



Introduction
Cognitive impairment is common in adults after stroke, which might increase the disability and mortality in post-stroke patient as well [1, 2]. Post-stroke cognitive impairment (PSCI) refers to cognitive impairment that develops after a stroke without any indications of major pre-stroke cognitive decline [3]. Prevalence of PSCI varies among different reports, ranging from 20% to 82% [3–6]. Because PSCI might recover due to rehabilitation and neuroplasticity during the first few months after stroke [3, 7], while less improvement would be found after 6 months [8, 9]. Therefore, it is essential to identify stroke survivors with high risk of developing PSCI as early as possible, so that early preventive and treatment measures could be taken to prevent or delay PSCI [1–3].
As a screening tool, the Montreal Cognitive Assessment (MoCA) is sensitive in detecting early PSCI. Though it was reported that MoCA score was a good predictor of PSCI in 6-9 month after stroke [4, 10], some risk factors such as age, level of education, medical history of hypertension, diabetes mellitus, smoking and atrial fibrillation reported, were associated with higher risk of PSCI [3, 11, 12]. However, the role of MoCA results in acute phase or any other bedside tool for PSCI risk is still lacking.
The aim of this study was to identify factors associated with 6-month PSCI. Using the characteristics and features in the acute stage of AIS, to build an easy and practical predictive model for PSCI in Chinese population would be helpful in identifying high-risk patients as early as the acute phase of AIS. In addition, there was of interest to explore the potential subgroup of patients with cognitive impairment at acute phase who returned to normal cognitive performance (“reverters”) 6 months after AIS onset.
Materials and Methods
Study design and patients
This study was a multicenter retrospective study, which was approved by the Huashan Hospital Institutional Review Board (IRB protocol number V2.0; ethical approval number KY2017-201) and of each participating center before the study began. The trial was conducted in accordance with the guiding principles of the Declaration of Helsinki. All patients or their caregivers gave written informed consent before data collection.
The records of consecutive patients with confirmed AIS treated at 4 regional stroke centers from June 2017 to February 2018 were retrospectively reviewed. AIS was diagnosed by a neurologist according to the World Health Organization definition. Patients with AIS were provided with a MoCA assessment both within 2 weeks after AIS onset (baseline MoCA) and 6 months after AIS (6-month MoCA) [13]. Patients with pre-existing cognitive impairment before AIS according to their medical records and patients with severe cognitive impairment or aphasia who might be unable to undertake MoCA assessment were excluded. Then those patients’ medical records were further extracted including their demographic, baseline characteristics and clinical information such as the National Institutes of Health Stroke Scale (NIHSS) score [8, 10, 12], the subtype of stroke classification [8, 12] and the Oxfordshire Community Stroke Project (OCSP) classification were also collected [14].
Outcome measures
A patient with a baseline MoCA score < 22 was considered to have acute cognitive impairment, and a patient with a 6-month MoCA score <22 was diagnosed as PSCI [10]. An additional point was added to a patient's MoCA total score when his/her education was less than 12 years [10]. The scores of the 7 MoCA subdomains (visuospatial/executive, naming, attention, language, abstraction, delayed recall and orientation) [13] were also recorded, separately. Additionally, the changes of patients’ 6-month MoCA scores were assessed for all patients [13].
The number and percentage of patients with acute cognitive impairment who recovered and had normal cognitive performance 6 month after AIS (MoCA ≥22) (“reverters”) were calculated and factors associated with the reverters were determined.
Statistical analysis
Categorical data was described with number (n) and percentage (%) while normally distributed continuous data was described with mean ± standard deviation (SD) and non-normally distributed continuous data was described with median (interquartile range [IQR]). Prevalence of acute cognitive impairment and 6-month PSCI were calculated with the number of patients with cognitive impairment as numerator and the number of all included patients as denominator, and 95% confidential interval (CI) was estimated with Poisson distribution. Comparisons between two groups were performed using the chi-square test or Fisher’s exact test for categorical data, the Student t test for normally distributed continuous data and the Mann-Whitney U test or Wilcoxon rank sum tests (when appropriate) for non-normally distributed continuous data. Factors associated with PSCI were studied using univariate analysis entering patients’ baseline demographic and clinical characteristics. We put most variables with p<0.1 into the multivariate logistic regression and interactions would be tested before. The results were presented as odds ratios (ORs) with 95%CI. Statistical analyses were performed using the Stata V15.1(College Station, TX, USA). All tests were two-tailed, and a P value < 0.05 was considered statistically significant.
Modeling and validation
The risk factors associated with PSCI at 6 months identified by the multivariate analysis were included in multivariate logistic regression analysis based on data from patients from 2 of the 4 centers (Huashan Hospital and the Tenth People’s Hospital) to build a predictive model for predicting a patient’s risk of developing PSCI 6 months after AIS. A scoring system (point 1-3) was used to score each risk factor in the model based on their OR and 95% CI. The model’s discriminatory ability was assessed with receiver operating characteristic (ROC) analysis using the area under the curve (AUC), and the Hosmer–Lemeshow test was used to confirm that the observed event rates match expected event rates in subgroups of the modeling population and to assess calibration of the model. Internal cross-validation of the regression model between parameters of the DREAM-LDL Scale score and 6-month cognitive impairment was based on 1,000 bootstrap replicates. Estimated mean accuracy and 95% confidence intervals would be analyzed. External validation of our predictive model was done in a separate cohort, another 2 of the 4 hospitals (East Hospital and Sixth People’s Hospital).
Results
Prevalence of PSCI 6 months after AIS and its risk factors
The study flow diagram was illustrated in Figure 1 total of 383 AIS patients were included in this study. They had a median age of 63 (interquartile range [IQR]: 56-70) years, and 75.46% of them were male. Most of them had mild or moderate stroke (NIHSS≤15, 88.77%).
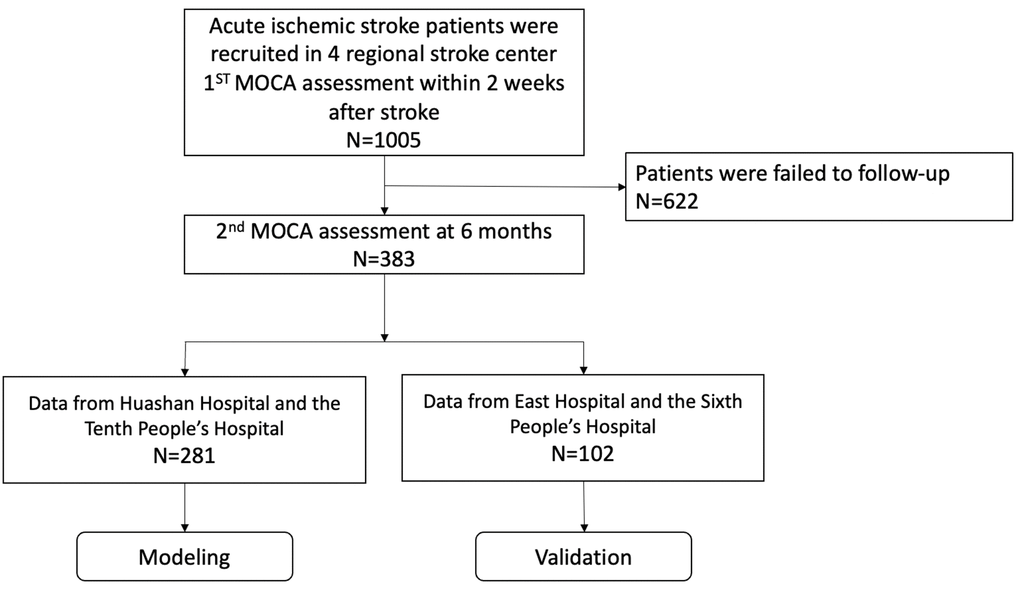
Figure 1. Study flowchart.
Of the 383 patients, 131 patients had PSCI 6 months after their AIS onset and the prevalence of PSCI is 34.2% (95%CI 29.5%-39.1%). Demographics and baseline characteristics of the PSCI and non-PSCI patients at 6 months were described in Table 1. Univariate analysis revealed that compared to the non-PSCI population, the PSCI population had higher percentage of patients who were elder, female and more severe stroke and with fewer years of education. The PSCI population also had a significantly different distribution of patients with LDL- C level <1.8mmol/L, 1.8-2.5 mmol/L and ≥2.6mmol/L (Supplementary Figure 1).
Table 1. Patient demographic and baseline characteristics.
| Variables | All patients (N=383) | Non-PSCI (N=252) | PSCI (N=131) | P value* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years, median (IQR) | 63.00 (56.00-70.00) | 62.00 (56.00-69.50) | 64.00 (56.00-71.00) | 0.063 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 63<Age<80, n (%) | 93 (24.28) | 58 (21.64) | 35 (30.43) | 0.140 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥80, n (%) | 102 (26.63) | 64(23.88) | 38 (33.04) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male, n (%) | 289 (75.46) | 211 (78.73) | 78 (67.83) | 0.023* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2, median (IQR) | 24.22 (22.49-26.45) | 23.48 (21.54-25.39) | 0.058 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Level of education | 0.002* | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤5 years, n (%) | 63 (16.45) | 33 (12.31) | 30 (26.09) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >5 and ≤9 years, n (%) | 140 (36.55) | 95 (35.45) | 45 (39.13) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >9 and ≤12 years, n (%) | 116 (30.29) | 91 (33.96) | 25 (21.74) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >12 years, n (%) | 64 (16.71) | 49 (18.28) | 15 (13.04) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severity of stroke, median [interquartile] | 11[2-14] | 11[2-14] | 11[3-14] | 0.016* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mild-Moderate (NIHSS≤8), n (%) | 199 (51.96) | 137 (51.11) | 62 (65.35) | 0.985 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate (8<NIHSS<15), n (%) | 141(36.81) | 87(32.46) | 54 (28.71) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severe (NIHSS≥15), n (%) | 43 (11.23) | 28 (6.28) | 15 (5.94) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TOAST classification | 0.120 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Large artery atherosclerosis, n (%) | 241 (63.09) | 174 (64.93) | 67(58.77) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardioembolism, n (%) | 22 (5.76) | 15 (5.60) | 7(6.14) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Small vessel occlusion, n (%) | 88 (23.04) | 61 (22.76) | 27 (23.68) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other cause, n (%) | 11 (2.88) | 9 (3.36) | 2 (1.75) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown cause, n (%) | 20 (5.24) | 9 (3.36) | 11 (9.65) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OCSP classification | 0.112 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TACI, n (%) | 12 (3.14) | 5 (1.87) | 7 (6.14) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PACI, n (%) | 218 (56.62) | 152 (56.72) | 66 (57.89) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| POCI, n (%) | 21 (5.50) | 17 (6.34) | 4 (3.51) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LACI, n (%) | 131 (34.39) | 94 (35.07) | 37 (32.46) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBG, mmol/L, median (IQR) | 5.40(4.80-7.16) | 5.30(4.80-6.50) | 5.60(4.90-7.53) | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5.4<FBG<7.1, n(%) | 101(37.62) | 63(23.51) | 38(33.04) | 0.080 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥7.1, n(%) | 105(39.04) | 64(23.88) | 41(35.65) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C, mmol/L, median (IQR) | 2.64 (2.11-3.19) | 2.65 (2.14-3.22) | 2.58 (1.82-3.23) | 0.201 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <1.8, n (%) | 63 (16.62) | 35 (13.21) | 28 (24.56) | 0.014* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1.8≤LDL-C<2.6, n (%) | 122 (32.19) | 93 (35.09) | 29 (25.44) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥2.6, n (%) | 194 (51.19) | 137 (51.70) | 57 (50.00) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medical history | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension, n (%) | 185 (48.30) | 134 (50.00) | 51 (44.35) | 0.310 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes, n (%) | 102 (26.63) | 66 (24.63) | 36 (31.30) | 0.175 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia, n (%) | 7 (1.83) | 5(1.87) | 2(1.74) | 0.320 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Atrial fibrillation, n (%) | 16 (0.41) | 8(0.32) | 8(0.61) | 0.175 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prior stroke, n (%) | 8 (2.09) | 8(2.99) | 0(0.00) | 0.055 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Myocardial infarction, n (%) | 2 (0.052) | 2(0.75) | 0(0.00) | 0.489 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P value referred to comparison between PSCI and non-PSCI patients. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PSCI, post-stroke cognitive impairment; IQR, interquartile range; FBG, fasting blood glucose; LDL-C, low density lipoprotein (LDL) cholesterol; NIHSS, The National Institutes of Health Stroke Scale; TOAST, Trial of ORG 10172 in Acute Stroke Treatment; OCSP, The Oxfordshire Community Stroke Project; TACI, total anterior circulation infarct; PACI, partial anterior circulation infarct; POCI, posterior circulation infarct; LACI, lacunar circulation infarct. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Multivariate logistic regression analysis were listed in Supplementary Table 1 and only MoCA performance was independently related to the risk of PSCI at 6 months (Table 2).
Table 2. Multivariate logistic regression analysis of risk/protective factors for patients developing PSCI 6 month after acute ischemic stroke.
| Variables | OR | 95% CI | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline MoCA | 0.74 | 0.69~0.78 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Level of education (<6yr as reference, as categorical variables) | 0.219 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 6-9 years | 1.15 | 0.50~2.63 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9-12 years | 0.72 | 0.30~1.71 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥12 years | 0.70 | 0.27~1.89 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age(as categorical variables) | 0.572 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤63 years old | As refer | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 63<Age<80 years old | 1.30 | 0.73~2.32 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥80 years old | 0.94 | 0.29~3.03 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBG (as categorical variables) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤5.4mmol/L | As refer | 0.482 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5.4mmol/L<FBG<7.1mmol/L | 1.49 | 0.76~2.95 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥7.1mmol/L | 1.27 | 0.64~2.53 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDLC level (LDL-C<1.8mmol/L or LDL-C≥2.6mmol/L as reference) | 0.327 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0.3342.6>LDL-C≥1.8mmol/L | 0.76 | 0.43~1.33 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severity of Stroke (NIHSS, points, as categorical variables) | 0.876 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate (8<NIHSS<15), n (%) | 1.11 | 0.57~2.14 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severe (NIHSS≥15), n (%) | 0.90 | 0.43~1.89 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PSCI, post-stroke cognitive impairment; OR, odd ratio; CI, confidential interval; LDL-C, low density lipoprotein (LDL) cholesterol. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Spearman’s rank correlation indicated that a patient’s baseline MoCA score was negatively correlated to the risk of PSCI at 6-month (rs=-0.61, P<0.001).
Temporal changes of the patients’ cognitive performance
According to these patients’ baseline MoCA assessments taken within 2 weeks of their AIS onset, 190 of the 383 patients had acute cognitive impairment (49.6%), the prevalence of acute phase was significantly higher than the prevalence of PSCI 6 months after AIS (34.2%). Of the 190 patients with acute/subacute cognitive impairment, 76 (40.0%) patients recovered (reverter) and had normal cognitive status 6 month after AIS, while 17 (8.9%) with normal cognitive status at baseline deteriorated and had PSCI 6 month after AIS.
The patients’ general and domain-specific changes in their cognitive performance were described in Table 3. Among them, the mean MoCA score of patients with PSCI at 6 months (N=131) had insignificant improvement from baseline (15.78±5.60 at baseline vs 16.13±4.40 at 6 months, P=0.0519), while there was significant improvement in the 252 non-PSCI patients’ mean MoCA score (24.03±4.17 at baseline vs 26.58±2.27 at 6 months, P<0.001). For patients with PSCI, their visuospatial/executive and delayed recall improved significantly, naming and language abilities deteriorated while their attention, abstraction and orientation remained stable. Overall, non-PSCI patients performed significantly better than PSCI patients in all of the 7 subdomains of MoCA and also MoCA total scores at baseline as well as 6 months after their AIS (All P<0.001).
Table 3. Temporal changes of MoCA total and subdomain scores in patients with acute ischemic stroke.
| Domains | Scoring range | All patients (N=383) | PSCI (N=131) | Non-PSCI (N=252) | t-testvalues# | P value* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline | 6-month | t-test values | Baseline | 6-month | t-testvalues | Baseline | 6-month | t-testvalues | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Visuospatial/ executive | 0-5 | 2.91 ± 1.64 | 3.39 ± 1.48 | 6.21 | 1.81 ± 1.43 | 2.16 ± 1.47 | 2.31 | 3.48 ± 1.44 | 4.02± 1.01 | 6.30 | 14.54 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Naming | 0-3 | 2.54 ± 0.80 | 2.44 ± 0.80 | -2.37 | 2.10 ± 1.00 | 1.90 ± 1.01 | -2.20 | 2.76 ± 0.55 | 2.72 ± 0.49 | -1.07 | 10.91 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Attention | 0-6 | 4.91 ± 1.37 | 5.02 ± 1.27 | 1.66 | 4.02 ± 1.62 | 4.07 ± 1.51 | 0.37 | 5.37 ± 0.96 | 5.52 ± 0.74 | 2.01 | 12.46 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Language | 0-3 | 1.97 ± 1.07 | 1.96 ± 1.01 | -0.24 | 1.26 ± 1.02 | 1.07 ± 0.92 | -1.85 | 2.35 ± 0.88 | 2.42 ± 0.69 | 1.19 | 16.04 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abstraction | 0-2 | 1.15 ± 0.79 | 1.46 ± 0.91 | 6.09 | 0.72 ± 0.73 | 0.79 ± 0.75 | 1.00 | 1.37 ± 0.72 | 1.81 ± 0.79 | 1.00 | 12.06 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Delayed recall | 0-5 | 1.95 ± 1.71 | 2.91 ± 1.74 | 10.52 | 0.92 ± 1.44 | 1.31 ± 1.48 | 2.58 | 2.49± 1.60 | 3.75 ± 1.19 | 11.36 | 17.55 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Orientation | 0-6 | 5.29 ± 1.29 | 5.43 ± 1.17 | 2.07 | 4.70 ± 1.63 | 4.67 ± 1.67 | -0.21 | 5.6 ± 0.93 | 5.82 ± 0.43 | 3.57 | 10.30 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | 0-30 | 21.55 ± 5.99 | 23.44 ± 5.69 | 9.20 | 16.41 ± 5.72 | 16.85 ± 4.54 | 1.11 | 24.23 ± 4.07 | 26.87± 2.01 | 11.84 | 29.83 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The t tests were performed to compare the baseline performance to the 6-month performance in all patients, PCSI population and non-PSCI population, respectively. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| #t tests were also performed between PCSI population and non-PSC population at 6months. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *P value referred to comparison between PSCI and non-PSCI patients at 6 months. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Variables were expressed as mean ± standard deviation (SD). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MoCA, the Montreal Cognitive Assessment. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In addition, 76 the 190 patients (40.0%) with cognitive impairment at acute phase recovered and reverted back to have normal cognitive status at 6-month after AIS. The reverters’ mean MoCA score improve to 25.71±1.89 at 6-month from the baseline 19.34±3.23 (P<0.001). Multivariate logistic regression in patients with acute cognitive impairment revealed that patient with appropriate LDL level was more likely to be reverters (OR 1.79, 95%CI: 1.00~3.22, P=0.041).
Predictive model building and validation
The internal validation model was based on 281 patients from Huashan Hospital and the Tenth People’s Hospital. The predictive model, DREAM-LDL, included 6 variables: diabetes (fasting blood glucose level), rating (severity of stroke as reflected by NIHSS at admission), level of education, age, baseline MoCA and LDL-C level. DREAM-LDL had a risk score ranging from 0 to 10 (Table 4). We scored these risk factors according to their odds ratio (Supplementary Tables 1, 2). The DREAM-LDL had an AUROC of 0.93, its Hosmer-Lemeshow chi2(8) was 1.49 (Figure 2A). Accuracy of the derivation model based on 1,000 bootstrap replicates was 75.7% (66.4%– 84.9%). A 3-tier scoring system was used to evaluate a patient’s risk of having PSCI 6 months after AIS. A patient with a score of 0-2 points was considered to have low risk, a patient with a score of 3-5 points was considered to have a moderate risk and a patient with 6 points or high was considered to have a high risk.
Table 4. DREAM-LDL: a clinical model for the risk of PSCI at 6-month.
| Risk factors | Scores | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes(FBG, mmol/L) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBG>7.1 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7.1>FBG>5.4 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Rating(Severity of Stroke, NIHSS) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NIHSS8≥15 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 15≥NIHSS≥8 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Level of Education | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No more than 9 years | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No more than 12 years | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| > 80 years old | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| > 63 years old | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baseline MoCA<22 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Inappropriate LDL-C (1.8-2.6mmol/L) | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DREAM LDL scale predict PSCI after stroke is ranged from 0-10 points. Low risk is as 0-2 points. Moderate risk is as 3-5 points. High risk is defined as 6 or higher. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBG, Fasting blood glucose; NIHSS, The National Institutes of Health Stroke Scale; LDL-C, low density lipoprotein (LDL) cholesterol; MoCA, Montreal Cognitive Assessment. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
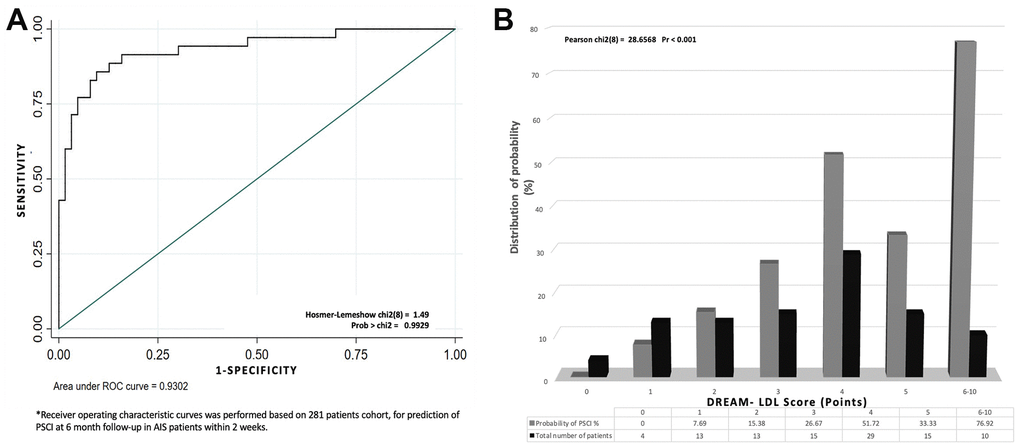
Figure 2. The establishment and validation of the DREAM-LDL scale. (A) Receiver operating characteristic (ROC) curve based on a cohort of 281 patients for identifying AIS patients at risk of mid-term PSCI as early as within 2 weeks of AIS onset. (B) The DREAM-LDL scale was validated in another cohort of 102 AIS patients.
External validation of the model was performed on the 102 patients from the 2 of the 4 hospitals in the study (East Hospital and the Sixth People’s Hospital). 7.89% of the patients with a score of 0-2 points, 40.68% of the patients with a score of 3-5 points and 78.82% of the patients with a score of 6 points or higher had PSCI 6 months after AIS (Figure 2B). The higher the DREAM-LDL score was, the higher the likelihood of PSCI at 6-month. There was no statistical difference in AUC-ROC between the derivation and validation cohorts. Additionally, we compared the performance of DREAM-LDL in reverters and non-reverters in Supplementary Figure 2, which showed no statistical difference.
Discussion
Our finding of PSCI prevalence of 34.2% was consistent with the mid-term PSCI prevalence reported by these previous studies [1, 4, 6, 15]. Based on this AIS database, we found PSCI was common at 6-months and that old age, fewer year of education, history of atrial fibrillation and acute cognitive impairment were risk factors for PSCI. However, the LDL-C level of 1.8-2.5mmol/L was a likely protective factor against PSCI. We established and validated a bedside predictive tool, DREAM-LDL, which could be helpful in early detection of PSCI and potential reverters.
Our study showed that LDL-C played a paradox role in whether a patient was at risk of PSCI 6 months after AIS (Supplementary Figure 1). Previous studies produced conflicting results on relationship between LDL-C level and cognitive ability [16–32]. According to the National Lipid Association recommendations for patient-centered management of dyslipidemia, the desirable LDL-C level was <1.8mmol/L (100mg/dL) for people at very high risk of atherosclerotic cardiovascular disease (ASCVD) and <2.6mmol/L (130mg/dL) for those without clinical evidence of ASCVD or other very high-risk conditions [33]. Our result indicated that LDL-C in the upper range of normal is most suitable for reducing the risk of PSCI as well as increasing the likelihood of patients with acute cognitive impairment to recover.
Therefore, our DREAM-LDL bedside tool might be helpful to identify AIS patients at risk of mid- and long-term PSCI as early as possible. Most variables included in our DREAM-LDL risk score were identified by previous studies as important risk factors for PSCI [3, 11–13, 34–39]. Several current available predictive tools input some neuroimaging and techniques [3, 12, 38, 39]. The SIGNAL2 risk score consists of age stages, education<6 years, global cortical atrophy stages, Fazekas stages, non-lacunar cortical infarct stages, chronic lacunes≥2 and intracranial stenosis [12]. The CHANGE risk score includes age, education, cortical atrophy, acute cortical non-lacunar infarcts, white matter hyperintensities (WMH) and chronic lacunes [3]. The GRECogVASC cognitive risk score consists of NIHSS≥7 at admission (≥7), multiple strokes, adjusted MMSE≤27, and Fazekas score≥2 [37]. Finally, Ding et al. developed a PSCI risk model consisting of age, years of education, periventricular hyperintensity grading, diabetes mellitus and the number of acute non-lacunar infarcts as variables [36]. Neuroimaging information is needed for all of these 4 models [3, 12, 36, 37]. Our risk score does not rely on any neuroimaging information, therefore, is simple and easy to administer in intensive stroke unit. Of course, the model needs to be tested and further validated in other AIS patient populations.
Our study has certain limitations. First, it was a 6-month study, therefore how these patients’ cognitive performance would evolve beyond 6 months could not be evaluated. Secondly, only very few of the included patients (11.23%) suffered severe stroke and as such, the effect of severity of stroke on the risk of PSCI and patients’ likelihood to recover could not be adequately evaluated. However, it was the nature or limit of a retrospective study. Thirdly, we used a MoCA cutoff value of 22 in the current study for estimating prevalence of PSCI and for building the predicting model for PSCI. which was lower than mean MoCA score of old healthy subjects reported by many studies [40–45]. Fourthly, the MoCA testing was originally designed for detecting mild cognitive impairment, but not for PSCI and therefore it does not include assessment of some of the cognitive deficits commonly seen after stroke such as aphasia, neglect, visual loss, apraxia and reading/writing problems [46–48]. However, up till now, the MoCA test is still the commonly used bedside screening tool for PSCI. Therefore, it should be assumed that AIS patients with severe stroke symptoms incapable of completing the MoCA testing were at high risk of developing PSCI.
In conclusion, PSCI was common among AIS survivor 6 months after AIS. Our finding provided a tool for early identification of AIS patients at high risk of developing PSCI.
Author Contributions
Y.D. performed data analysis, drafted the manuscript. M.Y.D., M.C., M.F., L.G., Z.J.X, Y.Z., X.Z.W. and X.F.X participated in patient assessment, data collection. Y.D., X.Y.L., Y.W.Z. and G.L participated in the study design and revised the manuscript. Q.D. was in charge of the study conception, supervised the analysis and finalized the manuscript. All authors have reviewed and approved the submitted version and have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Conflicts of Interest
The funder had no role in study design, data collection and analysis, or writing of this study. There were no other conflicts of interests.
Funding
This study was funded by Eisai China Inc.
References
- 1. Qu Y, Zhuo L, Li N, Hu Y, Chen W, Zhou Y, Wang J, Tao Q, Hu J, Nie X, Zhan S. Prevalence of post-stroke cognitive impairment in China: a community-based, cross-sectional study. PLoS One. 2015; 10:e0122864. https://doi.org/10.1371/journal.pone.0122864 [PubMed]
- 2. Tang EY, Amiesimaka O, Harrison SL, Green E, Price C, Robinson L, Siervo M, Stephan BC. Longitudinal Effect of Stroke on Cognition: A Systematic Review. J Am Heart Assoc. 2018; 7:e006443. https://doi.org/10.1161/JAHA.117.006443 [PubMed]
- 3. Chander RJ, Lam BY, Lin X, Ng AY, Wong AP, Mok VC, Kandiah N. Development and validation of a risk score (CHANGE) for cognitive impairment after ischemic stroke. Sci Rep. 2017; 7:12441. https://doi.org/10.1038/s41598-017-12755-z [PubMed]
- 4. Chaurasia RN, Sharma J, Pathak A, Mishra VN, Joshi D. Poststroke Cognitive Decline: A Longitudinal Study from a Tertiary Care Center. J Neurosci Rural Pract. 2019; 10:459–64. https://doi.org/10.1055/s-0039-1697872 [PubMed]
- 5. Zhou DH, Wang JY, Li J, Deng J, Gao C, Chen M. Frequency and risk factors of vascular cognitive impairment three months after ischemic stroke in China: the Chongqing stroke study. Neuroepidemiology. 2005; 24:87–95. https://doi.org/10.1159/000081055 [PubMed]
- 6. Tu Q, Ding B, Yang X, Bai S, Tu J, Liu X, Wang R, Tao J, Jin H, Wang Y, Tang X. The current situation on vascular cognitive impairment after ischemic stroke in Changsha. Arch Gerontol Geriatr. 2014; 58:236–47. https://doi.org/10.1016/j.archger.2013.09.006 [PubMed]
- 7. Lim JS, Oh MS, Lee JH, Jung S, Kim C, Jang MU, Lee SH, Kim YJ, Kim Y, Park J, Kang Y, Yu KH, Lee BC. Prediction of post-stroke dementia using NINDS-CSN 5-minute neuropsychology protocol in acute stroke. Int Psychogeriatr. 2017; 29:777–84. https://doi.org/10.1017/S1041610216002520 [PubMed]
- 8. Turunen KE, Laari SP, Kauranen TV, Uimonen J, Mustanoja S, Tatlisumak T, Poutiainen E. Domain-Specific Cognitive Recovery after First-Ever Stroke: A 2-Year Follow-Up. J Int Neuropsychol Soc. 2018; 24:117–27. https://doi.org/10.1017/S1355617717000728 [PubMed]
- 9. Rasquin SM, Lodder J, Verhey FR. Predictors of reversible mild cognitive impairment after stroke: a 2-year follow-up study. J Neurol Sci. 2005; 229:21–25. https://doi.org/10.1016/j.jns.2004.11.015 [PubMed]
- 10. Salvadori E, Pasi M, Poggesi A, Chiti G, Inzitari D, Pantoni L. Predictive value of MoCA in the acute phase of stroke on the diagnosis of mid-term cognitive impairment. J Neurol. 2013; 260:2220–27. https://doi.org/10.1007/s00415-013-6962-7 [PubMed]
- 11. Sun JH, Tan L, Yu JT. Post-stroke cognitive impairment: epidemiology, mechanisms and management. Ann Transl Med. 2014; 2:80. https://doi.org/10.3978/j.issn.2305-5839.2014.08.05 [PubMed]
- 12. Kandiah N, Chander RJ, Lin X, Ng A, Poh YY, Cheong CY, Cenina AR, Assam PN. Cognitive Impairment after Mild Stroke: Development and Validation of the SIGNAL2 Risk Score. J Alzheimers Dis. 2016; 49:1169–77. https://doi.org/10.3233/JAD-150736 [PubMed]
- 13. Nijsse B, Visser-Meily JM, van Mierlo ML, Post MW, de Kort PL, van Heugten CM. Temporal Evolution of Poststroke Cognitive Impairment Using the Montreal Cognitive Assessment. Stroke. 2017; 48:98–104. https://doi.org/10.1161/STROKEAHA.116.014168 [PubMed]
- 14. De Silva DA, Woon FP, Pin LM, Chen CP, Chang HM, Wong MC. Intracranial large artery disease among OCSP subtypes in ethnic South Asian ischemic stroke patients. J Neurol Sci. 2007; 260:147–49. https://doi.org/10.1016/j.jns.2007.04.020 [PubMed]
- 15. Zhang Y, Zhang Z, Yang B, Li Y, Zhang Q, Qu Q, Wang Y, Zhang S, Yue W, Tan Y, Zhang B, Xu T. Incidence and risk factors of cognitive impairment 3 months after first-ever stroke: a cross-sectional study of 5 geographic areas of China. J Huazhong Univ Sci Technolog Med Sci. 2012; 32:906–11. https://doi.org/10.1007/s11596-012-1056-9 [PubMed]
- 16. Williamson JB, Nyenhuis DL, Pedelty L, Byrd S, Jhaveri M, Wang C, deToledo-Morrell L, Sripathirathan K, Gorelick P. Baseline differences between vascular cognitive impairment no dementia reverters and non-reverters. J Neurol Neurosurg Psychiatry. 2008; 79:1208–14. https://doi.org/10.1136/jnnp.2007.137554 [PubMed]
- 17. Yoon JA, Kim DY, Sohn MK, Lee J, Lee SG, Lee YS, Han EY, Joo MC, Oh GJ, Han J, Park M, Park KP, Noh KH, et al. Factors associated with improvement or decline in cognitive function after an ischemic stroke in Korea: the Korean stroke cohort for functioning and rehabilitation (KOSCO) study. BMC Neurol. 2017; 17:9. https://doi.org/10.1186/s12883-016-0780-3 [PubMed]
- 18. He Q, Li Q, Zhao J, Wu T, Ji L, Huang G, Ma F. Relationship between plasma lipids and mild cognitive impairment in the elderly Chinese: a case-control study. Lipids Health Dis. 2016; 15:146. https://doi.org/10.1186/s12944-016-0320-6 [PubMed]
- 19. Kálmán J, Kudchodkar BJ, Murray K, McConathy WJ, Juhász A, Janka Z, Lacko AG. Evaluation of serum-lipid-related cardiovascular risk factors in Alzheimer’s disease. Dement Geriatr Cogn Disord. 1999; 10:488–93. https://doi.org/10.1159/000017195 [PubMed]
- 20. Liu Y, Zhong X, Shen J, Jiao L, Tong J, Zhao W, Du K, Gong S, Liu M, Wei M. Elevated serum TC and LDL-C levels in Alzheimer’s disease and mild cognitive impairment: A meta-analysis study. Brain Res. 2020; 1727:146554. https://doi.org/10.1016/j.brainres.2019.146554 [PubMed]
- 21. Lv YB, Yin ZX, Chei CL, Brasher MS, Zhang J, Kraus VB, Qian F, Shi XM, Matchar DB, Zeng Y. Serum Cholesterol Levels within the High Normal Range Are Associated with Better Cognitive Performance among Chinese Elderly. J Nutr Health Aging. 2016; 20:280–87. https://doi.org/10.1007/s12603-016-0701-6 [PubMed]
- 22. Moroney JT, Tang MX, Berglund L, Small S, Merchant C, Bell K, Stern Y, Mayeux R. Low-density lipoprotein cholesterol and the risk of dementia with stroke. JAMA. 1999; 282:254–60. https://doi.org/10.1001/jama.282.3.254 [PubMed]
- 23. Reitz C, Tang MX, Luchsinger J, Mayeux R. Relation of plasma lipids to Alzheimer disease and vascular dementia. Arch Neurol. 2004; 61:705–14. https://doi.org/10.1001/archneur.61.5.705 [PubMed]
- 24. Reitz C, Tang MX, Manly J, Schupf N, Mayeux R, Luchsinger JA. Plasma lipid levels in the elderly are not associated with the risk of mild cognitive impairment. Dement Geriatr Cogn Disord. 2008; 25:232–37. https://doi.org/10.1159/000115847 [PubMed]
- 25. Romero-Sevilla R, Casado-Naranjo I, Portilla-Cuenca JC, Duque-de San Juan B, Fuentes JM, Lopez-Espuela F. Vascular Risk Factors and Lesions of Vascular Nature in Magnetic Resonance as Predictors of Progression to Dementia in Patients with Mild Cognitive Impairment. Curr Alzheimer Res. 2018; 15:671–78. https://doi.org/10.2174/1567205015666180119100840 [PubMed]
- 26. Sparks DL, Kryscio RJ, Connor DJ, Sabbagh MN, Sparks LM, Lin Y, Liebsack C. Cholesterol and cognitive performance in normal controls and the influence of elective statin use after conversion to mild cognitive impairment: results in a clinical trial cohort. Neurodegener Dis. 2010; 7:183–86. https://doi.org/10.1159/000295660 [PubMed]
- 27. West R, Beeri MS, Schmeidler J, Hannigan CM, Angelo G, Grossman HT, Rosendorff C, Silverman JM. Better memory functioning associated with higher total and low-density lipoprotein cholesterol levels in very elderly subjects without the apolipoprotein e4 allele. Am J Geriatr Psychiatry. 2008; 16:781–85. https://doi.org/10.1097/JGP.0b013e3181812790 [PubMed]
- 28. Yin ZX, Shi XM, Kraus VB, Fitzgerald SM, Qian HZ, Xu JW, Zhai Y, Sereny MD, Zeng Y. High normal plasma triglycerides are associated with preserved cognitive function in Chinese oldest-old. Age Ageing. 2012; 41:600–06. https://doi.org/10.1093/ageing/afs033 [PubMed]
- 29. Zhou F, Deng W, Ding D, Zhao Q, Liang X, Wang F, Luo J, Zheng L, Guo Q, Hong Z. High Low-Density Lipoprotein Cholesterol Inversely Relates to Dementia in Community-Dwelling Older Adults: The Shanghai Aging Study. Front Neurol. 2018; 9:952. https://doi.org/10.3389/fneur.2018.00952 [PubMed]
- 30. Zou Y, Zhu Q, Deng Y, Duan J, Pan L, Tu Q, Dai R, Zhang X, Chu LW, Lü Y. Vascular risk factors and mild cognitive impairment in the elderly population in Southwest China. Am J Alzheimers Dis Other Demen. 2014; 29:242–47. https://doi.org/10.1177/1533317513517042 [PubMed]
- 31. Presećki P, Mück-Seler D, Mimica N, Pivac N, Mustapić M, Stipcević T, Smalc VF. Serum lipid levels in patients with Alzheimer’s disease. Coll Antropol. 2011 (Suppl 1); 35:115–20. [PubMed]
- 32. Lo JW, Crawford JD, Desmond DW, Godefroy O, Jokinen H, Mahinrad S, Bae HJ, Lim JS, Köhler S, Douven E, Staals J, Chen C, Xu X, et al, and Stroke and Cognition (STROKOG) Collaboration. Profile of and risk factors for poststroke cognitive impairment in diverse ethnoregional groups. Neurology. 2019; 93:e2257–71. https://doi.org/10.1212/WNL.0000000000008612 [PubMed]
- 33. Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, Wilson DP, Brown WV. National lipid association recommendations for patient-centered management of dyslipidemia: part 1--full report. J Clin Lipidol. 2015; 9:129–69. https://doi.org/10.1016/j.jacl.2015.02.003 [PubMed]
- 34. Jacquin A, Binquet C, Rouaud O, Graule-Petot A, Daubail B, Osseby GV, Bonithon-Kopp C, Giroud M, Béjot Y. Post-stroke cognitive impairment: high prevalence and determining factors in a cohort of mild stroke. J Alzheimers Dis. 2014; 40:1029–38. https://doi.org/10.3233/JAD-131580 [PubMed]
- 35. Zietemann V, Georgakis MK, Dondaine T, Müller C, Mendyk AM, Kopczak A, Hénon H, Bombois S, Wollenweber FA, Bordet R, Dichgans M. Early MoCA predicts long-term cognitive and functional outcome and mortality after stroke. Neurology. 2018; 91:e1838–50. https://doi.org/10.1212/WNL.0000000000006506 [PubMed]
- 36. Ding MY, Xu Y, Wang YZ, Li PX, Mao YT, Yu JT, Cui M, Dong Q. Predictors of Cognitive Impairment After Stroke: A Prospective Stroke Cohort Study. J Alzheimers Dis. 2019; 71:1139–51. https://doi.org/10.3233/JAD-190382 [PubMed]
- 37. Godefroy O, Yaïche H, Taillia H, Bompaire F, Nédélec-Ciceri C, Bonnin C, Varvat J, Vincent-Grangette F, Diouf M, Mas JL, Canaple S, Lamy C, Arnoux A, et al, and GRECogVASC Study Group. Who should undergo a comprehensive cognitive assessment after a stroke? A cognitive risk score. Neurology. 2018; 91:e1979–87. https://doi.org/10.1212/WNL.0000000000006544 [PubMed]
- 38. Chaudhari TS, Verma R, Garg RK, Singh MK, Malhotra HS, Sharma PK. Clinico-radiological predictors of vascular cognitive impairment (VCI) in patients with stroke: a prospective observational study. J Neurol Sci. 2014; 340:150–58. https://doi.org/10.1016/j.jns.2014.03.018 [PubMed]
- 39. Kopecek M, Stepankova H, Lukavsky J, Ripova D, Nikolai T, Bezdicek O. Montreal cognitive assessment (MoCA): Normative data for old and very old Czech adults. Appl Neuropsychol Adult. 2017; 24:23–29. https://doi.org/10.1080/23279095.2015.1065261 [PubMed]
- 40. Larouche E, Tremblay MP, Potvin O, Laforest S, Bergeron D, Laforce R, Monetta L, Boucher L, Tremblay P, Belleville S, Lorrain D, Gagnon JF, Gosselin N, et al. Normative Data for the Montreal Cognitive Assessment in Middle-Aged and Elderly Quebec-French People. Arch Clin Neuropsychol. 2016; 31:819–26. https://doi.org/10.1093/arclin/acw076 [PubMed]
- 41. Lu J, Li D, Li F, Zhou A, Wang F, Zuo X, Jia XF, Song H, Jia J. Montreal cognitive assessment in detecting cognitive impairment in Chinese elderly individuals: a population-based study. J Geriatr Psychiatry Neurol. 2011; 24:184–90. https://doi.org/10.1177/0891988711422528 [PubMed]
- 42. Malek-Ahmadi M, Powell JJ, Belden CM, O’Connor K, Evans L, Coon DW, Nieri W. Age- and education-adjusted normative data for the Montreal Cognitive Assessment (MoCA) in older adults age 70-99. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2015; 22:755–61. https://doi.org/10.1080/13825585.2015.1041449 [PubMed]
- 43. Mellor D, Lewis M, McCabe M, Byrne L, Wang T, Wang J, Zhu M, Cheng Y, Yang C, Dong S, Xiao S. Determining appropriate screening tools and cut-points for cognitive impairment in an elderly Chinese sample. Psychol Assess. 2016; 28:1345–53. https://doi.org/10.1037/pas0000271 [PubMed]
- 44. Narazaki K, Nofuji Y, Honda T, Matsuo E, Yonemoto K, Kumagai S. Normative data for the montreal cognitive assessment in a Japanese community-dwelling older population. Neuroepidemiology. 2013; 40:23–29. https://doi.org/10.1159/000339753 [PubMed]
- 45. Tan JP, Li N, Gao J, Wang LN, Zhao YM, Yu BC, Du W, Zhang WJ, Cui LQ, Wang QS, Li JJ, Yang JS, Yu JM, et al. Optimal cutoff scores for dementia and mild cognitive impairment of the Montreal Cognitive Assessment among elderly and oldest-old Chinese population. J Alzheimers Dis. 2015; 43:1403–12. https://doi.org/10.3233/JAD-141278 [PubMed]
- 46. Cameron JD, Gallagher R, Pressler SJ, McLennan SN, Ski CF, Tofler G, Thompson DR. Sensitivity and Specificity of a Five-Minute Cognitive Screening Test in Patients With Heart Failure. J Card Fail. 2016; 22:99–107. https://doi.org/10.1016/j.cardfail.2015.08.343 [PubMed]
- 47. Demeyere N, Riddoch MJ, Slavkova ED, Jones K, Reckless I, Mathieson P, Humphreys GW. Domain-specific versus generalized cognitive screening in acute stroke. J Neurol. 2016; 263:306–15. https://doi.org/10.1007/s00415-015-7964-4 [PubMed]
- 48. Benaim C, Barnay JL, Wauquiez G, Bonnin-Koang HY, Anquetil C, Pérennou D, Piscicelli C, Lucas-Pineau B, Muja L, le Stunff E, de Boissezon X, Terracol C, Rousseaux M, et al. The Cognitive Assessment scale for Stroke Patients (CASP) vs. MMSE and MoCA in non-aphasic hemispheric stroke patients. Ann Phys Rehabil Med. 2015; 58:78–85. https://doi.org/10.1016/j.rehab.2014.12.001 [PubMed]