



Introduction
An outbreak of new pneumonia caused by the 2019 novel coronavirus (2019-nCoV) started in Wuhan, China, in December 2019 [1]. In January 2020, Chinese scientists isolated this 2019-nCoV from patients with viral pneumonia, officially naming it as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [2]. Since then, the disease has rapidly spread from Wuhan to other regions. In February 2020, the World Health Organization (WHO) named the disease caused by this virus as coronavirus disease 2019 (COVID-19). At the time of this article's submission, some cases have been reported internationally across the six continents.
The COVID-19 pandemic has caused severe illness in infected patients, such as pneumonia and acute respiratory distress syndrome, which even resulted in death. According to the COVID-19 joint study report released by the National Health Commission of the People’s Republic of China, about 80% of patients have light and common infection, whereas 13.8% have severe/critical infections, making them highly at risk for mortality [3]. In addition, prevention and control of severe and critically ill patients are yet to be implemented [3]. Thus, clinicians and radiologists should identify the characteristic imaging manifestations in chest CT findings of critically ill individuals, so that they can perform specific symptomatic treatment at the earliest, prevent complications, and provide organ functional support. Compared to other methods, computed tomography (CT) is the best technique for the early detection of pneumonia. Only a few reports demonstrated the clinical imaging features of severe and critically ill patients during the epidemic in Heilongjiang Province. This study describes the clinical and radiological characteristics and laboratory examination data of 59 patients with COVID-19 and compares between those admitted in the intensive care unit (ICU) and non-ICU departments. Thus, we hope that these current results could be used by clinicians in Heilongjiang Province and worldwide for the treatment plan of COVID-19.
Results
A total of 59 patients confirmed with COVID-19 in Heilongjiang Province were included in this study. The general clinical data of patients are shown in Table 1. The median age was 64.0 (IQR, 56–72) years. The most common complication in the patient group was cardiovascular disease (44%), followed hypertension (42%) and diabetes (15%), and the rarest complication was chronic obstructive disease (3%), followed by malignancy (2%) and chronic liver disease (2%). Compared to non-ICU patients, ICU patients were older (median age: 67 vs. 56); P = 0.037) and more likely at risk for cardiovascular diseases (52% vs. 20%; P = 0.030). The most common clinical symptoms in this study were fever (41/59, 69%), cough (30/59, 51%), and muscle soreness (15/59, 25%), whereas the less common were dyspnea (14/59, 24%), headache (8/59, 13%), abdominal pain, diarrhea (5/59, 8%), and nausea (3/59, 5%). However, compared to non-ICU patients, the incidence of muscle soreness in the ICU patients was reduced (18% vs. 47%; P = 0.042).
Table 1. Demographics and baseline characteristics of two groups of patients infected with 2019-nCoV.
| All patients (n=59) | ICU care (n=44) | No ICU care (n=15) | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Characteristics | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (y) | 64.0(56.0-72.0) | 66.5(57.3-75.8) | 56.0(50.0-68.0) | 0.037 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender | 0.552 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 29(49%) | 23(52%) | 6(40%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 30(51%) | 21(48%) | 9(60%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exposure history | 0.516 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Contact with infected patients | 42(71%) | 30(68%) | 12(80%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown history | 17 (29%) | 14(32%) | 3(20%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any comorbidity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | 9(15%) | 6(14%) | 3(20%) | 0.680 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 25(42%) | 20(45%) | 5(33%) | 0.412 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardiovascular disease | 26(44%) | 23(52%) | 3(20%) | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| COPD | 2(3%) | 1(2%) | 1(7%) | 0.447 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Malignancy | 1(2%) | 1(2%) | 0(0%) | -- | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chronic liver disease | 1(2%) | 0(0%) | 1(7%) | -- | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Signs and symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fever | 41(69%) | 31(70%) | 10(67%) | 0.785 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Highest temperature, °C | 0.412 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <37.3 | 18(31%) | 14(32%) | 4(27%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 37.3–38.0 | 25(42%) | 16(36%) | 9(60%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 38.1–39.0 | 15(25%) | 13(30%) | 2(13%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >39.0 | 1(2%) | 1(2%) | 0(0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cough | 30(51%) | 20(45%) | 10(67%) | 0.205 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Myalgia or fatigue | 15(25%) | 8(18%) | 7(47%) | 0.042 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Headache | 8 14%) | 4(9%) | 4(27%) | 0.184 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diarrhoea, bellyache | 5(8%) | 4(9%) | 1(7%) | 0.624 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyspnoea | 14(24%) | 9(20%) | 5(33%) | 0.316 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nausea | 3(5%) | 1(2%) | 2(13%) | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data are median (IQR), n (%), or n/N (%), where N is the total number of patients with available data. P values comparing Group1 and Group2 are from χ² test, Fisher’s exact test, or Mann-Whitney U test. 2019-nCoV=2019 novel coronavirus. COPD=Chronic obstructive pulmonary disease. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Laboratory examination results of 59 patients are summarized in Table 2. White blood cell count (<4 × 109/L; 11/59, 19%) and lymphocyte count (<1.0 ×109/L; 26/59, 44%) were low in some patients. Compared to non-ICU patients, ICU patients are more likely to have lymphopenia (52% vs. 20%; P = 0.003), with higher neutrophil and D-dimer levels (median: 3.5 [IQR, 2.6–5.2] vs. median 1.7 [IQR, 0.8–3.1], P = 0.003; median 364.6 [IQR, 3.5–1475.0] vs. median 0.5 [IQR, 0.4–6.5], P = 0.000, respectively) and lower hemoglobin levels (median, 100.5 [IQR, 86.0–115.0] vs. median, 128.0 [IQR, 122.0–136.0], P < 0.001).
Table 2. Laboratory findings of two groups of patients infected with 2019-nCoV.
| Laboratory Findings | All patients (n=59) | ICU care (n=44) | No ICU care (n=15) | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White blood cell count(×109/L) | 5.5(4.3-7.1) | 5.2(4.1-7.0) | 5.8(4.6-7.0) | 0.334 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <4 | 11(19%) | 9(20%) | 2(13%) | 0.894 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4-10 | 42(71%) | 30(68%) | 12(80%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >10 | 6(10%) | 5(11%) | 1(7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ne utrophil count(×109/L) | 3.2(1.9-4.8) | 3.5(2.6-5.2) | 1.7(0.8-3.1) | 0.003 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymphocyte count(×109/L) | 1.1(0.6-1.5) | 0.9(0.6-1.3) | 1.6(0.9-2.3) | 0.004 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <1.0 | 26(44%) | 23(52%) | 3(20%) | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥1.0 | 33(56%) | 21(48%) | 12(80%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Haemoglobin, g/L | 104.0(92.0-122.0) | 100.5(86.0-115.0) | 128.0(122.0-136.0) | 0.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Platelet count(×109/L) | 189.0(145.0-260.0) | 194.5(142.0-264.5) | 189.0(152.0-255.0) | 0.734 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <100 | 11(19%) | 9(20%) | 2(13%) | 0.712 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥100 | 48(81%) | 35(80%) | 13(87%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prothrombin time, s | 12.4(12.0-13.3) | 12.6(12.0-13.4) | 12.0(11.9-13.0) | 0.458 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Activated partial thromboplastin time, s | 30.9(28.0-33.3) | 31.0(27.0-33.9) | 30.5(29.0-31.8) | 0.651 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| D-dimer, mg/L | 6.1(1.5-1090.0) | 364.6(3.5-1475.0) | 0.5(0.4-6.5) | 0.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C-reactive protein, mg/L | 8.4(2.0-30.9) | 9.9(0.3-180.7) | 8.0(0.2-77.9) | 0.807 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alanine aminotransferase, U/L | 37.6(30.2-45.0) | 37.8(25.9-46.7) | 36.7(34.4-40.7) | 0.862 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspartate aminotransferase, U/L | 26.5(21.2-33.3) | 26.5(19.3-35.0) | 26.1(23.8-33.3) | 0.708 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤40 | 51(86%) | 36(82%) | 15(100%) | 0.100 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >40 | 8(14%) | 8(18%) | 0(0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Creatinine, μmol/L | 57.1(44.7-89.9) | 55.7(42.0-83.0) | 89.9(57.0-133.0) | 0.008 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤133 | 53(90%) | 41(93%) | 12(80%) | 0.165 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >133 | 6(10%) | 3(7%) | 3(20%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Creatine kinase, U/L | 116.0(34.6-175.3) | 130.1(34.8-200.0) | 113.9(31.5-167.7) | 0.676 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤185 | 45(76%) | 32(73%) | 13(87%) | 0.483 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >185 | 14(24%) | 12(27%) | 2(13%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data are median (IQR) or n/N (%), where N is the total number of patients with available data. p values comparing Group1 and Group2 are from χ², Fisher’s exact test, or Mann-Whitney U test. 2019-nCoV=2019 novel coronavirus. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
All patients (59/59; 100%) showed abnormal CT findings (Table 3). The main features of the imaging examination were ground-glass opacity (58/59; 98%; Figure 1A), consolidation (37/59; 63%), and ground-glass opacity combined with consolidation (36/59; 61%; Figure 1B). Compared to non-ICU patients, the incidence of consolidation and ground-glass opacity combined with consolidation in ICU patients was higher (73% vs. 33%, P = 0.006; 70% vs. 33%, P = 0.011, respectively). Furthermore, 40/59 (68%) patients showed involvement of all lung lobes in the ICU group (Figure 1C) as compared to the non-ICU patients, whereas the incidence of all lung lobes (75% vs. 47%, P = 0.043) and the number of lung lobes were higher in patients with ICU (median, 5 [IQR, 5–5] vs. median, 4 [IQR, 2–5], P = 0.012). Among 59 patients with COVID-19, 43 (73%) were multifocal, 15 (25%) were diffuse, and only 1 (2%) was focal. A significant difference was detected in the degree of lung involvement between ICU and non-ICU patients (P = 0.032). Furthermore, 23 (39%) patients had abnormal density shadows around the bronchi: 21/44 (48%) ICU patients and 2/15 (13%) non-ICU patients. The incidence of bronchovascular involvement in ICU patients was significantly higher than that in non-ICU patients (48% vs. 13%, P = 0.040), which might be observed by breathing difficulty and need for mechanical ventilation (Figure 1D). Unilateral or bilateral pleural effusion occurred in 7/59 (12%) patients: 6 in the ICU group (6/44, 14%) and 1 in the non-ICU group (1/15, 7%). In addition, mediastinal lymphadenopathy (short axis, >1 cm) was observed in 13 of 59 patients (22%), fibrous cord shadow in 22 (37%), and arterial plaque in 32 (54%).
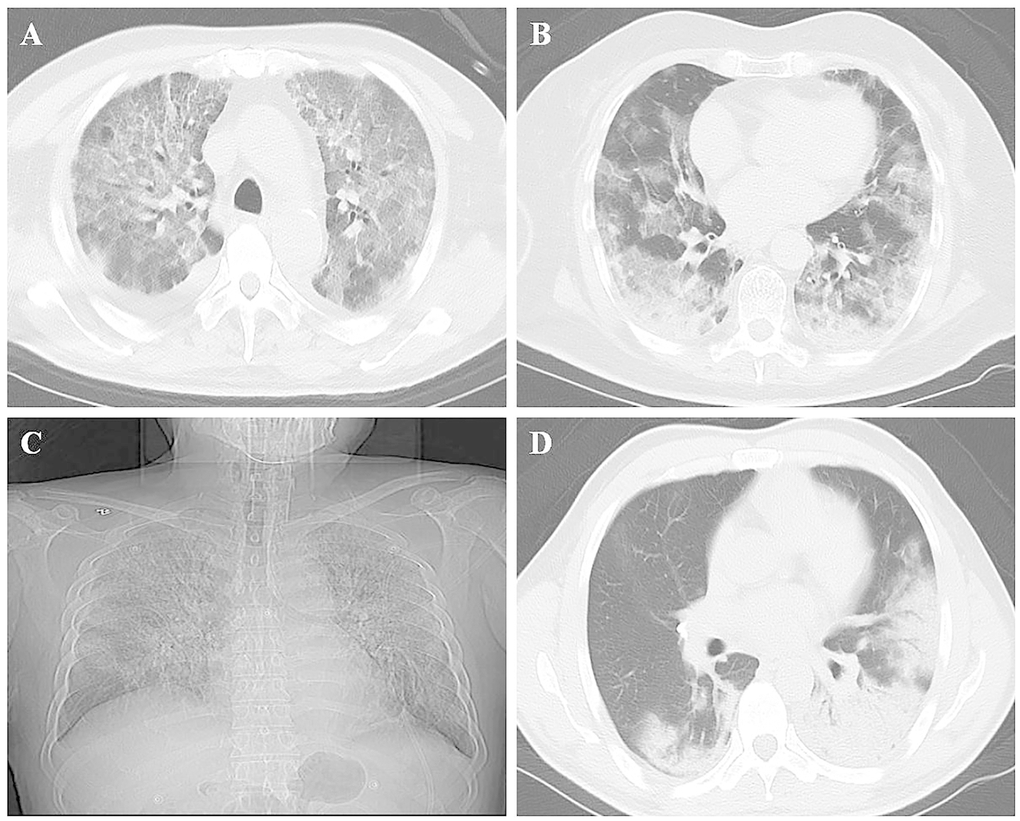
Figure 1. Chest imaging of patients with COVID-19. (A) Ground-glass opacity; (B) Lesion with ground-glass opacity and consolidation; (C) Lesion involving all lung lobes of both lungs; (D) Lesion involving the surrounding area of the bronchial blood vessel.
Table 3. CT diagnosis characteristics of two groups of patients infected with 2019-nCoV.
| Imaging Findings | All patients (n=59) | ICU care (n=44) | No ICU care (n=15) | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Parenchymal opacities | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Consolidation | 37(63%) | 32(73%) | 5(33%) | 0.006 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GGO | 58(98%) | 43(98%) | 15(100%) | 0.746 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GGO and consolidation | 36(61%) | 31(70%) | 5(33%) | 0.011 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reticular opacities | 13(22%) | 7(16%) | 6(40%) | 0.073 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nodular opacities | 11(19%) | 8(18%) | 3(20%) | 0.574 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laterality | 0.265 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral | 4(7%) | 2(5%) | 2(13%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unilateral | 55(93%) | 42(95%) | 13(87%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Involvement range of lung lobes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| All lung lobe | 40(68%) | 33(75%) | 7(47%) | 0.043 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right upper lobe | 51(86%) | 38(86%) | 7(47%) | 0.673 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right middle lobe | 49(83%) | 39(89%) | 10(67%) | 0.104 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right lower lobe | 54(92%) | 42(95%) | 12(80%) | 0.099 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left upper lobe | 51(86%) | 39(89%) | 12(80%) | 0.407 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left lower lobe | 52(88%) | 41(93%) | 11(73%) | 0.062 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Number of lung lobes, mean | 5(4-5) | 5(5-5) | 4(2-5) | 0.012 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Distribution | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Central and peripheral | 9(15%) | 8(18%) | 1(7%) | 0.424 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Central | 12(20%) | 11(25%) | 1(7%) | 0.160 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peripheral | 53(90%) | 39(89%) | 14(93%) | 0.518 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peribronchovascular | 23(39%) | 21(48%) | 2(13%) | 0.040 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Extent | 0.032 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single shot | 1(2%) | 0(0%) | 1(7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multiple | 43(73%) | 30(68%) | 13(87%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diffuse | 15(25%) | 14(32%) | 1(7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pleural effusion | 6(10%) | 3(7%) | 3(20%) | 0.165 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Arterial plaque | 22(37%) | 15(34%) | 7(47%) | 0.384 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fiber rope | 32(54%) | 27(61%) | 5(33%) | 0.060 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mediastinal lymphadenopathy | 13(22%) | 10(23%) | 3(20%) | 0.569 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data is n/N (%), where N is the total number of patients with available data. Abbreviations: CT, computed tomography; GGO, ground-glass opacity. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
A total of 15 (25%) patients were intubated with respiratory failure. All of them (100%) had ground-glass opacity, showed bilateral lung involvement, and involved more than three lung lobes. Compared to the non-mechanically ventilated patients, these patients requiring mechanical ventilation were more likely to have abnormal lung changes in the area around the bronchi (53% vs. 34%) and showed diffuse distribution (47% vs. 18%).
Discussion
COVID-19 is a new viral outbreak that may have a profound impact on public health. With the increased number of confirmed cases, the number of severe and critical cases in Heilongjiang Province is also continuously increasing. This might be caused by lung tissue inflammation, which in turn, causes organ dysfunction and is even life-threatening. In addition, patients who are severely/critically ill have poor prognosis and higher mortality than non-critically ill ones [6, 7]. A recent assessment showed that the fatality rate of severe pneumonia is 30–50%, leading to severe complications and increasing the medical burden [8]. Thus, early identification of such cases based on changes in chest radiography and clinical features is crucial. In the present study, clinical and imaging characteristics of patients with COVID-19 in the ICU group were determined by comparing the ICU and non-ICU patients.
The most common clinical symptoms in this group of patients were fever and cough. We found that the ICU group was older and more likely to have cardiovascular disease than the non-ICU group. Moreover, older people or people with poor health conditions were found to have a worsening pneumonia, which might be due to the weakened immune system [9]. According to a study report on patients with COVID 19 in Wuhan [10], the probability of all patients with hypertension and cardiovascular disease is 15% and 15%, whereas the corresponding incidence in patients with COVID 19 in Heilongjiang Province is 42% and 44%, which may be attributed to the specific geographical environment of Heilongjiang Province, resulting in a high incidence of cardiovascular diseases. Studies on SARS-CoV and Middle East Respiratory Syndrome (MERS)-CoV infections demonstrated that the risk of exacerbation markedly increases with age and presence of underlying diseases [11–13], which was consistent with the conclusions of this study. The difference in the male-to-female ratio was not significant between the two groups, indicating that gender is not a high-risk cause of disease severity, which is consistent with that of a recent report [14]. Compared to the ICU group, the incidence of muscle soreness was significantly higher in the non-ICU group. This clinical symptom is rarely observed in other related studies and may be related to regional environmental characteristics. Taken together, these clinical manifestations can help clinicians determine the disease severity in clinical practice. Other symptoms in our patients with COVID-19 were similar to that of other coronavirus infections, including dyspnea, headache, abdominal pain, diarrhea, and nausea. For example, SARS and MERS may belong to the same attributed infection and also indicate that the SARS-CoV-2 target cells are located in the lower respiratory tract [15–17].
The present study identified multiple laboratory index differences between non-ICU groups and ICU groups, including lymphocyte, neutrophil, and D-dimer levels. Compared to the non-ICU group, the ICU group is prone to lymphopenia, which is consistent with the results of the latest research report of patients with COVID-19 in Wuhan and China [10, 18]. Lymphopenia in the ICU group indicates that a large number of immune cells are consumed and the immune function is suppressed, demonstrating that lymphocyte damage may be the key to the deterioration of the patient’s condition; therefore, decreased lymphocyte count could be a critical indicator of disease severity [19]. Increased neutrophil and D-dimer levels in patients in the ICU group may be related to cytokine storms caused by the viral invasion, which is supported by recent studies [9, 20]. Notably, patients with high D-dimer levels for the first time are predictive of poor prognosis [20], which is consistent with the opinion of this study.
From a broad perspective, CT manifestations of COVID-19 pneumonia are similar to that of other viral pneumonia. Imaging findings of viral pneumonia include reticular pattern and patchy or diffuse ground-glass opacity, with or without consolidation [21]. In influenza pneumonia, lobular septal thickening and grid-like density shadows are frequently observed, whereas pleural effusion is rare [21]. Despite similarities, some of our patients’ imaging findings are different from those of the traditional seasonal flu.
In this study, all patients with COVID-19 had abnormal chest CT findings. Additionally, ground-glass opacity (98%) and consolidation (63%) are the most common imaging findings in the current study, which is consistent with the results of the recent COVID-19 studies [22]. This phenomenon may be related to exudative inflammation caused by alveolar and interstitial edema of the lung due to viral invasion, and CT is mainly manifested as ground-glass opacity [23]. An autopsy report of patients with COVID-19 pneumonia deaths shows that the ground-glass opacity corresponds to the gray-white alveolar lesions observed by the naked eye, suggesting that the virus mainly causes inflammatory reactions characterized by deep airway and alveolar damage [24]. Herein, we found that compared to the non-ICU group, the incidence of consolidation and ground-glass opacity combined with consolidation in patients in the ICU group was higher (P = 0.006; P = 0.011), indicating that the alveoli of critically ill patients were filled with inflammatory exudates. This means that the virus has spread to the respiratory tract, leading to necrotic bronchitis and diffuse alveolar damage [25, 26], which is consistent with the results of recently published studies [27–29]. Among the 59 (68%) patients, 40 displayed imaging abnormalities involving all lung lobes (5) as compared to 7/15 (47%) of non-ICU patients, whereas 33/44 (75%) of all ICU patients were involved; the difference between the two groups was statistically significant (P = 0.043). In addition, we found that the degree of involvement of lung lesions was statistically significant between the two groups (P = 0.032). Chest imaging features may help the early prediction of the patients’ clinical development early.
In this group of patients, 15 needed mechanical ventilation. Compared to non-mechanical ventilation patients, CT abnormalities in the lungs of patients requiring mechanical ventilation were primarily distributed around the bronchial blood vessels, and diffuse distribution was likely to occur, making patients prone to dyspnea. Some other studies demonstrated that the distribution of abnormal lesions during CT examination may be the decisive factor for the clinical course of patients with COVID-19 [22, 30]. Other imaging features in this study included bilateral lung involvement in 93% of patients, and majority of them (90%) had lung lesions in the peripheral area without emphysema or pulmonary nodules; these imaging abnormalities and distribution patterns are consistent the previously published results [31, 32]. Among the patients in this study, only 7 (12%) had pleural effusion, including 6 (14%) in the ICU group and 1 (7%) in the non-ICU group. Furthermore, pleural effusion is a rare imaging manifestation in patients with COVID-19, and the incidence rate in the ICU group is higher than that in the non-ICU group, which is consistent with the results of Junhua et al.’s study [33].
Nevertheless, this study has some limitations. (1) None of the patients underwent lung biopsy or autopsy, which might have established a correlation between imaging and histopathology. (2) The sample size of the non-ICU group is relatively small. Collecting standardized data for larger populations will help explore clinical manifestations and high-risk factors. (3) As most patients are still in the hospital at the time of submission of this manuscript, risk factors for poor prognosis were not assessed.
Conclusions
In summary, existing cardiovascular disease, fever, and cough in elderly patients with COVID-19 may worsen the condition. Lymphopenia and elevated neutrophil and D-dimer levels are also indicators of COVID-19 disease progression. In addition, imaging findings of patients with severe COVID-19 mainly include consolidation and ground-glass opacity combined with consolidation, which putatively involves all lung lobes and the area around the bronchi. Since several patients are currently in the critical stage, we hope that the results of this study would be beneficial for the disease control, diagnosis, treatment, and prognosis in Heilongjiang Province and worldwide and even reduce the mortality rate.
Materials and Methods
Study population
The study has been approved by the Ethics Committee of the Second Affiliated Hospital of Harbin Medical University and is in accordance with the Helsinki Declaration. According to the COVID-19 pneumonia diagnostic criteria for the diagnosis and treatment of new coronavirus-caused pneumonia (trial version 6) issued by the National Health Commission of the People’s Republic of China [4], the inclusion criteria were as follows: (1) real-time fluorescent reverse transcription-polymerase chain reaction (RT-PCR) for detection of positive cDNA of SARS-CoV-2; (2) untreated newly diagnosed patients; (3) patients with complete clinical data; and (4) all patients who underwent at least one CT scan. Exclusion criteria were as follows: (1) treated non-newly diagnosed patients and (2) missing clinical data. This study included a total of 76 patients confirmed with COVID-19 between February and March 2020, and 59 of them met the above criteria. The cohort was divided into the ICU (n = 44) and non-ICU groups (n = 15). Clinical data of all patients were evaluated: background information such as gender and age and clinical symptoms such as fever, cough, and underlying diseases (hypertension, diabetes, cardiovascular disease, and chronic obstructive pulmonary disease). Laboratory examination results upon admission, including white blood cells, lymphocytes, neutrophils, D-dimer, and C-reactive protein levels, as well as imaging data, were collected.
Image analysis
All CT images were analyzed and diagnosed by two radiologists trained for novel coronavirus. Both radiologists have >5 years of diagnostic experience. Two doctors independently diagnosed all patient images and reached a consensus. In case of disagreement between the two radiologists, a third trained radiologist with >10 years of diagnostic experience was consulted to reach a consensus. Imaging features (ground-glass opacity, consolidation, reticular pattern, and nodular opacity), lesion distribution (unilateral/bilateral, upper/middle/lower lobe, and central/peripheral/bronchial blood vessel surrounding), and degree of involvement (focal/multifocal/diffuse and number of lung lobes) were all abnormal. Radiographic images and CT scans using descriptors were defined using the Fleischner Society Naming Committee [5]. Ground-glass opacity is defined as a hazy area showing increased lung opacity with indistinct pulmonary vessel margins on a radiograph but with preserved bronchial and vascular margins on CT. Consolidation is defined as a homogeneous increase in parenchymal attenuation that obscures vessel margins and airway walls. The reticular pattern is defined as small linear opacities forming a net pattern. Nodular opacity is defined as a well- or poorly defined rounded opacity, measuring up to 3 cm in diameter. Lesion distribution features include unilateral/bilateral and upper/middle/lower lobes. The extent of lesion involvement was divided into focality, multifocality, and diffuse. Focality is defined as an abnormal single lesion, whereas multifocality is defined as the presence of more than one lesions; if it is diffusely distributed, it involves one or both lungs. Moreover, whether the lesion occurs centrally (<4 cm from the hilum) or peripherally or involves the bronchi should be determined. The presence of pleural effusion, laterality, and any other lung findings such as mediastinal lymphadenopathy was also noted.
Statistical analysis
The SPSS 19.0 statistical software was used for analysis. Continuous variables were expressed as median (interquartile ratio [IQR]) and compared using the Mann–Whitney U test. Categorical variables were expressed as number of cases (n) and percentage/rate (%); χ² test or Fisher’s exact test was used to compare ICU and non-ICU groups. P < 0.05 was considered statistically significant.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This study was supported by grants from the National Key Research and Development Program of China (2019YFC0118100), National Natural Science Foundation of China (81671760 and 81873910), Scientific Research Transformation Special Fund of Heilongjiang Academy of Medical Sciences (2018415); Scientific Research Project of Health and Family Planning Commission of Heilongjiang Province (201812 and 201622) and Postgraduate Research & Practice Innovation Program of Harbin Medical University (YJSKYCX2018-62HYD).
References
- 1. World Health Organization. WHO/Novel Coronavirus-China. 2020. https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/.
- 2. Gorbalenya AE. Severe acute respiratory syndrome-related coronavirus–The species and its viruses, a statement of the Coronavirus Study Group. BioRxiv. 2020.
- 3. National Health Commission of the People’s Republic of China, World Health Organization. China-WHO new coronavirus pneumonia (COVID-19) joint inspection report. 2020. https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
- 4. National Health Commission of the People’s Republic of China. New coronavirus pneumonia diagnosis and treatment plan (trial version 6). 2020.
- 5. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner society: glossary of terms for thoracic imaging. Radiology. 2008; 246:697–722. https://doi.org/10.1148/radiol.2462070712 [PubMed]
- 6. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020; 395:470–73. https://doi.org/10.1016/S0140-6736(20)30185-9 [PubMed]
- 7. Bernheim A, Mei X, Huang M, Yang Y, Fayad ZA, Zhang N, Diao K, Lin B, Zhu X, Li K, Li S, Shan H, Jacobi A, Chung M. Chest CT findings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology. 2020; 295:200463. https://doi.org/10.1148/radiol.2020200463 [PubMed]
- 8. Wu P, Hao X, Lau EH, Wong JY, Leung KS, Wu JT, Cowling BJ, Leung GM. Real-time tentative assessment of the epidemiological characteristics of novel coronavirus infections in Wuhan, China, as at 22 january 2020. Euro Surveill. 2020; 25:2000044. https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000044 [PubMed]
- 9. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020; 395:507–13. https://doi.org/10.1016/S0140-6736(20)30211-7 [PubMed]
- 10. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395:497–506. https://doi.org/10.1016/S0140-6736(20)30183-5 [PubMed]
- 11. Cowling BJ, Muller MP, Wong IO, Ho LM, Lo SV, Tsang T, Lam TH, Louie M, Leung GM. Clinical prognostic rules for severe acute respiratory syndrome in low- and high-resource settings. Arch Intern Med. 2006; 166:1505–11. https://doi.org/10.1001/archinte.166.14.1505 [PubMed]
- 12. Lau EH, Hsiung CA, Cowling BJ, Chen CH, Ho LM, Tsang T, Chang CW, Donnelly CA, Leung GM. A comparative epidemiologic analysis of SARS in Hong Kong, Beijing and Taiwan. BMC Infect Dis. 2010; 10:50. https://doi.org/10.1186/1471-2334-10-50 [PubMed]
- 13. Hui DS, Azhar EI, Kim YJ, Memish ZA, Oh MD, Zumla A. Middle east respiratory syndrome coronavirus: risk factors and determinants of primary, household, and nosocomial transmission. Lancet Infect Dis. 2018; 18:e217–27. https://doi.org/10.1016/S1473-3099(18)30127-0 [PubMed]
- 14. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020; 323:1061–69. https://doi.org/10.1001/jama.2020.1585 [PubMed]
- 15. Lee N, Hui D, Wu A, Chan P, Cameron P, Joynt GM, Ahuja A, Yung MY, Leung CB, To KF, Lui SF, Szeto CC, Chung S, Sung JJ. A major outbreak of severe acute respiratory syndrome in hong kong. N Engl J Med. 2003; 348:1986–94. https://doi.org/10.1056/NEJMoa030685 [PubMed]
- 16. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, Al-Rabiah FA, Al-Hajjar S, Al-Barrak A, Flemban H, Al-Nassir WN, Balkhy HH, Al-Hakeem RF, Makhdoom HQ, Zumla AI, Memish ZA. Epidemiological, demographic, and clinical characteristics of 47 cases of middle east respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study. Lancet Infect Dis. 2013; 13:752–61. https://doi.org/10.1016/S1473-3099(13)70204-4 [PubMed]
- 17. Müller NL, Ooi GC, Khong PL, Zhou LJ, Tsang KW, Nicolaou S. High-resolution CT findings of severe acute respiratory syndrome at presentation and after admission. AJR Am J Roentgenol. 2004; 182:39–44. https://doi.org/10.2214/ajr.182.1.1820039 [PubMed]
- 18. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DS, Du B, Li LJ, Zeng G, et al, and China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382:1708–20. https://doi.org/10.1056/NEJMoa2002032 [PubMed]
- 19. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, Liu S, Zhao P, Liu H, Zhu L, Tai Y, Bai C, Gao T, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020; 8:420–22. https://doi.org/10.1016/S2213-2600(20)30076-X [PubMed]
- 20. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395:1054–62. https://doi.org/10.1016/S0140-6736(20)30566-3 [PubMed]
- 21. Kim EA, Lee KS, Primack SL, Yoon HK, Byun HS, Kim TS, Suh GY, Kwon OJ, Han J. Viral pneumonias in adults: radiologic and pathologic findings. Radiographics. 2002; 22:S137–49. https://doi.org/10.1148/radiographics.22.suppl_1.g02oc15s137 [PubMed]
- 22. Li K, Wu J, Wu F, Guo D, Chen L, Fang Z, Li C. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Invest Radiol. 2020; 55:327–31. https://doi.org/10.1097/RLI.0000000000000672 [PubMed]
- 23. Ketai LH. Conventional wisdom: unconventional virus. AJR Am J Roentgenol. 2009; 193:1486–87. https://doi.org/10.2214/AJR.09.3758 [PubMed]
- 24. Liu Q, Wang R, Qu G. Anatomy of a new coronavirus pneumonia death corpse system. J Forensic Med. 2020; 36:19–21.
- 25. Koo HJ, Lim S, Choe J, Choi SH, Sung H, Do KH. Radiographic and CT features of viral pneumonia. Radiographics. 2018; 38:719–39. https://doi.org/10.1148/rg.2018170048 [PubMed]
- 26. Franquet T. Imaging of pulmonary viral pneumonia. Radiology. 2011; 260:18–39. https://doi.org/10.1148/radiol.11092149 [PubMed]
- 27. Song F, Shi N, Shan F, Zhang Z, Shen J, Lu H, Ling Y, Jiang Y, Shi Y. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology. 2020; 295:210–17. https://doi.org/10.1148/radiol.2020200274 [PubMed]
- 28. Pan F, Ye T, Sun P, Gui S, Liang B, Li L, Zheng D, Wang J, Hesketh RL, Yang L, Zheng C. Time course of lung changes at chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology. 2020; 295:715–21. https://doi.org/10.1148/radiol.2020200370 [PubMed]
- 29. Kanne JP. Chest CT findings in 2019 novel coronavirus (2019-nCoV) infections from Wuhan, China: key points for the radiologist. Radiology. 2020; 295:16–17. https://doi.org/10.1148/radiol.2020200241 [PubMed]
- 30. Wu J, Wu X, Zeng W, Guo D, Fang Z, Chen L, Huang H, Li C. Chest CT Findings in Patients With Coronavirus Disease 2019 and Its Relationship With Clinical Features. Invest Radiol. 2020; 55:257–261. https://doi.org/10.1097/RLI.0000000000000670 [PubMed]
- 31. Xu X, Yu C, Qu J, Zhang L, Jiang S, Huang D, Chen B, Zhang Z, Guan W, Ling Z, Jiang R, Hu T, Ding Y, et al. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur J Nucl Med Mol Imaging. 2020; 47:1275–80. https://doi.org/10.1007/s00259-020-04735-9 [PubMed]
- 32. Chung M, Bernheim A, Mei X, Zhang N, Huang M, Zeng X, Cui J, Xu W, Yang Y, Fayad ZA, Jacobi A, Li K, Li S, Shan H. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology. 2020; 295:202–07. https://doi.org/10.1148/radiol.2020200230 [PubMed]
- 33. Cheng K, Wei M, Sheng C, Chen D, Xiong W, Zhou X, Zhang D, Zheng J. [Analysis of clinical characteristics of 463 patients with common and severe new coronavirus pneumonia]. Shanghai Medical Journal=Shang Hai Yi Xue. 2020.