



Introduction
Over the past decades, the incidence of thyroid cancer has increased markedly worldwide. In the United States, the yearly incidence tripled during the past 30 years [1]. Moreover, in China it has became the fifth most common cancer [2]. This increment can be partly ascribed to the rapid development and widely use of sonography techniques. However, it can not explain all, especially macrocarcinoma. Nowadays, the known risk factors for thyroid carcinoma include the head and neck radioactive exposure, female, advanced age, iodine deficiency or excessive and family history of thyroid carcinoma [3, 4]. Unfortunately, most of these are ineluctable. Recently, some scientists proposed that insulin resistance or hyperinsulinemia might be associated with thyroid carcinoma [5–11]. The homeostatic model assessment of insulin resistance (HOMA-IR) was used to calculate and determine if insulin resistance. The specific calculation equation is as follows: HOMA-IR = Fasting Serum Insulin (μIU/ml) • Fasting Plasma Glucose (mmol/l) / 22.5. It has been shown that insulin resistance is significantly associated with a larger thyroid volume and higher prevalence of thyroid nodules [12]. The association between insulin resistance or hyperinsulinemia and thyroid carcinoma has been reported by some studies [5–11], while others did not found the relationship [13–17]. Whether insulin resistance or hyperinsulinemia is related to thyroid carcinoma is still inconsistent. So, this study plans to investigate the association between insulin resistance and thyroid carcinoma, thus propose insulin resistance as a risk factor.
Results
Search results and characteristics of included studies
1278 relevant articles were collected after preliminary screening. Sixty-one articles were selected for full-text review after screening the abstract. Finally, 14 articles were included in this study. Figure 1 showed the details of systematic search process. Of these included 14 studies, three are published in Chinese [10, 11, 17] and the rest are all published in English [5–9, 13–16, 18, 19]. Four studies were conducted in Turkey and three in China. The rest countries including Italy, Argentina, Nepal, Korea and Iran, each has one study. Totally, there are 2024 patients with thyroid carcinoma in case group, and 1460 persons in control group which including healthy controls and patients with benign thyroid diseases. The sample size in case group ranges from 20 to 735 while 20 to 537 in control group. Patients in case group were diagnosed with histopathological. Among which, five studies reported the relationship between insulin resistance and PTC, and the rest seven reported the DTC. Table 1 summarized the detailed characteristics of these 14 studies.
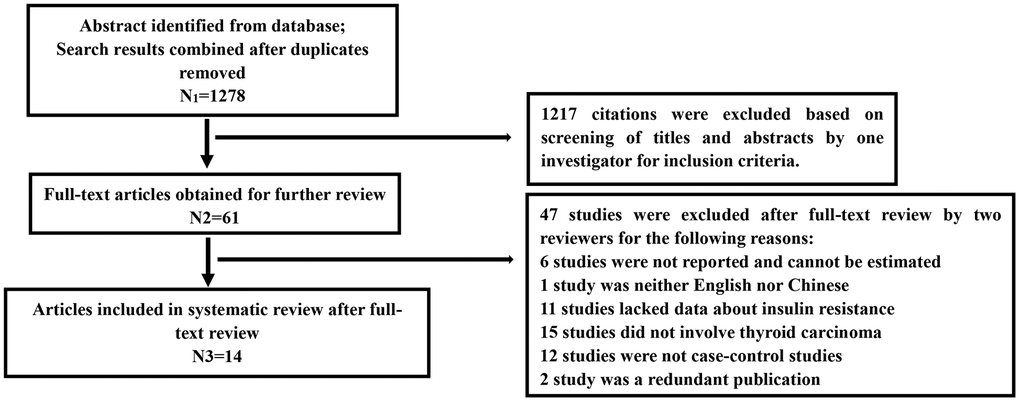
Figure 1. Flow chart of the systematic search process.
Table 1. Characteristic of 14 included studies.
| First author, year | Country | Pathological type | Source of controls | Number of participants, n | Mean age, year | Female (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cases | Control | Cases | Control | Cases | Control | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Massimo Giusti, 2008 | Italy | DTC | Outpatients who had undergone thyroid surgery for benign thyroid diseases. | 96 | 87 | 57.0±13.7 | 56.5±15.9 | 80 | 90 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jorge N. Rezzonico, 2009 | Argentina | DTC | Normal thyroid function, normal thyroid gland palpation, negative titers of antithyroid antibodies and normal thyroid ultrasonography. | 20 | 20 | 46.1±13.6 | 46.7±13.3 | 100 | 100 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ankush Mittal, 2012 | Nepal | DTC | Normal healthy controls. | 50 | 50 | 58.9±11.0 | 57.6±10.0 | 76 | 76 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mustafa Sahin, 2013 | Turkey | DTC | Not mentioned. | 344 | 116 | 45.5±11 | 44.9±8 | 84 | 85 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fevzi Balkan, 2014 | Turkey | DTC | Euthyroid patients with nodular goiter who underwent surgery. | 41 | 41 | 43.7±10.4 | 47.3±10.9 | 90 | 90 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Musrafa Akker, 2014 | Turkey | DTC | Subjects without a history of cancer, determined by thyroid ultrasonography not to have a thyroid nodule, or found to be cancer free following thyroid surgery. | 93 | 111 | 50.2±12.2 | 36.9±9.8 | 85 | 57 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wang Dan, 2014 | China | PTC | Benign thyroid nodule. | 50 | 49 | 46.68±12.72 | 49.40±11.10 | 68 | 80 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Min Jung Bae, 2016 | Korea | PTC | No definite nodules or showed a typical nodule that was benign-looking in nature, and benign results after fine-needle aspiration cytology. | 735 | 537 | 50.2±11.1 | 48.7±9.8 | Not mentioned. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jiang Yanyan, 2016 | China | PTC | Normal healthy controls. | 358 | 290 | 44.0±11.8 | 43.9±14.0 | 78 | 66 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Wo Xiaoyan, 2017 | China | PTC | Benign thyroid nodule. | 153 | 105 | 45.67±11.61 | 48.42±11.85 | 76 | 76 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bekir Ucan, 2017 | Turkey | PTC | Age-, sex-, and body mass index-matched controls. | 54 | 24 | 42.4±10 | 42.5±9 | 87 | 75 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Zahra Heidari, 2017 | Iran | DTC | Healthy euthyroid control participants were chosen with normal thyroid sonography. | 30 | 30 | 34.4±12.7 | 34.1±12.8 | 80 | 80 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Guo XY, 2019 | China | PTC | Benign thyroid nodule. | 153 | 105 | 45.7±11.6 | 48.4±11.9 | 76 | 76 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mele Chiara, 2019* | Italy | DTC | Benign thyroid nodule and healthy control. | 30 | 27; 20 | 50.0 (41.0-58.8) | 56.0 (53.5-65.0); 47.0 (37.0-62.5) | 70 | 85; 75 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DTC, Differentiated Thyroid Carcinoma; PTC, Papillary Thyroid Carcinoma; *Data are expressed as the median (interquartile range); The rest data are expressed as the mean ± standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Quality of included studies
Methodological quality of the case-control study was evaluated by NOS scores. Table 2 summarized the results of quality assessment of these 14 studies. Case control studies that achieved five scores or above were considered as a high quality study. As a result, all of these included studies were high quality.
Table 2. Quality assessment according to the Newcastle-Ottawa scale.
| First author, year | Section | Comparability | Exposure | Total |
| Massimo Giusti, 2008 | 3 | 0 | 3 | 6 |
| Jorge N. Rezzonico, 2009 | 3 | 1 | 3 | 7 |
| Ankush Mittal, 2012 | 2 | 1 | 3 | 6 |
| Mustafa Sahin, 2013 | 3 | 0 | 3 | 6 |
| Fevzi Balkan, 2014 | 3 | 2 | 3 | 8 |
| Musrafa Akker, 2014 | 3 | 1 | 3 | 7 |
| Wang Dan, 2014 | 3 | 0 | 3 | 6 |
| Min Jung Bae, 2016 | 3 | 0 | 3 | 6 |
| Jiang Yanyan, 2016 | 3 | 0 | 3 | 6 |
| Wo Xiaoyan, 2017 | 3 | 0 | 3 | 6 |
| Bekir Ucan, 2017 | 3 | 1 | 3 | 7 |
| Zahra Heidari, 2017 | 2 | 2 | 3 | 7 |
| Guo XY, 2019 | 3 | 1 | 3 | 7 |
| Mele Chiara, 2019 | 3 | 1 | 3 | 7 |
Level of fasting serum insulin and thyroid carcinoma
Thirteen studies reported the level of fasting serum insulin [5–9, 11, 13–19]. Fixed-effect model was used to merge the WMD and pooled effect size is 1.24 (95% CI 1.08 to 1.40, P<0.00001), which showed that thyroid carcinoma patients have a higher level of fasting serum insulin than controls. Subgroup analysis with fixed-effect model was done by the different original of control participants that including benign nodule diseases, normal control and not mentioned. All the three subgroups show a significantly higher level of fasting serum insulin in the group of thyroid carcinoma (Figure 2). The pooled WMD in subgroup of benign nodule diseases is 1.55 (95% CI 0.85 to 2.25, P<0.0001) and no significant heterogeneity was detected (heterozygosity test, Chi2=3.4, P=0.64, I2= 0%). The pooled WMD values is 0.86 in subgroup of normal control (95%CI 0.52 to 1.20), whereas, a high heterogeneity was calculated (heterozygosity test, Chi2=22.32, P=0.001, I2= 73%). In conclusion, the level of fasting serum insulin in thyroid carcinoma patients is statistically significant increased compared to persons without thyroid carcinoma.
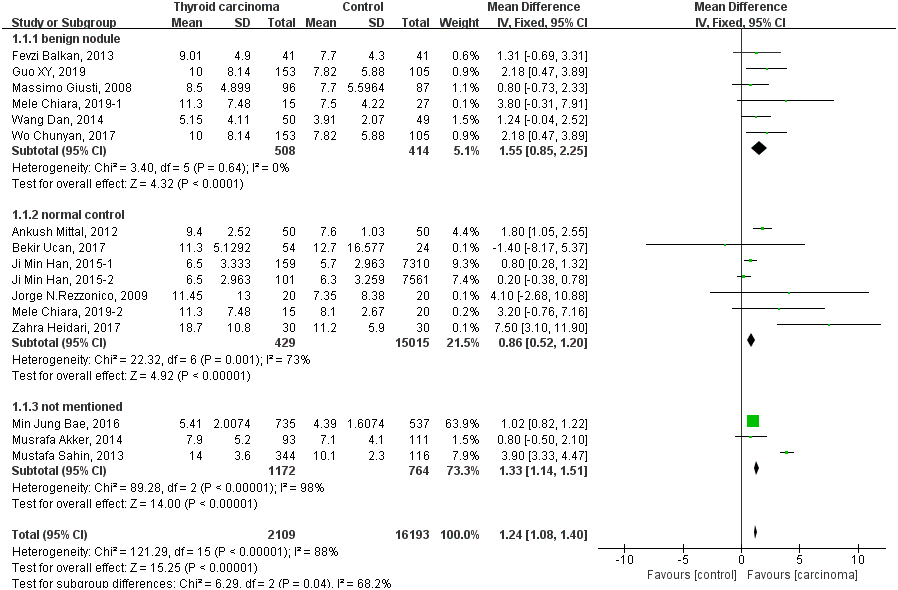
Figure 2. Forest plot of the fasting serum insulin level in patients with thyroid carcinoma.
HOMA-IR and thyroid carcinoma
Thirteen studies analyze the relationship between HOMA-IR and thyroid carcinoma [5, 7–11, 13–19]. Random-effect model was used to estimate pooled WMD. The pooled WMD is 0.56 (95% CI 0.34 to 0.78, P<0.00001), whereas heterogeneity was detected between included studies (heterozygosity test, Chi2=275.10, P<0.00001, I2= 96%) and the results showed in Figure 3. That means a higher HOMA-IR is related to a high incidence of thyroid carcinoma.
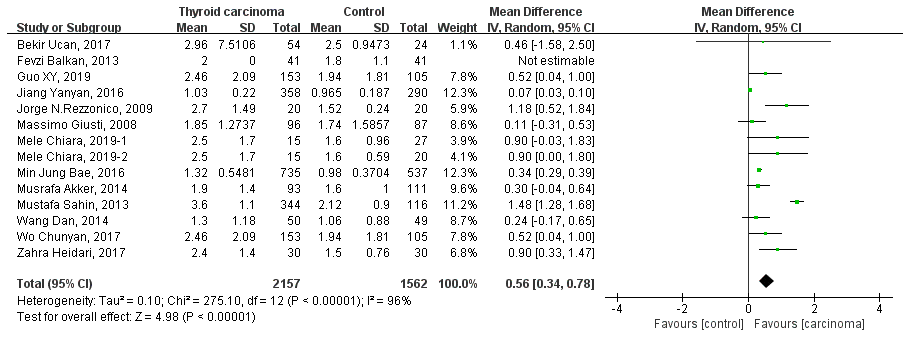
Figure 3. Forest plot of HOMA-IR in patients with thyroid carcinoma.
Insulin resistance and risk of thyroid carcinoma
Four studies reported the association of insulin resistance with the risk of thyroid carcinoma [5, 7, 9, 15]. Fixed-effect model was used to estimate pooled OR. The pooled OR is 3.16 (95% CI 2.09 to 4.77, P<0.0001) and showed in Figure 4. Whereas, a heterogeneity was detected between these four studies (heterozygosity test, Chi2=5.23, P=0.16, I2= 43%). In sum, insulin resistance increase the risk of thyroid carcinoma 216% compared with participants without insulin resistance.
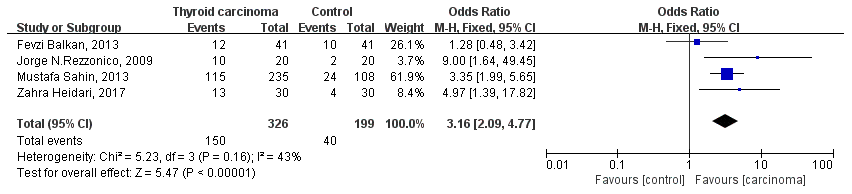
Figure 4. Forest plot of insulin resistance and risk of thyroid carcinoma.
Publication bias
Funnel plot, a method for qualitative evaluation of publication bias, was done in this meta-analysis. All the studies are symmetry distributed at the top of the funnel plot made with review manage by visual observation (Figure 5A). We use stata16.0 software to detect publication bias, as shown in Figure 5B, the results show that there is no publication bias (Egger`s test P=0.565). According to the results showed above, there was no obvious publication bias in the included studies.
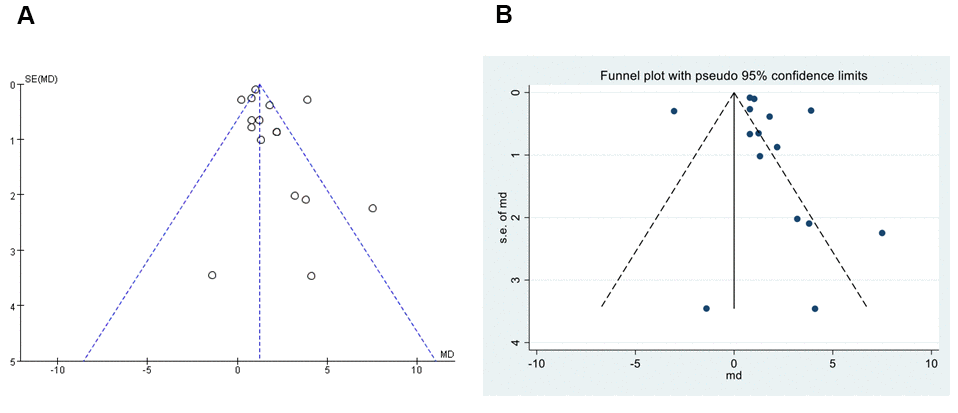
Figure 5. Funnel plot of publication bias. (A) Funnel plot, qualitative evaluation of publication bias, performed by Review Manager 5.3. (B) Egger`s test, quantitatively measurement of publication bias, performed by Stata16.0.
Discussion
The incidence of thyroid carcinoma has been markedly increased all over the word [2, 20, 21], therefore the risk factor of thyroid carcinoma attracting more and more attentions, especially the risk factors that can be prevented. Recently, insulin resistance [5, 7], obesity [22, 23], diabetic mellitus [24, 25] and other metabolic index have been found to be associated with higher incidence of thyroid carcinoma.
Whereas, the role of insulin resistance in carcinogenesis is still debatable [9, 15]. Previous studies have reported that the level of fasting serum insulin is higher in thyroid carcinoma patients than controls [5–11]. However, other studies did not show the same result [13–17]. We conducted this meta-analysis and finally concluded that insulin resistance and hyperinsulinemia might be a risk factor for thyroid carcinoma.
Insulin resistance has been reported to be a risk factor in many kinds of cancers, such as melanoma, endometrial, hepatocellular, colorectal, breast and even lung cancer [26–32]. In addition, it is also found to be associated with nodular thyroid disease [28]. Insulin resistance is generally paralleled by hyperinsulinemia. Insulin that beyond physiological dosage can promote thyroid cell growth, thus it can lead a carcinogenesis in patients with some benign thyroid diseases [33]. Furthermore, hyperinsulinemia can affect the metabolism of energy by increasing glucose uptake of cells, which can active some signal transduction pathway in cells, causing an excessive proliferation, and even promote the carcinogenesis and development of malignant tumors. The tumor markers in patients with hyperinsulinemia and normal control have already been detected. Moreover, it was found that proto-oncogene, such as human epidermal growth factor receptor-2 and B-cell lymphoma-2, were highly expressed, meanwhile tumor suppressor gene (p 53) was significantly decreased in patients with hyperinsulinemia [33]. In a word, it is reasonable speculate that insulin resistance or hyperinsulinemia may be the risk factor for thyroid carcinoma.
Nowadays, the mechanisms by which insulin exerts the carcinogenesis efficiency mainly focus on the study of insulin-like growth factor-1 (IGF-1). IGF-1, IGF-1 receptor and insulin receptors has been found in thyroid carcinoma, hyperinsulinemia and insulin resistance were also found to play a role of carcinogenesis [34]. Insulin shares structural homology with IGF-1 and thus it can bind to the IGF-1 receptor, thus participating in thyroid stimulating hormone -mediated proliferation of thyroid cells [35]. Liu et al. found that comparing with normal healthy population, the expression of IGF-1 and IGF-1 receptor in patients with follicular thyroid tumor, nodular goiter and papillary thyroid cancer were significantly higher [36]. It was supposed that the role of insulin in promoting the formation of thyroid nodule may be partially mediated by the proliferation effective of IGF-1. Moreover, hyperinsulinemia can induce mitotic and anti-apoptotic effects by acting on the IGF-1 receptor, protein kinase B, mammalian target of rapamycin and other signal transduction pathways [37]. From the previous research results, the mechanisms of hyperinsulin-induced carcinogenesis are not completely clear and needs further study.
It is reported that a reduced risk of thyroid nodules and decreased thyroid volume and nodule size were found when insulin resistance was decreased by metformin [38, 39]. And metformin can also inhibit the growth and migration of thyroid cancer cells, inhibit the self-renewal of tumor stem cells, and enhance the effect of chemotherapeutic drugs [40, 41]. Moreover, as an insulin-sensitizing agent, metformin was supposed to reduce the risk of thyroid cancer in Taiwanese type 2 diabetes mellitus patients [42]. Therefore, it is reasonable to suppose that insulin resistance or hyperinsulinemia was the risk factor for thyroid carcinoma.
There are some limitations in this meta-analysis: (1) results of insulin resistance were reported in only four studies, not all fourteen; (2) the cut-off level of insulin resistance were not consistent across these studies, which also caused some variation in results Meanwhile, the source of control groups in different studies were diversity, which may induce the heterogeneity and influence the results. Even so, we can still assume that insulin resistance is associated with an increased risk of thyroid carcinoma.
Conclusions
The association between insulin resistance and thyroid carcinoma was summarized in this meta-analysis. Both high level of fasting serum insulin and insulin resistance are associated with increased risk of thyroid carcinoma. Thus, it can conclude that insulin resistance might be a risk factor for thyroid carcinoma. Due to the current limitations of this meta-analysis that described above, we believe that more prospective clinical studies with a large sample size may strengthen our conclusions. Meanwhile, more researches are needed to further elucidate the mechanism of insulin resistance causing increased risk of thyroid carcinoma.
Materials and Methods
Searching progress
We searched for case-control studies that focus on thyroid carcinoma and insulin resistance simultaneously in the following databases: PubMed, Cochrane library, Sinomed, CNKI and Wanfang. The literature retrieval time limitation was: from the earliest data to 1 February, 2021. We used the following search terms for literature retrieval in the database: (“insulin resistance” or “IR” or “hyperinsulinemia” or “hyperinsulinaemia” or “hyperinsulinism” or “hyperinsulinism”) and (“thyroid cancer*” or “thyroid neoplasm*” or “thyroid tumor” or “thyroid carcinoma*” or “differentiated thyroid carcinoma” or “DTC” or “Papillary thyroid carcinoma” or “Thyroid carcinoma, papillary” or “PTC” or “Thyroid cancer, follicular” or “FTC” or “Thyroid Carcinoma, Anaplastic” or “ATC” or “Thyroid cancer, medullary” or “MTC”). Reference to all articles which considered for inclusion and related reviews, systematic review, etc. are also hand searched. We also searched the clinical trial register centers (http://www.clinicaltrials.gov) for clinical studies on this topic. The literature search was restricted to published (databases) or publicized (clinical trial register centers) results.
Inclusion criteria for this meta-analysis: (1) study that published in English or Chinese language; (2) study focused on the association between insulin resistance or hypersinulinemia and thyroid carcinoma; (3) study type was a case-control study; (4) at least one of the three outcomes was reported: the level of fasting serum insulin, HOMA-IR and the incidence of insulin resistance in patients with thyroid carcinoma. Articles that do not meet the inclusion criteria above will not be included in this meta-analysis.
Study selection and data extraction
Two authors screened the literature and extracted the data independently. If there is any disagreement, the two authors will discuss it and decide. If discussions fail to resolve the doubt, a third, more experienced author (corresponding author) decides finally. The following information was extracted from the included studies: (1) characteristic of populations, including the pathological type of thyroid carcinoma, source of controls (benign thyroid diseases, healthy control, etc.), mean age and gender; (2) the results, including the fasting serum insulin level, HOMA-IR and the incidence of insulin resistance in patients with thyroid carcinoma.
Methodological quality assessment
Newcastle-Ottawa Scale (NOS) was used to assess the methodological quality by two authors independently. If any disagreement, discuss and redecide. In the category of “Selection” and “Exposure”, each numered item can scored one star if the study meet the condition. While two stars can be got in the category of “Comparability”. Nine score is highest and shows a highest quality. This study has been conducted according to the PRISMA guideline and we have registered in INPLASY website, the registration number is INPLASY202180043 and the DOI number is 10.37766/inplasy2021.8.0043.
Statistical analysis
The outcomes include the level of fasting serum insulin, HOMA-IR, the incidence of insulin resistance in patients with thyroid cancer. Fixed-model or random-model was performed by weighted mean difference (WMD), standardized mean difference (SMD) and 95% confidence intervals (CI) for continuous variables. Fixed-model performed by computing odds ratio (OR) and 95%CI for dichotomous variables. The heterogeneity of the included studies was evaluated by calculating I2. The analyses were performed by Review Manager 5.3 (Cochrane Collaboration, United Kingdom, http://www.cochrane.org) and STATA.
Abbreviations
DTC: differentiated thyroid carcinoma; PTC: Papillary thyroid carcinoma; FTC: Thyroid cancer, follicular; ATC: Thyroid Carcinoma, Anaplastic; MTC: Thyroid cancer, medullary; NOS: Newcastle-Ottawa Scale; WMD: weighted mean difference; SMD: standardized mean difference; CI: confidence intervals; OR: odds ratio; IGF-1: insulin-like growth factor-1.
Author Contributions
JZ, LL and JD designed the study and wrote the manuscript. JZ, QZ and JY performed the literature searches and collected the data. JZ, YY and JY performed the statistical analysis. All authors approved the final content of the manuscript.
Acknowledgments
Thanks for the funding of Projects of Medical and Health Technology Development Program in Shandong Province and Shandong Provincial Natural Science Foundation of China Grants. Thanks to all authors for their efforts in this meta-analysis.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This study was funded by Projects of Medical and Health Technology Development Program in Shandong Province [grant number 2016WS0499], Shandong Provincial Natural Science Foundation of China Grants [grant number ZR2019PH025]. They support the study design; the data collection, analysis and interpretation of data; the writing of the report; and the decision to submit the article for publication.
References
- 1. Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014; 140:317–22. https://doi.org/10.1001/jamaoto.2014.1 [PubMed]
- 2. Zheng R, Zeng H, Zhang S, Chen W. Estimates of cancer incidence and mortality in China, 2013. Chin J Cancer. 2017; 36:66. https://doi.org/10.1186/s40880-017-0234-3 [PubMed]
- 3. Nagataki S, Nyström E. Epidemiology and primary prevention of thyroid cancer. Thyroid. 2002; 12:889–96. https://doi.org/10.1089/105072502761016511 [PubMed]
- 4. Sherman SI. Thyroid carcinoma. Lancet. 2003; 361:501–11. https://doi.org/10.1016/s0140-6736(03)12488-9 [PubMed]
- 5. Rezzónico JN, Rezzónico M, Pusiol E, Pitoia F, Niepomniszcze H. Increased prevalence of insulin resistance in patients with differentiated thyroid carcinoma. Metab Syndr Relat Disord. 2009; 7:375–80. https://doi.org/10.1089/met.2008.0062 [PubMed]
- 6. Mittal A, Poudel B, Pandeya DR, Gupta SP, Sathian B, Yadav SK. Metabolic changes enhance the cardiovascular risk with differentiated thyroid carcinoma--a case control study from Manipal Teaching Hospital of Nepal. Asian Pac J Cancer Prev. 2012; 13:2335–38. https://doi.org/10.7314/apjcp.2012.13.5.2335 [PubMed]
- 7. Sahin M, Uçan B, Giniş Z, Topaloğlu O, Güngüneş A, Bozkurt NÇ, Arslan MS, Ünsal İÖ, Akkaymak ET, Demirci T, Karaköse M, Çalışkan M, Çakal E, et al. Vitamin D3 levels and insulin resistance in papillary thyroid cancer patients. Med Oncol. 2013; 30:589. https://doi.org/10.1007/s12032-013-0589-5 [PubMed]
- 8. Bae MJ, Kim SS, Kim WJ, Yi YS, Jeon YK, Kim BH, Lee BJ, Lee JC, Kim IJ, Wang SG, Kim YK. High prevalence of papillary thyroid cancer in Korean women with insulin resistance. Head Neck. 2016; 38:66–71. https://doi.org/10.1002/hed.23848 [PubMed]
- 9. Heidari Z, Abdani M, Mansournia MA. Insulin Resistance Associated With Differentiated Thyroid Carcinoma: Penalized Conditional Logistic Regression Analysis of a Matched Case-Control Study Data. Int J Endocrinol Metab. 2017; 16:e14545. https://doi.org/10.5812/ijem.14545 [PubMed]
- 10. Yanyan J, Huijuan Z. [Correlation of 25-hydroxy vitaminD3 and insulin resistance with papillary thyroid carcinoma]. Journal of Chongqing Medical University. 2016; 41:1276–79. https://doi.org/10.13406/j.cnki.cyxb.000899
- 11. Wo XY. Correlation between serum insulin levels and papillary thyroid cancer. In: Dalian Medical University. 2017.
- 12. Rezzonico J, Rezzonico M, Pusiol E, Pitoia F, Niepomniszcze H. Introducing the thyroid gland as another victim of the insulin resistance syndrome. Thyroid. 2008; 18:461–64. https://doi.org/10.1089/thy.2007.0223 [PubMed]
- 13. Giusti M, Mortara L, Degrandi R, Cecoli F, Mussap M, Rodriguez G, Ferone D, Minuto F. Metabolic and cardiovascular risk in patients with a history of differentiated thyroid carcinoma: A case-controlled cohort study. Thyroid Res. 2008; 1:2. https://doi.org/10.1186/1756-6614-1-2 [PubMed]
- 14. Akker M, Güldiken S, Sipahi T, Palabıyık O, Tosunoğlu A, Çelik Ö, Tunçbilek N, Sezer A, Süt N. Investigation of insulin resistance gene polymorphisms in patients with differentiated thyroid cancer. Mol Biol Rep. 2014; 41:3541–47. https://doi.org/10.1007/s11033-014-3218-2 [PubMed]
- 15. Balkan F, Onal ED, Usluogullari A, Tuzun D, Ozdemir D, Inancli SS, Ersoy R, Cakir B. “Is there any association between insulin resistance and thyroid cancer? : A case control study”. Endocrine. 2014; 45:55–60. https://doi.org/10.1007/s12020-013-9942-x [PubMed]
- 16. Ucan B, Sahin M, Kizilgul M, Ozbek M, Ozdemir S, Calıskan M, Cakal E. Serum ghrelin levels in papillary thyroid carcinoma. Arch Endocrinol Metab. 2017; 61:464–69. https://doi.org/10.1590/2359-3997000000290 [PubMed]
- 17. Wang D. The relationship between benign or malignant thyroid nodules and insulin resistance. In: Dalian Medical University. 2014.
- 18. Mele C, Samà MT, Bisoffi AA, Caputo M, Bullara V, Mai S, Walker GE, Prodam F, Marzullo P, Aimaretti G, Pagano L. Circulating adipokines and metabolic setting in differentiated thyroid cancer. Endocr Connect. 2019; 8:997–1006. https://doi.org/10.1530/EC-19-0262 [PubMed]
- 19. Guo X, Chen X, Zhang C, Zhang J, Zhang C. Hyperinsulinemia and thyroid peroxidase antibody in Chinese patients with papillary thyroid cancer. Endocr J. 2019; 66:731–37. https://doi.org/10.1507/endocrj.EJ18-0358 [PubMed]
- 20. Jung KW, Won YJ, Oh CM, Kong HJ, Lee DH, Lee KH, and Community of Population-Based Regional Cancer Registries. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2014. Cancer Res Treat. 2017; 49:292–305. https://doi.org/10.4143/crt.2017.118 [PubMed]
- 21. Siegel R, Desantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin. 2014; 64:104–17. https://doi.org/10.3322/caac.21220 [PubMed]
- 22. Pellegriti G, De Vathaire F, Scollo C, Attard M, Giordano C, Arena S, Dardanoni G, Frasca F, Malandrino P, Vermiglio F, Previtera DM, D’Azzò G, Trimarchi F, Vigneri R. Papillary thyroid cancer incidence in the volcanic area of Sicily. J Natl Cancer Inst. 2009; 101:1575–83. https://doi.org/10.1093/jnci/djp354 [PubMed]
- 23. Biondi B, Arpaia D, Montuori P, Ciancia G, Ippolito S, Pettinato G, Triassi M. Under the shadow of vesuvius: a risk for thyroid cancer? Thyroid. 2012; 22:1296–97. https://doi.org/10.1089/thy.2012.0002 [PubMed]
- 24. Yeo Y, Ma SH, Hwang Y, Horn-Ross PL, Hsing A, Lee KE, Park YJ, Park DJ, Yoo KY, Park SK. Diabetes mellitus and risk of thyroid cancer: a meta-analysis. PLoS One. 2014; 9:e98135. https://doi.org/10.1371/journal.pone.0098135 [PubMed]
- 25. Shih SR, Chiu WY, Chang TC, Tseng CH. Diabetes and thyroid cancer risk: literature review. Exp Diabetes Res. 2012; 2012:578285. https://doi.org/10.1155/2012/578285 [PubMed]
- 26. Inoue M, Tsugane S. Insulin resistance and cancer: epidemiological evidence. Endocr Relat Cancer. 2012; 19:F1–8. https://doi.org/10.1530/ERC-12-0142 [PubMed]
- 27. Boyle P, Koechlin A, Pizot C, Boniol M, Robertson C, Mullie P, Bolli G, Rosenstock J, Autier P. Blood glucose concentrations and breast cancer risk in women without diabetes: a meta-analysis. Eur J Nutr. 2013; 52:1533–40. https://doi.org/10.1007/s00394-012-0460-z [PubMed]
- 28. Yasar HY, Ertuğrul O, Ertuğrul B, Ertuğrul D, Sahin M. Insulin resistance in nodular thyroid disease. Endocr Res. 2011; 36:167–74. https://doi.org/10.3109/07435800.2011.593011 [PubMed]
- 29. Soliman PT, Wu D, Tortolero-Luna G, Schmeler KM, Slomovitz BM, Bray MS, Gershenson DM, Lu KH. Association between adiponectin, insulin resistance, and endometrial cancer. Cancer. 2006; 106:2376–81. https://doi.org/10.1002/cncr.21866 [PubMed]
- 30. Antoniadis AG, Petridou ET, Antonopoulos CN, Dessypris N, Panagopoulou P, Chamberland JP, Adami HO, Gogas H, Mantzoros CS. Insulin resistance in relation to melanoma risk. Melanoma Res. 2011; 21:541–46. https://doi.org/10.1097/CMR.0b013e32834b0eeb [PubMed]
- 31. Siddique A, Kowdley KV. Insulin resistance and other metabolic risk factors in the pathogenesis of hepatocellular carcinoma. Clin Liver Dis. 2011; 15:281–96. https://doi.org/10.1016/j.cld.2011.03.007 [PubMed]
- 32. Djiogue S, Nwabo Kamdje AH, Vecchio L, Kipanyula MJ, Farahna M, Aldebasi Y, Seke Etet PF. Insulin resistance and cancer: the role of insulin and IGFs. Endocr Relat Cancer. 2013; 20:R1–17. https://doi.org/10.1530/ERC-12-0324 [PubMed]
- 33. Stoll BA. Premalignant breast lesions: role for biological markers in predicting progression to cancer. Eur J Cancer. 1999; 35:693–97. https://doi.org/10.1016/s0959-8049(99)00026-x [PubMed]
- 34. Vella V, Sciacca L, Pandini G, Mineo R, Squatrito S, Vigneri R, Belfiore A. The IGF system in thyroid cancer: new concepts. Mol Pathol. 2001; 54:121–24. https://doi.org/10.1136/mp.54.3.121 [PubMed]
- 35. Aschebrook-Kilfoy B, Sabra MM, Brenner A, Moore SC, Ron E, Schatzkin A, Hollenbeck A, Ward MH. Diabetes and thyroid cancer risk in the National Institutes of Health-AARP Diet and Health Study. Thyroid. 2011; 21:957–63. https://doi.org/10.1089/thy.2010.0396 [PubMed]
- 36. Liu YJ, Qiang W, Shi J, Lv SQ, Ji MJ, Shi BY. Expression and significance of IGF-1 and IGF-1R in thyroid nodules. Endocrine. 2013; 44:158–64. https://doi.org/10.1007/s12020-012-9864-z [PubMed]
- 37. Luo L, Lu AM, Wang Y, Hong A, Chen Y, Hu J, Li X, Qin ZH. Chronic resistance training activates autophagy and reduces apoptosis of muscle cells by modulating IGF-1 and its receptors, Akt/mTOR and Akt/FOXO3a signaling in aged rats. Exp Gerontol. 2013; 48:427–36. https://doi.org/10.1016/j.exger.2013.02.009 [PubMed]
- 38. Anil C, Kut A, Atesagaoglu B, Nar A, Bascil Tutuncu N, Gursoy A. Metformin Decreases Thyroid Volume and Nodule Size in Subjects with Insulin Resistance: A Preliminary Study. Med Princ Pract. 2016; 25:233–36. https://doi.org/10.1159/000442821 [PubMed]
- 39. Rezzónico J, Rezzónico M, Pusiol E, Pitoia F, Niepomniszcze H. Metformin treatment for small benign thyroid nodules in patients with insulin resistance. Metab Syndr Relat Disord. 2011; 9:69–75. https://doi.org/10.1089/met.2010.0026 [PubMed]
- 40. Han B, Cui H, Kang L, Zhang X, Jin Z, Lu L, Fan Z. Metformin inhibits thyroid cancer cell growth, migration, and EMT through the mTOR pathway. Tumour Biol. 2015; 36:6295–304. https://doi.org/10.1007/s13277-015-3315-4 [PubMed]
- 41. Chen G, Xu S, Renko K, Derwahl M. Metformin inhibits growth of thyroid carcinoma cells, suppresses self-renewal of derived cancer stem cells, and potentiates the effect of chemotherapeutic agents. J Clin Endocrinol Metab. 2012; 97:E510–20. https://doi.org/10.1210/jc.2011-1754 [PubMed]
- 42. Tseng CH. Metformin reduces thyroid cancer risk in Taiwanese patients with type 2 diabetes. PLoS One. 2014; 9:e109852. https://doi.org/10.1371/journal.pone.0109852 [PubMed]