



Introduction
Cardiovascular disease (CVD) is the leading global cause of death [1]. Age, sex, hypertension (HTN), dyslipidemia, hyperglycemia, obesity, and smoking are significant determinants of incident CVD in the general population [2].
Albuminuria (AU), defined as urine albumin-to-creatinine ratio (UACR) more than 30 mg/g, is recognized as the earliest sign of not only vascular disease but also of renal dysfunction [3, 4]. Although 24-hour urine protein collection is the gold-standard urinary albumin excretion assay, it is cumbersome for patients and is unreliable due to under or over collection and laboratory processing methods [5]. MA can be diagnosed more easily by UACR determinations [6, 7]. Increased UACR has been associated with cardiovascular morbidity and mortality and incident strokes in diabetics [8]. Furthermore, MA is an independent risk factor of coronary heart disease, peripheral vascular disease, and stroke in non-diabetics [9, 10]. Although increased UACR has been associated with maladaptive carotid remodeling that may predispose to stroke [11]; and may result from multiple cardiovascular risk factors such as HTN, age, obesity, and dyslipidemia; the pathophysiologic links of MA to the above diseases are still unknown [12].
Carotid intima-media thickening (CIMT) is an accepted ultrasonographic marker of early subclinical atherosclerosis (SA) and may be a predictive factor of incident CVD [13, 14]. Well-known determinants of CIMT are age, HTN, and sex. Females have exhibited lower CIMT than males in numerous studies, including the Gutenberg-Heart Study in Germany [15], the Atherosclerosis Risk in Communities study [16], and the Suita study of Japanese subjects [17].
Albuminuria has been associated with CIMT. A significant association of urinary albumin excretion and CIMT was observed in hypertensive men with diabetes mellitus (DM) [18]. However, MA was unrelated to CIMT in hypertensive men without DM [19]. Clinical investigations regarding a differential sex-based association of pathological albuminuria (PAU) (UACR ≥30 mg/g) on SA have been limited. This study aimed to determine whether PAU is associated with the early phase of SA, and whether such an association may be sex-determined, especially in relatively healthy populations.
Results
A total of 1228 participants (46.0% women; mean age 62.56 ± 8.77 years) without coronary artery disease (CAD), DM, or chronic kidney disease (CKD) were investigated. In women, there were no differences of age, body mass index (BMI), waist circumference, waist-to-height ratio, or prevalence of smoking between subjects with or without PAU. In contrast, men with PAU were older and exhibited elevated waist circumference and an increased prevalence of waist circumference >90 cm (a metabolic syndrome criterion) compared to those with normal AU. Significantly higher prevalence rates of HTN and anti-HTN therapy were observed in both women and men with PAU. However, women had more elevated total body fat than men (37.1% vs. 24.8% respectively; p < 0.001). Men with PAU had significantly higher total body fat than those with normal AU (26.48 ± 7.42 vs. 24.52 ± 6.46; p = 0.027).
Total serum cholesterol, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), hemoglobin A1c, uric acid, and creatinine values were similar between men and women. PAU was associated with higher fasting glucose in women but not in men. Men with PAU exhibited higher triglyceride levels and lower estimated glomerular filtration rate (eGFR). PAU was associated with substantially increased mean CIMT and higher prevalence of SA (CIMT ≥0.75 mm) in men, but not in women (Table 1).
Table 1. Baseline characteristics according to UACR ≥ 30 mg/g or not stratified by gender.
| Female (n = 655) | Male (573) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR <30 mg/g n = 565 | UACR ≥30 mg/g n = 90 | p value | UACR <30 mg/g n = 485 | UACR ≥30 mg/g n = 88 | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | 59.9 (54.95–67.75) | 60.7 (55.30–69.45) | 0.501 | 61.1 (55.3–70.0) | 65.1 (58.28–74.78) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 23.92 (21.90–26.3) | 24.25 (22.18–27.24) | 0.303 | 24.42 (22.34–26.48) | 25.33 (22.47–27.34) | 0.087 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference | 80.0 (74.0–86.5) | 81.5 (75.0–87.13) | 0.496 | 86 (80.5–91.75) | 88.75 (82.88–94.0) | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist-to-height ratio | 0.53 ± 0.067 | 0.53 ± 0.063 | 0.351 | 0.52 ± 0.050 | 0.54 ± 0.054 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking (%) | 17 (3.0) | 3 (3.3) | 0.747 | 160 (33.0) | 34 (38.6) | 0.328 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Underlying disease | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension (%) | 161 (28.5) | 46 (51.1) | <0.001 | 147 (30.3) | 42 (47.7) | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anti-Hypertensive agents (%) | 73 (12.9) | 25 (27.8) | 0.001 | 77 (15.9) | 23 (26.1) | 0.031 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 29 (5.1) | 9 (10.0) | 0.085 | 16 (3.3) | 4 (4.5) | 0.529 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 26 (4.6) | 9 (10.0) | 0.043 | 14 (2.9) | 3 (3.4) | 0.734 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome (%) | 136 (24.1) | 32 (35.6) | 0.027 | 101 (20.8) | 30 (34.1) | 0.009 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome_BS | 131 (23.2) | 27 (30.0) | 0.184 | 133 (27.4) | 33 (37.5) | 0.073 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome_BP | 301 (53.3) | 66 (73.3) | <0.001 | 281 (57.9) | 68 (77.3) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome_HDL | 117 (20.7) | 26 (28.9) | 0.098 | 67 (13.8) | 15 (17.0) | 0.411 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome_TG | 86 (15.2) | 17 (18.9) | 0.354 | 118 (24.3) | 23 (26.1) | 0.689 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome_WC | 297 (52.6) | 52 (57.8) | 0.366 | 164 (33.8) | 41 (46.6) | 0.029 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity (%) | 116 (20.5) | 23 (25.6) | 0.270 | 94 (19.4) | 24 (27.3) | 0.114 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body total fat % (DXA) | 37.17 ± 6.01 | 36.61 ± 7.58 | 0.505 | 24.52 ± 6.46 | 26.48 ± 7.42 | 0.027 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laboratory data | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total Cholesterol (mg/dl) | 205 (182–225.5) | 199 (170.75–227.25) | 0.181 | 192 (170.5–215.0) | 191.5 (168.8–212.3) | 0.979 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL (mg/dl) | 58 (51–69) | 56 (47–67.25) | 0.141 | 50 (43–57) | 49.5 (42–57) | 0.873 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL (mg/dl) | 122 (101–142.5) | 118.5 (98–145.75) | 0.484 | 119 (99–142) | 122 (105.3–134) | 0.550 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fasting glucose (mg/dl) | 93 (87–99) | 94.5 (89–101.25) | 0.028 | 94 (89–100) | 96 (89–104) | 0.136 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c (%) | 5.8 (5.6–6.0) | 5.8 (5.58–6.10) | 0.197 | 5.7 (5.4–5.9) | 5.8 (5.5–6.0) | 0.068 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Uric acid | 5.0 (4.4–5.8) | 5.1 (4.3–5.9) | 0.836 | 6.4 (5.5–7.2) | 6.4 (5.4–7.4) | 0.809 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Triglyceride (mg/dl) | 94 (70–131) | 108.5 (79–137.75) | 0.056 | 102 (74–148) | 118 (90–151.5) | 0.020 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Creatinine (mg/dl) | 0.67 (0.60–0.75) | 0.65 (0.58–0.74) | 0.223 | 0.89 (0.80–1.00) | 0.90 (0.77–1.01) | 0.677 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR (ml/min/1.73 m2) | 94.34 (85.81–100.33) | 94.98 (87.13–101.23) | 0.525 | 89.49 (79.97–95.98) | 86.66 (75.10–96.19) | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR | 8.09 (5.54–12.97) | 55.01 (36.78–97.44) | <0.001 | 6.06 (3.76–10.40) | 47.89 (36.15–72.67) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean cIMT (mm) | 0.6 (0.6–0.7) | 0.65 (0.6–0.7) | 0.445 | 0.7 (0.6–0.75) | 0.75 (0.66–0.90) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| cIMT ≥ 0.75 mm | 129 (22.8) | 16 (17.8) | 0.339 | 155 (32.0) | 45 (51.1) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Values are median (25th–75th percentile) or n (%). Abbreviations: BMI: body mass index; DM: diabetes mellitus; HDL: high density lipoprotein; LDL: low density lipoprotein; HbA1c: hemoglobin A1c; eGFR: estimated glomerular filtration rate; UACR: urine albumin creatinine ratio; cIMT: carotid intima-media thickness. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2 shows the correlation coefficients of CIMT and UACR with other variables in women and men. Age, HTN, waist circumference, and waist-to-height ratio were positively correlated with CIMT and UACR in both groups. Obesity and higher BMI were associated with CIMT and UACR only in women, while higher total body fat percentage was positively related to CIMT and UACR in men. Smoking, total serum cholesterol, and low-density cholesterol were unassociated with CIMT or UACR in men and women. Simple linear correlations between UACR and other CV risk factors, including total body fat percentage, BMI, and waist to height ratio by sex are displayed by scatter plots in Figure 1A–1C.
Table 2. Correlation coefficients of UACR and the carotid intima-media thickness with other cardiovascular risk factors in the whole population.
| Women | cIMT | UACR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 0.348** | 0.151** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 0.044 | 0.015 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 0.193** | 0.181** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 0.033 | 0.098* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome | 0.147** | 0.157** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist | 0.164** | 0.104** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 0.120** | 0.112** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 0.109** | 0.135** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total body fat percentage | 0.046 | −0.017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist to height ratio | 0.188** | 0.146** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR | −0.260** | −0.017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total Cholesterol | −0.029 | −0.045 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG | 0.091* | 0.092* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL | −0.002 | −0.014 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL | −0.090* | −0.060 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c | 0.081* | 0.080* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Uric acid | 0.134** | 0.033 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR | 0.093* | – | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Men | cIMT | UACR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 0.390** | 0.259** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 0.025 | 0.061 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 0.160** | 0.177** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 0.001 | 0.083* | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome | 0.066 | 0.114** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist | 0.149** | 0.164** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 0.078 | 0.065 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Obesity | 0.004 | 0.045 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total body fat percentage | 0.118** | 0.154** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist to height ratio | 0.212** | 0.225** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR | −0.220** | −0.124** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total Cholesterol | −0.024 | 0.044 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG | 0.015 | 0.111** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL | 0.041 | 0.052 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL | −0.092* | −0.015 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c | 0.070 | 0.128** | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Uric acid | 0.067 | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR | 0.187** | – | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| *Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2 tailed). Abbreviations: BMI: body mass index; HDL: high density lipoprotein; LDL: low density lipoprotein; HbA1c: hemoglobin A1c; eGFR: estimated glomerular filtration rate; UACR: urine albumin creatinine ratio; cIMT: carotid intima-media thickness. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
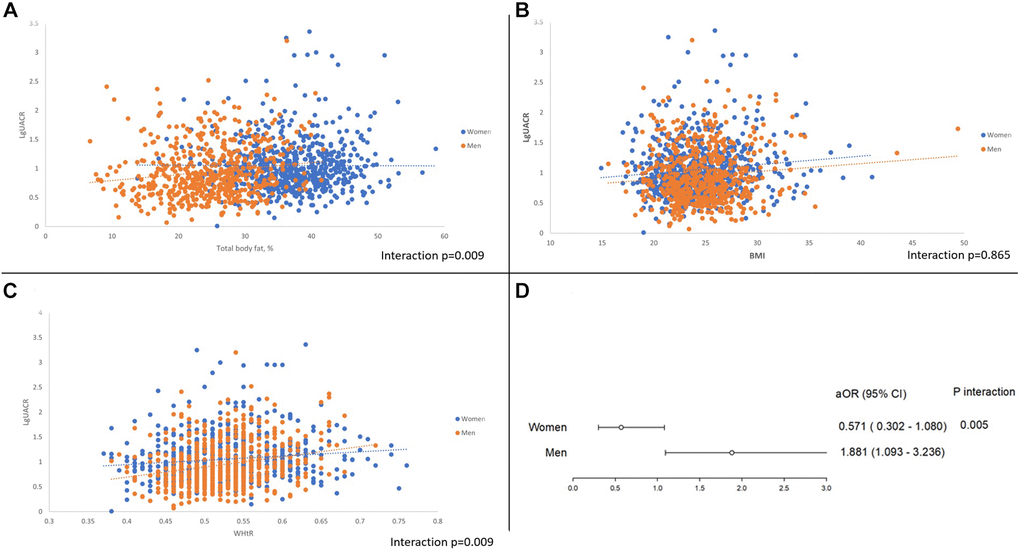
Figure 1. (A) Gender disparity between UACR and total body fat percentage. (B) Gender disparity between UACR and BMI. (C) Gender disparity between UACR and Waist to height ratio. (D) Pathological albuminuria and the adjusted odds ratio of subclinical atherosclerosis between sex.
Sex-based disparities are shown in Table 3. Multivariate logistic regression analysis of women showed that age (adjusted odds ratio [aOR] 1.076, 95% CI: 1.042–1.110) and HTN (aOR 2.089, 95% CI 1.223–3.570) were independently associated with SA but not PAU after adjusting for confounding factors (aOR 0.571, 95% CI 0.302–1.080). For men, independent factors related to SA were PAU (aOR 1.881, 95% CI 1.093–3.236), age (aOR 1.105, 95% CI 1.075–1.136), and BMI (aOR 1.149, 95% CI 1.039–1.271). After multivariate adjustment, the interaction between PAU and sex was significant (p = 0.005) (Figure 1D).
Table 3. Univariate and multivariate logistic regression analysis of factors associated with the incidence of cIMT ≥0.75 mm (75th percentile) in non-DM patients (n = 1228).
| Female (n = 655) Variable | Univariate analysis | Multivariate analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OR | 95% CI | p value | OR | 95% CI | p value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR ≥30 mg/g | 0.731 | 0.411−1.299 | 0.285 | 0.571 | 0.302−1.080 | 0.085 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 1.096 | 1.071−1.123 | <0.001 | 1.076 | 1.042−1.110 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 1.061 | 1.009−1.114 | 0.020 | 1.023 | 0.938−1.115 | 0.608 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 1.939 | 0.759−4.955 | 0.166 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 2.541 | 1.738−3.716 | <0.001 | 2.089 | 1.223−3.570 | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anti-HTN medications | 1.905 | 1.191−3.048 | 0.007 | 0.827 | 0.432−1.583 | 0.567 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 1.680 | 0.825−3.418 | 0.153 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total Cholesterol | 1.001 | 0.996−1.006 | 0.695 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG | 1.003 | 1.000−1.007 | 0.059 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL | 0.992 | 0.978−1.005 | 0.227 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL | 1.001 | 0.996−1.007 | 0.646 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA | 1.359 | 1.157−1.596 | <0.001 | 1.179 | 0.961−1.446 | 0.114 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBS | 1.001 | 0.983−1.019 | 0.939 | 0.982 | 0.960−1.004 | 0.103 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR | 0.953 | 0.938−0.968 | <0.001 | 0.993 | 0.970−1.016 | 0.529 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome | 2.061 | 1.387−3.063 | <0.001 | 1.486 | 0.824−2.678 | 0.188 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total body fat percentage | 1.005 | 0.975−1.035 | 0.766 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male (n = 573) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UACR ≥30 mg/g | 2.228 | 1.407−3.528 | 0.001 | 1.881 | 1.093−3.236 | 0.023 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | 1.087 | 1.065−1.109 | <0.001 | 1.105 | 1.075−1.136 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI | 1.055 | 1.003−1.110 | 0.039 | 1.149 | 1.039−1.271 | 0.007 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 1.045 | 0.727−1.501 | 0.812 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 2.046 | 1.426−2.934 | <0.001 | 1.660 | 0.951−2.898 | 0.075 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anti-HTN medications | 1.518 | 0.978−2.357 | 0.063 | 0.714 | 0.360−1.416 | 0.335 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 1.253 | 0.504−3.119 | 0.627 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total Cholesterol | 0.998 | 0.993−1.004 | 0.521 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG | 0.998 | 0.996−1.000 | 0.080 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL | 0.992 | 0.979−1.006 | 0.272 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL | 1.003 | 0.997−1.008 | 0.291 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA | 1.094 | 0.965−1.240 | 0.160 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FBS | 0.999 | 0.982−1.016 | 0.897 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR | 0.974 | 0.960−0.989 | 0.001 | 1.007 | 0.986−1.029 | 0.508 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Metabolic syndrome | 1.364 | 0.913−2.036 | 0.130 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total body fat percentage | 1.037 | 1.009−1.066 | 0.009 | 0.976 | 0.930−1.025 | 0.338 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BMI: body mass index; HTN: hypertension; TG: triglyceride; HDL: high density lipoprotein; LDL: low density lipoprotein; UA: uric acid; FBS: fasting blood sugar; eGFR: estimated glomerular filtration rate. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
The present study investigated whether an association of PAU with SA may be sex-determined in subjects without CAD, DM, or CKD. Men with PAU were older, had larger waist circumference, and exhibited a higher prevalence of HTN and metabolic syndrome than those with normal UACR. After adjusting for confounding factors, PAU was significantly associated with SA in men, but not in women.
PAU and sex difference
We recruited healthy individuals and focused on sex-based differences in the prevalence of PAU and SA. In previous studies, age-related increases of urinary albumin excretion are more pronounced in men than in women [20, 21]. Studies of potential sex-based differences in the association of obesity and MA have reached divergent conclusions in different regions and race.
Foster et al. [22] found that visceral adipose tissue volume determined by multi-detector computed tomography was related to MA in men but not in women and the similar result was found in Japan and Singapore studies [23, 24]. In contrast, two cross-sectional studies in Chinese and Korea revealed that women with central obesity tended to develop albuminuria but insignificant relationship between albuminuria and obesity in men [25, 26]. Our data support that in men, microalbuminuria is the clusters with the components of MetS, especially central obesity more propensity than women, consistent with a finding in 408,527 UK Biobank participants that each 0.06 increase of waist-to-hip ratio was associated with 75% (71–79%) and 40% (38–43%) increases in odds of higher UACR in men and women, respectively [27]. This suggests that the long-term sequelae of obesity, fat metabolism, and fat deposition may differ between men and women.
PAU and the risk of CVD and CIMT
The potential clinical utility of MA as a marker of endothelial dysfunction, which precedes atherosclerosis, has been suggested by studies in type I and type II DM [28, 29]. In the PREVEND study of 7579 non-diabetic, non-hypertensive individuals, MA, defined as urinary albumin excretion 20–200 mg/L, was also linked to ECG evidence of either myocardial infarction or ischemia [30].
Sex-specific associations were an important part of this study. One of the possible reasons is that numerous changes in vascular function influenced by aging and sex hormones may interact in multiple pathways to dysregulate endothelial function. During aging, lower levels of the testosterone precursor dehydroepiandrosterone (DHEA) may promote central obesity, insulin resistance, and sarcopenia, predominantly in men [31, 32]. Elevated serum PAI-1 [33], endothelin [34], von Willebrand factor [35], and oxidative stress may trigger mechanisms linking MA and SA, and the male rats with spontaneous hypertension related much of the pro-atherosclerotic markers with MA than female rats [36–39]. Another possible reason is that the impact of potential confounders on PAU and CIMT may be greater in females.
A Korean cross-sectional study of adults aged 45 to 74 years showed a significant association between high normal UACR (<30 mg/g) and CIMT >0.9 mm without sex difference [40]. Another single-center prospective 15-year follow-up study with 3128 participants reported significant sex differences in the relationship between triglycerides, smoking, physical activity, and the risk of atherosclerosis [41], UACR is not related to atherosclerosis. According to the Kidney Disease: Improving Global Outcomes working group suggests that UACR ≥30 mg/g indicates a moderate risk of CKD even in the normal eGFR, our study separated the UACR according to whether more than 30 mg/g or not. The clinical utility of MA as a standard independent risk indicator in the absence of diabetes is still debated, and the association of elevated UACR with CIMT may differ by sex; the evidence is limited. Our study demonstrated sex-based disparity in the association of PAU with SA in the relatively healthy community dwelling populations.
Limitations
Several limitations of our study should be mentioned. First, the retrospective and observational study design could not fully assess the etiologic relationship between PAU, CVD risk factors, and SA. Second, although the measurement of albumin and creatinine from spot urine samples is straightforward, results may be less accurate than those of 24-hour urine collections. Third, confounding effects of diet, exercise, and psychological stress of 24-hour urine collections could not be excluded. Fourth, the cross-sectional cohort study lacked the long-term follow-up characteristic of longitudinal study designs; thus, we could not investigate the impact of PAU on the risk of CVD. Fifth, a potential residual confounding effect of PAU between men and women may explain the discrepant associations between UACR and SA. Sixth, the binary classification of CIMT as greater or less than the 75th percentile was an indirect assay of the severity of carotid atherosclerosis. Seventh, this study did not identify the pathogenic link between albuminuria level and the severity of atherosclerosis.
Conclusion
This retrospective cohort study demonstrated a sex-based disparity in the association of PAU with SA in patients without CAD, DM, or CKD after adjusting for traditional risk factors of atherosclerosis. Our findings suggest a sex-specific risk management strategy for preventing atherosclerosis.
Methods
Study population
This retrospective cohort study was excerpted from the first wave of the I-Lan Longitudinal Aging Study (ILAS), a cohort study of community-dwelling adults aged more than 50 years who were randomly recruited through household registration records. The ILAS design, participant recruitment, and data collection have been reported previously [42]. Exclusion criteria of the present study were: (i) inability to cooperate or communicate with study investigators; (ii) declined to grant consent; (iii) currently institutionalized; comorbidities, such as active cancer, sepsis, heart failure, chronic obstructive pulmonary disease, or functional dependence; (v) life expectancy of less than six months; and (vi) planned to leave I-Lan county. A total of 1,839 community-dwelling older adults were enrolled from August 2011 to August 2013. After in-person face-to-face interviews conducted by well-trained research nurses, all participants provided written informed consent. Three hundred eighty-two subjects were excluded, including 88 with coronary artery disease, 124 with incomplete data, 320 with DM, and 79 with renal dysfunction (Figure 2). The study protocol complied with the Declaration of Helsinki and was approved by the institutional review board of the National Yang-Ming University (YM103008).
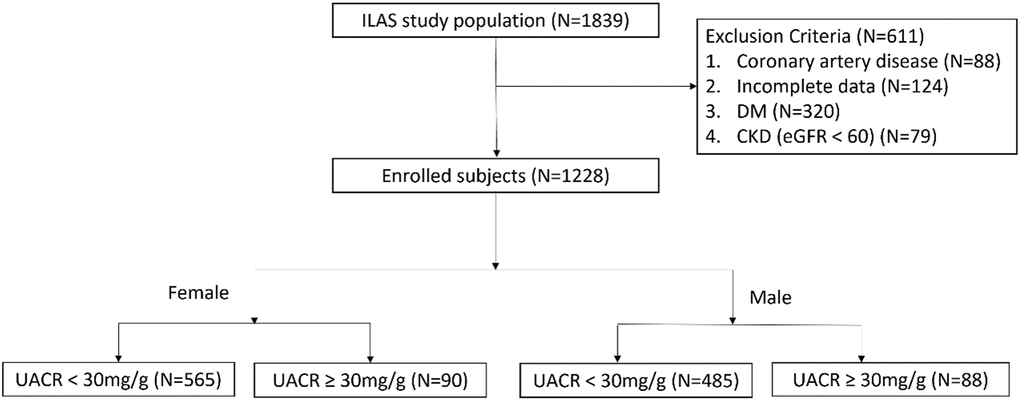
Figure 2. Flow chart of patient enrollment.
Anthropometry, demography, and laboratory examinations
The research nurse collected the participants’ demographic and medical data, including weight, height, BMI, and waist circumference. Brachial blood pressure was measured with a mercury sphygmomanometer after the subjects rested for 15 min. Medical histories of underlying diseases, medications, and smoking were obtained from personal interviews and medical records. Peripheral blood samples were collected at 7–9 AM, after fasting for at least ten hours, to determine the concentrations of hemoglobin A1c, fasting blood glucose, total cholesterol, HDL, LDL, triglyceride, uric acid, and high-sensitivity C-reactive protein by using an automatic analyzer (ADVIA 1800; Siemens, Malvern, PA, USA).
Metabolic syndrome was defined according to the criteria proposed by Taiwan’s Ministry of Health and Welfare, with more than three of the following risk determinants: (i) waist circumference >90 cm for men or >80 cm for women; (ii) systolic blood pressure ≥130 mmHg, diastolic blood pressure ≥85 mmHg, or taking antihypertensive agents; (iii) HDL <40 mg/dL for men or <50 mg/dL for women; triglyceride ≥150 mg/dL; (iv) fasting blood glucose ≥100 mg/dL or antihyperglycemic therapy. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [43]. Renal dysfunction was defined as a glomerular filtration rate of <60 (mL × min–1 per 1.73 m2 body surface area) according to the 2012 KDIGO CKD classification [44].
All participants underwent whole-body dual-energy X-ray absorptiometry to measure total fat weight with a Lunar Prodigy instrument (GE Healthcare, Madison, WI, USA). Total fat percentage was defined as total fat weight divided by total body mass.
Definition of albuminuria
A single voided morning urine sample was used to measure UACR (mg/g). UACR measured in a spot urine sample is highly correlated with 24-h urine albumin excretion [45]. UACR ≥30 mg/g was considered pathological [46]. Patients were separated into two groups whether UACR ≥30 mg/g. The flowchart of patient enrollment and classification is illustrated in Figure 2.
Assessment of CIMT and SA
CIMT was measured using a high-resolution, broad-width, linear array transducer (LOGIQ 400 PRO; GE, Cleveland, OH, USA) at the level of the common carotid artery. All examinations were performed by the same trained technician who obtained bilateral longitudinal views of the proximal to distal sections of the common carotid arteries. The mean CIMT was defined as the average of right-and left-side CIMT values. The 75th percentile of CIMT was defined as the upper limit of normal, the threshold indicative of increased cardiovascular risk and early phase of SA [47, 48]. In the present study, the 75th percentile of CIMT was 0.75 mm.
Statistical analysis
Data were expressed as frequencies (percentages) for categorical variables and as means ± standard deviations for continuous variables with normal distribution and median with the interquartile range due to non-normal distribution. The chi-square test was used for comparisons between two groups of categorical variables. The independent t-test was employed for continuous variables with normal distribution. The Kruskal-Wallis test was used for non-normally distributed continuous variables. Pearson and Spearman’s tests were used to assess the correlation between the UACR and CIMT with other variables. Associations between factors and SA were expressed as odds ratios (ORs). Multivariate logistic regression evaluated the SA by dividing both sexes after using the enter methods to explore the association between microalbuminuria and subclinical atherosclerosis and other variables. ORs with 95% confidence intervals (95% CI) for the risk of CIMT ≥0.75 mm were reported. Statistical analyses were performed using SPSS (version 22.0; IBM Corporation, Armonk, New York, NY, USA). Two-tailed p values <0.05 were regarded as statistically significant.
Consent for publication
No individual participant data were reported that would require consent from the participant to publish.
Availability of data and materials
The dataset used and analyzed during the current study is available from the corresponding author upon request.
Author Contributions
Data were interpreted and analyzed by YWL and CCC with assistance from RHC and YLT. YWL drafted the manuscript. CCC and PHH revised the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
The study protocol complied with the Declaration of Helsinki and was approved by the institutional review board of the National Yang-Ming University (YM103008). All participants provided written informed consent.
Funding
This study was supported in part by research grants from the Novel Bioengineering and Technological Approaches to Solve Two Major Health Problems in Taiwan program, sponsored by the Taiwan Ministry of Science and Technology Academic Excellence Program (MOST 108-2633-B-009-001); Taipei Veterans General Hospital (VGH-V100E2-002 and VGHUST103-G7-2-1); the National Taiwan University Hospital, Hsinchu Branch (107-HCH002 and 108-HCH004); and the Ministry of Science and Technology (MOST-105-2314-B-002-119, 106-2314-B-002-173-MY3, MOHW 106-TDU-B-211-113001). The funding institutions took no part in the study design, data collection or analysis, publication intent, or manuscript preparation.
References
- 1. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, Bonny A, Brauer M, Brodmann M, et al, and GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020; 76:2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010 [PubMed]
- 2. Francula-Zaninovic S, Nola IA. Management of Measurable Variable Cardiovascular Disease' Risk Factors. Curr Cardiol Rev. 2018; 14:153–63. https://doi.org/10.2174/1573403X14666180222102312 [PubMed]
- 3. de Jong PE, Brenner BM. From secondary to primary prevention of progressive renal disease: the case for screening for albuminuria. Kidney Int. 2004; 66:2109–18. https://doi.org/10.1111/j.1523-1755.2004.66001.x [PubMed]
- 4. de Zeeuw D. Albuminuria, just a marker for cardiovascular disease, or is it more? J Am Soc Nephrol. 2005; 16:1883–5. https://doi.org/10.1681/ASN.2005050524 [PubMed]
- 5. Boyd C, Wood K, Whitaker D, Ashorobi O, Harvey L, Oster R, Holmes RP, Assimos DG. Accuracy in 24-hour Urine Collection at a Tertiary Center. Rev Urol. 2018; 20:119–24. [PubMed]
- 6. Toto RD. Microalbuminuria: definition, detection, and clinical significance. J Clin Hypertens (Greenwich). 2004; 6:2–7. https://doi.org/10.1111/j.1524-6175.2004.4064.x [PubMed]
- 7. Smith ER, Cai MM, McMahon LP, Wright DA, Holt SG. The value of simultaneous measurements of urinary albumin and total protein in proteinuric patients. Nephrol Dial Transplant. 2012; 27:1534–41. https://doi.org/10.1093/ndt/gfr708 [PubMed]
- 8. Lee M, Saver JL, Chang KH, Liao HW, Chang SC, Ovbiagele B. Impact of microalbuminuria on incident stroke: a meta-analysis. Stroke. 2010; 41:2625–31. https://doi.org/10.1161/STROKEAHA.110.581215 [PubMed]
- 9. Howard BV, Lee ET, Cowan LD, Fabsitz RR, Howard WJ, Oopik AJ, Robbins DC, Savage PJ, Yeh JL, Welty TK. Coronary heart disease prevalence and its relation to risk factors in American Indians. The Strong Heart Study. Am J Epidemiol. 1995; 142:254–68. https://doi.org/10.1093/oxfordjournals.aje.a117632 [PubMed]
- 10. Fabsitz RR, Sidawy AN, Go O, Lee ET, Welty TK, Devereux RB, Howard BV. Prevalence of peripheral arterial disease and associated risk factors in American Indians: the Strong Heart Study. Am J Epidemiol. 1999; 149:330–8. https://doi.org/10.1093/oxfordjournals.aje.a009817 [PubMed]
- 11. Hermans MM, Henry RM, Dekker JM, Nijpels G, Heine RJ, Stehouwer CD. Albuminuria, but not estimated glomerular filtration rate, is associated with maladaptive arterial remodeling: the Hoorn Study. J Hypertens. 2008; 26:791–7. https://doi.org/10.1097/HJH.0b013e3282f50066 [PubMed]
- 12. Cirillo M, Laurenzi M, Panarelli P, Mancini M, Zanchetti A, De Santo NG. Relation of urinary albumin excretion to coronary heart disease and low renal function: role of blood pressure. Kidney Int. 2004; 65:2290–7. https://doi.org/10.1111/j.1523-1755.2004.00652.x [PubMed]
- 13. Nezu T, Hosomi N, Aoki S, Matsumoto M. Carotid Intima-Media Thickness for Atherosclerosis. J Atheroscler Thromb. 2016; 23:18–31. https://doi.org/10.5551/jat.31989 [PubMed]
- 14. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, Najjar SS, Rembold CM, Post WS, and American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008; 21:93–111. https://doi.org/10.1016/j.echo.2007.11.011 [PubMed]
- 15. Sinning C, Wild PS, Echevarria FM, Wilde S, Schnabel R, Lubos E, Herkenhoff S, Bickel C, Klimpe S, Gori T, Münzel TF, Blankenberg S, Espinola-Klein C, and Gutenberg-Heart Study. Sex differences in early carotid atherosclerosis (from the community-based Gutenberg-Heart Study). Am J Cardiol. 2011; 107:1841–7. https://doi.org/10.1016/j.amjcard.2011.02.318 [PubMed]
- 16. Yao L, Folsom AR, Alonso A, Lutsey PL, Pankow JS, Guan W, Cheng S, Lederle FA, Tang W. Association of carotid atherosclerosis and stiffness with abdominal aortic aneurysm: The atherosclerosis risk in communities (ARIC) study. Atherosclerosis. 2018; 270:110–6. https://doi.org/10.1016/j.atherosclerosis.2018.01.044 [PubMed]
- 17. Kokubo Y, Watanabe M, Higashiyama A, Nakao YM, Nakamura F, Miyamoto Y. Impact of Intima-Media Thickness Progression in the Common Carotid Arteries on the Risk of Incident Cardiovascular Disease in the Suita Study. J Am Heart Assoc. 2018; 7:e007720. https://doi.org/10.1161/JAHA.117.007720 [PubMed]
- 18. Agewall S, Wikstrand J, Ljungman S, Fagerberg B. Urinary albumin excretion is associated with the intima-media thickness of the carotid artery in hypertensive males with non-insulin-dependent diabetes mellitus. J Hypertens. 1995; 13:463–9. [PubMed]
- 19. Pedrinelli R, Dell'Omo G, Penno G, Bandinelli S, Giannini D, Balbarini A, Mariani M. Dissociation between microalbuminuria and common carotid thickness in essential hypertensive men. J Hum Hypertens. 2000; 14:831–5. https://doi.org/10.1038/sj.jhh.1001123 [PubMed]
- 20. Cirillo M, Senigalliesi L, Laurenzi M, Alfieri R, Stamler J, Stamler R, Panarelli W, De Santo NG. Microalbuminuria in nondiabetic adults: relation of blood pressure, body mass index, plasma cholesterol levels, and smoking: The Gubbio Population Study. Arch Intern Med. 1998; 158:1933–9. https://doi.org/10.1001/archinte.158.17.1933 [PubMed]
- 21. Halimi JM, Forhan A, Balkau B, Novak M, Wilpart E, Tichet J, Marre M, and D.E.S.I.R. Study Group. Is microalbuminuria an integrated risk marker for cardiovascular disease and insulin resistance in both men and women? J Cardiovasc Risk. 2001; 8:139–46. https://doi.org/10.1177/174182670100800304 [PubMed]
- 22. Foster MC, Hwang SJ, Massaro JM, Hoffmann U, DeBoer IH, Robins SJ, Vasan RS, Fox CS. Association of subcutaneous and visceral adiposity with albuminuria: the Framingham Heart Study. Obesity (Silver Spring). 2011; 19:1284–9. https://doi.org/10.1038/oby.2010.308 [PubMed]
- 23. Iseki K. Body mass index and the risk of chronic renal failure: the Asian experience. Contrib Nephrol. 2006; 151:42–56. https://doi.org/10.1159/000095318 [PubMed]
- 24. Shankar A, Leng C, Chia KS, Koh D, Tai ES, Saw SM, Lim SC, Wong TY. Association between body mass index and chronic kidney disease in men and women: population-based study of Malay adults in Singapore. Nephrol Dial Transplant. 2008; 23:1910–8. https://doi.org/10.1093/ndt/gfm878 [PubMed]
- 25. Lin WY, Pi-Sunyer FX, Liu CS, Li CI, Davidson LE, Li TC, Lin CC. Central obesity and albuminuria: both cross-sectional and longitudinal studies in Chinese. PLoS One. 2012; 7:e47960. https://doi.org/10.1371/journal.pone.0047960 [PubMed]
- 26. Noh HM, Kim UY, Park YS, Song YR, Oh HY, Park KH, Paek YJ, Roh YK, Song HJ. Sex differences in the association between obesity and albuminuria among Korean adults: a cross-sectional study using the Korea National Health and Nutrition Examination Survey data. Clin Exp Nephrol. 2017; 21:27–34. https://doi.org/10.1007/s10157-016-1238-z [PubMed]
- 27. Zhu P, Lewington S, Haynes R, Emberson J, Landray MJ, Cherney D, Woodward M, Baigent C, Herrington WG, Staplin N. Cross-sectional associations between central and general adiposity with albuminuria: observations from 400,000 people in UK Biobank. Int J Obes (Lond). 2020; 44:2256–66. https://doi.org/10.1038/s41366-020-0642-3 [PubMed]
- 28. Järvisalo MJ, Raitakari M, Toikka JO, Putto-Laurila A, Rontu R, Laine S, Lehtimäki T, Rönnemaa T, Viikari J, Raitakari OT. Endothelial dysfunction and increased arterial intima-media thickness in children with type 1 diabetes. Circulation. 2004; 109:1750–5. https://doi.org/10.1161/01.CIR.0000124725.46165.2C [PubMed]
- 29. Siddiqi FS, Advani A. Endothelial-podocyte crosstalk: the missing link between endothelial dysfunction and albuminuria in diabetes. Diabetes. 2013; 62:3647–55. https://doi.org/10.2337/db13-0795 [PubMed]
- 30. Hillege HL, Janssen WM, Bak AA, Diercks GF, Grobbee DE, Crijns HJ, Van Gilst WH, De Zeeuw D, De Jong PE, and Prevend Study Group. Microalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity. J Intern Med. 2001; 249:519–26. https://doi.org/10.1046/j.1365-2796.2001.00833.x [PubMed]
- 31. Tchernof A, Labrie F. Dehydroepiandrosterone, obesity and cardiovascular disease risk: a review of human studies. Eur J Endocrinol. 2004; 151:1–14. https://doi.org/10.1530/eje.0.1510001 [PubMed]
- 32. Yoon HE, Nam Y, Kang E, Hwang HS, Shin SJ, Hong YS, Kang KY. Gender-Specific Associations between Low Skeletal Muscle Mass and Albuminuria in the Middle-Aged and Elderly Population. Int J Med Sci. 2017; 14:1054–64. https://doi.org/10.7150/ijms.20286 [PubMed]
- 33. Stehouwer CD, Lambert J, Donker AJ, van Hinsbergh VW. Endothelial dysfunction and pathogenesis of diabetic angiopathy. Cardiovasc Res. 1997; 34:55–68. https://doi.org/10.1016/s0008-6363(96)00272-6 [PubMed]
- 34. Takahashi K, Ghatei MA, Lam HC, O'Halloran DJ, Bloom SR. Elevated plasma endothelin in patients with diabetes mellitus. Diabetologia. 1990; 33:306–10. https://doi.org/10.1007/BF00403325 [PubMed]
- 35. Stehouwer CD, Nauta JJ, Zeldenrust GC, Hackeng WH, Donker AJ, den Ottolander GJ. Urinary albumin excretion, cardiovascular disease, and endothelial dysfunction in non-insulin-dependent diabetes mellitus. Lancet. 1992; 340:319–23. https://doi.org/10.1016/0140-6736(92)91401-s [PubMed]
- 36. Maeda S, Tanabe T, Miyauchi T, Otsuki T, Sugawara J, Iemitsu M, Kuno S, Ajisaka R, Yamaguchi I, Matsuda M. Aerobic exercise training reduces plasma endothelin-1 concentration in older women. J Appl Physiol (1985). 2003; 95:336–41. https://doi.org/10.1152/japplphysiol.01016.2002 [PubMed]
- 37. Bryk D, Olejarz W, Zapolska-Downar D. The role of oxidative stress and NADPH oxidase in the pathogenesis of atherosclerosis. Postepy Hig Med Dosw (Online). 2017; 71:57–68. https://doi.org/10.5604/17322693.1229823 [PubMed]
- 38. Wenner MM, Sebzda KN, Kuczmarski AV, Pohlig RT, Edwards DG. ETB receptor contribution to vascular dysfunction in postmenopausal women. Am J Physiol Regul Integr Comp Physiol. 2017; 313:R51–7. https://doi.org/10.1152/ajpregu.00410.2016 [PubMed]
- 39. Poznyak AV, Grechko AV, Orekhova VA, Chegodaev YS, Wu WK, Orekhov AN. Oxidative Stress and Antioxidants in Atherosclerosis Development and Treatment. Biology (Basel). 2020; 9:60. https://doi.org/10.3390/biology9030060 [PubMed]
- 40. Kweon SS, Shin MH, Lee YH, Choi JS, Nam HS, Park KS, Kim DH, Jeong SK. Higher normal ranges of urine albumin-to-creatinine ratio are independently associated with carotid intima-media thickness. Cardiovasc Diabetol. 2012; 11:112. https://doi.org/10.1186/1475-2840-11-112 [PubMed]
- 41. Stensland-Bugge E, Bønaa KH, Joakimsen O, Njølstad I. Sex differences in the relationship of risk factors to subclinical carotid atherosclerosis measured 15 years later: the Tromsø study. Stroke. 2000; 31:574–81. https://doi.org/10.1161/01.str.31.3.574 [PubMed]
- 42. Liu LK, Lee WJ, Chen LY, Hwang AC, Lin MH, Peng LN, Chen LK. Sarcopenia, and its association with cardiometabolic and functional characteristics in Taiwan: results from I-Lan Longitudinal Aging Study. Geriatr Gerontol Int. 2014 (Suppl 1); 14:36–45. https://doi.org/10.1111/ggi.12208 [PubMed]
- 43. Earley A, Miskulin D, Lamb EJ, Levey AS, Uhlig K. Estimating equations for glomerular filtration rate in the era of creatinine standardization: a systematic review. Ann Intern Med. 2012; 156:785–95. [PubMed]
- 44. Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, Kurella Tamura M, Feldman HI. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014; 63:713–35. https://doi.org/10.1053/j.ajkd.2014.01.416 [PubMed]
- 45. Vart P, Scheven L, Lambers Heerspink HJ, de Jong PE, de Zeeuw D, Gansevoort RT, and PREVEND Study Group and the RENAAL Investigators. Urine Albumin-Creatinine Ratio Versus Albumin Excretion for Albuminuria Staging: A Prospective Longitudinal Cohort Study. Am J Kidney Dis. 2016; 67:70–8. https://doi.org/10.1053/j.ajkd.2015.05.025 [PubMed]
- 46. Mogensen CE, Chachati A, Christensen CK, Close CF, Deckert T, Hommel E, Kastrup J, Lefebvre P, Mathiesen ER, Feldt-Rasmussen B. Microalbuminuria: an early marker of renal involvement in diabetes. Uremia Invest. 1985; 9:85–95. https://doi.org/10.3109/08860228509088195 [PubMed]
- 47. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CH, Azen SP. The role of carotid arterial intima-media thickness in predicting clinical coronary events. Ann Intern Med. 1998; 128:262–9. https://doi.org/10.7326/0003-4819-128-4-199802150-00002 [PubMed]
- 48. Mohan A, Sada S, Kumar BS, Sarma KV, Devi BV, Rao PV, Rajasekhar D, Katyarmal DT. Subclinical atherosclerosis in patients with rheumatoid arthritis by utilizing carotid intima-media thickness as a surrogate marker. Indian J Med Res. 2014; 140:379–86. [PubMed]