tang W, Bouzyk M, Seth A, Leyland-Jones B. Prostate cancer genes associated with TMPRSS2-ERG gene fusion and prognostic of biochemical recurrence in multiple cohorts. Br J Cancer. 2010; 102:570–76. https://doi.org/10.1038/sj.bjc.6605519 [PubMed]
- 31. Moon HG, Jeong SH, Ju YT, Jeong CY, Lee JS, Lee YJ, Hong SC, Choi SK, Ha WS, Park ST, Jung EJ. Up-regulation of RhoGDI2 in human breast cancer and its prognostic implications. Cancer Res Treat. 2010; 42:151–56. https://doi.org/10.4143/crt.2010.42.3.151 [PubMed]
- 32. Zhang Y, Zhang B. D4-GDI, a Rho GTPase regulator, promotes breast cancer cell invasiveness. Cancer Res. 2006; 66:5592–98. https://doi.org/10.1158/0008-5472.CAN-05-4004 [PubMed]
- 33. Shi J, Wu X, Surma M, Vemula S, Zhang L, Yang Y, Kapur R, Wei L. Distinct roles for ROCK1 and ROCK2 in the regulation of cell detachment. Cell Death Dis. 2013; 4:e483. https://doi.org/10.1038/cddis.2013.10 [PubMed]
- 34. Lamm N, Ben-David U, Golan-Lev T, Storchová Z, Benvenisty N, Kerem B. Genomic Instability in Human Pluripotent Stem Cells Arises from Replicative Stress and Chromosome Condensation Defects. Cell Stem Cell. 2016; 18:253–61. https://doi.org/10.1016/j.stem.2015.11.003 [PubMed]
- 35. Yang S, Kim HM. The RhoA-ROCK-PTEN pathway as a molecular switch for anchorage dependent cell behavior. Biomaterials. 2012; 33:2902–15. https://doi.org/10.1016/j.biomaterials.2011.12.051 [PubMed]
- 36. Mithal P, Allott E, Gerber L, Reid J, Welbourn W, Tikishvili E, Park J, Younus A, Sangale Z, Lanchbury JS, Stone S, Freedland SJ. PTEN loss in biopsy tissue predicts poor clinical outcomes in prostate cancer. Int J Urol. 2014; 21:1209–14. https://doi.org/10.1111/iju.12571 [PubMed]
- 37. Singh RV, Agashe SR, Gosavi AV, Sulhyan KR. Interobserver reproducibility of Gleason grading of prostatic adenocarcinoma among general pathologists. Indian J Cancer. 2011; 48:488–95. https://doi.org/10.4103/0019-509X.92277 [PubMed]
- 38. Uehata M, Ishizaki T, Satoh H, Ono T, Kawahara T, Morishita T, Tamakawa H, Yamagami K, Inui J, Maekawa M, Narumiya S. Calcium sensitization of smooth muscle mediated by a Rho-associated protein kinase in hypertension. Nature. 1997; 389:990–94. https://doi.org/10.1038/40187 [PubMed]
- 39. Asano T, Ikegaki I, Satoh S, Suzuki Y, Shibuya M, Takayasu M, Hidaka H. Mechanism of action of a novel antivasospasm drug, HA1077. J Pharmacol Exp Ther. 1987; 241:1033–40. [PubMed]
- 40. Suzuki Y, Shibuya M, Satoh S, Sugiyama H, Seto M, Takakura K. Safety and efficacy of fasudil monotherapy and fasudil-ozagrel combination therapy in patients with subarachnoid hemorrhage: sub-analysis of the post-marketing surveillance study. Neurol Med Chir (Tokyo). 2008; 48:241–47. https://doi.org/10.2176/nmc.48.241 [PubMed]
- 41. Doggrell SA. Rho-kinase inhibitors show promise in pulmonary hypertension. Expert Opin Investig Drugs. 2005; 14:1157–59. https://doi.org/10.1517/13543784.14.9.1157 [PubMed]
- 42. Huentelman MJ, Stephan DA, Talboom J, Corneveaux JJ, Reiman DM, Gerber JD, Barnes CA, Alexander GE, Reiman EM, Bimonte-Nelson HA. Peripheral delivery of a ROCK inhibitor improves learning and working memory. Behav Neurosci. 2009; 123:218–23. https://doi.org/10.1037/a0014260 [PubMed]
- 43. Ying H, Biroc SL, Li WW, Alicke B, Xuan JA, Pagila R, Ohashi Y, Okada T, Kamata Y, Dinter H. The Rho kinase inhibitor fasudil inhibits tumor progression in human and rat tumor models. Mol Cancer Ther. 2006; 5:2158–64. https://doi.org/10.1158/1535-7163.MCT-05-0440 [PubMed]
- 44. Deng L, Li G, Li R, Liu Q, He Q, Zhang J. Rho-kinase inhibitor, fasudil, suppresses glioblastoma cell line progression in vitro and in vivo. Cancer Biol Ther. 2010; 9:875–84. https://doi.org/10.4161/cbt.9.11.11634 [PubMed]
- 45. Guerra FS, Oliveira RG, Fraga CA, Mermelstein CD, Fernandes PD. ROCK inhibition with Fasudil induces beta-catenin nuclear translocation and inhibits cell migration of MDA-MB 231 human breast cancer cells. Sci Rep. 2017; 7:13723. https://doi.org/10.1038/s41598-017-14216-z [PubMed]
- 46. Zhang X, Wu N. Fasudil inhibits proliferation and migration of Hep-2 laryngeal carcinoma cells. Drug Des Devel Ther. 2018; 12:373–81. https://doi.org/10.2147/DDDT.S147547 [PubMed]
- 47. Yap TA, Walton MI, Grimshaw KM, Te Poele RH, Eve PD, Valenti MR, de Haven Brandon AK, Martins V, Zetterlund A, Heaton SP, Heinzmann K, Jones PS, Feltell RE, et al. AT13148 is a novel, oral multi-AGC kinase inhibitor with potent pharmacodynamic and antitumor activity. Clin Cancer Res. 2012; 18:3912–23. https://doi.org/10.1158/1078-0432.CCR-11-3313 [PubMed]
- 48. Xi Y, Niu J, Shen Y, Li D, Peng X, Wu X. AT13148, a first-in-class multi-AGC kinase inhibitor, potently inhibits gastric cancer cells both in vitro and in vivo. Biochem Biophys Res Commun. 2016; 478:330–36. https://doi.org/10.1016/j.bbrc.2016.01.167 [PubMed]
- 49. Rath N, Munro J, Cutiongco MF, Jagiełło A, Gadegaard N, McGarry L, Unbekandt M, Michalopoulou E, Kamphorst JJ, Sumpton D, Mackay G, Vennin C, Pajic M, et al. Rho Kinase Inhibition by AT13148 Blocks Pancreatic Ductal Adenocarcinoma Invasion and Tumor Growth. Cancer Res. 2018; 78:3321–36. https://doi.org/10.1158/0008-5472.can-17-1339 [PubMed]
- 50. Sauter G, Steurer S, Clauditz TS, Krech T, Wittmer C, Lutz F, Lennartz M, Janssen T, Hakimi N, Simon R, von Petersdorff-Campen M, Jacobsen F, von Loga K, et al. Clinical Utility of Quantitative Gleason Grading in Prostate Biopsies and Prostatectomy Specimens. Eur Urol. 2016; 69:592–98. https://doi.org/10.1016/j.eururo.2015.10.029 [PubMed]
- 51. Minner S, Enodien M, Sirma H, Luebke AM, Krohn A, Mayer PS, Simon R, Tennstedt P, Müller J, Scholz L, Brase JC, Liu AY, Schlüter H, et al. ERG status is unrelated to PSA recurrence in radically operated prostate cancer in the absence of antihormonal therapy. Clin Cancer Res. 2011; 17:5878–88. https://doi.org/10.1158/1078-0432.CCR-11-1251 [PubMed]
- 52. Burkhardt L, Fuchs S, Krohn A, Masser S, Mader M, Kluth M, Bachmann F, Huland H, Steuber T, Graefen M, Schlomm T, Minner S, Sauter G, et al. CHD1 is a 5q21 tumor suppressor required for ERG rearrangement in prostate cancer. Cancer Res. 2013; 73:2795–805. https://doi.org/10.1158/0008-5472.CAN-12-1342 [PubMed]
- 53. Kluth M, Hesse J, Heinl A, Krohn A, Steurer S, Sirma H, Simon R, Mayer PS, Schumacher U, Grupp K, Izbicki JR, Pantel K, Dikomey E, et al. Genomic deletion of MAP3K7 at 6q12-22 is associated with early PSA recurrence in prostate cancer and absence of TMPRSS2:ERG fusions. Mod Pathol. 2013; 26:975–83. https://doi.org/10.1038/modpathol.2012.236 [PubMed]
- 54. Krohn A, Diedler T, Burkhardt L, Mayer PS, De Silva C, Meyer-Kornblum M, Kötschau D, Tennstedt P, Huang J, Gerhäuser C, Mader M, Kurtz S, Sirma H, et al. Genomic deletion of PTEN is associated with tumor progression and early PSA recurrence in ERG fusion-positive and fusion-negative prostate cancer. Am J Pathol. 2012; 181:401–12. https://doi.org/10.1016/j.ajpath.2012.04.026 [PubMed]
- 55. Krohn A, Seidel A, Burkhardt L, Bachmann F, Mader M, Grupp K, Eichenauer T, Becker A, Adam M, Graefen M, Huland H, Kurtz S, Steurer S, et al. Recurrent deletion of 3p13 targets multiple tumour suppressor genes and defines a distinct subgroup of aggressive ERG fusion-positive prostate cancers. J Pathol. 2013; 231:130–41. https://doi.org/10.1002/path.4223 [PubMed]
- 56. Minner S, Jessen B, Stiedenroth L, Burandt E, Köllermann J, Mirlacher M, Erbersdobler A, Eichelberg C, Fisch M, Brümmendorf TH, Bokemeyer C, Simon R, Steuber T, et al. Low level HER2 overexpression is associated with rapid tumor cell proliferation and poor prognosis in prostate cancer. Clin Cancer Res. 2010; 16:1553–60. https://doi.org/10.1158/1078-0432.CCR-09-2546 [PubMed]
- 57. Simon R, Mirlacher M, Sauter G. Tissue microarrays. Biotechniques. 2004; 36:98–105. https://doi.org/10.2144/04361RV01 [PubMed]
- 58. Tennstedt P, Sauter G. Quality aspects of TMA analysis. Methods Mol Biol. 2010; 664:17–26. https://doi.org/10.1007/978-1-60761-806-5_2 [PubMed]