



Introduction
Olfactory function has been found to be closely related to episodic memory [1]. Structural and functional neuroimaging studies have shown that the olfactory nerve projects to several regions in the medial temporal lobe, [2] suggesting that the episodic quality of olfactory experiences might be due to this neuroanatomical overlap [3, 4].
Previous studies in older adults have shown that odor identification ability may predict decline in cognition, in particular episodic memory, as well as cognitive impairment and dementia [5–11]. Only a few studies thus far have examined the longitudinal relationship between olfaction and episodic memory [12–14]. One study reported that fluctuations in episodic memory correspond to fluctuations in olfaction over time, particularly for individuals with Alzheimer's disease (AD) pathology [12]. Moreover, the close overlap of olfactory and episodic memory areas in the middle temporal cortex, suggests that these two processes may decline together, possibly due to a shared relationship with neuropathological changes in mediotemporal lobe areas [15, 16].
Both odor identification and episodic memory decline with increasing age [17, 18]. Other factors, such as male sex, [19] apolipoprotein epsilon 4 (APOE ε4) status, [20] depression [21] and leisure activities [22–24] have been individually associated with odor or memory function. However, to our knowledge no study has addressed if episodic memory and olfactory abilities show joint vs distinctive age-related trajectories, and which factors may predict these patterns. Such classification would contribute to a better understanding of the factors related to cognitive decline and dementia.
The aims of this study were therefore, a) to examine the extent to which trajectories of episodic memory and odor identification decline are similar, b) to characterize patterns of episodic memory and odor identification trajectories, and c) identify the predictors of the observed patterns. To address these aims, we used data from a population-based study with annual follow-up examination over an 8-year interval.
Results
Characteristics of the study population
The characteristics of the 1023 subjects are shown in Table 1. The majority, 794 (77.6%), were female, and the mean age at baseline was 78.2 (SD 7.5) years. The mean B-SIT and episodic memory (z-score) were 9.4 (SD 2.0) and 0.3 (SD 0.6) at baseline, respectively. During the follow-up period, among all participants, 290 (28.3%) participants died, and the participation rate of survivors exceeded 90%. The median number of assessments was 8 (IQR=8-5).
Table 1. Characteristics of the study sample (n= 1023) and per joint class membership.
| Characteristic | Values at baselinea | Class 1 joint stable n= 690 (67.5%) | Class 2 OI decline n= 231 (22.6%) | Class 3 joint decline n=102 (10.0%) | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Women | 794 (77.6) | 550 (79.7) | 157 (68.0) | 87 (85.3) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 79.4 (±7.4) | 77.7 (±7.3) | 82.5 (±6.1)a | 83.8 (±5.8)a | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Years of education | 15.1 (±3.2) | 15.2 (±3.2) | 14.9 (±3.2) | 14.5 (±3.3) | 0.113 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 553 (55.9) | 379 (56.8) | 120 (53.3) | 54 (55.1) | 0.652 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart disease | 79 (8.0) | 46 (6.9) | 25 (11.1) | 8 (8.2) | 0.130 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | 90 (9.1) | 61 (9.1) | 21 (9.3) | 8 (8.2) | 0.946 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 27.7 (±5.4) | 28.12 (±5.6) | 27.03 (±4.7)a | 25.9 (±5.0)a | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Depression | 157 (15.8) | 100 (14.9) | 39 (17.3) | 18 (18.4)a | 0.535 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status Never Current smoker | 596 (58.3) 404 (39.5) | 407 (59.0) 269 (39.0) | 129 (55.8) 94 (40.7) | 60 (59.4) 41 (40.6) | 0.338 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Previous smoker | 22 (2.2) | 14 (2.0) | 8 (3.5) | 0 (0.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE ε4 carriers | 213 (21.9) | 134 (20.4) | 46 (20.8)a | 33 (33.7)a | 0.011 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cognitive activity (hours per week) | 3.2 (±0.7) | 3.2 (±0.7) | 3.2 (±0.7) | 3.0 (±0.7)a | 0.045 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Social activity (hours per week) | 2.7 (±0.6) | 2.7 (±0.6) | 2.6 (±0.6)a | 2.6 (±0.6)a | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical activity (hours per week) | 3.4 (±3.5) | 3.6 (±3.7) | 3.2 (±3.2) | 3.1 (±3.1) | 0.313 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Episodic memory (z-score) | 0.3 (±0.6) | 0.4 (±0.5) | -0.1 (±0.7)a | -0.1 (±0.6)a | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| B-SIT | 9.4 (±2.0) | 10.1 (±1.3) | 7.8 (±2.2)a | 7.8 (±2.4)a | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nr of assessments | 6.6 (±2.0) | 6.3 (±2.1) | 5.7 (±1.6)a | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Incident dementia | 59 (8.6) | 59 (25.5)a | 69 (67.7)a | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Death during follow-up | 144 (20.9) | 84 (36.4)a | 62 (60.8)a | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aData are numbers (%) or means±(SD). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: APOE ε4, Apolipoprotein epsilon 4; B-SIT, Brief Smell Identification Test; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Heterogeneity of trajectories
Quadratic curves were fit for episodic memory and odor identification trajectories separately and in a joint model across 8 years. The observed individual trajectories of episodic memory and B-SIT means of the entire sample are depicted in Supplementary Figure 1A, 1E. The trajectories of B-SIT and episodic memory were clearly related, as shown by the positive correlation between their random slopes (1-class model; r= 0.57, p < .001). The joint trajectories mean of the entire sample is depicted in Figure 1A.
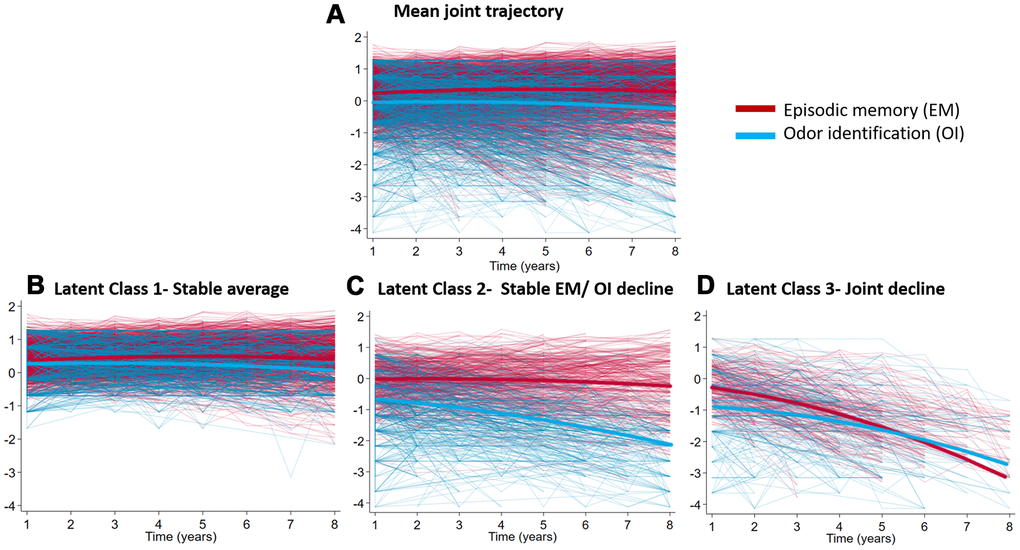
Figure 1. Fitted and observed trajectories of jointly modelled episodic memory and B-SIT scores. Scales are z-scores (mean 0, SD 1). (A) The trajectories of the entire sample (n= 1023; (B) Latent Class 1-Stable average (n= 690, 67.4%); (C) Latent Class 2- Stable EM/OI decline (n= 231, 22.6%); (D) Latent Class 3- Joint decline (n= 102, 10.0%). The mean trajectories of each plot are shown in bold.
Episodic memory
When fitting models with increasing numbers of classes, the 3-class model provided the best balance between model fit and model complexity, as confirmed by the LMR test (3- vs 4-class model: −2LL(4) = 1895.3, p = 0.321). An overview of the model fit criteria is shown in Supplementary Table 1. The difference in BIC between the 3-class model and the 4-class model was small, indicating that the model fit improvement caused by the 4th class was minimal. The best-fitting 3-class model included a class-specific intercept variance and class-invariant slope variance. The parameter estimates of the 3-class model are shown in Supplementary Table 2, and the trajectories are depicted in Supplementary Figure 1B–1D. Class 1 was the largest class (n=799, 78.1%) and was characterized by above average episodic memory at baseline, and a stable trajectory over time. Class 2 was the second largest class (n=158, 15.4%), showing average episodic memory at baseline, as well as a quadratic decline over time. Class 3 was the smallest class (n=66, 6.5%), with below average episodic memory at baseline and faster decline over time.
Odor identification
When we fitted models with increasing numbers of classes, the 3-class model provided the best fit according to the LMR test (3- vs 4-class model: −2LL(4) = 358.48, p = 0.095) and the class sizes (Supplementary Table 1). The difference in BIC between the 3-class model and the 4-class model was small, indicating that the model fit improvement caused by the 4th class was minimal. The best-fitting 3-class model included a class-specific intercept variance and class-invariant slope variance. The parameter estimates of this 3-class model are shown in Supplementary Table 1 and the trajectories are depicted in Supplementary Figure 1F–1H. Class 1 was the largest (n= 731, 71.5%) and showed above average odor identification at baseline, which remained stable over time. Class 2 was the smallest class (n=79, 7.8%), showing around average odor identification performance at baseline, as well as a linear decline over time. Class 3 was the second largest (n=212, 20.7%), with the lowest odor identification at baseline, remaining rather stable over time.
Episodic memory and odor identification
When we fitted models with increasing numbers of classes, the 3-class model provided the best balance between model fit and model complexity, as confirmed by the LMR test (3- vs 4-class model: −2LL(7)=908.95, p=0.345 (Supplementary Table 1). The difference in BIC between the 3-class model and the 4-class model was small, indicating that the model fit improvement caused by the 4th class was minimal. The 3-class model with the best fit included a class-specific intercept variance and class-invariant slope variance. The parameter estimates of this 3-class model are shown in Table 2, and the trajectories are depicted in Figure 1B–1D. Participants in Class 1 (690, 67.4%) exhibited joint stable average performance, those in Class 2 showed stable average episodic memory and decline in odor identification (n=231, 22.6%), and Class 3 was characterized by joint decline in both episodic memory and odor identification (n=102, 10.0%).
Table 2. Parameter estimates for episodic memory and odor identification trajectories by latent class membershipa.
| Parameters | Functions | Class 1- joint stable | Class 2 - OI decline | Class 3- joint decline | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| n=690 (67.4%) | n=231 (22.6%) | n= 102 (10.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| mean (SE) | mean (SE) | mean (SE) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fixed effects | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intercept | Episodic memory | 0.441 | 0.008 | -0.111 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.370 | -0.692 | -0.855 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Linear annual rate of decline | Episodic memory | 0.067 | 0.013 | -0.130 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.035 | -0.134 | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Quadratic annual rate of decline | Episodic memory | -0.008 | -0.011 | -0.036 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | -0.009 | -0.006 | -0.043 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Random effects | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intercept variance | Episodic memory | 0.130 | 0.346 | 0.322 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.104 | 0.801 | 1.161 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Linear slope variance | Episodic memory | 0.004 | 0.004 | 0.004 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.004 | 0.004 | 0.004 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance baseline | Episodic memory | 0.079 | 0.079 | 0.079 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.384 | 0.384 | 0.384 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 1 | Episodic memory | 0.09 | 0.09 | 0.09 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.26 | 0.26 | 0.26 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 2 | Episodic memory | 0.09 | 0.09 | 0.09 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.33 | 0.33 | 0.33 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 3 | Episodic memory | 0.09 | 0.09 | 0.09 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.38 | 0.38 | 0.38 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 4 | Episodic memory | 0.09 | 0.09 | 0.09 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.41 | 0.41 | 0.41 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 5 | Episodic memory | 0.08 | 0.08 | 0.08 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.35 | 0.35 | 0.35 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance follow up 6 | Episodic memory | 0.10 | 0.10 | 0.10 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.45 | 0.45 | 0.45 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Residual variance at follow up 7 | Episodic memory | 0.10 | 0.10 | 0.10 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Odor identification | 0.39 | 0.39 | 0.39 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| an was based on the final class counts of the estimated model. Note that individuals are in fact assigned a probability of class membership. OI, odor identification. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The sample characteristics of the three classes are shown in Table 1. Noteworthy is that 144 out of 690 (20.9%) participants died in Class 1 (stable average) during follow-up, 84 out of 231 (36.4%) died in Class 2 (average episodic memory/declining odor identification), and 62 out of 102 (60.8%) participants died in Class 3 (joint decline); 59 participants (8.6%) developed dementia over follow-up in Class 1, 59 (25.5%) in Class 2 and 69 (67.7%) in Class 3; participants in Class 1 were younger than those in Class 2 or 3, however the latter two classes did not differ significantly in age.
Predictors of class membership
Having established 3 distinct patterns of decline and their relative occurrence, we next sought to determine what predictors could be used to characterize these groups. We first predicted decline outcomes for episodic memory, then for odor identification, and finally for both functions.
Episodic memory
Using multivariable logistic regression, potential predictors of class membership listed in Table 1 were examined, with the class membership from the final 3-class model of episodic memory the dependent variable. This analysis was based on 914 participants; 109 (10.7%) were excluded due to missing values in covariates; the excluded participants did not differ significantly in B-SIT or episodic memory at baseline. Higher age at baseline and being an APOE ε4 carrier increased the likelihood of belonging to the lower performing Classes 2 and 3, relative to Class 1 (stable class). Higher BMI and cognitive activity decreased the likelihood of being in Class 3 relative to Class 1 (Supplementary Table 3).
Odor identification
In the multivariable logistic regression, with the class membership from our final 3-class model of odor identification as the dependent variable, higher age at baseline was associated with higher odds of belonging to Class 2 relative to Class 1 (stable class). Moreover, higher baseline age and being an APOE ε4 carrier increased the likelihood of belonging to the lowest performing Class 3 relative to Class 1 (Supplementary Table 3).
Episodic memory and odor identification
Table 3 shows the significant predictors of joint class membership presenting three patterns (joint stable, declining odor identification, and joint decline). Compared to the stable Class 1, people in the declining odor identification Class 2 were more likely to be older and male. People in the joint declining Class 3 were more likely to be older, APOE ε4 carriers, have a lower BMI, and be less engaged in cognitive activities (Table 3).
Table 3. Odds ratios (ORs) from multivariate prediction of joint class membership (n =914)a.
| Predictor | Class 2 odor function decline n= 211 | Class 3 joint decline n= 94 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OR (95% CI) | P value | OR (95% CI) | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 1.11 (1.08 to 1.14) | <0.001 | 1.15 (1.10 to 1.20) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex: male | 1.98 (1.33 to 2.95) | 0.001 | 0.73 (0.38 to 1.42) | 0.350 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Education | 0.94 (0.89 to 1.00) | 0.056 | 0.98 (0.90 to 1.07) | 0.698 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Previous | 0.98 (0.62 to 1.39) | 0.920 | 1.00 (0.61 to 1.63) | 0.994 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current | 2.11 (0.67 to 6.64) | 0.200 | 0.44 (0.09 to 2.06) | 0.299 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE ε4 carrier | 1.39 (0.92 to 2.12) | 0.119 | 2.66 (1.57 to 4.52) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes | 1.02 (0.55 to 1.91) | 0.941 | 1.43 (0.58 to 3.57) | 0.437 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart failure | 1.23 (0.69 to 2.20) | 0.488 | 1.08 (0.44 to 2.70) | 0.861 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 0.77 (0.54 to 1.08) | 0.132 | 0.79 (0.48 to 1.29) | 0.343 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 0.98 (0.95 to 1.02) | 0.309 | 0.93 (0.88 to 0.98) | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Depression | 1.50 (0.95 to 2.38) | 0.082 | 1.30 (0.68 to 2.50) | 0.423 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Social activity (hours per week) | 0.83 (0.61 to 1.13) | 0.236 | 0.82 (0.53 to 1.25) | 0.348 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cognitive activity (hours per week) | 1.00 (0.75 to 1.32) | 0.981 | 0.62 (0.43 to 0.89) | 0.010 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical activity (hours per week) | 0.99 (0.94 to 1.04) | 0.661 | 0.98 (0.91 to 1.06) | 0.609 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reference: Class 1-Joint stable (n=609). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: APOE ε4, apolipoprotein epsilon 4; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aN= 109 missing information on any 1 or more predictors. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Sensitivity analysis
As both decline in episodic memory and olfaction are strongly related to aging, we conducted a sensitivity analysis by rerunning the models of joint prediction of class membership for episodic memory and odor identification, adjusting for age at baseline. The best-fitting 3-class model included a class-specific intercept variance and class-invariant slope variance.
The parameter estimates of the 3-class model are depicted in Supplementary Table 4. Participants in Class 1 (747, 73.0%) exhibited joint stable average performance, those in Class 2 showed stable average episodic memory and decline in odor identification (n=216, 21.1%), and Class 3 was characterized by joint decline in both episodic memory and odor identification (n=60, 6.0%).
Discussion
In this study of community-dwelling older adults with long-term follow-up, we found that episodic memory and odor identification show similar aging trajectories. We identified three distinct patterns, using 8 years of longitudinal data on episodic memory and odor identification. These patterns were characterized by 1) average performance in both episodic memory and odor identification stable over time; 2) decline in odor identification only; and 3) joint decline in both functions. The patterns were associated with variables such as age, sex, APOE ε4 carrier status, BMI, cognitive activity, and were differently related to key outcomes such as dementia and death.
Previous research suggests that odor identification impairment may reflect an accumulation in brain pathology affecting brain areas involved in both olfaction and episodic memory [25–27]. Studies from MAP have previously shown that impaired baseline odor identification is associated with a steeper decline in episodic memory and smaller volumes in the hippocampus and entorhinal cortex [10, 28]. Individuals with low odor identification performance and high AD pathology have faster episodic memory decline, [12] and post-mortem AD pathology in mesiotemporal brain regions may account for 12% of the variation in odor identification before death [27]. Evidence from other cohort studies suggests that odor identification may serve as an early marker of incipient cognitive impairment and dementia [5–11]. To the best of our knowledge, this is the first study categorizing functional decline in terms of joint trajectories of episodic memory and odor identification.
We found that odor identification and episodic memory were correlated over time, showing similar trajectories. Our findings are compatible with those of a recent study, which showed that episodic memory scores and B-SIT scores vary together over time using B-SIT scores as a time-varying covariate when modelling episodic memory decline [12]. The authors of the previous study also reported that there was a stronger association between B-SIT and episodic memory variation in persons with intermediate to high AD pathology. The evidence thus points to AD pathology as a mediator between the link between decline in both behavioral domains. Indeed, the present study found that being an APOE ε4 carrier, a known risk factor for AD, [29] increased the likelihood of belonging to the “concurrent decline” class by almost 3-fold. A previous study found that episodic memory decline was associated with odor identification impairment only in ɛ4-carriers, suggesting that the ɛ4 is involved in the functional association between ongoing episodic memory decline and olfaction [30]. In a study investigating “change-change” correlation in episodic memory and odor identification, the correlation was only seen in APOE ε4 carries, specifically ε4 homozygotes [13]. This is consistent with evidence showing that ɛ4-carriers with Alzheimer’s dementia, compared to those with no ɛ4 allele, exhibit cortical atrophy patterns more pronounced in mesialtemporal lobe regions, supporting olfactory and episodic memory functions [31].
In two out of the three joint classes identified (stable Class 1 and declining Class 3), odor identification and episodic memory progressed in parallel. This is in line with evidence showing a close overlap of olfaction and episodic memory areas in the middle temporal cortex, and would suggest that these two processes reflect the integrity of mesiotemporal lobe areas, possibly due to a shared relationship with pathological changes linked to neurofibrillary tangles [15, 16]. Interestingly, in Class 2, episodic memory had a stable average trajectory, whereas odor identification was steadily declining. This may seem contrary to the patterns observed in the other two classes. However, compared to memory structures, the olfactory system has been shown to be especially sensitive to non-dementia related pathology, and environmental agents [32]. Olfactory decline is quite common in old age, and such decline may be caused by a wide variety of factors, including accumulated environmental damage to the olfactory epithelium, changes in nasal airflow and mucus composition, or declining sensitivity and tuning of receptor neurons, all of which would contribute to poor or declining olfactory performance [33, 34]. We speculate that Class 2, characterized by declining odor identification but retained memory ability, is to a large extent made up of individuals with peripheral olfactory dysfunction.
In addition to the APOE ε4 carrier status, we found that age, sex, BMI, and cognitive activity were predictors of joint class membership. The findings are consistent with previous studies showing that both odor identification and episodic memory decline with increasing age [18, 35]. Male sex has been associated with lower olfactory performance in previous studies, [19] and was also a predictor of Class 2 membership in the current study. Higher BMI was associated with lower probability of belonging to Class 3, which is in line with an emerging body of work reporting high BMI appearing to be protective of dementia due to weight loss in pre-clinical stages, [36] as this class had the highest number of individuals who were diagnosed with dementia over follow-up. Lastly, a low engagement in cognitive activities predicted joint class membership. Such activities are postulated to be protective against dementia and to delay the clinical manifestation of AD pathology as “resilience” factors [23, 24, 37]. In the joint declining class, cognitive activity at baseline was reduced, which may partly explain the steep joint decline. However, whether or not the decline in cognitive activity contributed to cognitive decline or may be a reflection of it, cannot be determined in this study. In addition, Class 3 had the highest number of incident dementia cases as well as deaths over the follow-up, suggesting that a steep decline in episodic memory as well as odor identification may be indicative of a particularly vulnerable group with rapid deterioration in cognition and higher mortality.
The strengths of this study include the annual follow-up assessments of episodic memory and odor identification, the composite score of episodic memory created from several tests, the coordinated univariate analysis of odor identification and episodic memory which characterized trajectories and their predictors separately, and the joint modelling, allowing for the characterization of these processes together and their shared predictors. Moreover, the B-SIT has been found to be valid in most cross-cultural settings, making it possible to generalize our findings to other cultures than North America [17]. The limitations of this study are that we relied on only one test for odor identification which made this measure more susceptible to missing values as well as ceiling and floor effects. Further, the measure cannot separate different aspects of olfactory dysfunction (e.g. detection, quality discrimination or word-odor matching). Moreover, the MAP study participants were recruited from retirement facilities and were on average highly educated, which may limit the generalizability to other populations. Related to this issue, the study sample was restricted to those with at least one concurrent assessment of episodic memory and odor identification. The excluded participants were older, were in worse physical health and less educated, which likely would have implications for the trajectories we identified biasing towards an underestimation of decline, especially as two of the classes had little to no decline in episodic memory during the eight years of follow up. In addition, the GMMs handle missing data patterns assuming missing at random, this assumption may not hold, with the implication of potentially underestimating the trajectories of decline in episodic memory and odor identification, due to selective survival. Furthermore, odor identification and episodic memory were tested annually, thus there may be practice effects, which may underestimate decline. However, in previous studies in MAP, we have seen little evidence that practice would substantially diminish individual differences in rates of change [10, 38]. Lastly, we did not have a comprehensive comorbidity assessment available to include as a predictor of class membership; comorbidities are common in old age and may contribute to both worse episodic memory [39] and odor identification [19].
In conclusion, this study points to the interrelation between episodic memory and olfaction in old age, which may reflect their shared vulnerability to changes in the medio-temporal lobes.
Materials and Methods
Study population
The Rush Memory and Aging Project (MAP) is an ongoing prospective clinical-pathologic study on risk factors for common chronic conditions of old age. Eligibility for participation involves agreeing to annual clinical evaluations and to the donation of brain, spinal cord, and selected nerves and muscles to Rush investigators at death. Detailed information on the MAP study design and the evaluation protocol is provided elsewhere [39]. In brief, participants were recruited from church groups, senior centers, retirement communities, and senior citizen housing facilities, within the greater Chicago area. At baseline and thereafter, all participants underwent extensive clinical assessments, including detailed medical history, neurological examination, extensive cognitive function testing, and odor identification testing.
Enrollment began in 1997. However, annual olfaction testing did not start until 2011, therefore 2011 serves as the analytic baseline for these analyses. Through 2018, 1041 participants were enrolled and annually followed-up. Out of the 1041 participants, we excluded participants with prevalent dementia (n = 18), leaving 1023 for the current analyses.
The study was approved by the Institutional Review Board of Rush University Medical Center and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all participants. All participants signed an Anatomic Gift Act for organ donation. Participants also signed a repository consent that allowed their data to be shared. More information on obtaining data can be found on the RADC Resource Sharing Hub at https://www.radc.rush.edu.
Data collection
Participants underwent uniform evaluations with trained staff including structured interviews, clinical and neurological examinations, and cognitive testing as described previously [39]. Data on socio-demographic characteristics (i.e., age, sex, and education), lifestyle factors (i.e., smoking), medical conditions, and cognitive function were collected at each wave following standardized procedures [39].
Education was recorded as participants’ maximum years of formal schooling. Smoking was categorized as “never smoked”, “former smoker” and “current smoker”. Self-reported information on medical conditions including heart disease, hypertension, diabetes was collected during the interview at baseline [39]. at study entry blood samples were taken and the APOE gene was genotyped utilizing high-throughput sequencing. Participants were stratified as epsilon 4 (ε4) carriers or ε4 non–carriers. Depression was determined according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 3rd ed, Revised, implemented with a subset of questions from the Diagnostic Interview Schedule at baseline [40]. Clinical diagnosis of dementia was conducted on the basis of criteria of the joint working group of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and Related Disorders Association (NINCDS/ADRDA) [41].
Outcomes
Odor identification
At the analytic baseline and at each follow-up, the Brief Smell Identification Test (B-SIT) (Sensonics. Inc., Haddon Heights, USA) was administered. The B-SIT is a 12-item standardized test, with 4 alternatives per item. In this test, a booklet is presented containing a scratchable patch of microencapsulated odorant on each page. The examiner scratches the odor patch with a pencil to release the odorant and places it under the participant’s nose, the participant is then asked which of four specific odors the sample most closely resembles. The score reflects the number of odors correctly recognized, with possible scores ranging from 0-12. If an item response is missing for a maximum of two, a score of 0.25 is assigned, corresponding to a chance level performance. If responses to three or more items are missing, data on this test are considered missing. The B-SIT has previously shown to be internally consistent, with good correspondence to the 40-item University of Pennsylvania Smell Identification Test from which it was derived [27].
Episodic memory
Episodic memory was measured using CERAD (Consortium to Establish a Registry for Alzheimer’s Disease) Word List Memory, Recall, and Recognition, immediate and delayed recall of the East Boston Story, and Logical Memory immediate and delayed recall. Raw scores on each test were converted to z-scores (i.e. standardized based on all MAP participants at baseline) and then the average z-score among the tests for episodic memory was computed, as reported in detail in a previous study [28].
Assessment of lifestyle factors
Three measures of stimulating mental, social and physical activities were recorded during the baseline interview.
Cognitive activities
Participants completed a 7-item cognitive activity questionnaire [22, 36]. Activities include reading, writing letters, visiting a library, and playing games such as chess or checkers. Frequency of participation in each activity was rated from 1 (once a year or less) to 5 (every day or about every day) [36].
Physical activity
Frequency of activity was recorded as the hours per week participants reported engagement in 5 categories of activities: walking for exercise, gardening or yard work, calisthenics or general exercise, bicycle riding (including stationary bikes), and swimming or water exercises [36].
Predictors on class membership
The following variables were included as potential predictors of class membership: age (years); sex (male/female); education (years); history of hypertension (yes/no), depression (yes/no), smoking (never/previous/current,) APOE ε4 status (any ε4/no ε4), diabetes (yes/no), history of heart failure (yes/no), BMI (continuous), social activity (hours per week), cognitive activity (hours per week), physical activity (hours per week).
Statistical analyses
We used growth mixture models (GMMs) to model trajectories of episodic memory and odor identification separately and jointly over time. We used yearly assessments of episodic memory and odor identification to model the trajectories. The time scale was time from the first assessment (2011) until last follow-up (2018), maximum 8 years. Episodic memory and odor identification were assessed yearly; thus the timescale is in years. The GMM is a longitudinal form of latent class analysis, using mixed models. The GMMs therefore groups participants into latent classes, on the basis of similarities in their trajectory patterns over time. This is done by fitting an increasing number of curves until an optimal balance between model fit and model complexity is reached. Quadratic models with 1 to 5 classes were fit, and the final model was chosen based on the Bayesian information criterion (BIC), Lo-Mendell-Rubin (LMR) likelihood ratio test, and class size. The BIC indicates the fit of a model, the lower the value, the better the fit of the model is. The LMR test is used to compare model fit between 2 nested models. A significant LMR test indicates that the model with k classes has a better fit than the same model with k − 1 classes. The parameter estimates were obtained using maximum likelihood estimation, with standard errors (SEs) that are robust to non-normality. The quadratic slope variance was fixed to zero. For ease of interpretation and presentation, the B-SIT scores were standardized (based on all participants at baseline) for comparability with the global cognition z-score. For parsimony, the residual variances assumed to be equal across classes and were allowed to vary over time. After the model with the best fit was decided, we examined which factors predicted class membership using multinomial logistic regression with the 3-step method in a multivariable model [42]. The GMMs were fit using Mplus version 8.2. Further analyses and processing of results and multinomial logistic regression models, were performed using Stata v. 15 and RStudio v. 1.2.5001.
Author Contributions
Christina S, Dintica, Karolinska Institutet, Stockholm, Sweden, Design and conceptualized study; analyzed the data; drafted the manuscript for intellectual content; Miriam Haaksma, Leiden University Medical Center, Leiden, Netherlands, Statistical supervision/advice; Drafting/revising manuscript for content; Jonas K, Olofsson Stockholm University, Stockholm, Sweden, Drafting/revising manuscript for content; analysis interpretation; David A. Bennett, Rush University Medical Center, Chicago, United States, Acquisition of data; Drafting/revising manuscript for content; study supervision; Weili Xu, Karolinska Institutet, Stockholm, Sweden Drafting/revising manuscript for content; Design and conceptualized study; study supervision.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
The study was supported by grant R01AG17917 from the National Institutes on Aging. MAP data can be requested at https://www.radc.rush.edu.
WX received grants from the Swedish Research Council (No. 2017-00981), the National Natural Science Foundation of China (No. 81771519), Konung Gustaf V:s och Drottning Victorias Frimurare Foundation (No. 2016-2017) and Alzheimerfonden (2017-2018). CSD is supported in part by KID-funding from Karolinska Institutet and SWEAH. JO received grants from the Swedish Foundation for Humanities and Social Sciences (M14-0375:1) and Knut and Alice Wallenberg Foundation (KAW 2016:0229). DB received grants from the National Institutes of Health (R01AG17917 and UH2NS100599). This project is part of CoSTREAM (http://www.costream.eu/) and received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement 70 No 667375.
References
- 1. Willander J, Larsson M. Smell your way back to childhood: autobiographical odor memory. Psychon Bull Rev. 2006; 13:240–44. https://doi.org/10.3758/bf03193837 [PubMed]
- 2. Carmichael ST, Clugnet MC, Price JL. Central olfactory connections in the macaque monkey. J Comp Neurol. 1994; 346:403–34. https://doi.org/10.1002/cne.903460306 [PubMed]
- 3. Arshamian A, Iannilli E, Gerber JC, Willander J, Persson J, Seo HS, Hummel T, Larsson M. The functional neuroanatomy of odor evoked autobiographical memories cued by odors and words. Neuropsychologia. 2013; 51:123–31. https://doi.org/10.1016/j.neuropsychologia.2012.10.023 [PubMed]
- 4. Herz RS, Eliassen J, Beland S, Souza T. Neuroimaging evidence for the emotional potency of odor-evoked memory. Neuropsychologia. 2004; 42:371–78. https://doi.org/10.1016/j.neuropsychologia.2003.08.009 [PubMed]
- 5. Swan GE, Carmelli D. Impaired olfaction predicts cognitive decline in nondemented older adults. Neuroepidemiology. 2002; 21:58–67. https://doi.org/10.1159/000048618 [PubMed]
- 6. Olofsson JK, Rönnlund M, Nordin S, Nyberg L, Nilsson LG, Larsson M. Odor identification deficit as a predictor of five-year global cognitive change: interactive effects with age and ApoE-epsilon4. Behav Genet. 2009; 39:496–503. https://doi.org/10.1007/s10519-009-9289-5 [PubMed]
- 7. Sohrabi HR, Bates KA, Weinborn MG, Johnston AN, Bahramian A, Taddei K, Laws SM, Rodrigues M, Morici M, Howard M, Martins G, Mackay-Sim A, Gandy SE, Martins RN. Olfactory discrimination predicts cognitive decline among community-dwelling older adults. Transl Psychiatry. 2012; 2:e118. https://doi.org/10.1038/tp.2012.43 [PubMed]
- 8. Lipnicki DM, Sachdev PS, Crawford J, Reppermund S, Kochan NA, Trollor JN, Draper B, Slavin MJ, Kang K, Lux O, Mather KA, Brodaty H. Risk factors for late-life cognitive decline and variation with age and sex in the Sydney Memory and Ageing Study. PLoS One. 2013; 8:e65841. https://doi.org/10.1371/journal.pone.0065841 [PubMed]
- 9. Devanand DP, Lee S, Manly J, Andrews H, Schupf N, Doty RL, Stern Y, Zahodne LB, Louis ED, Mayeux R. Olfactory deficits predict cognitive decline and Alzheimer dementia in an urban community. Neurology. 2015; 84:182–89. https://doi.org/10.1212/WNL.0000000000001132 [PubMed]
- 10. Dintica CS, Marseglia A, Rizzuto D, Wang R, Seubert J, Arfanakis K, Bennett DA, Xu W. Impaired olfaction is associated with cognitive decline and neurodegeneration in the brain. Neurology. 2019; 92:e700–09. https://doi.org/10.1212/WNL.0000000000006919 [PubMed]
- 11. Devanand DP, Tabert MH, Cuasay K, Manly JJ, Schupf N, Brickman AM, Andrews H, Brown TR, DeCarli C, Mayeux R. Olfactory identification deficits and MCI in a multi-ethnic elderly community sample. Neurobiol Aging. 2010; 31:1593–600. https://doi.org/10.1016/j.neurobiolaging.2008.09.008 [PubMed]
- 12. Knight JE, Bennett DA, Piccinin AM. Variability and Coupling of Olfactory Identification and Episodic Memory in Older Adults. J Gerontol B Psychol Sci Soc Sci. 2020; 75:577–84. https://doi.org/10.1093/geronb/gby058 [PubMed]
- 13. Josefsson M, Larsson M, Nordin S, Adolfsson R, Olofsson J. APOE-ɛ4 effects on longitudinal decline in olfactory and non-olfactory cognitive abilities in middle-aged and old adults. Sci Rep. 2017; 7:1286. https://doi.org/10.1038/s41598-017-01508-7 [PubMed]
- 14. Wehling EI, Wollschlaeger D, Nordin S, Lundervold AJ. Longitudinal changes in odor identification performance and neuropsychological measures in aging individuals. Neuropsychology. 2016; 30:87–97. https://doi.org/10.1037/neu0000212 [PubMed]
- 15. Arnold SE, Hyman BT, Flory J, Damasio AR, Van Hoesen GW. The topographical and neuroanatomical distribution of neurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer’s disease. Cereb Cortex. 1991; 1:103–16. https://doi.org/10.1093/cercor/1.1.103 [PubMed]
- 16. Arnold SE, Hyman BT, Van Hoesen GW. Neuropathologic changes of the temporal pole in Alzheimer’s disease and Pick’s disease. Arch Neurol. 1994; 51:145–50. https://doi.org/10.1001/archneur.1994.00540140051014 [PubMed]
- 17. Tromp D, Dufour A, Lithfous S, Pebayle T, Després O. Episodic memory in normal aging and Alzheimer disease: Insights from imaging and behavioral studies. Ageing Res Rev. 2015; 24:232–62. https://doi.org/10.1016/j.arr.2015.08.006 [PubMed]
- 18. Attems J, Walker L, Jellinger KA. Olfaction and Aging: A Mini-Review. Gerontology. 2015; 61:485–90. https://doi.org/10.1159/000381619 [PubMed]
- 19. Seubert J, Laukka EJ, Rizzuto D, Hummel T, Fratiglioni L, Bäckman L, Larsson M. Prevalence and Correlates of Olfactory Dysfunction in Old Age: A Population-Based Study. J Gerontol A Biol Sci Med Sci. 2017; 72:1072–79. https://doi.org/10.1093/gerona/glx054 [PubMed]
- 20. Olofsson JK, Nordin S, Wiens S, Hedner M, Nilsson LG, Larsson M. Odor identification impairment in carriers of ApoE-varepsilon4 is independent of clinical dementia. Neurobiol Aging. 2010; 31:567–77. https://doi.org/10.1016/j.neurobiolaging.2008.05.019 [PubMed]
- 21. Pentzek M, Grass-Kapanke B, Ihl R. Odor identification in Alzheimer’s disease and depression. Aging Clin Exp Res. 2007; 19:255–58. https://doi.org/10.1007/BF03324698 [PubMed]
- 22. Wilson RS, Scherr PA, Schneider JA, Tang Y, Bennett DA. Relation of cognitive activity to risk of developing Alzheimer disease. Neurology. 2007; 69:1911–20. https://doi.org/10.1212/01.wnl.0000271087.67782.cb [PubMed]
- 23. Fratiglioni L, Paillard-Borg S, Winblad B. An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol. 2004; 3:343–53. https://doi.org/10.1016/S1474-4422(04)00767-7 [PubMed]
- 24. Wang HX, MacDonald SW, Dekhtyar S, Fratiglioni L. Association of lifelong exposure to cognitive reserve-enhancing factors with dementia risk: A community-based cohort study. PLoS Med. 2017; 14:e1002251. https://doi.org/10.1371/journal.pmed.1002251 [PubMed]
- 25. Attems J, Walker L, Jellinger KA. Olfactory bulb involvement in neurodegenerative diseases. Acta Neuropathol. 2014; 127:459–75. https://doi.org/10.1007/s00401-014-1261-7 [PubMed]
- 26. Kovács T. Mechanisms of olfactory dysfunction in aging and neurodegenerative disorders. Ageing Res Rev. 2004; 3:215–32. https://doi.org/10.1016/j.arr.2003.10.003 [PubMed]
- 27. Wilson RS, Arnold SE, Schneider JA, Tang Y, Bennett DA. The relationship between cerebral Alzheimer’s disease pathology and odour identification in old age. J Neurol Neurosurg Psychiatry. 2007; 78:30–35. https://doi.org/10.1136/jnnp.2006.099721 [PubMed]
- 28. Wilson RS, Arnold SE, Tang Y, Bennett DA. Odor identification and decline in different cognitive domains in old age. Neuroepidemiology. 2006; 26:61–67. https://doi.org/10.1159/000090250 [PubMed]
- 29. Kanekiyo T, Xu H, Bu G. ApoE and Aβ in Alzheimer’s disease: accidental encounters or partners? Neuron. 2014; 81:740–54. https://doi.org/10.1016/j.neuron.2014.01.045 [PubMed]
- 30. Olofsson JK, Josefsson M, Ekström I, Wilson D, Nyberg L, Nordin S, Nordin Adolfsson A, Adolfsson R, Nilsson LG, Larsson M. Long-term episodic memory decline is associated with olfactory deficits only in carriers of ApoE-є4. Neuropsychologia. 2016; 85:1–9. https://doi.org/10.1016/j.neuropsychologia.2016.03.004 [PubMed]
- 31. Wolk DA, Dickerson BC, and Alzheimer’s Disease Neuroimaging Initiative. Apolipoprotein E (APOE) genotype has dissociable effects on memory and attentional-executive network function in Alzheimer’s disease. Proc Natl Acad Sci USA. 2010; 107:10256–61. https://doi.org/10.1073/pnas.1001412107 [PubMed]
- 32. Attems J, Lintner F, Jellinger KA. Olfactory involvement in aging and Alzheimer’s disease: an autopsy study. J Alzheimers Dis. 2005; 7:149–57. https://doi.org/10.3233/jad-2005-7208 [PubMed]
- 33. Doty RL, Kamath V. The influences of age on olfaction: a review. Front Psychol. 2014; 5:20. https://doi.org/10.3389/fpsyg.2014.00020 [PubMed]
- 34. Mobley AS, Rodriguez-Gil DJ, Imamura F, Greer CA. Aging in the olfactory system. Trends Neurosci. 2014; 37:77–84. https://doi.org/10.1016/j.tins.2013.11.004 [PubMed]
- 35. Kivimäki M, Luukkonen R, Batty GD, Ferrie JE, Pentti J, Nyberg ST, Shipley MJ, Alfredsson L, Fransson EI, Goldberg M, Knutsson A, Koskenvuo M, Kuosma E, et al. Body mass index and risk of dementia: Analysis of individual-level data from 1.3 million individuals. Alzheimers Dement. 2018; 14:601–09. https://doi.org/10.1016/j.jalz.2017.09.016 [PubMed]
- 36. Wilson RS, Boyle PA, Yu L, Barnes LL, Schneider JA, Bennett DA. Life-span cognitive activity, neuropathologic burden, and cognitive aging. Neurology. 2013; 81:314–21. https://doi.org/10.1212/WNL.0b013e31829c5e8a [PubMed]
- 37. Doty RL, Marcus A, Lee WW. Development of the 12-item Cross-Cultural Smell Identification Test (CC-SIT). Laryngoscope. 1996; 106:353–56. https://doi.org/10.1097/00005537-199603000-00021 [PubMed]
- 38. Wilson RS, Beckett LA, Barnes LL, Schneider JA, Bach J, Evans DA, Bennett DA. Individual differences in rates of change in cognitive abilities of older persons. Psychol Aging. 2002; 17:179–93. [PubMed]
- 39. Bennett DA, Schneider JA, Buchman AS, Barnes LL, Boyle PA, Wilson RS. Overview and findings from the rush Memory and Aging Project. Curr Alzheimer Res. 2012; 9:646–63. https://doi.org/10.2174/156720512801322663 [PubMed]
- 40. Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health Diagnostic Interview Schedule. Its history, characteristics, and validity. Arch Gen Psychiatry. 1981; 38:381–89. https://doi.org/10.1001/archpsyc.1981.01780290015001 [PubMed]
- 41. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984; 34:939–44. https://doi.org/10.1212/wnl.34.7.939 [PubMed]
- 42. Vermunt JK. Latent class modeling with covariates: two improved three-step approaches. Polit Anal. 2010; 18:450–69. https://doi.org/10.1093/pan/mpq025