



Introduction
Alzheimer’s disease (AD) is a neurodegenerative disorder of elderly individuals and is characterized by the accumulation of β-amyloid and tau in brain, progressive brain atrophy, and cognitive decline [1]. With the increase of life expectancy in developed countries, the incidence of AD and its socioeconomic impact are also growing [2]. Currently, there is no preventive or disease-modifying therapeutic measures, therefore identification of modifiable risk factors is required. The well-established AD biomarkers include cerebrospinal fluid (CSF) biomarkers of β-amyloid 42 (Aβ42), total tau (T-tau), and phosphorylated tau (P-tau); positron emission tomography (PET) measurements of Aβ and tau; and structural magnetic resonance imaging (MRI) measurements [3–5], which are increasingly used to support the diagnosis of AD in research, clinical practice and drug development and have become part of the newly revised early diagnostic criteria for AD [6, 7]. Therefore, it is necessary to investigate the associations between susceptibility factors and biomarkers in the preclinical stage of AD, which is helpful for early identification of modifiable factors.
Pulse pressure (PP) is an index of vascular aging and displays a linear increase with age [8]. It has also been recognized as a marker of increased arterial stiffness and widespread atherosclerosis. Atherosclerosis and cerebrovascular diseases have been implicated in the occurrence and development of AD [9, 10]. Therefore, it is biologically plausible to suppose that high pulse pressure could be related to the development of AD [11]. Several relevant studies indicated that high PP was associated with AD pathophysiology [8, 12–14], suggesting that vascular aging might increase AD risk [11]. Some studies suggested PP elevation was associated with CSF P-tau and Aβ42 in cognitively normal older adults [8]. Others found arterial stiffness was associated with Aβ plaque deposition in the brain [15]. Furthermore, previous studies indicated arterial stiffness might play a role in early cognitive decline and brain atrophy in mid-to-late life [13, 14, 16]. However, these studies were mostly limited by their cross-sectional design and small samples, and the mechanisms underlying the association between PP and AD were still unclear.
More studies are warranted to explore whether PP might increase AD risk or not. This study was designed to investigate whether PP was related to baseline and longitudinal changes in AD biomarkers such as CSF biomarkers, cortical amyloid-beta load, MRI measurements and neuropsychological composites in a large sample of non-demented elderly from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) study.
Results
Demographic and clinical data
There were 669 people with high PP and 706 with normal PP in the ADNI. Comparisons of characteristics between groups were presented in Table 1. Participants in the high PP group were more likely to be older (P < .001) and hypertension (P < .001) than those with normal PP. But there was no group difference in gender, education, APOE Ɛ4 carrier status, and other vascular risk factors (all P > .050). Clinical profiles of patients changed drastically due to data availability issues, the new selected sub-datasets were presented in Supplementary Table 1.
Table 1. Participant demographic and clinical information.
| Participant features | Normal PP (<60mmHg) | High PP (≥60mmHg) | P Value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | 706 | 669 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age(Mean ± SD, year) | 72.31±6.91 | 74.73±6.86 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender (M/F) | 396/310 | 366/303 | 0.606 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education (Mean ± SD, year) | 16.19±2.76 | 16±2.83 | 0.214 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE Ɛ4 carrier status (2/1/0) | 59/248/399 | 47/226/396 | 0.500 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (Mean ± SD, kg/m2) | 27.1±4.84 | 26.94±4.78 | 0.373 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CVD(yes/no) | 156/550 | 154/515 | 0.682 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperlipemia (yes/no) | 329/377 | 320/349 | 0.647 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension (yes/no) | 296/410 | 347/322 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2DM (yes/no) | 44/662 | 60/609 | 0.055 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cognitive diagnoses | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CN/MCI | 255/451 | 259/410 | 0.320 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: Normal PP=normal pulse pressure; High PP=high pulse pressure; SD=standard deviation; APOE, apolipoprotein epsilon; BMI, Body Mass Index; CVD, Cardiovascular Disease; T2DM, Type 2 diabetes mellitus; CN, cognitively normal; MCI, mild cognitive impairment. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Pulse pressure and CSF biomarkers
CSF measurements were available for 977 non-demented participants at baseline (n = 364 CN, 613 MCI), of whom 517 had normal PP. In cross-sectional analyses, after excluding extreme outlines, high PP was associated with a decrease in Aβ42 (β = -.525, P = .015, Figure 1A), as well as increases in T-tau (β = .077, P = .011, Figure 1B), P-tau (β = .097, P = .003, Figure 1C), T-tau/Aβ42 (β = .131, P = .004, Figure 1D) and P-tau/Aβ42 (β = .157, P = .001, Figure 1E) after adjustment for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors, cognitive diagnosis and extracted CSF volume. When stratified by cognitive diagnosis, the associations between PP and CSF biomarkers still persisted within MCI group and high PP was associated with higher P-tau and P-tau/Aβ42 levels in CN group (Figure 1C and 1E); when stratified by age, the associations between PP and CSF biomarkers still persisted within very old group and PP elevation was associated with increased T-tau/Aβ42 in young old group (Supplementary Table 2).
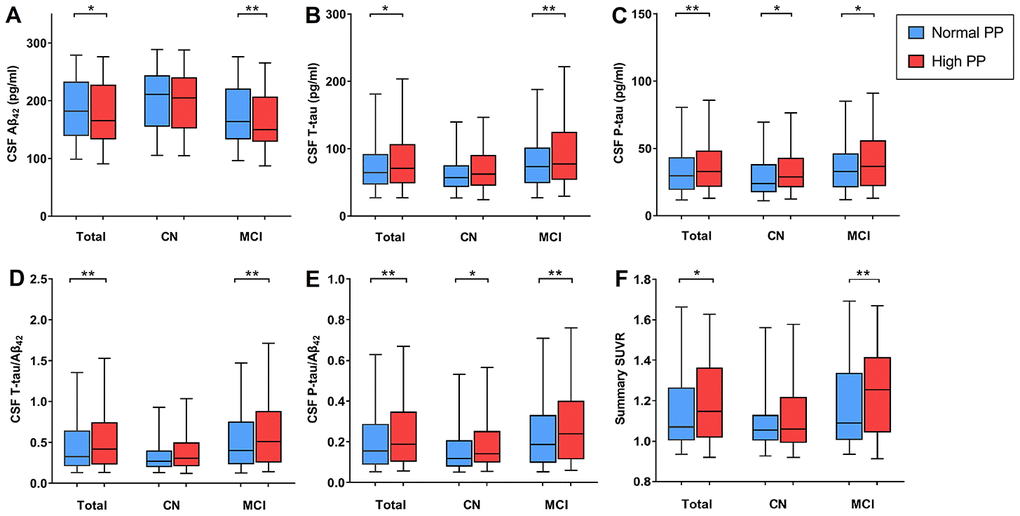
Figure 1. Association between pulse pressure (PP) and AD biomarkers at baseline. (A) PP is negatively correlated with CSF Aβ42 within non-dementia and MCI groups; (B) PP is positively correlated with CSF T-tau within non-dementia and MCI groups; (C) PP is positively correlated with P-tau in all diagnostic groups; (D) PP is positively correlated with CSF T-tau/ Aβ42 within non-dementia and MCI groups; (E) PP is positively correlated with CSF P-tau/Aβ42 in all diagnostic groups; (F) PP was positively correlated with cortical Aβ load in summary SUVR within non-dementia and MCI groups. Abbreviations: AD, Alzheimer’s disease; CSF, cerebrospinal fluid; CN, cognitively normal; MCI, mild cognitive impairment; Aβ, β-amyloid; SUVR, standardized uptake value ratio. *p<.05; **p<.01; *** p<.001.
There were 526 people who had at least one follow-up visit at baseline enrolled in the five-year longitudinal analysis. Longitudinally, we did not find any association between baseline PP and CSF biomarkers. Similarly, no associations were detected when the analyses were stratified by cognitive diagnosis (Supplementary Table 2), while baseline high PP was associated with lower T-tau/Aβ42 in the young old subgroup when stratified by age (Supplementary Table 2).
Pulse pressure and AV45 PET imaging
The mean Aβ load measured by the florbetapir AV45 standardized uptake value ratio (SUVR) was available in 739 participants at baseline (n = 280 CN, 459 MCI), of whom 358 had high PP. In cross-sectional analyses, after excluding extreme outlines, we found that PP was positively correlated with cortical Aβ load in summary SUVR (β = .018, P=.011, Figure 1F) when adjusted for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors, cognitive diagnosis and florbetapir mean of composite ref region. When stratified by cognitive diagnosis and age, the association between PP and cortical Aβ load remained significant within MCI (β = .034, P = .003, Figure 1F) and the young old group (Supplementary Table 2).
There were 550 people who had at least one follow-up visit at baseline enrolled in the five-year longitudinal analysis. Longitudinally, we did not identify a statistically significant association between PP and summary SUVR (β = 1.457*e-3, P = .144). Similarly, no associations were detected when the analyses were stratified by cognitive diagnosis or age (Supplementary Table 2).
Pulse pressure and MRI measurements
Measurements of hippocampal, entorhinal, and mid-temporal volumes were available in 1,137 participants at baseline (n = 694 MCI), of whom 554 had high PP. In cross-sectional analyses, after excluding extreme outlines, increased PP was not associated with hippocampal volume (β = -1.084*e3, P = .312), entorhinal volume (β = -2.311*e1, P = .554), or mid-temporal volume (β = 4.364*e1, P = .752) when adjusted for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors, cognitive diagnosis and intracranial volume. Similarly, no associations were detected between PP and MRI structure when the analyses were stratified by cognitive diagnosis and age (Supplementary Table 3).
There were 1,042 who had at least one follow-up visit at baseline enrolled in the five-year longitudinal analysis. Longitudinally, increased PP was associated with an accelerated decline in hippocampal volume (β = -16.903, P = .039, Figure 2A) and entorhinal volume (β = -20.014, P = .031, Figure 2B) over time. When stratified by cognitive diagnosis and age, the association between PP and entorhinal volume still persisted among those with MCI and the young old subgroup (Supplementary Figure 1A and Table 3).
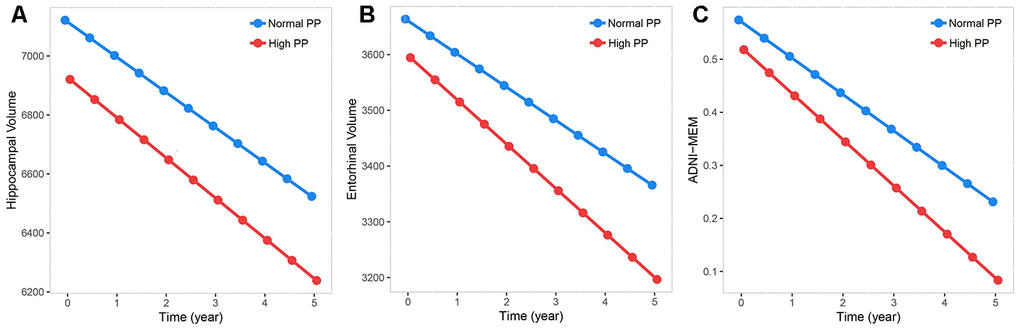
Figure 2. Associations between baseline pulse pressure and measurements of brain aging. Data from linear mixed-effects models adjusted for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors, cognitive diagnosis, as well as intracranial volume. Increased PP level was associated with an accelerated decline in measurements of brain aging. (A–C) Increased PP level was associated with accelerated decline in hippocampal volume, entorhinal volume and episodic memory performance.
Pulse pressure and ADNI-MEM & ADNI-EF
ADNI-MEM and ADNI-EF were available in 1,375 (n = 514 CN, 861 MCI) participants at baseline, of whom 706 had normal PP. In cross-sectional analyses, no association of PP was found with memory performance (β = −.030, P = .343) or executive function performance (β = −.042, P = .298). Similarly, no association was detected when the analyses were stratified by cognitive diagnosis while high PP was associated with worse memory performance in young old group when stratified by age (Supplementary Table 3).
There were 1322 who had at least one follow-up visit at baseline enrolled in the five-year longitudinal analysis. Longitudinally, increased PP was associated with worse memory performance with a strong tendency towards statistical significance (β = -1.829*e-2, P = .058, Figure 2C). In stratified analyses restricted to MCI participants, increased PP was associated with a greater decline in memory performance over time (β = −.034, P = .012, Supplementary Figure 1B and Table 3). We did not find any statistically significant associations in other stratified analyses (Supplementary Table 3).
Pulse pressure and clinical disease progression
Kaplan-Meier analysis revealed participants with high PP at baseline showed more rapid progression over the following five years, compared with those with normal PP (P <.001, Figure 3). In Cox regression models (adjusted for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors and cognitive diagnosis), the individuals with high PP had a higher risk of progression to AD (hazard ratio 1.216, 95% CI 1.051-1.461, P = .011).
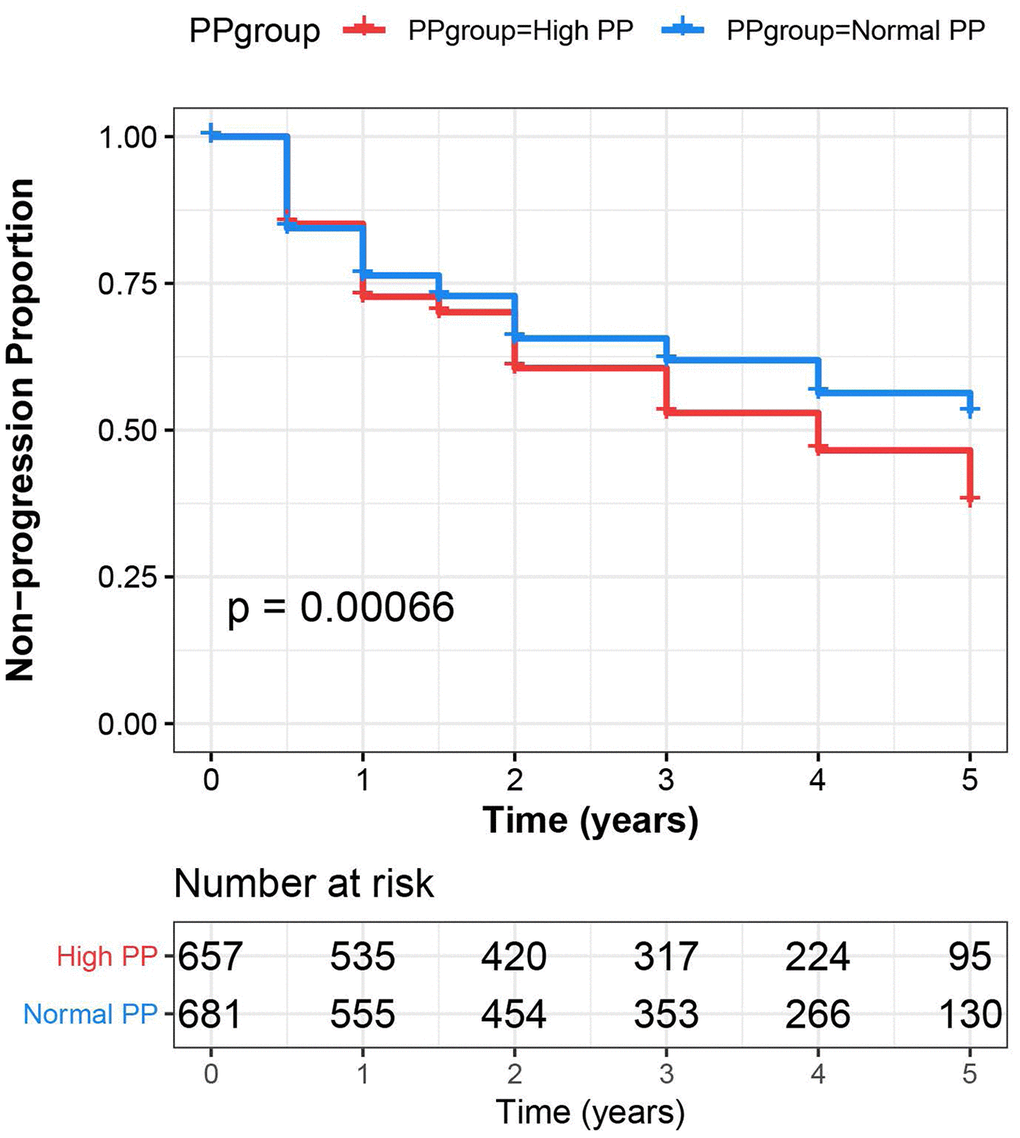
Figure 3. Pulse pressure predicts more rapid progression to dementia. The Cox regression indicates that a higher pulse pressure was associated with more rapid progression to dementia. Visually, the survival plot displays results for high pulse pressure in comparison with normal pulse pressure.
Systolic blood pressure (SBP), diastolic blood pressure (DBP) and hypertension
SBP exhibited the same pattern of associations with CSF biomarkers found in the PP analyses. Higher SBP was associated with a decrease in Aβ42, as well as increases in T-tau, P-tau, T-tau/Aβ42 and P-tau/Aβ42 (Supplementary Table 4); in AV45 PET imaging analyses, SBP was positively correlated with cortical Aβ load in summary SUVR, and the association still persisted within MCI and the young old subgroup (Supplementary Table 4); in MRI measurements analyses, we only found that higher SBP was associated with smaller mid-temporal volume within MCI (Supplementary Table 4); in ADNI-MEM and ADNI-EF analyses, higher SBP was associated with worse memory performance and executive function performance in the young old subgroup (Supplementary Table 4).
There was no association between DBP and CSF biomarkers or AV45 PET imaging analyses (Supplementary Table 5); in MRI measurements analyses, DBP was negatively correlated with mid-temporal volume and it still persisted within MCI subgroup (Supplementary Table 5); in ADNI-MEM and ADNI-EF analyses, higher DBP was associated with worse memory performance, and when stratified by age, the association still persisted within very old subgroup while higher DBP was associated with worse executive function performance in MCI subgroup when stratified by cognitive diagnosis (Supplementary Table 5).
Hypertension exhibited the same pattern of associations with CSF biomarkers and AV45 PET imaging found in the DBP analyses (Supplementary Table 6); in MRI measurements analyses, we found hypertension was negatively correlated with hippocampal volume, entorhinal volume, and mid-temporal volume in the young old subgroup (Supplementary Table 6); in ADNI-MEM and ADNI-EF analyses, hypertension was associated with worse executive function performance, and when stratified by age and cognitive diagnosis, the association still persisted within MCI, the young old and very old subgroups while association between hypertension and memory performance was found in the young old subgroup (Supplementary Table 6).
Discussion
In this study, PP elevation was found to be associated with CSF Aβ42, T-tau, P-tau, T-tau/ Aβ42 and P-tau/Aβ42, as well as cortical Aβ load at baseline; and longitudinally, an increase in PP was associated with an accelerated decline in hippocampal and entorhinal volumes, and with worsening episodic memory. These associations seemed to be more obvious in MCI and very old patients, suggesting that the relationships between pulse pressure and cognitive disorders were age- and diagnosis- dependent [17]. Individuals with higher PP also had a higher incidence of conversion to AD. Taken together, these findings supported that PP elevation could increase risk of AD, and the associations maybe driven by amyloid plaques and subclinical neurodegeneration, which was consistent with the conclusion from previous studies that elevated PP had a negative impact on hallmark neuropathological markers of AD [8, 12, 13, 18]. These likely suggested PP can be added to the current dementia risk models for dementia prevention, if controlled effectively, it would help delay the onset and reduce the number of demented people in the future.
In CSF biomarkers analyses, when stratified by cognitive diagnosis, the associations between PP and P-tau, P-tau/Aβ42 still persisted among MCI and CN groups, while the relationship between Aβ42 and PP only persisted within MCI group, which possibly revealed that the relationship between PP and P-tau was detected at early stages. These findings indicated that PP may be related to both amyloid plaques and tau-mediated neurodegeneration, and the latter mechanism may be more salient, which was consistent with previous articles [8, 19]. Although AD is characterized by both amyloid- and tau-based pathologies, P-tau is more strongly associated with neurodegeneration and cognitive decline; besides, we also find that PP is associated with brain atrophy and cognitive decline, suggesting that high PP may convey AD risk through its closer association with tau phosphorylation [8]. Previous work has indicated that amyloid is not cause of AD but the downstream result [20] and nearly 23% of elderly exhibit P-tau elevation in the absence of amyloidosis [21]. And the update of an AD model indicates that neurodegeneration may occur independently and ahead of amyloid pathology and may be exacerbated by the later development of amyloidosis [22, 23]. However, the underlying pathological mechanisms warrant further investigation. Longitudinally, baseline high PP was associated with lower T-tau/Aβ42 in the young old subgroup, it seemed conflicting, which may be explained by the large number of subjects lost to follow-up, especially in the 3-, 4-, 5-year follow-up.
In MRI analyses, increased PP accelerated the decrease in hippocampal and entorhinal volumes, which was consistent with the previous finding that blood pressure can preferentially affect the hippocampal volume [24]. Though the responsible mechanism linking PP to reduced hippocampal volume has not been elucidated, Beauchet et.al have showed preferential global and regional effects of blood pressure on the brain, including the hippocampus [25]. These effects may be mediated in part by blood pressure-related arteriolosclerosis, low blood flow, and consequent hypoperfusion in the hippocampal [25]. Importantly, loss of vascular elasticity and increased vascular resistance, caused partly by increased vascular amyloid deposit, may mediate such effects [26–28].
Despite the growing recognition that vascular risk factors may have an impact on the development of AD, the pathophysiological mechanism needs further understanding. In fact, mounting evidence suggests that the pulsation of the arteries contributes to the clearance of wastes from the central nervous system [29, 30]. Besides, some studies suggest that circulatory injuries, such as those caused by stiffening of the vasculature system, may result in failure of clearance of Aβ from the brain [31]. To be more specific, elevated PP may stimulate vascular hypertrophy, remodeling, or rare in the microcirculation, leading to increased vascular resistance, impaired microvascular reserve [32–34], which may subsequently cause structural changes, impair clearance of Aβ42 along the perivascular spaces [35], as well as decrease arterial pulsatility and capacity for amyloid drainage [36]. Therefore, dysfunction of this system may promote neurodegeneration [37]. It is also possible that changes in vascular function could lead to reduced tissue perfusion and arteriolar hypercontractility, or blood-brain barrier (BBB) leakage, either of which may result in neurodegeneration and increased P-tau [38]. More animal-model studies are needed to shed light on the potential mechanisms via which PP influences AD.
Although PP was the primary focus of the study, we also examined SBP, DBP and hypertension in relation to biomarkers to determine their contributions to PP. We found that increased SBP was associated with CSF biomarkers, cortical Aβ load, brain volume and cognition, and the associations seemed to be more obvious in MCI and very old patients, which revealed that SBP may exhibit the similar pattern of association found in PP, while associations between DBP, hypertension and AD biomarkers mainly reflected in MRI measurements and cognition, this likely reflected the greater relative contributions of SBP to PP. PP elevation represented either increased SBP or decreased DBP, which may provide insight into the relationship between blood pressure and neurodegeneration. Furthermore, the associations above supported that higher SBP, DBP and hypertension may increase AD risk.
In Table 1, we found participants in the high PP group were more likely to be T2DM (P = .055), it seemed a link between PP and T2DM in AD, which may be mediated in part by vascular injuries. Some studies suggest that micro-vascular damage, sympathetic damage, and enhanced renin-angiotensin system, caused by diabetes mellitus, may aggravate systolic blood pressure elevation [39], resulting in high PP; besides, vascular damage such as arteriosclerosis caused by T2DM glycosylation was associated with low blood flow, leading to BBB leakage [40], which may result in neurodegeneration.
The study have several limitations. (1) Although the relationship between PP and dementia is supported by longitudinal analyses in the present study, the attrition bias due to loss to follow-up was not corrected in the analyses. Future studies with larger sample sizes, longer follow-up duration, and lower attrition rates will assist in exploring whether the associations support causality; (2) blood pressure was not an a priori outcome in the ADNI study and its assessment did not employ strict standards (such as average of multiple measurements), which may result in measurement bias; (3) the sample of participants who received pressure-controlled treatment (like anti-hypertension medicine) was small, therefore the analyses about it didn’t performed.
In conclusion, this large-scale study identified the cross-sectional as well as the longitudinal associations of PP and the known biomarkers of AD, suggesting high PP could increase AD risk, and found the PP effects may be modified by cognitive diagnosis and age, and may be driven by amyloid plaques and subclinical neurodegeneration. Furthermore, our study encourages future studies to consider PP as a target for AD prevention. However, the potential pathological mechanisms linking age-related vascular stiffening to neurodegeneration warrant further investigation, such as reduced brain blood flow, increased blood-brain barrier permeability, and decreased clearance of misfolded proteins, and pharmacological modulation in human subjects or configured animal models maybe helpful to elucidate the underlying mechanisms.
Materials and Methods
ADNI
The data used for this analysis were downloaded from the ADNI database (adni.loni.usc.edu). The ADNI, an ongoing, multisite longitudinal, large-scale study launched in 2003, was designed to develop clinical, imaging, genetic and biochemical biomarkers for the early detection and tracking of AD [41]. Participants in the ADNI study underwent baseline and periodic physical and neurological examinations, standardized neuropsychological assessments, and biological sampling (blood, urine, and CSF) [13]. Regional ethical committees of all participating institutions approved the ADNI. All study participants provided written informed consent.
Participants
A total of 2,046 participants from ADNI1, ADNI Grand Opportunity, and ADNI 2 completed the blood pressure assessment at baseline. Among them, 335 participants without demographic and clinical information, and 336 who were classified as dementia were excluded. Finally, the remaining 1,375 non-demented participants were enrolled in this study (Figure 4). Clinical disease progression was ascertained for a large subset of participants (n = 1,338) who were followed up with serial clinical assessments at varying intervals for different length of time ranging from 0 year to 5 years.
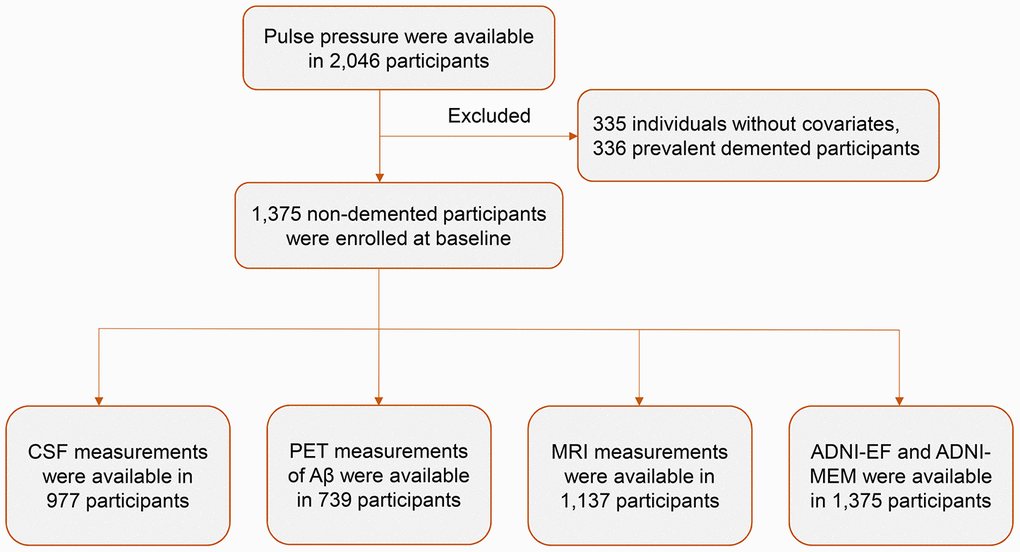
Figure 4. Flow diagram of participant selection. Abbreviations: CSF, cerebrospinal fluid; MRI, magnetic resonance imaging.
PP measurements
Seated brachial artery SBP and DBP were obtained and PP was calculated as the difference between SBP and DBP. PP of 60 mmHg or higher was defined as high PP [42].
Covariates
Accumulating evidence supports a role of vascular risk factors in the development and etiology of AD [43]. For purposes of this study, participant medical history data of vascular risk factors was obtained until the date of baseline blood pressure. The covariates consisted of age, gender, education, APOE Ɛ4 carrier status, body mass index (BMI) which was calculated as weight in kilograms divided by the square of height in meters, and vascular risk factors, such as type 2 diabetes mellitus (T2DM), hyperlipemia, hypertension, as well as medical history of cardiovascular disease (CVD) including myocardial infarction, angina, heart failure and atrial fibrillation. We classified these diseases based on the medical history information and/or use of anti-medications.
CSF biomarker measurements
The CSF collection and procedural protocols have been described previously [44]. All participants underwent lumbar puncture which was performed with a 20- or 24-gauge spinal needle as described in the ADNI procedures manual (http://www.adni-info.org/) and AD biomarkers including Aβ1-42, P-tau, and T-tau were measured using the multiplex xMAP Luminex platform (Luminex Corp, Austin, TX) with Innogenetics (INNO-BIA AlzBio3; Ghent, Belgium; for research use–only reagents) immunoassay kit–based reagents. All tests were administered at baseline and at 12, 24, 36, 48 and 60 months.
18F florbetapir AV45 PET imaging
Preprocessed florbetapir imaging data were downloaded from the LONI ADNI site (http://adni.loni.usc.edu). The data preprocessing is accessible online (adni. loni. ucla.edu/about-data-samples/image-data/). For quantifying cerebral cortical Aβ, preprocessed florbetapir image data and co-registered structural MRI were analyzed using Freesurfer (version 4.5.0) (surfer.nmr. mgh.harvard.edu/) as described previously and online (adni.loni.ucla.edu/research/pet-post-processing/). Briefly, image data were acquired in four 5-min frames 50–70 minutes after injection of approximately 10mCi of 18F florbetapir, the four frames were co-registered to one another, averaged, interpolated to a uniform image and voxel size (160×106×96, 1.5 mm3), and smoothed to a uniform resolution (8 mm FWHM) to account for differences between scanners [45]. The mean Aβ retention, measured by the florbetapir AV45 SUVR, was normalized to the whole cerebellum as a summary measure of florbetapir retention for each participant in cross-sectional analyses; and a composite reference region, which was made up of whole cerebellum, brainstem/pons, and eroded subcortical white matter, has been evaluated for longitudinal analyses. All tests were administered at baseline and at 12, 24, 36, 48 and 60 months.
Brain structure
The process for MRI acquisition has been described elsewhere in ADNI publications [2, 46–48]. Structural brain images were acquired using 1.5T or 3T MRI systems with T1-weighted scans using a sagittal volumetric magnetization-prepared rapid acquisition gradient echo sequence. The ADNI project offers scans that have been preprocessed (gradient warping, scaling, B1 correction, and N3 inhomogeneity correction) to correct for different scanners across sites [49]. All tests were administered at baseline and at 3, 6, 12, 18, 24, 36, 48 and 60 months.
Neuropsychological composites
The ADNI neuropsychological protocol, including calculation of ADNI-MEM and ADNI-EF composite measures, has been reported previously [50, 51]. The ADNI-MEM included a composite z score based on item-level data from the Rey Auditory Verbal Learning Test, the Mini-Mental State Examination (MMSE), the AD Assessment Scale Cognitive Test, and Logical Memory I and II. The ADNI-EF included item-level data from the Trail Making Test Parts A and B, Digit Span Backward, Digit Symbol, Animal Fluency, Vegetable Fluency, and Clock Drawing Test [52]. All tests were administered at baseline and at 6, 12, 18, 24, 36, 48 and 60 months.
Clinical disease progression
CN and MCI participants were divided into group of clinical disease progression and stable, respectively. Participants were defined as having clinical disease progression if their global CDR/MMSE or clinical classification score changed (CN subjects converted to MCI or AD, or their global CDR scores rose to 0.5 or greater; MCI subjects lost more than 3 points between first and last MMSE, or converted to AD at follow-up, or got a score less than 24 on the last MMSE) [53–55]. If the above criteria have not been met at follow-up, participants were considered stable; regardless of the lost of subjects, once the progression criteria have been met during 5-year follow-up, they were deemed progressive.
Statistical analyses
Baseline demographic, clinical and diagnostic characteristics were compared between PP groups using Mann-Whitney U test for continuous variables and χ2 analyses for categorical variables, respectively. We used means and standard errors for continuous measures and proportions for categories. Multiple linear regression was used to explore the association between PP and biomarkers in cross-sectional analyses after adjusting for age, gender, education, APOE Ɛ4 carrier status, vascular risk factors and cognitive diagnosis at baseline. Before regression analyses, participants who had a value >3 or <3 SD from the mean value were regarded as extreme outlines and excluded. In case of skewed distribution (Shapiro-Wilk test > 0.05) of biomarker data, transformation was performed to approximate a normal distribution via “car” package of R software. Interaction terms for age were used to explore whether strata effect existed, in order to minimize the difference between subgroup sample sizes, we chose 75 years old as the cutoff value (<75 years old vs. ≥ 75 years old). In case of any potential interactions (P < 0.1), subgroup analyses were further performed. Mixed-model regression with time modeled as years from baseline for each participant was used to explore the longitudinal influences of PP at baseline on AD biomarkers and cognition after adjusting with age, gender, education, APOE Ɛ4 carrier status, vascular risk factors, cognitive diagnosis. The time-by-exposure interaction terms tested whether PP were associated with changes in the given outcomes (CSF biomarkers, AV45 PET imaging biomarkers, MRI structure, as well as ADNI-MEM and ADNI-EF) over the follow-up period. Kaplan-Meier survival analysis investigated the relationship between baseline PP and clinical disease progression using years to cognitive decline as the time variable. Cox proportional hazards models (adjusted for age, gender, education, APOE Ɛ4 carrier status, diagnosis, and vascular risk factors) were used to test the predictive ability of baseline PP for clinical disease progression. All tests were two-tailed. Statistical significance was set at P < .05. R version 3.5.1 and GraphPad Prism 7.00 software were used for statistical analyses and figure preparation.
Although PP was the focus of the study, primary cross-sectional analyses which were identical to those used in PP were repeated to examine SBP (< 120mmHg, ≥ 120 and < 140mmHg, ≥ 140mmHg), DBP (< 80mmHg, ≥ 80 and < 90mmHg, ≥ 90mmHg) [56], and hypertension (based on the medical history information and/or use of anti-medications) in relation to biomarkers to determine their contributions to the PP findings. We did this because it was highly correlated with SBP and disambiguated the relative contributions of systolic and diastolic pressure to results, which may have provided mechanistic insight.
Author Contributions
JTY, LT and YY conceptualized the study, analyzed and interpreted the data, and revised the manuscript. WYS analyzed and interpreted the data, drafted and revised the manuscript, and prepared the figures. ZTW and FRS did the statistical analysis, and prepared the figures. YHM, WX and XNS interpreted the data and revised the manuscript. QD and YY drafted and revised the manuscript. LT designed and conceptualized the study, and revised the manuscript. Data used in preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (http://adni.loni.usc.edu). As such, the investigators within the ADNI contributed to the design and implementation of ADNI and/or provided data but did not participate in analysis or writing of this report.
Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by grants from the National Natural Science Foundation of China (91849126, 81571245, and 81771148), the National Key R&D Program of China (2018YFC1314700), Shanghai Municipal Science and Technology Major Project (No.2018SHZDZX01) and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, and the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, Fudan University. Data collection and sharing for this project was funded by the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research and Development, LLC.; Johnson and Johnson Pharmaceutical Research and Development LLC.; Lumosity; Lundbeck; Merck and Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (https://www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
Editorial Note
These corresponding authors have a verified history of publications using their personal email addresses for correspondence.
References
- 1. Scheltens P, Blennow K, Breteler MM, de Strooper B, Frisoni GB, Salloway S, Van der Flier WM. Alzheimer’s disease. Lancet. 2016; 388:505–17. https://doi.org/10.1016/S0140-6736(15)01124-1 [PubMed]
- 2. Mueller SG, Weiner MW, Thal LJ, Petersen RC, Jack CR, Jagust W, Trojanowski JQ, Toga AW, Beckett L. Ways toward an early diagnosis in Alzheimer’s disease: the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Alzheimers Dement. 2005; 1:55–66. https://doi.org/10.1016/j.jalz.2005.06.003 [PubMed]
- 3. Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol. 2010; 6:131–44. https://doi.org/10.1038/nrneurol.2010.4 [PubMed]
- 4. Frisoni GB, Fox NC, Jack CR
Jr , Scheltens P, Thompson PM. The clinical use of structural MRI in Alzheimer disease. Nat Rev Neurol. 2010; 6:67–77. https://doi.org/10.1038/nrneurol.2009.215 [PubMed] - 5. Nordberg A, Rinne JO, Kadir A, Långström B. The use of PET in Alzheimer disease. Nat Rev Neurol. 2010; 6:78–87. https://doi.org/10.1038/nrneurol.2009.217 [PubMed]
- 6. Mattsson N, Carrillo MC, Dean RA, Devous MD
Sr , Nikolcheva T, Pesini P, Salter H, Potter WZ, Sperling RS, Bateman RJ, Bain LJ, Liu E. Revolutionizing Alzheimer’s disease and clinical trials through biomarkers. Alzheimers Dement (Amst). 2015; 1:412–19. https://doi.org/10.1016/j.dadm.2015.09.001 [PubMed] - 7. Jack CR
Jr , Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, Holtzman DM, Jagust W, Jessen F, Karlawish J, Liu E, Molinuevo JL, Montine T, et al, and Contributors. NIA-AA research framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018; 14:535–62. https://doi.org/10.1016/j.jalz.2018.02.018 [PubMed] - 8. Nation DA, Edland SD, Bondi MW, Salmon DP, Delano-Wood L, Peskind ER, Quinn JF, Galasko DR. Pulse pressure is associated with Alzheimer biomarkers in cognitively normal older adults. Neurology. 2013; 81:2024–27. https://doi.org/10.1212/01.wnl.0000436935.47657.78 [PubMed]
- 9. Hofman A, Ott A, Breteler MM, Bots ML, Slooter AJ, van Harskamp F, van Duijn CN, Van Broeckhoven C, Grobbee DE. Atherosclerosis, apolipoprotein E, and prevalence of dementia and Alzheimer’s disease in the rotterdam study. Lancet. 1997; 349:151–54. https://doi.org/10.1016/S0140-6736(96)09328-2 [PubMed]
- 10. van Oijen M, de Jong FJ, Witteman JC, Hofman A, Koudstaal PJ, Breteler MM. Atherosclerosis and risk for dementia. Ann Neurol. 2007; 61:403–10. https://doi.org/10.1002/ana.21073 [PubMed]
- 11. Qiu C, Winblad B, Viitanen M, Fratiglioni L. Pulse pressure and risk of Alzheimer disease in persons aged 75 years and older: a community-based, longitudinal study. Stroke. 2003; 34:594–99. https://doi.org/10.1161/01.STR.0000060127.96986.F4 [PubMed]
- 12. Nation DA, Edmonds EC, Bangen KJ, Delano-Wood L, Scanlon BK, Han SD, Edland SD, Salmon DP, Galasko DR, Bondi MW, and Alzheimer’s Disease Neuroimaging Initiative Investigators. Pulse pressure in relation to tau-mediated neurodegeneration, cerebral amyloid-osis, and progression to dementia in very old adults. JAMA Neurol. 2015; 72:546–53. https://doi.org/10.1001/jamaneurol.2014.4477 [PubMed]
- 13. Ngwa JS, Fungwe TV, Ntekim O, Allard JS, Johnson SM, Castor C, Graham L, Nadarajah S, Gillum RF, Obisesan TO, and Alzheimer’s Disease Neuroimaging Initiative. Associations of pulse and blood pressure with hippocampal volume by APOE and cognitive phenotype: the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Dement Geriatr Cogn Disord. 2018; 45:66–78. https://doi.org/10.1159/000486955 [PubMed]
- 14. Nation DA, Preis SR, Beiser A, Bangen KJ, Delano-Wood L, Lamar M, Libon DJ, Seshadri S, Wolf PA, Au R. Pulse pressure is associated with early brain atrophy and cognitive decline: modifying effects of APOE-ε4. Alzheimer Dis Assoc Disord. 2016; 30:210–15. https://doi.org/10.1097/WAD.0000000000000127 [PubMed]
- 15. Hughes TM, Kuller LH, Barinas-Mitchell EJ, Mackey RH, McDade EM, Klunk WE, Aizenstein HJ, Cohen AD, Snitz BE, Mathis CA, Dekosky ST, Lopez OL. Pulse wave velocity is associated with β-amyloid deposition in the brains of very elderly adults. Neurology. 2013; 81:1711–18. https://doi.org/10.1212/01.wnl.0000435301.64776.37 [PubMed]
- 16. Tsao CW, Seshadri S, Beiser AS, Westwood AJ, Decarli C, Au R, Himali JJ, Hamburg NM, Vita JA, Levy D, Larson MG, Benjamin EJ, Wolf PA, et al. Relations of arterial stiffness and endothelial function to brain aging in the community. Neurology. 2013; 81:984–91. https://doi.org/10.1212/WNL.0b013e3182a43e1c [PubMed]
- 17. Ou YN, Tan CC, Shen XN, Xu W, Hou XH, Dong Q, Tan L, Yu JT. Blood pressure and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 209 prospective studies. Hypertension. 2020; 76:217–25. https://doi.org/10.1161/HYPERTENSIONAHA.120.14993 [PubMed]
- 18. Langbaum JB, Chen K, Launer LJ, Fleisher AS, Lee W, Liu X, Protas HD, Reeder SA, Bandy D, Yu M, Caselli RJ, Reiman EM. Blood pressure is associated with higher brain amyloid burden and lower glucose metabolism in healthy late middle-age persons. Neurobiol Aging. 2012; 33:827.e11–19. https://doi.org/10.1016/j.neurobiolaging.2011.06.020 [PubMed]
- 19. Glodzik L, Rusinek H, Pirraglia E, McHugh P, Tsui W, Williams S, Cummings M, Li Y, Rich K, Randall C, Mosconi L, Osorio R, Murray J, et al. Blood pressure decrease correlates with tau pathology and memory decline in hypertensive elderly. Neurobiol Aging. 2014; 35:64–71. https://doi.org/10.1016/j.neurobiolaging.2013.06.011 [PubMed]
- 20. Drachman DA. The amyloid hypothesis, time to move on: amyloid is the downstream result, not cause, of Alzheimer’s disease. Alzheimers Dement. 2014; 10:372–80. https://doi.org/10.1016/j.jalz.2013.11.003 [PubMed]
- 21. Jack CR
Jr , Knopman DS, Weigand SD, Wiste HJ, Vemuri P, Lowe V, Kantarci K, Gunter JL, Senjem ML, Ivnik RJ, Roberts RO, Rocca WA, Boeve BF, Petersen RC. An operational approach to national institute on aging-Alzheimer’s association criteria for preclinical Alzheimer disease. Ann Neurol. 2012; 71:765–75. https://doi.org/10.1002/ana.22628 [PubMed] - 22. Knopman DS. Β-amyloidosis and neurodegeneration in Alzheimer disease: who’s on first? Neurology. 2014; 82:1756–57. https://doi.org/10.1212/WNL.0000000000000438 [PubMed]
- 23. Jack CR
Jr , Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, Shaw LM, Vemuri P, Wiste HJ, Weigand SD, Lesnick TG, Pankratz VS, Donohue MC, Trojanowski JQ. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013; 12:207–16. https://doi.org/10.1016/S1474-4422(12)70291-0 [PubMed] - 24. Petrovitch H, White LR, Izmirilian G, Ross GW, Havlik RJ, Markesbery W, Nelson J, Davis DG, Hardman J, Foley DJ, Launer LJ. Midlife blood pressure and neuritic plaques, neurofibrillary tangles, and brain weight at death: the HAAS. Honolulu-asia aging study. Neurobiol Aging. 2000; 21:57–62. https://doi.org/10.1016/s0197-4580(00)00106-8 [PubMed]
- 25. Beauchet O, Celle S, Roche F, Bartha R, Montero-Odasso M, Allali G, Annweiler C. Blood pressure levels and brain volume reduction: a systematic review and meta-analysis. J Hypertens. 2013; 31:1502–16. https://doi.org/10.1097/HJH.0b013e32836184b5 [PubMed]
- 26. Sepehry AA, Lang D, Hsiung GY, Rauscher A. Prevalence of brain microbleeds in Alzheimer disease: a systematic review and meta-analysis on the influence of neuroimaging techniques. AJNR Am J Neuroradiol. 2016; 37:215–22. https://doi.org/10.3174/ajnr.A4525 [PubMed]
- 27. Shams S, Granberg T, Martola J, Charidimou A, Li X, Shams M, Fereshtehnejad SM, Cavallin L, Aspelin P, Wiberg-Kristoffersen M, Wahlund LO. Cerebral microbleeds topography and cerebrospinal fluid biomarkers in cognitive impairment. J Cereb Blood Flow Metab. 2017; 37:1006–13. https://doi.org/10.1177/0271678X16649401 [PubMed]
- 28. Schneider JA. High blood pressure and microinfarcts: a link between vascular risk factors, dementia, and clinical Alzheimer’s disease. J Am Geriatr Soc. 2009; 57:2146–47. https://doi.org/10.1111/j.1532-5415.2009.02521.x [PubMed]
- 29. Ueno M, Chiba Y, Murakami R, Matsumoto K, Kawauchi M, Fujihara R. Blood-brain barrier and blood-cerebrospinal fluid barrier in normal and pathological conditions. Brain Tumor Pathol. 2016; 33:89–96. https://doi.org/10.1007/s10014-016-0255-7 [PubMed]
- 30. Weller RO, Djuanda E, Yow HY, Carare RO. Lymphatic drainage of the brain and the pathophysiology of neurological disease. Acta Neuropathol. 2009; 117:1–14. https://doi.org/10.1007/s00401-008-0457-0 [PubMed]
- 31. Bell RD, Deane R, Chow N, Long X, Sagare A, Singh I, Streb JW, Guo H, Rubio A, Van Nostrand W, Miano JM, Zlokovic BV. SRF and myocardin regulate LRP-mediated amyloid-beta clearance in brain vascular cells. Nat Cell Biol. 2009; 11:143–53. https://doi.org/10.1038/ncb1819 [PubMed]
- 32. Baumbach GL. Effects of increased pulse pressure on cerebral arterioles. Hypertension. 1996; 27:159–67. https://doi.org/10.1161/01.hyp.27.2.159 [PubMed]
- 33. Mitchell GF. Effects of central arterial aging on the structure and function of the peripheral vasculature: implications for end-organ damage. J Appl Physiol (1985). 2008; 105:1652–60. https://doi.org/10.1152/japplphysiol.90549.2008 [PubMed]
- 34. Mitchell GF, van Buchem MA, Sigurdsson S, Gotal JD, Jonsdottir MK, Kjartansson Ó, Garcia M, Aspelund T, Harris TB, Gudnason V, Launer LJ. Arterial stiffness, pressure and flow pulsatility and brain structure and function: the Age, Gene/Environment Susceptibility–Reykjavik study. Brain. 2011; 134:3398–407. https://doi.org/10.1093/brain/awr253 [PubMed]
- 35. Weller RO, Boche D, Nicoll JA. Microvasculature changes and cerebral amyloid angiopathy in Alzheimer’s disease and their potential impact on therapy. Acta Neuropathol. 2009; 118:87–102. https://doi.org/10.1007/s00401-009-0498-z [PubMed]
- 36. Weller RO, Subash M, Preston SD, Mazanti I, Carare RO. Perivascular drainage of amyloid-beta peptides from the brain and its failure in cerebral amyloid angiopathy and Alzheimer’s disease. Brain Pathol. 2008; 18:253–66. https://doi.org/10.1111/j.1750-3639.2008.00133.x [PubMed]
- 37. Saito S, Ihara M. Interaction between cerebrovascular disease and Alzheimer pathology. Curr Opin Psychiatry. 2016; 29:168–73. https://doi.org/10.1097/YCO.0000000000000239 [PubMed]
- 38. Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011; 12:723–38. https://doi.org/10.1038/nrn3114 [PubMed]
- 39. Akalu Y, Belsti Y. Hypertension and its associated factors among type 2 diabetes mellitus patients at debre tabor general hospital, northwest Ethiopia. Diabetes Metab Syndr Obes. 2020; 13:1621–31. https://doi.org/10.2147/DMSO.S254537 [PubMed]
- 40. Chau AC, Cheung EY, Chan KH, Chow WS, Shea YF, Chiu PK, Mak HK. Impaired cerebral blood flow in type 2 diabetes mellitus - a comparative study with subjective cognitive decline, vascular dementia and Alzheimer’s disease subjects. Neuroimage Clin. 2020; 27:102302. https://doi.org/10.1016/j.nicl.2020.102302 [PubMed]
- 41. Weiner MW, Veitch DP, Aisen PS, Beckett LA, Cairns NJ, Green RC, Harvey D, Jack CR, Jagust W, Liu E, Morris JC, Petersen RC, Saykin AJ, et al, and Alzheimer’s Disease Neuroimaging Initiative. The Alzheimer’s Disease Neuroimaging Initiative: a review of papers published since its inception. Alzheimers Dement. 2012; 8:S1–68. https://doi.org/10.1016/j.jalz.2011.09.172 [PubMed]
- 42. Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, et al, and Task Force Members. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013; 31:1281–357. https://doi.org/10.1097/01.hjh.0000431740.32696.cc [PubMed]
- 43. Gottesman RF, Schneider AL, Zhou Y, Coresh J, Green E, Gupta N, Knopman DS, Mintz A, Rahmim A, Sharrett AR, Wagenknecht LE, Wong DF, Mosley TH. Association between midlife vascular risk factors and estimated brain amyloid deposition. JAMA. 2017; 317:1443–50. https://doi.org/10.1001/jama.2017.3090 [PubMed]
- 44. Shaw LM, Vanderstichele H, Knapik-Czajka M, Clark CM, Aisen PS, Petersen RC, Blennow K, Soares H, Simon A, Lewczuk P, Dean R, Siemers E, Potter W, et al, and Alzheimer’s Disease Neuroimaging Initiative. Cerebrospinal fluid biomarker signature in Alzheimer’s Disease Neuroimaging Initiative subjects. Ann Neurol. 2009; 65:403–13. https://doi.org/10.1002/ana.21610 [PubMed]
- 45. Joshi A, Koeppe RA, Fessler JA. Reducing between scanner differences in multi-center PET studies. Neuroimage. 2009; 46:154–59. https://doi.org/10.1016/j.neuroimage.2009.01.057 [PubMed]
- 46. Jack CR
Jr , Bernstein MA, Fox NC, Thompson P, Alexander G, Harvey D, Borowski B, Britson PJ, Whitwell JL, Ward C, Dale AM, Felmlee JP, Gunter JL, et al. The Alzheimer’s Disease Neuroimaging Initiative (ADNI): MRI methods. J Magn Reson Imaging. 2008; 27:685–91. https://doi.org/10.1002/jmri.21049 [PubMed] - 47. Weiner MW, Aisen PS, Jack CR
Jr , Jagust WJ, Trojanowski JQ, Shaw L, Saykin AJ, Morris JC, Cairns N, Beckett LA, Toga A, Green R, Walter S, et al, and Alzheimer’s Disease Neuroimaging Initiative. The Alzheimer’s disease neuroimaging initiative: progress report and future plans. Alzheimers Dement. 2010; 6:202–11.e7. https://doi.org/10.1016/j.jalz.2010.03.007 [PubMed] - 48. Wyman BT, Harvey DJ, Crawford K, Bernstein MA, Carmichael O, Cole PE, Crane PK, DeCarli C, Fox NC, Gunter JL, Hill D, Killiany RJ, Pachai C, et al, and Alzheimer’s Disease Neuroimaging Initiative. Standardization of analysis sets for reporting results from ADNI MRI data. Alzheimers Dement. 2013; 9:332–37. https://doi.org/10.1016/j.jalz.2012.06.004 [PubMed]
- 49. Moran C, Beare R, Phan TG, Bruce DG, Callisaya ML, Srikanth V, and Alzheimer’s Disease Neuroimaging Initiative (ADNI). Type 2 diabetes mellitus and biomarkers of neurodegeneration. Neurology. 2015; 85:1123–30. https://doi.org/10.1212/WNL.0000000000001982 [PubMed]
- 50. Gibbons LE, Carle AC, Mackin RS, Harvey D, Mukherjee S, Insel P, Curtis SM, Mungas D, Crane PK, and Alzheimer’s Disease Neuroimaging Initiative. A composite score for executive functioning, validated in Alzheimer’s Disease Neuroimaging Initiative (ADNI) participants with baseline mild cognitive impairment. Brain Imaging Behav. 2012; 6:517–27. https://doi.org/10.1007/s11682-012-9176-1 [PubMed]
- 51. Crane PK, Carle A, Gibbons LE, Insel P, Mackin RS, Gross A, Jones RN, Mukherjee S, Curtis SM, Harvey D, Weiner M, Mungas D, and Alzheimer’s Disease Neuroimaging Initiative. Development and assessment of a composite score for memory in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Brain Imaging Behav. 2012; 6:502–16. https://doi.org/10.1007/s11682-012-9186-z [PubMed]
- 52. Hohman TJ, Bell SP, Jefferson AL, and Alzheimer’s Disease Neuroimaging Initiative. The role of vascular endothelial growth factor in neurodegeneration and cognitive decline: exploring interactions with biomarkers of Alzheimer disease. JAMA Neurol. 2015; 72:520–29. https://doi.org/10.1001/jamaneurol.2014.4761 [PubMed]
- 53. Caroli A, Prestia A, Galluzzi S, Ferrari C, van der Flier WM, Ossenkoppele R, Van Berckel B, Barkhof F, Teunissen C, Wall AE, Carter SF, Schöll M, Choo IH, et al, and Alzheimer’s Disease Neuroimaging Initiative. Mild cognitive impairment with suspected nonamyloid pathology (SNAP): prediction of progression. Neurology. 2015; 84:508–15. https://doi.org/10.1212/WNL.0000000000001209 [PubMed]
- 54. Jack CR
Jr , Shiung MM, Gunter JL, O’Brien PC, Weigand SD, Knopman DS, Boeve BF, Ivnik RJ, Smith GE, Cha RH, Tangalos EG, Petersen RC. Comparison of different MRI brain atrophy rate measures with clinical disease progression in AD. Neurology. 2004; 62:591–600. https://doi.org/10.1212/01.wnl.0000110315.26026.ef [PubMed] - 55. Morris JC. The clinical dementia rating (CDR): current version and scoring rules. Neurology. 1993; 43:2412–14. https://doi.org/10.1212/wnl.43.11.2412-a [PubMed]
- 56. Wakabayashi I. Associations of blood lipid-related indices with blood pressure and pulse pressure in middle-aged men. Metab Syndr Relat Disord. 2015; 13:22–28. https://doi.org/10.1089/met.2014.0093 [PubMed]