



Introduction
Multiple sclerosis (MS) is an inflammatory disease affecting the central nervous system (CNS) of more than 2 million people worldwide [1]. Its symptoms vary from physical to mental such as visual problems, depression, anxiety and fatigue [2].
Although detailed pathological mechanisms still remain unclear, the key factor is considered to be dysfunction of the immune system associated with CNS inflammation and demyelination which ultimately leads to axonal damage and destruction of the neural network [3]. Recent studies have revealed the possible interference of inflammation related molecules and cytokines such as interleukin (IL)-1β, IL-6, IL-8, and tumor necrosis factor (TNF) in the induction of demyelination [4–6].
The major challenge of diagnosing MS is that clinical symptoms and results of imaging examinations vary substantially between patients [7].
As mentioned above, because neural inflammation is the key factor for developing MS, proinflammation and anti-inflammation cytokines in the cerebrospinal fluid (CSF) may be associated with the disease and may be useful as biomarkers to diagnose MS. In fact, recent studies reported the elevation of proinflammatory molecules in MS patients [4–6, 8].
On the other hand, nesfatin-1 is an 82-amino-acid peptide derived from NEFA/nucleobindin2 (NUCB2) which is expressed in both the peripheral and CNS [9]. NUCB2/nesfatin-1 was originally identified as an endogenous anorexigenic peptide but recent studies have indicated various additional functions aside from feeding regulation [9–16]. Among such newly discovered functions of NUCB2/nesfatin-1, some studies indicated possible involvement in anti-inflammation mechanism [17–19].
In this study, we collected the CSF from MS patients and examined the level of NUCB2/nesfatin-1 together with proinflammatory and anti-inflammatory cytokines. Our present results may indicate the potentials of NUCB2/nesfatin-1 as a biomarker for diagnosing MS. Also, the results of inflammation related cytokine levels provide insight into the pathological mechanism and the involvement of inflammation in developing MS.
Results
NUCB2/nesfatin-1 levels of CSF from MS patients
The mean ages were 43.2 + 1.8 for the MS patients and 36.5 + 5.1 for the control subjects.
As shown in Figure 1 (above), expression of NUCB2/nesfatin-1 was confirmed in western blot analysis. The levels of NUCB2/nesfatin-1 were 38.2 and 138.3 pg/ml in the control subjects and MS patients, respectively.
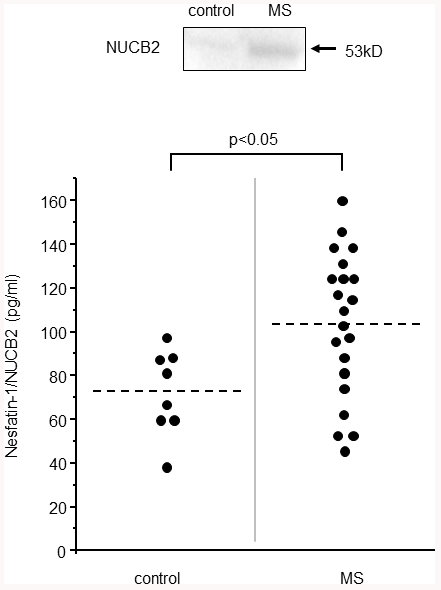
Figure 1. NUCB2/nesfatin-1 in the CSF of the MS patients. The expression of NUCB2/nesfatin-1 in the CSF of MS patient confirmed by western blot analysis (above). The NUCB2/nesfatin-1 levels in the control (n=10) and MS patients (n=24).
Analysis of the CSF showed significantly higher levels of NUCB2/nesfatin-1 in the MS patients (Figure 1; p=0.02) than in the control subjects. Serum and CSF levels of NUCB2/nesfatin-1 had no significant correlations (r = -0.6, P = 0.09).
When comparing the levels of NUCB2/nesfatin-1 in control subjects, patients with primary progressive MS and relapsing remitting MS, average NUCB2/nesfatin-1 level was significantly higher in CSF of relapsing remitting MS patients (Figure 2). There were no differences in levels of NUCB2/nesfatin-1 among each phenotypes of MS (Clinically isolated syndrome, relapsing-remitting MS, Primary progressive MS, Secondary progressive MS).
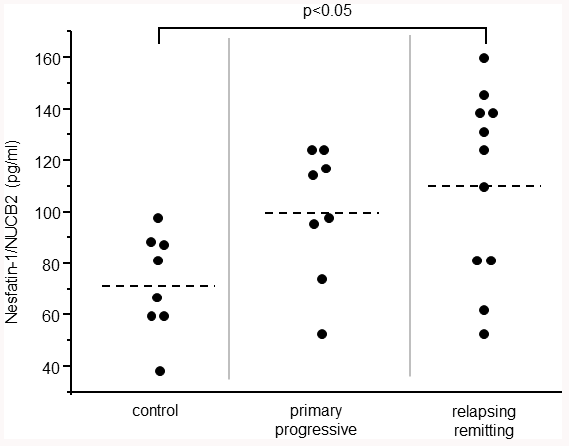
Figure 2. NUCB2/nesfatin-1 in the CSF of the control subjects, patients with primary progressive MS and relapsing remitting MS.
There were 2 subjects under steroid pulse treatment when CSFs were collected (which were excluded from results shown in Figures 1, 2). These two subjects showed low levels of NUCB2/nesfatin-1 that were undetectable by the assay kit we have used in this study.
Levels of proinflammatory cytokines in CSF of MS patients
We have measured the levels of IL-1β and TNFα as proinflammatory cytokines in the CSF. TNFα levels were not significantly different between the MS patients and control subjects (Figure 3 above right). However, to our surprise, IL-1β level of the CSF from the MS patients was significantly lower than that of the control subjects (Figure 3 above left).
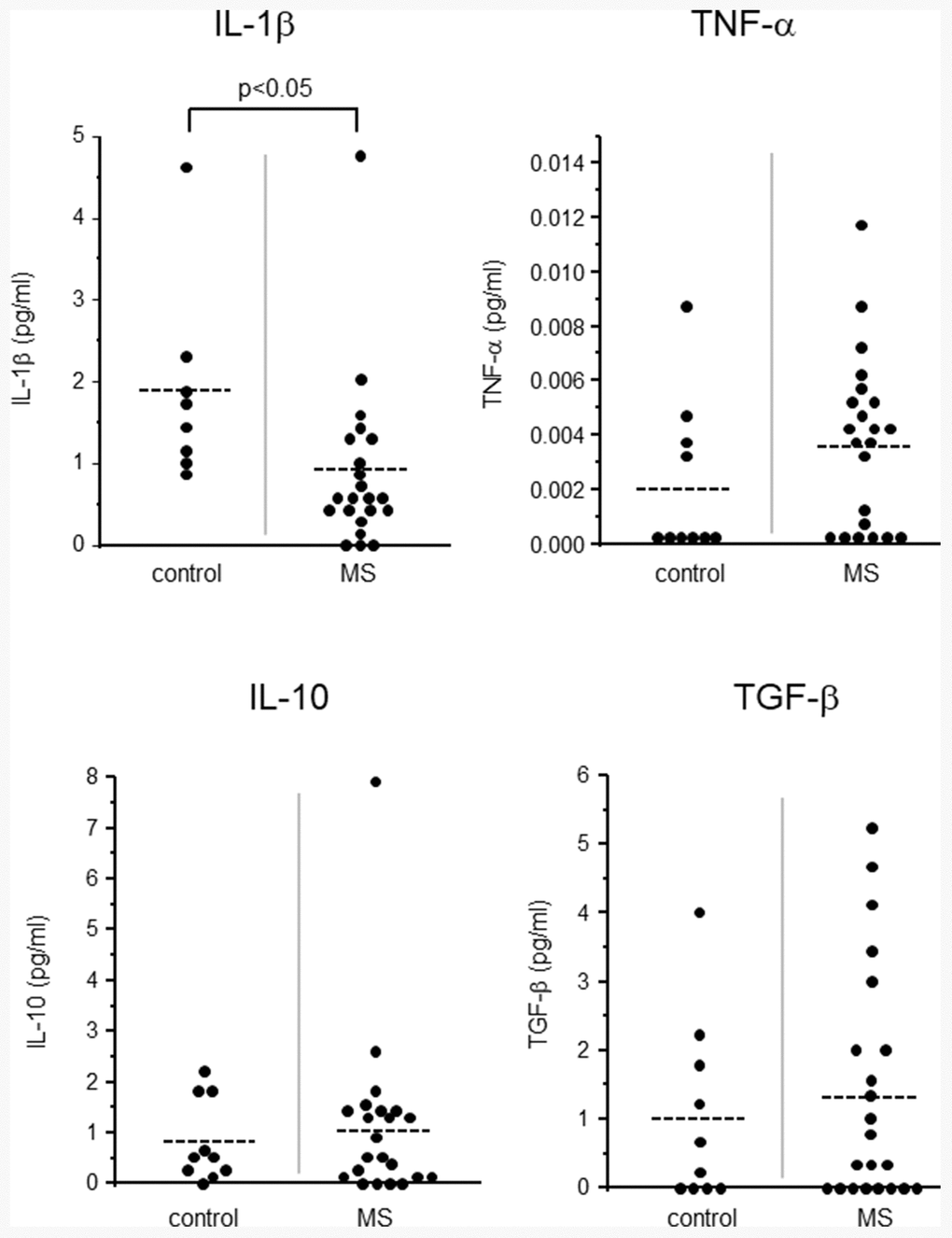
Figure 3. Levels of proinflammatory cytokines (IL-1β, TNF-α; above) and anti-inflammatory cytokines (IL-10, TGF-β; below).
Levels of anti-inflammatory cytokines in CSF of MS patients
We also measured the levels of IL-10 and TGF-β as anti-inflammatory cytokines in the CSF. Both IL-10 and TGF-β had no significant difference between the MS patients and control subjects (Figure. 3 below).
Discussion
In this study, we have shown increased NUCB2/nesfatin-1 level in the CSF of MS patients. Although the number of subjects is relatively small, to the best of our knowledge, this is the first study to evaluate NUCB2/nesfatin-1 levels in the CSF of human patients with neuroinflammatory disease.
It is considered that some form of immunological reaction may initiate neuroinflammation that ultimately leads to demyelination and neurodegeneration in the CNS [2, 20, 21]. Recently, many studies have been performed to evaluate the interference of inflammatory factors in the CSF of MS patients [4–6]. In these studies, proinflammatory conditions of the CSF were shown to be a critical factor that induces and maintains the disease. Proinflammatory cytokines such as IL-6 and IL-8 are reported to be related to long-term disease activity and progression of symptoms of MS [5]. It is thus obvious that existence of inflammation and inflammatory cytokines in the CSF are the key factors to understand the mechanism of developing MS.
NUCB2/nesfatin-1, which was originally discovered as an anorexigenic peptide is now considered to have various functions in both the CNS and peripheral tissues [9–16]. These new functions include regulations of blood pressure, glucose homeostasis and even cardiac performance [11–16]. In addition, regulation of inflammation by NUCB2/nesfatin-1 has been reported. Naseroleslami et al. reported that in cardiomyocytes NUCB2/nesfatin-1 attenuates myocardial infarction by reducing proinflammatory cytokines [17]. Also, Jiang et al. showed that NUCB2/nesfatin-1 can ameliorate osteoarthritis by suppressing inflammation [19]. These reports indicate the ability of NUCB2/nesfatin-1 to suppress inflammation. In the present study, we found that NUCB2/nesfatin-1 level in the CSF is increased in MS patients. The results showing NUCB2/nesfatin-1 level in the CSF of patients under steroid pulse treatment was undetectably low in assay kit we have used in this study, further support the involvement of NUCB2/nesfatin-1 on inflammation. Because exogenously applied NUCB2/nesfatin-1 is reported to suppress inflammation of post traumatic brain injury [22], increase of NUCB2/nesfatin-1 which was found in this study is likely to reflect the anti-inflammatory response rather than result of neuroinflammation itself. Further study is required to elucidate the detailed mechanism for the elevation of NUCB2/nesfatin-1 level in the CSF of MS patients.
To our surprise, a proinflammatory cytokine, IL-1β, was found to be significantly reduced in the CSF of MS patients. Because of ongoing inflammation in MS patients, the reduction of proinflammatory cytokine IL-1β was unexpected. In the past, Rossi et al. reported the detection of IL-1β in the CSF of MS patients only in the remission phase [4]. The present study analyzed CSF samples from both primary and remitted MS patients but IL-1β level was clearly and significantly reduced in both patients. This may be explained by the elevation of NUCB2/nesfatin-1 level in the CSF. Jiang et al. reported that NUCB2/nesfatin-1 can suppress IL-1β induced inflammation [19]. Therefore NUCB2/nesfatin-1 and IL-1β levels may have some functional connection in the CSF of MS patients. Further study is required.
Up to present, diagnosis of MS is based on symptoms and brain images obtained from MRI. In addition, oligoclonal bands of IgG on electrophoresis of the CSF are an effective marker for its diagnosis [7]. There are reports of other possible CSF biomarkers to diagnose MS but discovery of a promising new biomarker is expected. As a limitation of this study, the number of participants of this study is small and further large scale investigation is required. However, our present data show for the first time that level of NUCB2/nesfatin-1 in CSF may have a potential to be an effective biomarker for diagnosis of MS.
Materials and Methods
MS patient samples
CSF samples were collected from 24 MS patients (7 male and 17 female) admitted to the Department of Neurology in Matsumura General Hospital. As control, 10 CSF samples were collected from patients affected by non-inflammatory neurological diseases (patients with strong headache or conversion disorder: 4 males and 6 females). The study was approved by the ethics committee of Fukushima Medical University, School of Medicine and Matsumura General Hospital, according to the Declaration of Helsinki. All patients were provided written informed consent to this study. MS diagnosis was made according to 2017 McDonald Criteria for Diagnosis of Multiple Sclerosis, which is based on the combinations of clinical presentation and additional data (Table 1) [7].
Table 1. Diagnostic criteria for MS.
| Clinical presentation | Additional data needed for diagnosis |
| ≥2 clinical attacks and objective evidence of 1 lesion | Disseminated in space (DIS): an additional attack implicating a different CNS site OR by MRI (≥ new lesions on follow-up imaging both gadolinium-enhancing and non-enhancing lesions on single MRI.) |
| 1 clinical attack and objective clinical evidence of ≥ 2 lesions | Disseminated in time (DIT): an additional clinical attack implicating a different CNS site OR by MRI (≥1symptomatic or asymptomatic lesion in ≥2 areas including cortical/juxtacortical, periventricular, infratentorial, or spinal.) OR CSF-specific oligoclonal bands |
| 1 clinical attack and objective evidence of 1 lesion | DIS:an additional clinical attack implicating a different CNS site OR by MRI (≥ new lesions on follow-up imaging both gadolinium-enhancing and non-enhancing lesions on single MRI.) OR DIT:an additional clinical attack OR by MRI (≥1symptomatic or asymptomatic lesion in ≥2areas including cortical/juxtacortical, periventricular, infratentorial, or spinal.) OR CSF-specific oligoclonal bands |
Western blot analysis
Twenty μl of CSF samples dissolved in 2 X SDS sample buffer was loaded onto a 10% polyacrylamide gel (156103, Bio-Rad, CA, USA). The samples were separated at 20 mA. Proteins were transferred from the gel onto a PVDF membrane at 118 mA for 60 min with transfer buffer. The membrane was washed several times with PBS containing 0.05% of Tween-20 (PBST) and blocked with 5% skim milk in PBST for 60 min at room temperature. Then the membrane was incubated with a rabbit polyclonal NUCB2 antibody (1:1000, N9414, Sigma-Aldrich, MO, USA) for overnight at 4° C. The antibody was diluted in blocking solution. The membrane was washed with PBST and incubated with HRP-conjugated secondary antibodies against rabbit IgG (1:1000, Vector Laboratories, CA, USA) for 60 min at room temperature. Then the membrane was washed several times and peroxidase activity was detected.
ELISA assay
Levels of NUCB2/nesfatin-1 (Abcam, Cambridge, UK), IL-1β, TNFα, IL-10 and TGF-β (Biolegend, San Diego, CA, USA) in CSF and serum were measured by commercially available ELISA assay kit.
Statistical analysis
All data are presented as mean. Statistical analysis was made by student’s t-test and one-way ANOVA followed by Tukey test for Figure 2. P<0.05 was considered significant.
Author Contributions
MS, TM, MK, KM diagnosed the patients and provided samples. MS, KS and YM performed assay and analysis. KS and YM supervised overall experiments, KK provided critical comments. MS, KK, KS and YM wrote the text.
Acknowledgments
The authors thank Ms Rie Ohashi of Fukushima Medical University for her technical support.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1. GBD 2016 Multiple Sclerosis Collaborators. Global, regional, and national burden of multiple sclerosis 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019; 18:269–85. https://doi.org/10.1016/S1474-4422(18)30443-5 [PubMed]
- 2. Compston A, Coles A. Multiple sclerosis. Lancet. 2008; 372:1502–17. https://doi.org/10.1016/S0140-6736(08)61620-7 [PubMed]
- 3. Nakahara J, Maeda M, Aiso S, Suzuki N. Current concepts in multiple sclerosis: autoimmunity versus oligodendrogliopathy. Clin Rev Allergy Immunol. 2012; 42:26–34. https://doi.org/10.1007/s12016-011-8287-6 [PubMed]
- 4. Rossi S, Studer V, Motta C, Germani G, Macchiarulo G, Buttari F, Mancino R, Castelli M, De Chiara V, Weiss S, Martino G, Furlan R, Centonze D. Cerebrospinal fluid detection of interleukin-1β in phase of remission predicts disease progression in multiple sclerosis. J Neuroinflammation. 2014; 11:32. https://doi.org/10.1186/1742-2094-11-32 [PubMed]
- 5. Stampanoni Bassi M, Iezzi E, Landi D, Monteleone F, Gilio L, Simonelli I, Musella A, Mandolesi G, De Vito F, Furlan R, Finardi A, Marfia GA, Centonze D, Buttari F. Delayed treatment of MS is associated with high CSF levels of IL-6 and IL-8 and worse future disease course. J Neurol. 2018; 265:2540–47. https://doi.org/10.1007/s00415-018-8994-5 [PubMed]
- 6. Stelmasiak Z, Kozioł-Montewka M, Dobosz B, Rejdak K, Bartosik-Psujek H, Mitosek-Szewczyk K, Belniak-Legieć E. Interleukin-6 concentration in serum and cerebrospinal fluid in multiple sclerosis patients. Med Sci Monit. 2000; 6:1104–08. [PubMed]
- 7. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, Correale J, Fazekas F, Filippi M, Freedman MS, Fujihara K, Galetta SL, Hartung HP, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018; 17:162–73. https://doi.org/10.1016/S1474-4422(17)30470-2 [PubMed]
- 8. Kimura A, Takemura M, Saito K, Serrero G, Yoshikura N, Hayashi Y, Inuzuka T. Increased cerebrospinal fluid progranulin correlates with interleukin-6 in the acute phase of neuromyelitis optica spectrum disorder. J Neuroimmunol. 2017; 305:175–81. https://doi.org/10.1016/j.jneuroim.2017.01.006 [PubMed]
- 9. Oh-I S, Shimizu H, Satoh T, Okada S, Adachi S, Inoue K, Eguchi H, Yamamoto M, Imaki T, Hashimoto K, Tsuchiya T, Monden T, Horiguchi K, et al. Identification of nesfatin-1 as a satiety molecule in the hypothalamus. Nature. 2006; 443:709–12. https://doi.org/10.1038/nature05162 [PubMed]
- 10. Maejima Y, Sedbazar U, Suyama S, Kohno D, Onaka T, Takano E, Yoshida N, Koike M, Uchiyama Y, Fujiwara K, Yashiro T, Horvath TL, Dietrich MO, et al. Nesfatin-1-regulated oxytocinergic signaling in the paraventricular nucleus causes anorexia through a leptin-independent melanocortin pathway. Cell Metab. 2009; 10:355–65. https://doi.org/10.1016/j.cmet.2009.09.002 [PubMed]
- 11. Yoshida N, Maejima Y, Sedbazar U, Ando A, Kurita H, Damdindorj B, Takano E, Gantulga D, Iwasaki Y, Kurashina T, Onaka T, Dezaki K, Nakata M, et al. Stressor-responsive central nesfatin-1 activates corticotropin-releasing hormone, noradrenaline and serotonin neurons and evokes hypothalamic-pituitary-adrenal axis. Aging (Albany NY). 2010; 2:775–84. https://doi.org/10.18632/aging.100207 [PubMed]
- 12. Yamawaki H, Takahashi M, Mukohda M, Morita T, Okada M, Hara Y. A novel adipocytokine, nesfatin-1 modulates peripheral arterial contractility and blood pressure in rats. Biochem Biophys Res Commun. 2012; 418:676–81. https://doi.org/10.1016/j.bbrc.2012.01.076 [PubMed]
- 13. Özsavcí D, Erşahin M, Şener A, Özakpinar ÖB, Toklu HZ, Akakín D, Şener G, Yeğen BÇ. The novel function of nesfatin-1 as an anti-inflammatory and antiapoptotic peptide in subarachnoid hemorrhage-induced oxidative brain damage in rats. Neurosurgery. 2011; 68:1699–708. https://doi.org/10.1227/NEU.0b013e318210f258 [PubMed]
- 14. Aydin S. Multi-functional peptide hormone NUCB2/nesfatin-1. Endocrine. 2013; 44:312–25. https://doi.org/10.1007/s12020-013-9923-0 [PubMed]
- 15. Angelone T, Filice E, Pasqua T, Amodio N, Galluccio M, Montesanti G, Quintieri AM, Cerra MC. Nesfatin-1 as a novel cardiac peptide: identification, functional characterization, and protection against ischemia/reperfusion injury. Cell Mol Life Sci. 2013; 70:495–509. https://doi.org/10.1007/s00018-012-1138-7 [PubMed]
- 16. Maejima Y, Horita S, Kobayashi D, Aoki M, O’hashi R, Imai R, Sakamoto K, Mori M, Takasu K, Ogawa K, Takenoshita S, Zhao S, Hazama A, Shimomura K. Nesfatin-1 inhibits voltage gated K+ channels in pancreatic beta cells. Peptides. 2017; 95:10–15. https://doi.org/10.1016/j.peptides.2017.07.001 [PubMed]
- 17. Naseroleslami M, Sharifi M, Rakhshan K, Mokhtari B, Aboutaleb N. Nesfatin-1 attenuates injury in a rat model of myocardial infarction by targeting autophagy, inflammation, and apoptosis. Arch Physiol Biochem. 2020; 1. https://doi.org/10.1080/13813455.2020.1802486 [PubMed]
- 18. Wang ZZ, Chen SC, Zou XB, Tian LL, Sui SH, Liu NZ. Nesfatin-1 alleviates acute lung injury through reducing inflammation and oxidative stress via the regulation of HMGB1. Eur Rev Med Pharmacol Sci. 2020; 24:5071–81. https://doi.org/10.26355/eurrev_202005_21200 [PubMed]
- 19. Jiang L, Xu K, Li J, Zhou X, Xu L, Wu Z, Ma C, Ran J, Hu P, Bao J, Wu L, Xiong Y. Nesfatin-1 suppresses interleukin-1β-induced inflammation, apoptosis, and cartilage matrix destruction in chondrocytes and ameliorates osteoarthritis in rats. Aging (Albany NY). 2020; 12:1760–77. https://doi.org/10.18632/aging.102711 [PubMed]
- 20. Lassmann H. Multiple sclerosis pathology. Cold Spring Harb Perspect Med. 2018; 8:a028936. https://doi.org/10.1101/cshperspect.a028936 [PubMed]
- 21. Kutzelnigg A, Lucchinetti CF, Stadelmann C, Brück W, Rauschka H, Bergmann M, Schmidbauer M, Parisi JE, Lassmann H. Cortical demyelination and diffuse white matter injury in multiple sclerosis. Brain. 2005; 128:2705–12. https://doi.org/10.1093/brain/awh641 [PubMed]
- 22. Tang CH, Fu XJ, Xu XL, Wei XJ, Pan HS. The anti-inflammatory and anti-apoptotic effects of nesfatin-1 in the traumatic rat brain. Peptides. 2012; 36:39–45. https://doi.org/10.1016/j.peptides.2012.04.014 [PubMed]