



Introduction
According to the American Cancer Society (ACS), lung cancer is the second most common cancer, with 235,760 new cases diagnosed in 2021 [1]. It is also one of the cancers with the lowest 5-year relative survival rate (21%), especially for small cell lung cancer (SCLC) whose 2-year survival is even lower than that of non-small cell lung cancer (NSCLC) (14–15% vs. 42%) [1]. SCLC accounts for approximately 13% of all lung carcinomas [2]. Compared with NSSLC, SCLC is associated with poorer prognosis, earlier and more frequent brain metastasis [3, 4]. Lung cancer is also a cancer of the elderly, with a median age of about 71 years at diagnosis [5], and there is an increasing trend in the proportion of SCLC patients in the age group older than 75 years according to a study from Hebei, China [6].
Over the past three decades, chemotherapy has provided considerable survival benefits for SCLC patients [7], and remains the standard treatment for first- and second-line management of SCLC [8]. Immunotherapy also plays an important role in patients with relapsed SCLC [8]. There have been many clinical trials on immune checkpoints inhibitors (ICIs), tumor vaccines, antigenic targets, and adoptive cellular immunotherapy in SCLC, but the results have been somewhat disappointing so far [9]. Treatment planning and decision mainly depend on the cancer TNM staging system and the Veterans Administration Lung Study Group (VALG) staging system, according to the National Comprehensive Cancer Network Clinical Practice Guidelines for SCLC, the Chinese Society of Clinical Oncology Lung Cancer Guidelines, and the European Society for Medical Oncology Clinical Practice Guidelines for Metastatic SCLC [10]. With the overall population life expectancy improving, treatment for elderly patients has aroused increasing attention. Given the performance status (PS) of the elderly and the associated comorbidities and toxicity, some oncologists are not inclined to using chemotherapy in elderly patients with SCLC [11]. So, whether chemotherapy is beneficial to elderly patients needs to be further confirmed. Several retrospective cohort studies exploring the relationship between age and treatment choice have defined elderly patients as age ≥ 65 [12, 13], ≥ 70 [14, 15] or ≥ 75 years old [11, 16]. There is limited research on patients > 80 years old, much less in elderly SCLC patients older than 80 years. A recent single center retrospective study evaluated the survival outcome associated with the treatment strategies in 56 cancer patients aged over 80 years, but only 7 of them were SCLC patients [17]. The aim of present study is to explore the impact of chemotherapy on survival prognosis of elderly patients with SCLC using the Surveillance, Epidemiology and End Results (SEER) database.
Methods
Data source
We performed this study to verify the relationship between chemotherapy and the survival prognosis of SCLC patients of different ages. All the data were based on the Surveillance, Epidemiology, and End Results (SEER) database, which was established in 1973 and collects information on cancer incidences and survival in the United States (US), covering 17 population-based cancer registries, accounting for about 28% of the current US population [18].
Study population
From 74,294 SCLC patients initially identified from the SEER database between 2004 and 2015, we included 57,460 patients for final analysis after excluding 13,544 patients without first malignant primary indicators, 167 with unknown survival months and 3,123 with incomplete data according to the inclusion and exclusion criteria (Figure 1). They were divided into two age groups: ≤ 80 years group (n = 50,941) and >80 years group (n = 6,519), and each group was further divided into chemotherapy group (n = 37,136 for ≤ 80 and 2,774 for >80 years) and non-chemotherapy group (n = 13,805 for ≤ 80 and 3,745 for > 80 years).
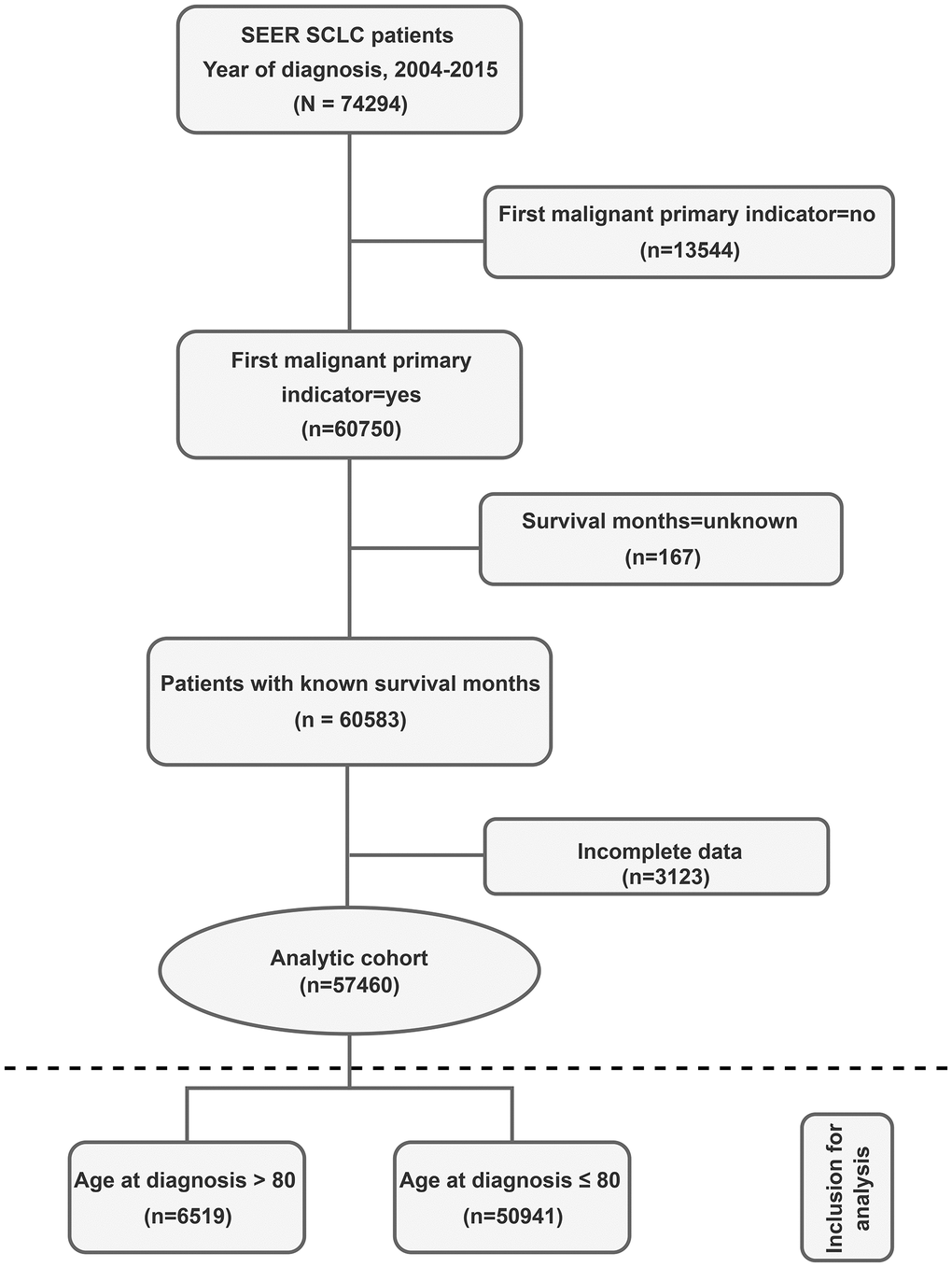
Figure 1. Study flow diagram. Abbreviations: SCLC: Small cell lung cancer; SEER: Surveillance, Epidemiology, and End Results registry.
Covariates
Baseline clinical characteristics including median age at diagnosis, gender, race, region, year of diagnosis, primary site, grade, laterality, stage, radiation, surgery, marital status, education level and median household income were collected.
Statistical analyses
Continuous variables were compared using t-test, and categorical variables were compared using chi-square. Potential deviation between chemotherapy and non-chemotherapy groups was controlled by propensity score matching (PSM) analysis. Kaplan-Meier (KM) analysis and the log rank test were applied to compare overall survival (OS) and lung-cancer specific survival (LCSS) between patients with or without chemotherapy. To study whether other variables could affect survival of SCLC patients, COX analysis was performed in each group. Statistical significance was set at a two-tailed P value < 0.05. All analyses were performed with IBM SPSS version 25.0.
Results
Study cohort characteristics
Demographic and clinical characteristics of the patients are included in Table 1. Among these, 50,941 were ≤ 80 years old and 6,519 were >80 years old, and their median age at diagnosis was 65 years (interquartile range, 59–72 years) and 83 years (interquartile range, 81–85 years) respectively. Both groups of patients were distributed roughly equally by gender (men 50.4%, women 49.6% in ≤ 80 years group; men 47.0%, women 53.0% in >80 years group). Most patients were Caucasian (86.9% in ≤80 years group; 87.8% in >80 years group), and from the East (50.8% in ≤80 years group; 41.6% in >80 years group) or Southwest (36.5% in ≤80 years group; 45.1% in >80 years group), only a few (0.2% in ≤80 years group; 0.1% in >80 years group) were living in the Northwest. Most patients did not receive surgical treatment (96.8% in ≤80 years group; 98.0% in >80 years group) or radiotherapy (51.1% in ≤80 years group; 74.4% in >80 years group). Patients in the early stage, married, treated with radiation but not surgery and had better education were more likely to receive chemotherapy. About 43% of the elderly patients in our study received chemotherapy. Most (73%) of the younger patients chose chemotherapy (Table 1). The proportion of SCLC patients choosing chemotherapy did not vary significantly with the year of diagnosis (Figure 2).
Table 1. Demographic and clinical characteristics of patients with SCLC.
| Variable | Age groups | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age ≤ 80 year Chemotherapy | Age > 80 year Chemotherapy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes n = 37136 (73) | No n = 13805 (27) | Total n = 50941 (100) | P | Yes n = 2774 (43) | No n = 3745 (57) | Total n = 6519 (100) | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median age at diagnosis | 64 (58–71) | 68 (61–74) | 65 (59–72) | <0.001 | 82 (81–84) | 83 (81–86) | 83 (81–85) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 18649 (50.2) | 7002 (50.7) | 25651 (50.4) | 0.314 | 1381 (49.8) | 1686 (45.0) | 3067 (47.0) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 18487 (49.8) | 6803 (49.3) | 25290 (49.6) | 1393 (50.2) | 2059 (55.0) | 3452 (53.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race recode | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White | 32288 (86.9) | 11972 (86.7) | 44260 (86.9) | 0.017 | 2447 (88.2) | 3275 (87.4) | 5722 (87.8) | 0.097 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Black | 3376 (9.1) | 1331 (9.6) | 4707 (9.2) | 156 (5.6) | 259 (6.9) | 415 (6.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 1441 (3.9) | 483 (3.5) | 1924 (3.8) | 170 (6.1) | 207 (5.5) | 377 (5.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 31 (0.1) | 19 (0.1) | 50 (0.1) | 1 (0.0) | 4 (0.1) | 5 (0.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHSDA region | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EAST | 19175 (51.6) | 6678 (48.4) | 25853 (50.8) | <0.001 | 1210 (43.6) | 1501 (40.1) | 2711 (41.6) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NORTHWEST | 81 (0.2) | 15 (0.1) | 96 (0.2) | 3 (0.1) | 2 (0.1) | 5 (0.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SOUTHWEST | 12904 (34.7) | 5704 (41.3) | 18608 (36.5) | 1162 (41.9) | 1779 (47.5) | 2941 (45.1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NORTH | 4976 (13.4) | 1408 (10.2) | 6384(12.5) | 399 (14.4) | 463 (12.4) | 862 (13.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Year of diagnosis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2004–2007 | 12499 (33.7) | 4796 (34.7) | 17295 (34.0) | 0.013 | 907 (32.7) | 1164 (31.1) | 2071 (31.8) | 0.097 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2008–2011 | 12264 (33.0) | 4587 (33.2) | 16851 (33.1) | 991 (35.7) | 1305 (34.8) | 2296 (35.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2012–2017 | 12373 (33.3) | 4422 (32.0) | 16795 (33.0) | 876 (31.6) | 1276 (34.1) | 2152 (33.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary Site | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Upper lobe | 17512 (47.2) | 5866 (42.5) | 23378 (45.9) | <0.001 | 1188 (42.8) | 1403 (37.5) | 2591 (39.7) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Middle lobe | 1431 (3.9) | 514 (3.7) | 1945 (3.8) | 118 (4.3) | 159 (4.2) | 277 (4.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lower lobe | 6941 (18.7) | 2522 (18.3) | 9463 (18.6) | 690 (24.9) | 851 (22.7) | 1541 (23.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NOS | 6301 (17.0) | 3173 (23.0) | 9474 (18.6) | 482 (17.4) | 939 (25.1) | 1421 (21.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overlapping lesion | 559 (1.5) | 226 (1.6) | 785 (1.5) | 54 (1.9) | 51 (1.4) | 105 (1.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Main bronchus | 4392 (11.8) | 1504 (10.9) | 5896 (11.6) | 242 (8.7) | 342 (9.1) | 584 (9.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 53 (0.1) | 29 (0.2) | 82 (0.2) | 0.019 | 0 (0.0) | 7 (0.2) | 7 (0.1) | 0.027 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 116 (0.3) | 57 (0.4) | 173 (0.3) | 6 (0.2) | 12 (0.3) | 18 (0.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 3239 (8.7) | 1224 (8.9) | 4463 (8.8) | 221 (8.0) | 303 (8.1) | 524 (8.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 6948 (18.7) | 2449 (17.7) | 9397 (18.4) | 556 (20.0) | 666 (17.8) | 1222 (18.7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 26780 (72.1) | 10046 (72.8) | 36826 (72.3) | 1991 (71.8) | 2757 (73.6) | 4748 (72.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laterality | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right-origin of primary | 20451 (55.1) | 7137 (51.7) | 27588 (54.2) | <0.001 | 1528 (55.1) | 1996 (53.3) | 3524 (54.1) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left-origin of primary | 14731 (39.7) | 5385 (39.0) | 20116 (39.5) | 1096 (39.5) | 1407 (37.6) | 2503 (38.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Paired sit | 1375 (3.7) | 931 (6.7) | 2306 (4.5) | 104 (3.7) | 253 (6.8) | 357 (5.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Only one side - side unspecified | 161 (0.4) | 101 (0.7) | 262 (0.5) | 8 (0.3) | 27 (0.7) | 35 (0.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not a paired site | 79 (0.2) | 29 (0.2) | 108 (0.2) | 8 (0.3) | 8 (0.2) | 16 (0.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral single primary | 339 (0.9) | 222 (1.6) | 561 (1.1) | 30 (1.1) | 54 (1.4) | 84 (1.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage Group | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 1416 (3.8) | 597 (4.3) | 2013 (4.0) | <0.001 | 156 (5.6) | 207 (5.5) | 363 (5.6) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 842 (2.3) | 182 (1.3) | 1024 (2.0) | 61 (2.2) | 56 (1.5) | 117 (1.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 11795 (31.8) | 2880 (20.9) | 14675 (28.8) | 884 (31.9) | 1022 (27.3) | 1906 (29.2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 23083 (62.2) | 10146 (73.5) | 33229 (65.2) | 1673 (60.3) | 2460 (65.7) | 4133 (63.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiation recode | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 22007 (59.3) | 2890 (20.9) | 24897 (48.9) | <0.001 | 1073 (38.7) | 594 (15.9) | 1667 (25.6) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 15129 (40.7) | 10915 (79.1) | 26044 (51.1) | 1701 (61.3) | 3151 (84.1) | 4852 (74.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 1117 (3.0) | 512 (3.7) | 1629 (3.2) | <0.001 | 39 (1.4) | 94 (2.5) | 133 (2.0) | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 36019 (97.0) | 13293 (96.3) | 49312 (96.8) | 2735 (98.6) | 3651 (97.5) | 6386 (98.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Marital status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 19567 (52.7) | 6015 (43.6) | 25582 (50.2) | <0.001 | 1257 (45.3) | 1356 (36.2) | 2613 (40.1) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single | 5024 (13.5) | 2386 (17.3) | 7410 (14.5) | 162 (5.8) | 255 (6.8) | 417 (6.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Divorced | 5777 (15.6) | 2060 (14.9) | 7837 (15.4) | 186 (6.7) | 258 (6.9) | 444 (6.8) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Windowed | 5001 (13.5) | 2505 (18.1) | 7506 (14.7) | 1073 (38.7) | 1689 (45.1) | 2762 (42.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 1211 (3.3) | 630 (4.6) | 1841 (3.6) | 86 (3.1) | 166 (4.4) | 252 (3.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unmarried or domestic partner | 65 (0.2) | 16 (0.1) | 81 (0.2) | 0 (0.0) | 2 (0.1) | 2 (0.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Separated | 491 (1.3) | 193 (1.4) | 684 (1.3) | 10 (0.4) | 19 (0.5) | 29 (0.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High school education | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >21 | 6990 (18.8) | 3338 (24.2) | 10328 (20.3) | <0.001 | 445 (16.0) | 730 (19.5) | 1175 (18.0) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 13–20 | 11319 (30.5) | 4366 (31.6) | 15685 (30.8) | 790 (28.5) | 1103 (29.5) | 1893 (29.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7–12 | 16421 (44.2) | 5385 (39.0) | 21806 (42.8) | 1320 (47.6) | 1611 (43.0) | 2931 (45.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤7 | 2406 (6.5) | 716 (5.2) | 3122 (6.1) | 219 (7.9) | 301 (8.0) | 520 (8.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median household income | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤38000 | 3626 (9.8) | 1440 (10.4) | 5066 (9.9) | 0.001 | 126 (4.5) | 208 (5.6) | 334 (5.1) | 0.051 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 38000–47999 | 7513 (20.2) | 2792 (20.2) | 10305 (20.2) | 452 (16.3) | 590 (15.8) | 1042 (16.0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 48000–62999 | 14408 (38.8) | 5489 (39.8) | 19897 (39.1) | 1062 (38.3) | 1511 (40.3) | 2573 (39.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63000 | 11589 (31.2) | 4084 (29.6) | 15673 (30.8) | 1134 (40.9) | 1436 (38.3) | 2570 (39.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: SCLC: Small cell lung cancer; NOS: Not otherwise specified. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
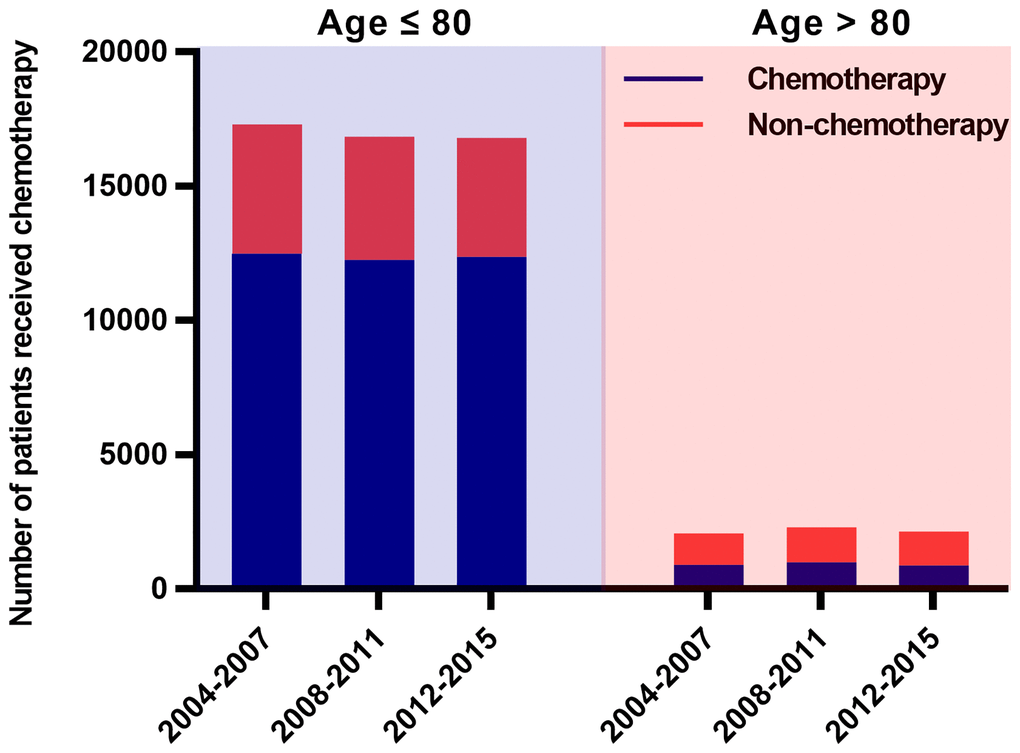
Figure 2. Numbers of SCLC patients who received chemotherapy over time (2004–2015). There were 12,499, 12,264 and 12,373 SCLC patients aged ≤ 80 years who received chemotherapy in 2004–2007, 2008–2011 and 2012–2015, accounting for 72%, 73% and 74% of all young patients respectively. During the same periods, 907 (44%), 991 (43%) and 876 (41%) patients older than 80 years underwent chemotherapy respectively. The proportion of patients receiving chemotherapy did not change significantly over time. Abbreviations: SCLC: Small cell lung cancer.
Comparison of survival curves between chemotherapy group and non-chemotherapy group
Enrolled in the study were 27,486 patients ≤ 80 years old and 4,550 patients >80 years old after propensity score matched analysis. KM analysis demonstrated improved OS and LCSS in patients of chemotherapy group compared to patients of non-chemotherapy group, with the survival curves showing statistically significant differences (log rank P < 0.0001) in both ≤ 80 years group and > 80 years group (Figure 3).
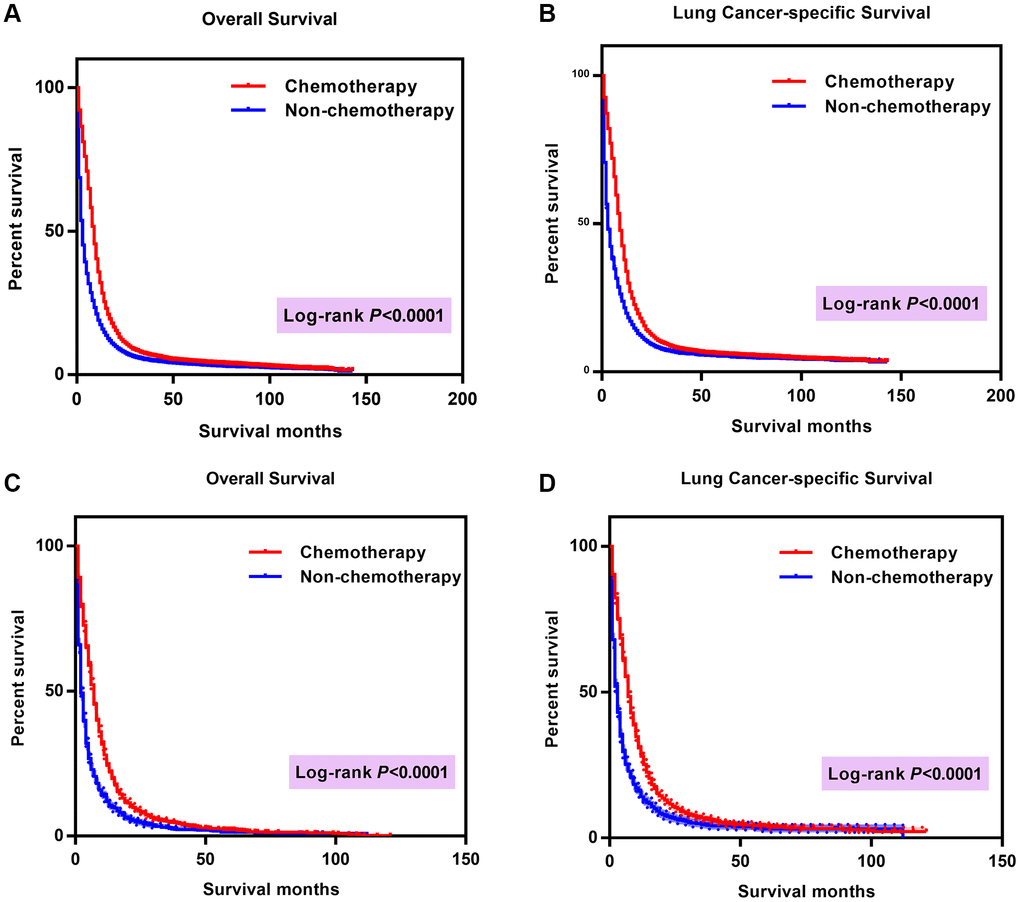
Figure 3. Comparison of survival curves between chemotherapy group and group without chemotherapy. (A) Comparison of OS in patients ≤ 80 years old; (B) Comparison of LCSS in patients ≤ 80 years old; (C) Comparison of OS in patients >80 years old; (D) Comparison of LCSS in patients > 80 years old. Abbreviations: OS: Overall survival; LCSS: Lung cancer-specific survival; Cum: Cumulative.
The effects of chemotherapy on the survival of patients with SCLC
Cox analysis demonstrated the survival benefit of chemotherapy in both ≤ 80 years group (OS: HR 0.435; 95% CI 0.424–0.447; P < 0.001; LCSS: HR 0.436; 95% CI 0.424–0.448; P < 0.001) and > 80 years group (OS: HR 0.424; 95% CI 0.397–0.451; P < 0.001; CSS: HR 0.415; 95% CI 0.389–0.444; P < 0.001). Also, survival varied with the change of other variables including sex, primary site, laterality, stage, surgery, radiation and household income. Additionally, variables like race, year of diagnosis, region, age, marital status, and education status also affected survival in in ≤ 80 years group (Tables 2 and 3; Figure 4). The following parameters had a negative impact on survival of patients in ≤ 80 years group: Caucasian, male sex, later year of diagnosis, older age, north region, tumor location in main bronchus, increased stage and grade, bilateral tumor, no surgery or radiation, separation, lower median household income and poorer educated, while the following parameters had a negative impact on survival of patients in > 80 years group: male sex, tumor location in main bronchus, increased stage, bilateral tumor, no surgery or radiation, and lower median household income.
Table 2. Multivariate analysis using a Cox proportional hazards model in SCLC patients ≤ 80.
| Variable | Multivariate analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OS | CSS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Race recode | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| White | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Black | 0.909 | 0.870 to 0.949 | <0.001 | 0.896 | 0.856 to 0.938 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.909 | 0.849 to 0.974 | 0.007 | 0.884 | 0.822 to 0.951 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 0.572 | 0.365 to 0.898 | 0.015 | 0.395 | 0.224 to 0.696 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 0.885 | 0.863 to 0.908 | <0.001 | 0.896 | 0.872 to 0.920 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Year of diagnosis | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2012-2015 | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2008-2011 | 0.922 | 0.894 to 0.951 | <0.001 | 0.924 | 0.894 to 0.955 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2004-2007 | 0.920 | 0.891 to 0.950 | <0.001 | 0.933 | 0.903 to 0.965 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHSDA Region | 0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NORTH | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SOUTHWEST | 0.946 | 0.902 to 0.992 | 0.023 | 0.946 | 0.900 to 0.993 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EAST | 0.919 | 0.879 to 0.960 | <0.001 | 0.907 | 0.866 to 0.949 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary Site | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Main bronchus | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Upper lobe | 0.918 | 0.881 to 0.957 | <0.001 | 0.913 | 0.874 to 0.953 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Middle lobe | 0.899 | 0.834 to 0.969 | 0.005 | 0.880 | 0.814 to 0.952 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lower lobe | 0.931 | 0.888 to 0.975 | 0.003 | 0.923 | 0.879 to 0.969 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NOS | 1.029 | 0.980 to 1.081 | 0.253 | 1.019 | 0.968 to 1.072 | 0.476 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overlapping lesion | 1.011 | 0.913 to 1.120 | 0.836 | 0.996 | 0.896 to 1.108 | 0.941 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grade | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 0.497 | 0.353 to 0.700 | <0.001 | 0.491 | 0.341 to 0.708 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 0.876 | 0.708 to 1.083 | 0.222 | 0.935 | 0.752 to 1.163 | 0.545 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 0.963 | 0.920 to 1.007 | 0.101 | 0.966 | 0.922 to 1.013 | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 0.982 | 0.950 to 1.014 | 0.265 | 0.986 | 0.953 to 1.020 | 0.43 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laterality | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral, single primary | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right-origin of primary | 1.092 | 0.985 to 1.211 | 0.096 | 1.058 | 0.952 to 1.175 | 0.297 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left-origin of primary | 1.101 | 0.993 to 1.222 | 0.069 | 1.068 | 0.960 to 1.187 | 0.224 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Paired sit | 0.922 | 0.825 to 1.030 | 0.152 | 0.886 | 0.791 to 0.992 | 0.036 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Only one side - side unspecified | 0.827 | 0.691 to 0.991 | 0.04 | 0.779 | 0.645 to 0.941 | 0.010 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not a paired site | 1.044 | 0.797 to 1.368 | 0.755 | 0.995 | 0.751 to 1.317 | 0.970 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage Group | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 0.653 | 0.633 to 0.673 | <0.001 | 0.623 | 0.603 to 0.644 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 0.521 | 0.465 to 0.583 | <0.001 | 0.477 | 0.422 to 0.539 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 0.307 | 0.283 to 0.333 | <0.001 | 0.255 | 0.233 to 0.279 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.500 | 0.461 to 0.543 | <0.001 | 0.495 | 0.453 to 0.540 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiation recode | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.685 | 0.664 to 0.706 | <0.001 | 0.695 | 0.673 to 0.718 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age at diagnosis | 1.013 | 1.011 to 1.015 | <0.001 | 1.012 | 1.010 to 1.013 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Marital status | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Separated | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Divorced | 1.023 | 0.917 to 1.142 | 0.681 | 1.021 | 0.911 to 1.144 | 0.721 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single | 1.011 | 0.906 to 1.128 | 0.839 | 0.997 | 0.890 to 1.117 | 0.956 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Windowed | 0.980 | 0.878 to 1.094 | 0.717 | 0.984 | 0.878 to 1.103 | 0.780 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 0.912 | 0.807 to 1.030 | 0.137 | 0.918 | 0.808 to 1.041 | 0.182 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Married | 0.907 | 0.815 to 1.010 | 0.075 | 0.918 | 0.822 to 1.026 | 0.132 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unmarried or domestic partner | 0.825 | 0.564 to 1.205 | 0.319 | 0.830 | 0.560 to 1.230 | 0.354 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High school education | 0.008 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <7 | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7-12 | 1.001 | 0.943 to 1.062 | 0.975 | 1.007 | 0.947 to 1.071 | 0.833 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 13-20 | 1.001 | 0.939 to 1.067 | 0.967 | 1.015 | 0.950 to 1.085 | 0.659 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >21 | 0.942 | 0.879 to 1.010 | 0.095 | 0.941 | 0.875 to 1.012 | 0.103 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median household income | <0.001 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63000 | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 48000-62999 | 1.018 | 0.985 to 1.053 | 0.287 | 1.027 | 0.992 to 1.064 | 0.133 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 38000-47999 | 1.053 | 1.009 to 1.100 | 0.018 | 1.055 | 1.009 to 1.104 | 0.019 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <38000 | 1.124 | 1.062 to 1.190 | <0.001 | 1.131 | 1.066 to 1.200 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chemotherapy recode | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.435 | 0.424 to 0.447 | <0.001 | 0.436 | 0.424 to 0.448 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: SCLC: Small cell lung cancer; NOS: Not otherwise specified; HR: hazard ratio; CI: Confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 3. Multivariate analysis using a Cox proportional hazards model in SCLC patients >80.
| Variable | Multivariate analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OS | CSS | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 0.883 | 0.831 to 0.939 | <0.001 | 0.896 | 0.841 to 0.955 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary Site | 0.002 | 0.003 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Main bronchus | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Upper lobe | 0.828 | 0.739 to 0.927 | 0.001 | 0.812 | 0.722 to 0.913 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Middle lobe | 0.820 | 0.683 to 0.985 | 0.033 | 0.819 | 0.677 to 0.991 | 0.404 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lower lobe | 0.872 | 0.774 to 0.983 | 0.024 | 0.858 | 0.757 to 0.972 | 0.016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NOS | 0.936 | 0.824 to 1.063 | 0.308 | 0.925 | 0.810 to 1.056 | 0.248 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overlapping lesion | 1.080 | 0.846 to 1.378 | 0.536 | 1.025 | 0.792 to 1.326 | 0.852 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laterality | 0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral, single primary | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right-origin of primary | 0.912 | 0.681 to 1.220 | 0.533 | 0.926 | 0.683 to 1.254 | 0.618 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left-origin of primary | 0.987 | 0.737 to 1.323 | 0.932 | 1.009 | 0.744 to 1.369 | 0.956 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Paired sit | 0.716 | 0.524 to 0.977 | 0.035 | 0.704 | 0.508 to 0.975 | 0.035 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Only one side - side unspecified | 0.636 | 0.380 to 1.064 | 0.085 | 0.660 | 0.388 to 1.122 | 0.124 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not a paired site | 0.917 | 0.458 to 1.833 | 0.805 | 0.890 | 0.429 to 1.844 | 0.753 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage Group | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 0.739 | 0.689 to 0.792 | <0.001 | 0.717 | 0.667 to 0.771 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| II | 0.539 | 0.428 to 0.679 | <0.001 | 0.480 | 0.373 to 0.618 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | 0.369 | 0.318 to 0.429 | <0.001 | 0.326 | 0.277 to 0.384 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Surgery | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.536 | 0.406 to 0.709 | <0.001 | 0.596 | 0.446 to 0.796 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiation recode | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.678 | 0.631 to 0.728 | <0.001 | 0.680 | 0.630 to 0.733 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median household income | <0.001 | 0.014 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63000 | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 48000–62999 | 1.050 | 0.981 to 1.123 | 0.162 | 1.047 | 0.976 to 1.125 | 0.201 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 38000–47999 | 1.159 | 1.061 to 1.266 | 0.001 | 1.157 | 1.055 to 1.269 | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <38000 | 0.994 | 0.867 to 1.139 | 0.929 | 0.967 | 0.837 to 1.116 | 0.643 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chemotherapy recode | <0.001 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | Reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 0.424 | 0.397 to 0.451 | <0.001 | 0.415 | 0.389 to 0.444 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: SCLC: Small cell lung cancer; NOS: Not otherwise specified; HR: hazard ratio; CI: Confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
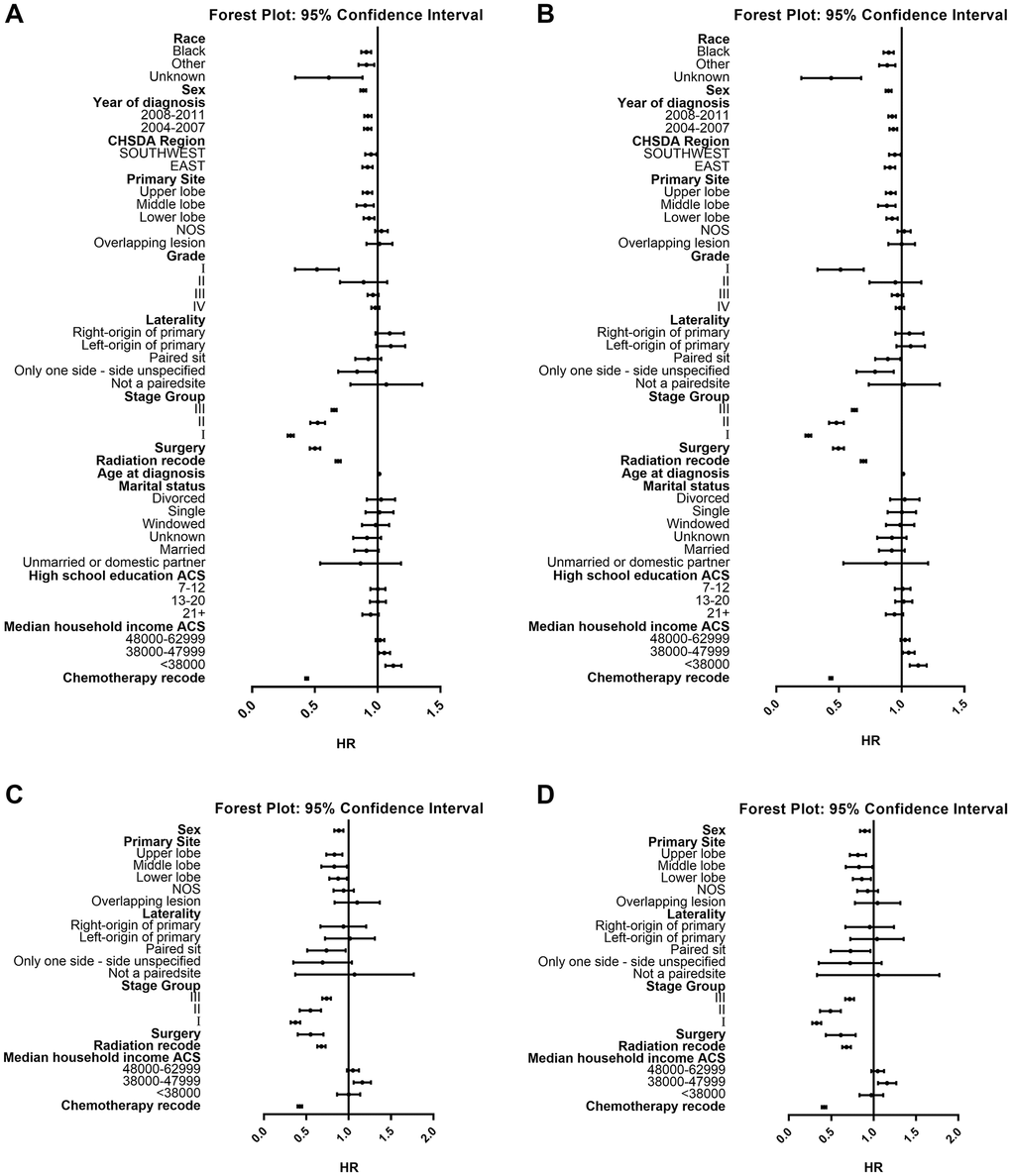
Figure 4. Forest plot of HRs of factors that can influence OS or LCSS in patients ≤ or >80. (A) HRs of factors influencing OS in patients ≤80 years old; (B) HRs of factors influencing LCSS in patients ≤80 years old; (C) HRs of factors influencing OS in patients >80 years old; (D) HRs of factors influencing LCSS in patients >80 years old. Abbreviations: HRs: Hazard ratios; OS: Overall survival; LCSS: Lung cancer-specific survival.
Discussion
The results of our study demonstrated the benefit of chemotherapy in both young and elderly SCLC patients. Although chemotherapy could benefit OS and LCSS regardless of age, patients older than 80 years tended to reject chemotherapy compared with patients younger than 80 years. Besides, the results of our COX analysis showed that male sex, an increased stage and grade, and no surgery or radiation were associated with worse prognoses. In < 80 years group, Caucasian patients who were diagnosed late or at an older age tended to have worse prognoses.
More studies have paid increasing attention to the relationship between chemotherapy and survival of SCLC patients, especially in elderly SCLC patients. Elegbede et al. reviewed 404 SCLC patients managed at a tertiary cancer center in Canada from 2010 to 2016 and found that chemotherapy benefited survival of SCLC patients, especially those in extensive stages (HR 0.33; 95% CI 0.22–0.48; P < 0.01) [19]. Another study developed a nomogram prognostic model based on a large cohort of 24,680 SCLC patients from the National Cancer Database (NCDB), and their result showed that chemotherapy was beneficial to improving prognosis (HR 0.35; 95% CI 0.33–0.36; P < 0.001) [20]. A study from the Japanese Joint Committee of Lung Cancer Registry [21] reported that OS of their 228 SCLC patients aged > 75 years who received second-line chemotherapy was 13.9 weeks, which was significantly higher than 7.5 months in those who received supportive care alone in a previous randomized controlled study [22]. A meta-analysis recruiting 14 relevant randomized clinical trials from the Medline and Cochrane databases reported that the 1-year OS improved from 30% to 39% and the 2-year OS improved from 10% to 14% in SCLC patients who received maintenance chemotherapy [23]. Several previous studies concluded that patients of advanced age tended to reject chemotherapy, which is consistent with our study. By reviewing a number of retrospective studies, Deppermann et al. [24] concluded that elderly patients were often offered only suboptimal or no treatment. Researchers from the British Columbia Cancer Agency carried out a retrospective review on 174 patients with SCLC between 1991 and 1999, and categorized them into three age groups: < 65 years (n = 55), 65–74 years (n = 76), and ≥ 75 years (n = 43). The results displayed that elder patients tended to fail to complete an “optimal” course (intravenous regimens, more than 85% total doses, 4+ cycles, and less than 2 weeks total treatment delays) of first-line chemotherapy (P < 0.05), and patients >65 years were less likely to administer second-line chemotherapy (P < 0.05) [16]. In the light of a recently published retrospective analysis of SCLC patients at IPO-Porto, Portugal's largest oncology hospital, the median age of patients who received platinum doublet chemotherapy was lower than the respective full populations (LS-SCLC: 64 years vs. 70 years; ES-SCLC: 63 years vs. 64 years), suggesting that age may affect the patient’s decision whether to receive chemotherapy [25]. Stacey et al. [11] reported that PS and the presence of comorbidities were the most common factors that affected clinical oncologists not to recommend chemotherapy, and most patients rejected chemotherapy mainly because of their concerns about toxicity. Our COX analysis also demonstrated that surgery and radiation were positively associated with better survival, which is consist with other recent studies [26–29]. In a retrospective analysis of 366 SCLC patients receiving chemotherapy or chemoradiotherapy [28], Kanaji et al. found in LS-SCLC patients with idiopathic pulmonary fibrosis (IPF), chemoradiotherapy related to better progression-free survival (PFS) (281 days vs. 146 days, P = 0.0471) and OS (1163 vs. 355 days, P = 0.0012) compared with chemotherapy only. A comparative study involving 37 postoperative patients and 37 patients without surgery who both received chemotherapy of “etoposide + cisplatin or carboplatin” showed that the 1, 3, 5-year survival rates were significantly different (1-year survival rate: 72.97% vs. 54.05%; 2-year survival rate: 35.13% vs. 13.51%; 3-year survival rate: 21.62% vs. 5.41%) [29]. Elegbede et al. analyze the survival of 404 SCLC patients and fund that surgery benefited OS of LS-SCLC patients compared with no treatment (40 months vs. 8 months), and chemotherapy combined with thoracic radiotherapy correlated with longer OS compared with chemotherapy alone (13 months vs. 9 months) [19].
Our study investigated a large cohort of 57,460 SCLC patients from real world data. Although many other studies have also addressed the effect of chemotherapy on the survival prognosis of SCLC patients [16, 17, 19, 20, 22], they were mostly based on limited sample sizes, and there have been few investigations on the prognosis of different age subgroups. Given aging of the population, patients older than 80 years will account for a greater proportion. Therefore, the results of our study may provide useful information for clinical oncologists and elderly patients in choosing treatment options. Additionally, we also analyzed the impact of other factors on patient survival, which may also guide patient management. However, several deficiencies in our research need to be mentioned. Despite the large sample size of the SEER, the smoking status and PS are not available in the database, knowing that the former is strongly associated to SCLC [30, 31], and the latter has also proved to be related to the prognosis of SCLC patients [32]. It is possible that patients who smoke or have a low PS score were included in the non-chemotherapy group, which may induce biases in the results. Concurrently, reasons for not choosing chemotherapy, or potential factors affecting the receipt of chemotherapy, such as the nutritional status, cognitive function and geriatric syndrome, are not included in the SEER, either. These limitations need to be refined in future validation using data from hospitals, or randomized controlled trials.
Conclusions
To conclude, chemotherapy is a beneficial choice for patients with SCLC over 80 years old, although elderly patients are less likely to receive chemotherapy. Age should not be the main basis for deciding whether to receive chemotherapy or not.
Author Contributions
H.R., A.M., and S.Z. designed the study; H.R. and S.X. were responsible for collection and assembly of data; S.X. revised it critically for important intellectual content. All authors contributed to data analysis and interpretation have reviewed the final version.
Acknowledgments
We would like to thank all the staff of the National Cancer Institute for their efforts in the SEER program.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This work was supported by the Fundamental Research Funds of Shanghai Tenth Hospital’s Improvement Plan for NSFC (No. 04.03.20108).
References
- 1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021; 71:7–33. https://doi.org/10.3322/caac.21654 [PubMed]
- 2. Raso MG, Bota-Rabassedas N, Wistuba II. Pathology and Classification of SCLC. Cancers (Basel). 2021; 13:820. https://doi.org/10.3390/cancers13040820 [PubMed]
- 3. Marinova Marinova D, Vitkov Mekov E, Gosheva Dimitrova D, Todorov Titorenkov P, Martinov Mihailov M, Slavov Nachev S, Milosheva Youroukova V, Temelkov Kostadinov D, Georgieva Slavova Y. Immunohistochemical characteristics of brain metastases and corresponding primary lung cancer. J BUON. 2019; 24:1626–37. [PubMed]
- 4. Verma V, Sharma G, Singh A. Immunotherapy in extensive small cell lung cancer. Exp Hematol Oncol. 2019; 8:5. https://doi.org/10.1186/s40164-019-0129-x [PubMed]
- 5. Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA. SEER Cancer Statistics Review, 1975-2018, National Cancer Institute. 2021. https://seer.cancer.gov/csr/1975_2018/.
- 6. Li D, Xu X, Liu J, Liang D, Shi J, Li S, Jin J, He Y. Small cell lung cancer (SCLC) incidence and trends vary by gender, geography, age, and subcategory based on population and hospital cancer registries in Hebei, China (2008-2017). Thorac Cancer. 2020; 11:2087–93. https://doi.org/10.1111/1759-7714.13412 [PubMed]
- 7. Saltos A, Shafique M, Chiappori A. Update on the Biology, Management, and Treatment of Small Cell Lung Cancer (SCLC). Front Oncol. 2020; 10:1074. https://doi.org/10.3389/fonc.2020.01074 [PubMed]
- 8. Yang S, Zhang Z, Wang Q. Emerging therapies for small cell lung cancer. J Hematol Oncol. 2019; 12:47. https://doi.org/10.1186/s13045-019-0736-3 [PubMed]
- 9. Lum C, Alamgeer M. Technological and Therapeutic Advances in Advanced Small Cell Lung Cancer. Cancers (Basel). 2019; 11:1570. https://doi.org/10.3390/cancers11101570 [PubMed]
- 10. Zhao H, Ren D, Liu H, Chen J. Comparison and discussion of the treatment guidelines for small cell lung cancer. Thorac Cancer. 2018; 9:769–74. https://doi.org/10.1111/1759-7714.12765 [PubMed]
- 11. Fisher S, Al-Fayea TM, Winget M, Gao H, Butts C. Uptake and tolerance of chemotherapy in elderly patients with small cell lung cancer and impact on survival. J Cancer Epidemiol. 2012; 2012:708936. https://doi.org/10.1155/2012/708936 [PubMed]
- 12. Shao C, He J, Kachroo S, Jin F. Chemotherapy treatments, costs of care, and survival for patients diagnosed with small cell lung cancer: A SEER-Medicare study. Cancer Med. 2019; 8:7613–22. https://doi.org/10.1002/cam4.2626 [PubMed]
- 13. Kang EJ, Choi YJ, Lee SR, Sung HJ, Kim JS. Impact of subsequent chemotherapy on the survival of elderly patients with extensive stage small cell lung cancer. Korean J Intern Med. 2020; 35:1468–76. https://doi.org/10.3904/kjim.2019.136 [PubMed]
- 14. Doherty J, Dawe DE, Pond GR, Ellis PM. The effect of age on referral to an oncologist and receipt of chemotherapy among small cell lung cancer patients in Ontario, Canada. J Geriatr Oncol. 2019; 10:449–58. https://doi.org/10.1016/j.jgo.2018.10.001 [PubMed]
- 15. Johal S, Hettle R, Carroll J, Maguire P, Wynne T. Real-world treatment patterns and outcomes in small-cell lung cancer: a systematic literature review. J Thorac Dis. 2021; 13:3692–707. https://doi.org/10.21037/jtd-20-3034 [PubMed]
- 16. Ludbrook JJ, Truong PT, MacNeil MV, Lesperance M, Webber A, Joe H, Martins H, Lim J. Do age and comorbidity impact treatment allocation and outcomes in limited stage small-cell lung cancer? a community-based population analysis. Int J Radiat Oncol Biol Phys. 2003; 55:1321–30. https://doi.org/10.1016/s0360-3016(02)04576-5 [PubMed]
- 17. Wang P, Li C, An Y, Wang X, Liang Z, Chen L. The management of elderly patients with lung cancer: a single center retrospective study. Ann Palliat Med. 2021; 10:229–37. https://doi.org/10.21037/apm-20-2125 [PubMed]
- 18. Murphy M, Alavi K, Maykel J. Working with existing databases. Clin Colon Rectal Surg. 2013; 26:5–11. https://doi.org/10.1055/s-0033-1333627 [PubMed]
- 19. Elegbede AA, Gibson AJ, Fu H, Dean ML, Ezeife DA, Lau H, Cheung WY, Bebb DG. Real-World Adherence to Guideline-Recommended Treatment for Small Cell Lung Cancer. Am J Clin Oncol. 2020; 43:236–42. https://doi.org/10.1097/COC.0000000000000657 [PubMed]
- 20. Wang S, Yang L, Ci B, Maclean M, Gerber DE, Xiao G, Xie Y. Development and Validation of a Nomogram Prognostic Model for SCLC Patients. J Thorac Oncol. 2018; 13:1338–48. https://doi.org/10.1016/j.jtho.2018.05.037 [PubMed]
- 21. O'Brien ME, Ciuleanu TE, Tsekov H, Shparyk Y, Cuceviá B, Juhasz G, Thatcher N, Ross GA, Dane GC, Crofts T. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol. 2006; 24:5441–7. https://doi.org/10.1200/JCO.2006.06.5821 [PubMed]
- 22. Igawa S, Naoki K, Shintani Y, Sekine I, Shukuya T, Takayama K, Inoue A, Okamoto I, Kiura K, Takahashi K, Yamamoto N, Takiguchi Y, Miyaoka E, et al. Survival and prognostic factors in elderly patients receiving second-line chemotherapy for relapsed small-cell lung cancer: Results from the Japanese Joint Committee of Lung Cancer Registry. Lung Cancer. 2020; 146:160–4. https://doi.org/10.1016/j.lungcan.2020.05.038 [PubMed]
- 23. Bozcuk H, Artac M, Ozdogan M, Savas B. Does maintenance/consolidation chemotherapy have a role in the management of small cell lung cancer (SCLC)? A metaanalysis of the published controlled trials. Cancer. 2005; 104:2650–7. https://doi.org/10.1002/cncr.21540 [PubMed]
- 24. Deppermann KM. Influence of age and comorbidities on the chemotherapeutic management of lung cancer. Lung Cancer. 2001 (Suppl 1); 33:S115–20. https://doi.org/10.1016/s0169-5002(01)00311-7 [PubMed]
- 25. Soares M, Antunes L, Redondo P, Borges M, Grimson F, Hermans R, Chaib C, Lacoin L, Juarez-Garcia A, Daumont MJ, Penrod JR, Bento MJ, Gonçalves FR. Small cell lung cancer treatment and survival in Portugal: A retrospective analysis from the I-O Optimise initiative. Eur J Cancer Care (Engl). 2021; 30:e13496. https://doi.org/10.1111/ecc.13496 [PubMed]
- 26. Sun A, Durocher-Allen LD, Ellis PM, Ung YC, Goffin JR, Ramchandar K, Darling G. Guideline for the Initial Management of Small Cell Lung Cancer (Limited and Extensive Stage) and the Role of Thoracic Radiotherapy and First-line Chemotherapy. Clin Oncol (R Coll Radiol). 2018; 30:658–66. https://doi.org/10.1016/j.clon.2018.06.008 [PubMed]
- 27. Halvorsen TO, Herje M, Levin N, Bremnes RM, Brustugun OT, Fløtten Ø, Kaasa S, Sundstrøm S, Grønberg BH. Tumour size reduction after the first chemotherapy-course and outcomes of chemoradiotherapy in limited disease small-cell lung cancer. Lung Cancer. 2016; 102:9–14. https://doi.org/10.1016/j.lungcan.2016.10.003 [PubMed]
- 28. Kanaji N, Shimizu J, Sakai K, Ueda Y, Miyawaki H, Watanabe N, Uemura T, Hida T, Inoue T, Watanabe N, Oohara Y, Dobashi H, Kato M, Kadowaki N. Clinical features of patients with small cell lung cancer and idiopathic pulmonary fibrosis treated with chemotherapy or chemoradiotherapy. Ther Adv Respir Dis. 2020; 14:1753466620963866. https://doi.org/10.1177/1753466620963866 [PubMed]
- 29. Li GH, Wu Y, Zhang XJ, Cui YS. [A comparative study of survival time of surgery combined with chemotherapy and non-surgical chemotherapy in SCLC]. Zhonghua Yi Xue Za Zhi. 2010; 90:2212–4. [PubMed]
- 30. Bernhardt EB, Jalal SI. Small Cell Lung Cancer. Cancer Treat Res. 2016; 170:301–22. https://doi.org/10.1007/978-3-319-40389-2_14 [PubMed]
- 31. Pleasance ED, Stephens PJ, O'Meara S, McBride DJ, Meynert A, Jones D, Lin ML, Beare D, Lau KW, Greenman C, Varela I, Nik-Zainal S, Davies HR, et al. A small-cell lung cancer genome with complex signatures of tobacco exposure. Nature. 2010; 463:184–90. https://doi.org/10.1038/nature08629 [PubMed]
- 32. Jones GS, Elimian K, Baldwin DR, Hubbard RB, McKeever TM. A systematic review of survival following anti-cancer treatment for small cell lung cancer. Lung Cancer. 2020; 141:44–55. https://doi.org/10.1016/j.lungcan.2019.12.015 [PubMed]