



Introduction
Bladder cancer is one of the ten most common cancers worldwide with nearly 430,000 cancer cases being diagnosed per year [1]. Despite advances in treatment (e.g., immune checkpoint inhibitor therapeutics), the prognosis remains poor for bladder cancer, especially muscle-invasive tumors [2]. Smoking is the most well-established risk factor with approximately 50% attributable risk of bladder cancer [3]. A small proportion (5-6%) of bladder cancers arise from occupational exposure [4]. Less-established risk factors for bladder cancers include diabetes [5], lack of physical activity [6], obesity [7], nulliparity [8] and high consumption of processed red meat [9].
The potential relationship between dietary tomato/lycopene intake or serum lycopene and bladder cancer risk has been evaluated by a few observational studies and meta-analyses [10–14] with relatively small sample size and inconsistent results. For example, Huang et al. [13] reported that plasma lycopene was significantly inversely associated with bladder cancer risk based on a case-control study from Memorial Sloan-Kettering Cancer Center. By contrast, a recent large meta-analysis failed to find a significant relationship between dietary intake of lycopene or serum lycopene and the incidence of bladder cancer [14]. To contribute to the limited evidence base, we investigated the association between intakes of tomato products or lycopene and the incidence of bladder cancer in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) study.
Results
There were 774 incident bladder cancer cases after a median follow-up of 12.5 years. Compared to participants who had the largest consumption of raw tomatoes (i.e., quintile 5), participants with the smallest raw tomato intake (i.e., quintile 1), had lower body mass index (BMI), consumed less total energy, and were more likely to be male, Black non-Hispanic or Hispanic, not married, and current smokers, and tended to have an education level of below-college (Table 1).
Table 1. Main characteristic of participants in the PLCO cancer screening trial by raw tomato intake.
| Variables | Q1 (n=19831) | Q2 (n=20560) | Q3 (n=20906) | Q4 (n=20904) | Q5 (n=19482) | p-value* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (y), mean ± SD | 62.2 ± 5.4 | 62.4 ± 5.3 | 62.5 ± 5.3 | 62.6 ± 5.3 | 62.4 ± 5.2 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female (n, %) | 8924 (45.0%) | 10227 (49.7%) | 11186 (53.5%) | 12215 (58.4%) | 9680 (49.7%) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 9078 (45.8%) | 9883 (48.1%) | 10233 (48.9%) | 10278 (49.2%) | 9072 (46.6%) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 2294 (11.6%) | 2000 (9.7%) | 1736 (8.3%) | 1710 (8.2%) | 1650 (8.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former | 8458 (42.7%) | 8674 (42.2%) | 8931 (42.7%) | 8916 (42.7%) | 8757 (44.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 1 (0.0%) | 3 (0.0%) | 6 (0.0%) | 0 (0.0%) | 3 (0.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤High school | 9013 (45.4%) | 8891 (43.2%) | 8455 (40.4%) | 8646 (41.4%) | 7902 (40.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥Some college | 10778 (54.3%) | 11618 (56.5%) | 12410 (59.4%) | 12224 (58.5%) | 11550 (59.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 40 (0.2%) | 51 (0.2%) | 41 (0.2%) | 34 (0.2%) | 30 (0.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <25.0 kg/m2 | 6599 (33.3%) | 6868 (33.4%) | 7049 (33.7%) | 7099 (34.0%) | 6117 (31.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥25.0 kg/m2 | 12946 (65.3%) | 13409 (65.2%) | 13616 (65.1%) | 13545 (64.8%) | 13101 (67.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 286 (1.4%) | 283 (1.4%) | 241 (1.2%) | 260 (1.2%) | 264 (1.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White, Non-Hispanic | 16977 (85.6%) | 18600 (90.5%) | 19402 (92.8%) | 19454 (93.1%) | 18036 (92.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 2844 (14.3%) | 1953 (9.5%) | 1500 (7.2%) | 1443 (6.9%) | 1437 (7.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 10 (0.1%) | 7 (0.0%) | 4 (0.0%) | 7 (0.0%) | 9 (0.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Drinking (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never | 1928 (9.7%) | 2039 (9.9%) | 2024 (9.7%) | 2141 (10.2%) | 1981 (10.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former | 3380 (17.0%) | 3066 (14.9%) | 2750 (13.2%) | 2872 (13.7%) | 2678 (13.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 13882 (70.0%) | 14888 (72.4%) | 15601 (74.6%) | 15289 (73.1%) | 14285 (73.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 641 (3.2%) | 567 (2.8%) | 531 (2.5%) | 602 (2.9%) | 538 (2.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total energy intake (kcal/d), mean ± SD | 1551.2 ± 712.3 | 1632.8 ± 688.4 | 1716.1 ± 685.9 | 1785.1 ± 707.6 | 2015.2 ± 802.5 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Marital status (n, %) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 14522 (73.2%) | 15972 (77.7%) | 16738 (80.1%) | 16831 (80.5%) | 15524 (79.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not married | 5272 (26.6%) | 4539 (22.1%) | 4128 (19.7%) | 4040 (19.3%) | 3931 (20.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Missing | 37 (0.2%) | 49 (0.2%) | 40 (0.2%) | 33 (0.2%) | 27 (0.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PLCO, Prostate, Lung, Colorectal, and Ovarian Cancer; Q, quintile; y, year; SD, Standard deviation; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *The p-values were calculated from the comparison of all the 5 groups. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the multivariate analysis model, there was no statistically significant association between consumption of raw tomatoes and bladder cancer incidence (Table 2, HRQ5 VS Q1 = 1.20, 95% CI: 0.95-1.52; P for trend = 0.243). The corresponding adjusted HR was 1.06 (95% CI 0.99-1.13) per 1 SD increment of raw tomato intake. Likewise, dietary intakes of tomato catsup, tomato salsa and tomato juice were not associated with the risk of bladder cancer in the multivariate analysis (all P for trend > 0.05). This is also true for the association between dietary consumption of lycopene and bladder cancer risk (Adjusted model: HRQ5 vs. Q1 = 1.04, 95% CI 0.82-1.33; P for trend = 0.590). These associations were not modified by potential confounders, including age, sex, race, education level, drinking habits, smoking status and BMI (all P for interaction > 0.05).
Table 2. Association between tomato/lycopene intake and bladder cancer risk in the PLCO cancer screening trial.
| Variables | Median (g/day) | Cohort (n) | Cases (n) | Crude HR (95% CI), p-value | Adjusted HR (95% CI)*, p-value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Raw tomato (g/day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (≤ 3.57) | 1.63 | 19831 | 143 | Reference | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (≥ 3.60 to ≤ 9.41) | 6.33 | 20560 | 165 | 1.10 (0.88-1.38), p=0.401 | 1.17 (0.93-1.46), p=0.176 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (≥ 9.44 to ≤ 17.56) | 12.91 | 20906 | 156 | 1.02 (0.81-1.28), p=0.880 | 1.14 (0.91-1.43), p=0.267 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (≥ 17.67 to ≤ 32.44) | 23.79 | 20904 | 153 | 1.00 (0.79-1.25), p=0.973 | 1.19 (0.94-1.50), p=0.151 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q5 (≥ 32.64) | 50.24 | 19482 | 157 | 1.11 (0.88-1.39), p=0.381 | 1.20 (0.95-1.52), p=0.118 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| p for trend = 0.571 | p for trend = 0.243 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Per 1 SD increment | 1.02 (0.95-1.09), p=0.551 | 1.06 (0.99-1.13), p=0.122 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tomato catsup (g/day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (≤ 0.11) | 0 | 21591 | 154 | Reference | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (≥ 0.13 to ≤ 0.44) | 0.17 | 19540 | 110 | 0.79 (0.62-1.01), p=0.058 | 0.90 (0.70-1.15), p=0.383 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (≥ 0.48 to ≤ 1.15) | 0.58 | 21219 | 132 | 0.87 (0.69-1.10), p=0.240 | 0.91 (0.72-1.15), p=0.443 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (≥ 1.20 to ≤ 2.53) | 1.99 | 19460 | 198 | 1.42 (1.15-1.75), p=0.001 | 0.95 (0.76-1.18), p=0.629 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q5 (≥ 2.95) | 5.06 | 19873 | 180 | 1.28 (1.03-1.58), p=0.026 | 0.96 (0.77-1.20), p=0.712 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| p for trend < 0.001 | p for trend = 0.887 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Per 1 SD increment | 1.09 (1.05-1.14), p<0.001 | 1.05 (0.99-1.11), p=0.088 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tomato salsa (g/day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (= 0) | 0 | 26673 | 231 | Reference | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (≥ 0.10 to ≤ 0.38) | 0.38 | 19279 | 114 | 0.68 (0.54-0.85), p=0.001 | 1.20 (0.95-1.51), p=0.129 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (≥ 0.39 to ≤ 1.13) | 1.10 | 18951 | 164 | 0.98 (0.80-1.20), p=0.853 | 0.87 (0.71-1.06), p=0.172 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (≥ 1.23 to ≤ 2.99) | 1.43 | 19494 | 148 | 0.87 (0.71-1.07), p=0.179 | 1.06 (0.85-1.31), p=0.616 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q5 (≥ 3.52) | 9.33 | 17286 | 117 | 0.78 (0.62-0.97), p=0.029 | 0.96 (0.76-1.21), p=0.713 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| p for trend = 0.181 | p for trend = 0.593 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Per 1 SD increment | 0.98 (0.91-1.06), p=0.612 | 1.01 (0.94-1.08), p=0.824 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tomato juice (g/day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (= 0) | 0 | 28524 | 205 | Reference | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (≥ 5.07 to ≤ 5.15) | 5.07 | 17642 | 122 | 0.95 (0.76-1.19), p=0.644 | 0.97 (0.77-1.21), p=0.784 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (≥ 8.12 to ≤ 8.28) | 8.28 | 23990 | 189 | 1.08 (0.89-1.32), p=0.434 | 1.07 (0.87-1.30), p=0.520 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (≥ 11.36 to ≤ 18.19) | 13.38 | 12698 | 123 | 1.33 (1.06-1.66), p=0.013 | 0.94 (0.75-1.18), p=0.596 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q5 (≥ 18.54) | 52.27 | 18829 | 135 | 1.00 (0.80-1.24), p=0.968 | 1.04 (0.83-1.29), p=0.759 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| p for trend = 0.891 | p for trend = 0.773 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Per 1 SD increment | 1.03 (0.97-1.09), p=0.376 | 0.99 (0.92-1.07), p=0.818 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lycopene (mcg/day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (≤ 2791.29) | 2074.73 | 20337 | 147 | Reference | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (≥ 2791.35 to ≤ 4059.34) | 3416.12 | 20337 | 157 | 1.05 (0.84-1.32), p=0.660 | 1.02 (0.81-1.28), p=0.869 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (≥ 4059.38 to ≤ 5611.78) | 4756.86 | 20336 | 137 | 0.92 (0.73-1.16), p=0.475 | 0.88 (0.70-1.12), p=0.309 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (≥ 5611.82 to ≤ 8436.94) | 6736.32 | 20337 | 153 | 1.03 (0.82-1.29), p=0.810 | 0.95 (0.75-1.21), p=0.671 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q5 (≥ 8437.60) | 12062.24 | 20336 | 180 | 1.22 (0.98-1.52), p=0.070 | 1.04 (0.82-1.33), p=0.748 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| p for trend = 0.035 | p for trend = 0.590 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Per 1 SD increment | 1.06 (1.00-1.11), p=0.036 | 1.02 (0.96-1.09), p=0.469 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PLCO, Prostate, Lung, Colorectal, and Ovarian Cancer; HR, hazard ratio; CI, confidence interval; Q, quintile; SD, Standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Adjusted for age, sex, race, body mass index, education, smoking status, drinking status, total energy intake, randomization arm, family history of any cancer and marital status. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In sensitivity analysis, there was little change in the findings after excluding cases who were diagnosed within the first two years of follow-up (all P for trend > 0.05). We also performed another sensitivity analysis by dividing the data into two parts (high versus low intake). No significant associations were observed for any types of tomatoes or lycopene (Supplementary Table 1, all P > 0.05). There was no statistical evidence for nonlinearity according to the spline curve which is shown in Supplementary Figure 1 (P for nonlinearity > 0.05).
Discussion
In this large PLCO study, we did not observe a significant association between bladder cancer risk and dietary intakes of raw tomatoes, tomato products or lycopene after adjusting for confounders. Similar results were found after excluding cases diagnosed within the first two years of follow-up.
Several case-control studies of dietary tomato/lycopene consumption or serum lycopene (as a marker of consumption of tomatoes and tomato-based products) and the risk of bladder cancer have been published [10, 12, 13, 15] with inconsistent results. Retrospective case-control studies are at risk of selection and recall biases. Two prospective cohort studies by Michaud et al. [11] and Park et al. [16] found that dietary lycopene intake was not related to the bladder cancer incidence in the ATBC cohort study and in the Multiethnic Cohort Study, respectively.
Intake of tomato and/or lycopene has been associated with reduced risk of several cancers, such as hepatocellular carcinoma [17], gastric cancer [18] and prostate cancer [19]. It has been proposed that lycopene, found in high amounts in tomato, may contribute to cancer prevention, which could be the biological mechanisms in the lower development of cancers with higher consumption of tomato, [20]. Owing to its potent antioxidant properties, lycopene can reduce potentially harmful proinflammatory mediators and modulate the downstream cellular signaling [21]. Okajima et al. [22] reported that tomato juice, presumably containing lycopene and other anti-oxidants, inhibited the development of bladder cancer in a rat model.
The strengths of this study include the prospective design, large sample size and a high and complete follow-up rate, which substantially decreased the chance of reverse causality and selection bias. The collected data on smoking status and many other potential confounders made the adjustment as comprehensive as possible. However, several limitations should also be discussed. First, as this was an observational study, causality can only be suggested and residual or unmeasured confounding cannot be fully excluded. Second, the most participants analyzed in this study were non-Hispanic Whites, and as such our findings may not be applicable to other populations (e.g., Asians). Third, it is inevitable that errors commonly exist in nutritional exposures measured by dietary history questionnaire, which may distort the true risk estimates. Finally, participants’ information was collected at baseline only and the exposures could have changed during the long follow-up period.
In summary, analysis of the PLCO study suggested that dietary consumption of tomato or lycopene was not related to the incidence of bladder cancer. Future large prospective studies with detailed information on tomato preparation, molecular subtypes of bladder cancer and genotypes of population could provide more definitive conclusion on the potential effects of tomato or lycopene intake on risk of bladder cancer.
Materials and Methods
Subjects and study design
PLCO screening trial is a population-based clinical trial aimed to determine whether certain screening tests would reduce death from prostate, lung, colorectal, and ovarian cancer [23]. PLCO consisted of 154,897 eligible participants aged 55 to 74 years and enrolled at 10 screening centers across the United States from 1993 to 2001. The institutional review boards of the National Cancer Institute (NCI) and each of the participating centers approved the PLCO study. All eligible participants provided informed consent in the study.
Data collection and dietary assessment
The baseline questionnaire (BQ) included participants’ self-reported information on demographics (e.g., age, gender and race), medical history, and other factors. Dietary data were collected using the dietary history questionnaire (DHQ), which included the portion size and frequency of 124 individual food items and supplement use in the past year [24]. The USDA 1994 to 1996 Continuing Survey of Food Intakes by Individuals [25] were used to calibrate DHQ data and calculate the daily intake of raw tomatoes, tomato catsup, tomato salsa, tomato juice and lycopene.
Subject selection
Participants were excluded from this study if they did not return a BQ (n = 4,920); had a history of cancer at baseline (n = 6,849); had no data on follow-up time (n = 696); had died from unknown causes or had an undetermined case status (n = 78); did not complete DHQ or the DHQ was not valid (n = 40,671). Finally, this study comprised 101,683 participants in total. The detailed process of subject selection has been shown in Figure 1.
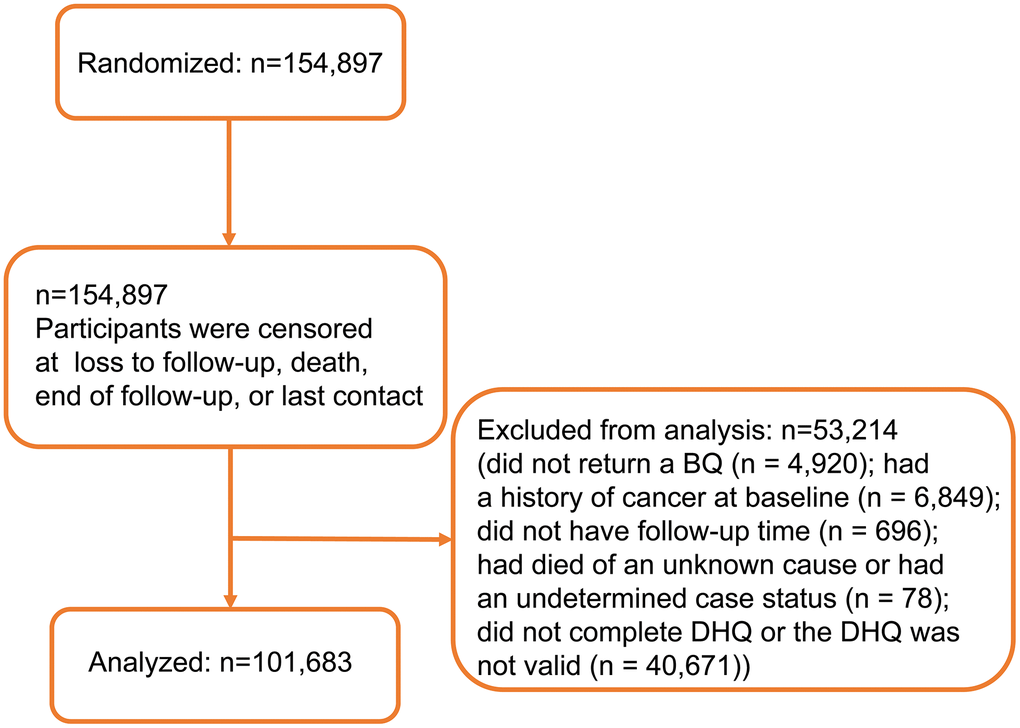
Figure 1. Flow diagram of participant inclusion.
Outcome assessment
Study participants were mailed a questionnaire each year to identify cancer cases. Diagnosis of cancer was then ascertained via medical record abstraction. Information on vital status was also supplemented by periodic linkage to the National Death Index. The primary endpoint of interest was the incidence of bladder cancer.
Statistical analysis
We used Cox proportional hazards regression to estimate HRs and 95% CIs. Participants were censored until cancer diagnosis, occurrence of death, or end of follow-up (December 31, 2009). Models were adjusted for randomization arm (intervention vs. control), age (continuous), sex, race (White, Non-Hispanic vs. Other), BMI (< 25 vs. ≥ 25 kg/m2), education (≤ high school vs. ≥ some college), smoking status (never vs. former ≤ 15 years since quit vs. former > 15 years since quit vs. former with years since quit unknown vs. current smoker ≤ 1 pack per day vs. current smoker >1 pack per day vs. current smoker with intensity unknown), drinking habits (never vs. former vs. current), total energy intake (continuous), family history of any cancer (yes vs. no), and marital status (married vs. not married). Interaction was examined using likelihood-ratio tests compared models with and without the interaction term including age, sex, race, education level, drinking habits, smoking status and BMI. The Schoenfeld residuals were used to check the proportional hazards (PH) assumption [26]. Dietary tomato/lycopene consumption was categorized into quintiles before fitting into the models. Restricted cubic spline models [27] were used to examine a potential non-linear association between tomato intake and bladder cancer incidence with three fitted knots (i.e., 10th, 50th and 90th percentiles). All statistical analyses were performed using the software STATA version 15 (Stata Corp, College Station, TX, USA). All tests were two-sided.
Author Contributions
XX and HM contributed to the conception or design of the work. XX and SL contributed to the acquisition, analysis, or interpretation of data for the work. XX and BX drafted the manuscript. SW and DX critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study was supported by grants from the Zhejiang Provincial Natural Science Foundation (LY20H160019), National Natural Science Foundation of China (81800588), and Zhejiang Provincial Medical and Health Science and Technology Plan (2018KY032). The authors thank the National Cancer Institute for access to NCI’s data collected by the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. The statements contained herein are solely those of the authors and do not represent or imply concurrence or endorsement by NCI.
References
- 1. Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol. 2017; 71:96–108. https://doi.org/10.1016/j.eururo.2016.06.010 [PubMed]
- 2. Tran L, Xiao JF, Agarwal N, Duex JE, Theodorescu D. Advances in bladder cancer biology and therapy. Nat Rev Cancer. 2021; 21:104–21. https://doi.org/10.1038/s41568-020-00313-1 [PubMed]
- 3. Cumberbatch MG, Rota M, Catto JW, La Vecchia C. The Role of Tobacco Smoke in Bladder and Kidney Carcinogenesis: A Comparison of Exposures and Meta-analysis of Incidence and Mortality Risks. Eur Urol. 2016; 70:458–66. https://doi.org/10.1016/j.eururo.2015.06.042 [PubMed]
- 4. Westhoff E, Maria de Oliveira-Neumayer J, Aben KK, Vrieling A, Kiemeney LA. Low awareness of risk factors among bladder cancer survivors: New evidence and a literature overview. Eur J Cancer. 2016; 60:136–45. https://doi.org/10.1016/j.ejca.2016.03.071 [PubMed]
- 5. Fang H, Yao B, Yan Y, Xu H, Liu Y, Tang H, Zhou J, Cao L, Wang W, Zhang J, Zhao L, Chen X, Zhang F, Zhao Y. Diabetes mellitus increases the risk of bladder cancer: an updated meta-analysis of observational studies. Diabetes Technol Ther. 2013; 15:914–22. https://doi.org/10.1089/dia.2013.0131 [PubMed]
- 6. Keimling M, Behrens G, Schmid D, Jochem C, Leitzmann MF. The association between physical activity and bladder cancer: systematic review and meta-analysis. Br J Cancer. 2014; 110:1862–70. https://doi.org/10.1038/bjc.2014.77 [PubMed]
- 7. Zhao L, Tian X, Duan X, Ye Y, Sun M, Huang J. Association of body mass index with bladder cancer risk: a dose-response meta-analysis of prospective cohort studies. Oncotarget. 2017; 8:33990–4000. https://doi.org/10.18632/oncotarget.16722 [PubMed]
- 8. Xu X, Mo Q, Shen H, Wang S, Liu B. Reproductive and hormonal factors and bladder cancer risk: a prospective study and meta-analysis. Aging (Albany NY). 2020; 12:14691–98. https://doi.org/10.18632/aging.103523 [PubMed]
- 9. Xu X. Processed Meat Intake and Bladder Cancer Risk in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cohort. Cancer Epidemiol Biomarkers Prev. 2019; 28:1993–97. https://doi.org/10.1158/1055-9965.EPI-19-0604 [PubMed]
- 10. Bruemmer B, White E, Vaughan TL, Cheney CL. Nutrient intake in relation to bladder cancer among middle-aged men and women. Am J Epidemiol. 1996; 144:485–95. https://doi.org/10.1093/oxfordjournals.aje.a008955 [PubMed]
- 11. Michaud DS, Pietinen P, Taylor PR, Virtanen M, Virtamo J, Albanes D. Intakes of fruits and vegetables, carotenoids and vitamins A, E, C in relation to the risk of bladder cancer in the ATBC cohort study. Br J Cancer. 2002; 87:960–65. https://doi.org/10.1038/sj.bjc.6600604 [PubMed]
- 12. Nomura AM, Kolonel LN, Hankin JH, Yoshizawa CN. Dietary factors in cancer of the lower urinary tract. Int J Cancer. 1991; 48:199–205. https://doi.org/10.1002/ijc.2910480208 [PubMed]
- 13. Hung RJ, Zhang ZF, Rao JY, Pantuck A, Reuter VE, Heber D, Lu QY. Protective effects of plasma carotenoids on the risk of bladder cancer. J Urol. 2006; 176:1192–97. https://doi.org/10.1016/j.juro.2006.04.030 [PubMed]
- 14. Wu S, Liu Y, Michalek JE, Mesa RA, Parma DL, Rodriguez R, Mansour AM, Svatek R, Tucker TC, Ramirez AG. Carotenoid Intake and Circulating Carotenoids Are Inversely Associated with the Risk of Bladder Cancer: A Dose-Response Meta-analysis. Adv Nutr. 2020; 11:630–43. https://doi.org/10.1093/advances/nmz120 [PubMed]
- 15. Riboli E, González CA, López-Abente G, Errezola M, Izarzugaza I, Escolar A, Nebot M, Hémon B, Agudo A. Diet and bladder cancer in Spain: a multi-centre case-control study. Int J Cancer. 1991; 49:214–19. https://doi.org/10.1002/ijc.2910490212 [PubMed]
- 16. Park SY, Ollberding NJ, Woolcott CG, Wilkens LR, Henderson BE, Kolonel LN. Fruit and vegetable intakes are associated with lower risk of bladder cancer among women in the Multiethnic Cohort Study. J Nutr. 2013; 143:1283–92. https://doi.org/10.3945/jn.113.174920 [PubMed]
- 17. Thomas CE, Luu HN, Wang R, Adams-Haduch J, Jin A, Koh WP, Yuan JM. Association between Dietary Tomato Intake and the Risk of Hepatocellular Carcinoma: The Singapore Chinese Health Study. Cancer Epidemiol Biomarkers Prev. 2020; 29:1430–35. https://doi.org/10.1158/1055-9965.EPI-20-0051 [PubMed]
- 18. Yang T, Yang X, Wang X, Wang Y, Song Z. The role of tomato products and lycopene in the prevention of gastric cancer: a meta-analysis of epidemiologic studies. Med Hypotheses. 2013; 80:383–88. https://doi.org/10.1016/j.mehy.2013.01.005 [PubMed]
- 19. Xu X, Li J, Wang X, Wang S, Meng S, Zhu Y, Liang Z, Zheng X, Xie L. Tomato consumption and prostate cancer risk: a systematic review and meta-analysis. Sci Rep. 2016; 6:37091. https://doi.org/10.1038/srep37091 [PubMed]
- 20. Cohen LA. A review of animal model studies of tomato carotenoids, lycopene, and cancer chemoprevention. Exp Biol Med (Maywood). 2002; 227:864–68. https://doi.org/10.1177/153537020222701005 [PubMed]
- 21. Saini RK, Rengasamy KR, Mahomoodally FM, Keum YS. Protective effects of lycopene in cancer, cardiovascular, and neurodegenerative diseases: An update on epidemiological and mechanistic perspectives. Pharmacol Res. 2020; 155:104730. https://doi.org/10.1016/j.phrs.2020.104730 [PubMed]
- 22. Okajima E, Tsutsumi M, Ozono S, Akai H, Denda A, Nishino H, Oshima S, Sakamoto H, Konishi Y. Inhibitory effect of tomato juice on rat urinary bladder carcinogenesis after N-butyl-N-(4-hydroxybutyl)nitrosamine initiation. Jpn J Cancer Res. 1998; 89:22–26. https://doi.org/10.1111/j.1349-7006.1998.tb00474.x [PubMed]
- 23. Prorok PC, Andriole GL, Bresalier RS, Buys SS, Chia D, Crawford ED, Fogel R, Gelmann EP, Gilbert F, Hasson MA, Hayes RB, Johnson CC, Mandel JS, et al, and Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial Project Team. Design of the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. Control Clin Trials. 2000; 21:273S–309S. https://doi.org/10.1016/s0197-2456(00)00098-2 [PubMed]
- 24. Subar AF, Thompson FE, Kipnis V, Midthune D, Hurwitz P, McNutt S, McIntosh A, Rosenfeld S. Comparative validation of the Block, Willett, and National Cancer Institute food frequency questionnaires : the Eating at America’s Table Study. Am J Epidemiol. 2001; 154:1089–99. https://doi.org/10.1093/aje/154.12.1089 [PubMed]
- 25. Subar AF, Midthune D, Kulldorff M, Brown CC, Thompson FE, Kipnis V, Schatzkin A. Evaluation of alternative approaches to assign nutrient values to food groups in food frequency questionnaires. Am J Epidemiol. 2000; 152:279–86. https://doi.org/10.1093/aje/152.3.279 [PubMed]
- 26. Schoenfeld D. Chi-squared goodness-of-fit tests for the proportional hazards regression model. Biometrika. 1980; 67:145–53. https://doi.org/10.1093/biomet/67.1.145
- 27. Marrie RA, Dawson NV, Garland A. Quantile regression and restricted cubic splines are useful for exploring relationships between continuous variables. J Clin Epidemiol. 2009; 62:511–7.e1. https://doi.org/10.1016/j.jclinepi.2008.05.015 [PubMed]