



Introduction
Arterial stiffness indicates an impaired capability of arterial vessels to expand and contract as a reaction to blood pressure changes [1]. Previous studies have shown that atherosclerotic risk factors such as aging, cigarette smoking, hypertension, diabetes, dyslipidemia, and hyperuricemia are linked to increased arterial stiffness [2, 3]. Furthermore, arterial stiffness is a surrogate marker of atherosclerosis and a risk factor for several cardiovascular (CV) diseases, including stroke [1, 4, 5]. Furthermore, a previous study demonstrated that increased arterial stiffness is associated with both CV disease-associated mortality and all-cause mortality [6]. Therefore, identifying potential risk factors of arterial stiffness may be clinically significant for preventing and managing CV diseases.
In clinical practice, arterial stiffness is commonly assessed by measuring pulse wave velocity (PWV) [7]. Brachial-ankle PWV (baPWV) is measured using a noninvasive vascular screening device evaluating the participant’s blood pressure and pulse waves in the bilateral brachial and tibial arteries. The baPWV value is then calculated by dividing the distance traveled by the pulse wave by the time interval taken for the waveform to travel to such a distance [7]. BaPWV is a well-established index for evaluating arterial stiffness and has been widely used clinically [7–9]. Studies have also demonstrated a positive association between high baPWV value and CV diseases, such as acute myocardial infarction [10], congestive heart failure [11], and even all-cause mortality [12].
Platelets originally played an essential role in the regulation of hemostasis and thrombosis [13]. Furthermore, platelet function and activation were further found to be associated with inflammation and the pathogenesis of atherosclerosis. A high platelet count predicts the risk of acute coronary syndrome [14]. Additionally, mean platelet volume (MPV), one indicator of platelet activation [15], was associated with CV disease [16], hypertension [17], stroke [18], and congestive heart failure [19]. However, studies focusing on arterial stiffness and platelet indicators are very rare. MPV was demonstrated to be associated with baPWV [20, 21]. As for platelet count and arterial stiffness, only one cohort study showed that increased platelet count is related to higher baPWV values in elderly patients with diabetes [22]. However, although platelet counts were shown to be attenuated in the elderly [23] and MPV values may be easily affected by cigarette smoking [24], those confounders were not well considered in previous studies. Furthermore, studies evaluating platelet count in young and middle-aged adults are lacking.
Therefore, we aimed to investigate the association between platelet count and MPV with arterial stiffness in a middle-aged population.
Methods
Study population
The participants of this study were recruited from those who underwent health checkups at the National Cheng Kung University Hospital (NCKUH) health management center from November 2018 to December 2019. We excluded subjects aged <18 or >50 years; who are pregnant; on medication for dyslipidemia; and with abnormal platelet count (<150,000/μL or > 450,000/μL), incomplete data, and past history of hematologic disorders. The detailed exclusion process was shown in Figure 1. The analysis was based on delinked secondary data without personally identifiable information, and the institutional review board approved the study protocol at NCKUH (IRB Number: B-ER-108-326). Informed consent was waived because the analysis was based on anonymous data.
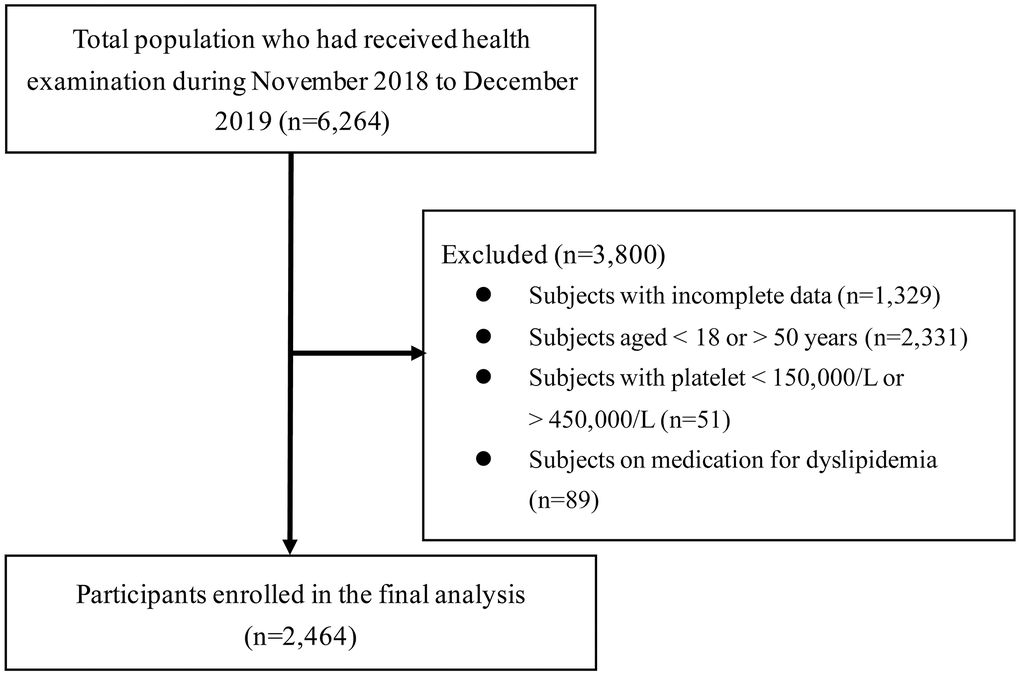
Figure 1. Flow diagram showing the exclusion process for selecting eligible participants.
All the participants were asked to complete a self-administered questionnaire to assess personal and family medical history and lifestyle factors. The status of cigarette smoking and alcohol use was also obtained, and the participants were categorized into noncurrent and current users. Participants who had smoked at least one pack per month or had alcohol consumption of at least one drink per week for the past 6 months were defined as current smokers and current alcohol users, respectively [25]. Additionally, regular exercisers were individuals who engaged in an intense activity for a minimum of 30 min each time and at least three times per week and were defined to have regular exercise habits.
We measured each subject’s body weight and height, and the body mass index (BMI) was calculated as weight (kg)/height (m2). Those with BMI ≥27 kg/m2 were obese according to the domestic authority [26]. The right brachial systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured after the participants rested for at least 10 min. Hypertension was defined as (1) SBP ≥140 mmHg, (2) DBP ≥90 mmHg, or (3) past medical history of hypertension [27]. Then, each participant had their blood drawn to gather biochemical and hematological information. Platelet, white blood cell (WBC), and red blood cell (RBC) counts (WBC) and MPV, hemoglobin, fasting plasma glucose (FPG), glycated hemoglobin (HbA1c), alanine aminotransferase, aspartate aminotransferase, creatinine, total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C), triglyceride (TG), high-density lipoprotein-cholesterol (HDL-C), high sensitivity C-reactive protein (hs-CRP), and uric acid levels were measured. Diabetes mellitus was defined as (1) FPG level ≥126 mg/dL, (2) HbA1c level ≥6.5%, or (3) a history of diabetes [28]. Hyperuricemia was defined as a serum uric acid level >7.0 mg/dL in men and >6.0 mg/dL in women [29].
Assessment of platelets
Subjects were further categorized into subgroups based on their platelet count and MPV levels. According to the quartiles of platelet count, we categorized the participants into four subgroups: (1) Q1, platelet count ≥150,000–215,000/μL; (2) Q2, platelet count ≥216,000–248,000/μL; (3) Q3, platelet count ≥249,000–289,000/μL; and (4) Q4, platelet count ≥290,000–450,000/μL. We also divided the participants into quartiles by their MPV levels: (1) Q1, MPV ≥6.2–7.7 fL; (2) Q2, MPV ≥7.8–8.2 fL; (3) Q3, MPV ≥8.3–8.8 fL; and (4) Q4, MPV ≥8.9–11.8 fL.
Assessment of arterial stiffness
BaPWV was used to evaluate arterial stiffness. The baPWV value was measured using a noninvasive vascular screening device (BP-203RPE II; Colin Medical Technology, Komaki, Japan) with pneumatic pressure cuffs covering the bilateral ankles and upper arms. Each participant’s blood pressure and pulse waves in the bilateral brachial and tibial arteries were simultaneously assessed while in a supine position for at least 5 min. The baPWV value was then calculated automatically by dividing the distance traveled by pulse wave (the distance from the brachial area to the ankle) by the time interval taken for the waveform to travel to such a distance. BaPWV >1400 cm/s were defined as increased arterial stiffness.
Statistical analysis
SPSS software (v.17.0, SPSS, Inc., Chicago, IL) was used for data analysis. Continuous variables were expressed as mean ± standard deviations, and categorical variables were presented as numbers (percentages). Independent t-tests and Pearson’s chi-square analysis were performed both in total subjects and by gender to compare continuous and categorical variables between the participants with and without increased arterial stiffness. In multivariate analysis, both linear and binary logistic regression models were performed to evaluate the association of platelet count and MPV levels with baPWV values and increased arterial stiffness (baPWV >1400 cm/s). Among the adjustment variables were age, sex, BMI, SBP, TC/HDL-C ratio, uric acid, creatinine, hs-CRP, cigarette smoking, and regular exercise. The binary logistic regression model was also conducted by males and females separately to examine the gender difference between the association of platelet-associated parameter and arterial stiffness. A P value <0.05 was defined as statistically significant.
Results
Table 1 compares the demographic characteristics of subjects with and without increased arterial stiffness. Participants with increased arterial stiffness were mostly men and had higher BMI, SBP, DBP, FPG, TC, LDL-C, TG, uric acid, creatinine, WBC, RBC, hemoglobin, and hs-CRP levels than those with normal baPWV levels. Additionally, individuals with increased arterial stiffness had higher hypertension, diabetes, and cigarette smoking rates in total participants. Besides, in both males and females, those with increased arterial stiffness had higher BMI, SBP, DBP, FPG, TC, LDL-C, TG, uric acid, and hs-CRP levels than those with normal baPWV when analyzed separately (shown in Supplementary Table 1).
Table 1. Comparisons of clinical characteristics among subjects with and without increased arterial stiffness (baPWV >1,400 cm/s).
| Variables | Increased arterial stiffness | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No (n = 2,125) | Yes (n = 339) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 40.1 ± 6.5 | 43.7 ± 4.9 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 1190 (56.0) | 275 (81.1) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 125 (5.9) | 144 (42.5) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes mellitus | 46 (2.2) | 22 (6.5) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hyperuricemia | 590 (27.8) | 148 (43.7) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current alcohol use | 318 (15.0) | 85 (25.1) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoking | 260 (12.2) | 71 (20.9) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exercise ≥ 3/wk | 935 (44.0) | 157 (46.3) | 0.426 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2 | 23.6 ± 3.7 | 25.4 ± 3.6 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP, mmHg | 114.5 ± 11.9 | 134.8 ± 13.5 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DBP, mmHg | 68.1 ± 9.5 | 84.1 ± 10.5 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FPG, mg/dL | 91.3 ± 13.8 | 98.9 ± 28.9 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT, U/L | 29.2 ± 27.3 | 38.9 ± 27.5 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST, U/L | 24.5 ± 15.0 | 27.7 ± 12.2 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cholesterol, mg/dL | 186.1 ± 33.6 | 198.3 ± 36.0 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Triglyceride, mg/dL | 114.2 ± 75.5 | 150.8 ± 88.9 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C, mg/dL | 54.8 ± 15.5 | 48.7 ± 13.9 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C, mg/dL | 129.2 ± 33.5 | 142.0 ± 35.1 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cholesterol/HDL-C | 3.7 ± 1.2 | 4.3 ± 1.3 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Creatinine, mg/dL | 0.74 ± 0.18 | 0.80 ± 0.17 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Uric acid, mg/dL | 5.9 ± 1.5 | 6.7 ± 1.5 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC, 103/μL | 5.8 ± 1.5 | 6.2 ± 1.6 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBC, 106/μL | 4.86 ± 0.54 | 5.13 ± 0.47 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hemoglobin, g/dL | 14.2 ± 1.6 | 15.1 ± 1.6 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| hs-CRP, mg/L | 1.89 ± 3.59 | 2.74 ± 4.25 | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data expressed as mean ± standard deviation or number (percent). Abbreviations: baPWV: brachial-ankle pulse wave velocity; ALT: alanine aminotransferase; AST: aspartate aminotransferase; BMI: body mass index; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HDL-C: high-density lipoprotein-cholesterol; hs-CRP: high sensitivity C-reactive protein; LDL-C: low-density lipoprotein-cholesterol; RBC: red blood cell; SBP: systolic blood pressure; WBC: white blood cell. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 2 shows the comparisons between platelet-associated parameters and increased arterial stiffness in total participants by univariate analysis. The results showed that platelet count was significantly higher in subjects with increased arterial stiffness than in those without (platelet count: 254.3 ± 53.8 × 103/μL vs. 262.8 ± 52.4 × 103/μL, P = 0.007). Additionally, Table 2 demonstrated that higher platelet count quartiles exhibited significantly higher prevalence of arterial stiffness than lower platelet count quartiles. Contrarily, there was no statistical difference in MPV levels among subjects with or without arterial stiffness. When examined individually by gender, the platelet counts were significantly higher in those with increased arterial stiffness in both males and females, whereas there was no significant difference of MPV values in those with and without increased arterial stiffness (shown in Supplementary Figures 1 and 2). While performing the linear regression analysis (shown in Table 3), we initially investigated the association of baPWV value with platelet count and MPV separately. The results showed that platelet count was positively associated with baPWV values (β = 1.82, 95% confidence interval (CI): 0.51 to 3.13, P = 0.007), whereas there was an inverse relationship between MPV and baPWV values (β = −11.85, 95% CI: −20.36 to −3.34, P = 0.006). The relationship between increased arterial stiffness, platelet count, and MPV level was further examined using a multiple linear regression model. The results showed that platelet count remained positively associated with baPWV after adjusting potential confounders (β = 1.88, 95% CI: 0.96 to 2.80, P = 0.007). However, the relationship between MPV and baPWV levels became insignificant after multivariable adjustment (β = −2.68, 95% CI: −8.39 to 3.03, P = 0.358). Age; male sex; BMI; blood pressure; blood glucose, TC, uric acid, and hs-CRP levels; and cigarette smoking were also independently and positively correlated with baPWV value. Simultaneously, exercise habit was negatively related to baPWV value.
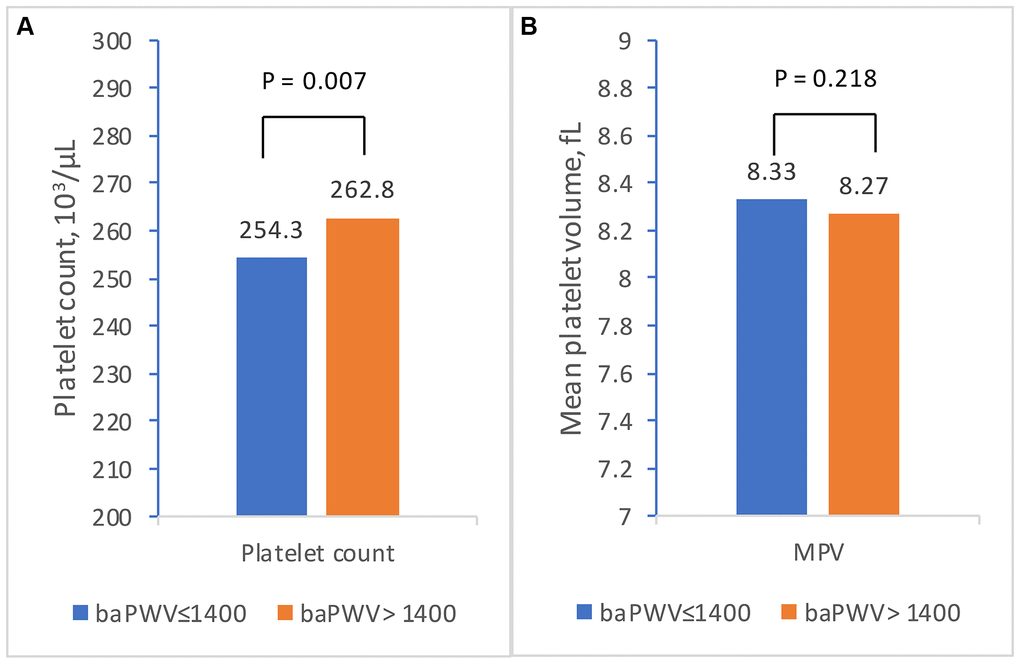
Figure 2. The relationship between platelet-associated parameters and increased arterial stiffness (baPWV >1,400 cm/s) by independent t-test. (A) Comparisons of platelet count between subjects with and without increased arterial stiffness. (B) Comparisons of mean platelet volume subjects with and without increased arterial stiffness. The orange and blue bars represent the mean levels in subjects with and without increased arterial stiffness, respectively. A P value < 0.05 was defined as statistically significant. Abbreviations: baPWV: brachial-ankle pulse wave velocity; MPV: mean platelet volume.
Table 2. Univariate analysis of the relationship between platelet-associated parameters and increased arterial stiffness (baPWV >1,400 cm/s).
| Variables | Increased arterial stiffness | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No (n = 2,125) | Yes (n = 339) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Platelet count, 103/μL | 254.3±53.8 | 262.8±52.4 | 0.007 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Platelet count, quartiles | 0.023 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (150~215, 103/μL) | 555 (26.1) | 64 (18.9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (216~248, 103/μL) | 518 (24.4) | 89 (26.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (249~289, 103/μL) | 533 (25.1) | 86 (25.4) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (290~450, 103/μL) | 519 (24.4) | 100 (29.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean platelet volume, fL | 8.33±0.83 | 8.27±0.80 | 0.218 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean platelet volume, quartiles | 0.499 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (6.2~7.7 fL) | 526 (24.8) | 97 (28.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (7.8~ 8.2 fL) | 528 (24.8) | 79 (23.3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (8.3~ 8.8 fL) | 536 (25.2) | 80 (23.6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (8.9~11.8 fL) | 535 (25.2) | 83 (24.5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data expressed as mean ± standard deviation or number (percent). Abbreviation: baPWV: brachial-ankle pulse wave velocity. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 3. Linear regression model for baPWV value (cm/s) with platelet count and mean platelet volume levels.
| Variables | Univariate | Multivariate | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| β (95% CI) | P value | β (95% CI) | P value | β (95% CI) | P value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Platelet count, 104/μL | 1.82 (0.51~3.13) | 0.007 | 1.88 (0.96~2.80) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean platelet volume, fL | −11.85(−20.36~−3.34) | 0.006 | −2.68(-8.39~−3.03) | 0.358 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 4.93 (4.17~5.70) | <0.001 | 4.86 (4.09~5.62) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex, male | 28.90 (12.25~−45.56) | 0.001 | 22.32 (5.87~−38.78) | 0.008 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2 | −9.11 (−10.71~−7.51) | <0.001 | −9.04 (−10.64~−7.44) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SBP, mmHg | 8.46 (8.05~8.87) | <0.001 | 8.53 (8.12~8.94) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FPG, mg/dL | 0.50 (0.21~0.80) | 0.001 | 0.50 (0.20~0.80) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cholesterol/HDL-C ratio | 9.11 (4.28~13.94) | <0.001 | 10.30 (5.50~15.11) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Uric acid, mg/dL | 6.44 (2.19~10.68) | 0.003 | 6.66 (2.40~10.91) | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Creatinine, mg/dL | −29.68 (−70.52~11.16) | 0.154 | −32.34 (−73.29~8.62) | 0.122 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| hs-CRP, mg/L | 2.01 (0.67~3.35) | 0.003 | 2.13 (0.79~3.47) | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking, yes vs. no | 14.55 (0.22~28.88) | 0.047 | 14.68 (0.30~29.05) | 0.045 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exercise, yes vs. no | −9.10 (−18.08~0.61) | 0.066 | −10.10 (−19.38~−0.38) | 0.042 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: baPWV: brachial-ankle pulse wave velocity; BMI: body mass index; CI: confidence interval; FPG: fasting plasma glucose; HDL-C: high-density lipoprotein-cholesterol; hs-CRP: high sensitivity C-reactive protein; SBP: systolic blood pressure. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The risk of increased arterial stiffness among subjects with different levels of platelet count and MPV level was further analyzed using the binary logistic regression model (Table 4). The results revealed that, compared with subjects in the lowest quartile (Q1), those in high quartiles (Q2–Q4) were all found to have a higher risk of increased arterial stiffness (Q2 vs. Q1: odds ratio (OR):1.54, 95% CI: 1.05 to 2.27, P = 0.029; Q3 vs. Q1: OR: 1.57, 95% CI: 1.06 to 2.33, P = 0.026; Q4 vs. Q1: OR: 2.23, 95% CI: 1.50 to 3.30, P < 0.001) after adjusting for age, sex, obesity, diabetes, hypertension, dyslipidemia, hyperuricemia, hs-CRP level, cigarette smoking, and regular exercise. In addition, the positive relationship between platelet and increased arterial stiffness remained significant when the logistic regression model was conducted by gender (shown in Supplementary Tables 2 and 3). Contrarily, there was no statistically significant difference in the risk of increased arterial stiffness among patients across different MPV quartiles in total (shown in Table 4), male (shown in Supplementary Table 2) and female participants (shown in Supplementary Table 3).
Table 4. Logistic regression model for increased arterial stiffness (baPWV >1,400 cm/s) with platelet count and mean platelet volume levels.
| Variables | Crude OR (95% CI) | P value | Adjusted ORa (95% CI) | P value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Platelet count, quartiles | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (150~215, 103/μL) | Reference | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (216~248, 103/μL) | 1.49 (1.06–2.10) | 0.023 | 1.54 (1.05–2.27) | 0.029 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (249~289, 103/μL) | 1.38 (0.98–1.95) | 0.067 | 1.57 (1.06–2.33) | 0.026 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (290~450, 103/μL) | 1.61 (1.15–2.26) | 0.006 | 2.23 (1.50–3.30) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean platelet volume, quartiles | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q1 (6.2~7.7 fL) | Reference | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q2 (7.8~8.2 fL) | 0.84 (0.61–1.16) | 0.296 | 0.96 (0.67–1.38) | 0.827 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q3 (8.3~8.8 fL) | 0.83 (0.60–1.14) | 0.251 | 0.99 (0.69–1.42) | 0.940 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Q4 (8.9~11.8 fL) | 0.87 (0.64–1.20) | 0.404 | 0.86 (0.60–1.24) | 0.860 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: baPWV: brachial-ankle pulse wave velocity; CI: confidence interval; OR: odds ratio. aadjusted for age, sex, obesity, hypertension, diabetes, hyperuricemia, total cholesterol/high-density lipoprotein-cholesterol ratio, high sensitivity C-reactive protein, cigarette smoking and regular exercise. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
Principal findings
This is the first study focusing on the association of platelet count and arterial stiffness in young and middle-aged populations with total adjustment of traditional risk factors of arterial stiffness, such as age; obesity; smoking; blood pressure; or FPG, uric acid, hs-CRP, or lipid profile levels. According to our research, young and middle-aged adults are significantly associated with a high risk of increased arterial stiffness when their platelet counts are elevated, even within the normal range.
Platelet-associated indices and arterial stiffness in previous studies
Platelet count and arterial stiffness
According to previous studies, platelet disorders with abnormally high and low platelet count, such as essential thrombocythemia and idiopathic thrombocytopenia purpura, were related to the risk of increased arterial stiffness [14, 30–32]. Although platelet activity is associated with CV diseases [16, 33] and the process of atherogenesis [34], studies focusing on platelet-associated parameters such as platelet count and MPV with arterial stiffness in general population remain extremely limited [20–22]. Only two studies discussed the correlation between arterial stiffness and platelet count [20, 22]. One study from Liu et al. found that increased platelet count was positively related to baPWV value in subjects with diabetes but not those without [22] and the other study from Marina et al. showed insignificant relationship between platelet count and arterial stiffness [20]. However, the population was relatively old in both studies from Liu et al. (mean age: 66.8 years for those without diabetes) and Mariana et al. (mean age: 55.3 years and 54.7 years in males and females). Because elevated platelet counts were correlated with increased mortality [35, 36], evaluation of platelet count and arterial stiffness in elderly adults may be potentially interfered with survivorship bias. Besides, the platelet count is relatively stable in young adulthood and midlife, and then starts to decline in people’s fifties and sixties [23, 37, 38]. Considering that platelet count is attenuated in the elderly [23, 37, 38], our study had the advantage of minimizing the confounding effect of age in the relationship between platelet count and arterial stiffness by taking aim at the young and middle-aged population. Additionally, although studies showed gender difference between both arterial stiffness [39] and platelet count [40], these significant disparities were not considered in the two aforementioned studies [20, 22]. Furthermore, the arterial stiffness was evaluated using the augmentation index [20] in study from Marina et al., which have several limitations in the assessment of wave reflection [41].
MPV and arterial stiffness
Two cross-sectional studies from Wang et al. and Marina et al. showed a positive relationship between MPV and increased arterial stiffness [20, 21] which was different from the findings of this study. However, despite that hematologic malignancy and abnormal platelet count (including thrombocytopenia and thrombocytosis) were found to affect the pathogenesis of arterial stiffness [30, 42, 43], subjects with hematologic disorders or abnormal platelet counts were not excluded from those two studies [20, 21]. Besides, several factors such as hyperuricemia and exercise habit might play a role in the pathogenesis of arterial stiffness, but these parameters were not adjusted in the regression model. In addition, the population in the study from Wang et al. had relatively high prevalence of cigarette smoking (approximately 37.5%); however, the habit of cigarette smoking was excluded in the final regression analysis. Considering that cigarette smoking leads to increased arterial stiffness [44] and also significantly elevates the MPV value [24], excluding cigarette smoking in the regression analysis may confound the final results [44]. Consequently, the disparity between our results and those of earlier studies [20–22] may be due to several unadjusted confounding factors and different population characteristics that were fully explored in the current study.
Possible mechanism of platelet counts and increased arterial stiffness
It is well recognized that extracellular matrix, inflammatory molecules, endothelial cell dysfunction, and oxidative stress interact to cause increased arterial stiffness [5, 45]. A previous study had found that platelets release several matrix metalloproteinases (MMP), such as MMP-1, MMP-2, MMP-3, MMP-9, and MMP-14 [46]. An in vitro study also revealed a positive association between platelet count and MMP level [47]. Considering that MMP-2, MMP-3, and MMP-9 are directly involved in the pathogenesis of arterial stiffness by degradation of elastic fiber with resultant reduced arterial elasticity [48–50], it is reasonable to hypothesize that subjects with high platelet count, potentially with higher MMP levels, may have increased risk of arterial stiffness. In addition, platelets contain granules that may cause elevation of chemokines or inflammatory cytokines such as transforming growth factor-beta [51] and interleukin-1 [52], which were all found to be associated with arterial stiffness [53, 54]. Furthermore, studies have demonstrated that platelet count was positively related to the production of transforming growth factor-beta and interleukin-1 [55–58], which might also result in the progression of arterial stiffness.
Another possible explanation for platelet count and arterial stiffness may be its role in the CD40–CD40 ligand interaction. CD40 and CD40 ligands are well known for involving vascular and systemic inflammation and the pathogenesis of CV diseases [59, 60]. The CD40 ligands were expressed by nonhematopoietic and hematopoietic cells, and the soluble form of CD40 ligands in the circulation was mainly generated from platelets [61]. In a previous study, platelet counts correlated highly with a soluble form of CD40 ligand concentrations [62]. Because platelets also expressed CD40, an elevated platelet count may represent a high activity of CD40–CD40 ligand signaling and thus contribute to vascular inflammation, leading to increased arterial stiffness.
Limitations
Although our study had the advantage of a relatively large sample size with comprehensive personal and medical information, including past history, lifestyle habits, and laboratory results, some limitations should be addressed. First, because of the cross-sectional design, it is difficult to establish a causal relationship between platelet-associated parameters and arterial stiffness. Second, because our analysis was confined to a Taiwanese population, whether it is plausible to extrapolate these results to other ethnic groups may need further investigation. Third, our participants were recruited from the health examination center of a tertiary medical center with potential selection bias. Fourth, although MMPs, transforming growth factor-beta, and interleukin-1 were associated with platelet count and arterial stiffness, these data were unavailable in the current study. Further investigation with more thorough information about such crucial biomarkers might be necessary for verifying the relationship and possible pathogenesis between platelet count and arterial stiffness.
In conclusion, the platelet counts in young age and midlife, even within normal range were positively associated with baPWV levels without gender difference. Additionally, participants in high platelet count quartiles (Q2–Q4) were related to an increased risk of arterial stiffness. In contrast, the relationship between MPV levels and arterial stiffness was insignificant. Our data suggest that platelet count is a useful marker of arterial stiffness in young and middle-aged adults. A high-normal platelet count should prompt further evaluation of potential atherosclerosis. The clinical application of this widely available marker in risk stratification warrants further investigation.
Author Contributions
Professor Ting-Hsing Chao had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Yu-Tsung Chou, Ting-Hsing Chao; Acquisition, analysis, or interpretation of data: All authors; Drafting of the manuscript: Yu-Tsung Chou, Ting-Hsing Chao; Critical revision of the manuscript for important intellectual content: All authors; Statistical analysis: Hung-Yu Chen, I-Hsuan Wu, Fei-Lin Su, Wen-Huang Li; Obtained funding: Yu-Tsung Chou; Administrative, technical, or material support: Hung-Lung Hsu, Jui-Ting Tai; Supervision: Hung-Yu Chen, I-Hsuan Wu, Fei-Lin Su, Wen-Huang Li, Hung-Lung Hsu, Jui-Ting Tai. All authors read and approved the final manuscript.
Acknowledgments
We are grateful to the investigators and staff of the Health Management Center of National Cheng Kung University Hospital for excellent research assistance. The authors also thank Enago (https://www.enago.tw/) for assistance with editing the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
The participants of this study were recruited from those who underwent health checkups at the National Cheng Kung University Hospital (NCKUH) health management center from November 2018 to December 2019. Informed consent was waived because the analysis was based on anonymous data.
Funding
This research was funded by the National Cheng Kung University Hospital (Grant number: NCKUH-11103034) and by Ministry of Science and Technology (MOST 109-2314-B-006-069-MY3; MOST 110-2634-F-038-006 and MOST 111-2314-B-006-019-MY3).
References
- 1. Cecelja M, Chowienczyk P. Role of arterial stiffness in cardiovascular disease. JRSM Cardiovasc Dis. 2012; 1:1–10. https://doi.org/10.1258/cvd.2012.012016 [PubMed]
- 2. Shen WC, Lu FH, Yang YC, Wu JS, Chang YF, Huang YH, Chang CJ. The relationship between high-density lipoprotein cholesterol levels and arterial stiffness in a Taiwanese population. Nutr Metab Cardiovasc Dis. 2017; 27:1136–42. https://doi.org/10.1016/j.numecd.2017.10.003 [PubMed]
- 3. Lee HY, Oh BH. Aging and arterial stiffness. Circ J. 2010; 74:2257–62. https://doi.org/10.1253/circj.cj-10-0910 [PubMed]
- 4. Mattace-Raso FU, van der Cammen TJ, Hofman A, van Popele NM, Bos ML, Schalekamp MA, Asmar R, Reneman RS, Hoeks AP, Breteler MM, Witteman JC. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation. 2006; 113:657–63. https://doi.org/10.1161/CIRCULATIONAHA.105.555235 [PubMed]
- 5. Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol. 2005; 25:932–43. https://doi.org/10.1161/01.ATV.0000160548.78317.29 [PubMed]
- 6. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010; 55:1318–27. https://doi.org/10.1016/j.jacc.2009.10.061 [PubMed]
- 7. Yamashina A, Tomiyama H, Takeda K, Tsuda H, Arai T, Hirose K, Koji Y, Hori S, Yamamoto Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens Res. 2002; 25:359–64. https://doi.org/10.1291/hypres.25.359 [PubMed]
- 8. Tanaka H, Munakata M, Kawano Y, Ohishi M, Shoji T, Sugawara J, Tomiyama H, Yamashina A, Yasuda H, Sawayama T, Ozawa T. Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness. J Hypertens. 2009; 27:2022–7. https://doi.org/10.1097/HJH.0b013e32832e94e7 [PubMed]
- 9. Yu WC, Chuang SY, Lin YP, Chen CH. Brachial-ankle vs carotid-femoral pulse wave velocity as a determinant of cardiovascular structure and function. J Hum Hypertens. 2008; 22:24–31. https://doi.org/10.1038/sj.jhh.1002259 [PubMed]
- 10. Li SW, Yao T, Zhang L, Zhao L, Zhang XL, Wei XX, Peng DX, Wu SL, Sun LX. Relationship Between Brachial–Ankle Pulse Wave Velocity and Risk of New-Onset Acute Myocardial Infarction. Am J Hypertens. 2022; 35:111–2. https://doi.org/10.1093/ajh/hpab119
- 11. Kwak S, Kim HL, In M, Lim WH, Seo JB, Kim SH, Zo JH, Kim MA. Associations of Brachial-Ankle Pulse Wave Velocity With Left Ventricular Geometry and Diastolic Function in Untreated Hypertensive Patients. Front Cardiovasc Med. 2021; 8:647491. https://doi.org/10.3389/fcvm.2021.647491 [PubMed]
- 12. Turin TC, Kita Y, Rumana N, Takashima N, Kadota A, Matsui K, Sugihara H, Morita Y, Nakamura Y, Miura K, Ueshima H. Brachial-ankle pulse wave velocity predicts all-cause mortality in the general population: findings from the Takashima study, Japan. Hypertens Res. 2010; 33:922–5. https://doi.org/10.1038/hr.2010.103 [PubMed]
- 13. Holinstat M. Normal platelet function. Cancer Metastasis Rev. 2017; 36:195–8. https://doi.org/10.1007/s10555-017-9677-x [PubMed]
- 14. Rossi C, Randi ML, Zerbinati P, Rinaldi V, Girolami A. Acute coronary disease in essential thrombocythemia and polycythemia vera. J Intern Med. 1998; 244:49–53. https://doi.org/10.1046/j.1365-2796.1998.00314.x [PubMed]
- 15. Park Y, Schoene N, Harris W. Mean platelet volume as an indicator of platelet activation: methodological issues. Platelets. 2002; 13:301–6. https://doi.org/10.1080/095371002220148332 [PubMed]
- 16. Uysal HB, Dağlı B, Akgüllü C, Avcil M, Zencir C, Ayhan M, Sönmez HM. Blood count parameters can predict the severity of coronary artery disease. Korean J Intern Med. 2016; 31:1093–100. https://doi.org/10.3904/kjim.2015.199 [PubMed]
- 17. Varol E, Akcay S, Icli A, Yucel H, Ozkan E, Erdogan D, Ozaydin M. Mean platelet volume in patients with prehypertension and hypertension. Clin Hemorheol Microcirc. 2010; 45:67–72. https://doi.org/10.3233/CH-2010-1327 [PubMed]
- 18. Bath P, Algert C, Chapman N, Neal B, and PROGRESS Collaborative Group. Association of mean platelet volume with risk of stroke among 3134 individuals with history of cerebrovascular disease. Stroke. 2004; 35:622–6. https://doi.org/10.1161/01.STR.0000116105.26237.EC [PubMed]
- 19. Kandis H, Ozhan H, Ordu S, Erden I, Caglar O, Basar C, Yalcin S, Alemdar R, Aydin M. The prognostic value of mean platelet volume in decompensated heart failure. Emerg Med J. 2011; 28:575–8. https://doi.org/10.1136/emj.2009.088401 [PubMed]
- 20. Panova-Noeva M, Arnold N, Hermanns MI, Prochaska JH, Schulz A, Spronk HM, Binder H, Pfeiffer N, Beutel M, Blankenberg S, Zeller T, Lotz J, Münzel T, et al. Mean Platelet Volume and Arterial Stiffness - Clinical Relationship and Common Genetic Variability. Sci Rep. 2017; 7:40229. https://doi.org/10.1038/srep40229 [PubMed]
- 21. Wang RT, Li Y, Zhu XY, Zhang YN. Increased mean platelet volume is associated with arterial stiffness. Platelets. 2011; 22:447–51. https://doi.org/10.3109/09537104.2011.565431 [PubMed]
- 22. Liu K, Xu J, Tao L, Yang K, Sun Y, Guo X. Platelet counts are associated with arterial stiffness in Chinese Han population: a longitudinal study. BMC Cardiovasc Disord. 2020; 20:353. https://doi.org/10.1186/s12872-020-01634-7 [PubMed]
- 23. Balduini CL, Noris P. Platelet count and aging. Haematologica. 2014; 99:953–5. https://doi.org/10.3324/haematol.2014.106260 [PubMed]
- 24. Varol E, Icli A, Kocyigit S, Erdogan D, Ozaydin M, Dogan A. Effect of smoking cessation on mean platelet volume. Clin Appl Thromb Hemost. 2013; 19:315–9. https://doi.org/10.1177/1076029612436675 [PubMed]
- 25. Chou YT, Cheng HJ, Wu JS, Yang YC, Chou CY, Chang CJ, Lu FH. The association of sleep duration and sleep quality with non-alcoholic fatty liver disease in a Taiwanese population. Obes Res Clin Pract. 2018; 12:500–5. https://doi.org/10.1016/j.orcp.2018.05.002 [PubMed]
- 26. Chu NF. Prevalence of obesity in Taiwan. Obes Rev. 2005; 6:271–4. https://doi.org/10.1111/j.1467-789X.2005.00175.x [PubMed]
- 27. National High Blood Pressure Education Program. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Bethesda (MD): National Heart, Lung, and Blood Institute (US). 2004. [PubMed]
- 28. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014 (Suppl 1); 37:S81–90. https://doi.org/10.2337/dc14-S081 [PubMed]
- 29. Yen PC, Chou YT, Li CH, Sun ZJ, Wu CH, Chang YF, Lu FH, Yang YC, Chang CJ, Wu JS. Hyperuricemia Is Associated with Significant Liver Fibrosis in Subjects with Nonalcoholic Fatty Liver Disease, but Not in Subjects without It. J Clin Med. 2022; 11:1445. https://doi.org/10.3390/jcm11051445 [PubMed]
- 30. Anžič Drofenik A, Vrtovec M, Božič Mijovski M, Sever M, Preložnik Zupan I, Kejžar N, Blinc A. Progression of coronary calcium burden and carotid stiffness in patients with essential thrombocythemia associated with JAK2 V617F mutation. Atherosclerosis. 2020; 296:25–31. https://doi.org/10.1016/j.atherosclerosis.2020.01.001 [PubMed]
- 31. Chandan JS, Thomas T, Lee S, Marshall T, Willis B, Nirantharakumar K, Gill P. The association between idiopathic thrombocytopenic purpura and cardiovascular disease: a retrospective cohort study. J Thromb Haemost. 2018; 16:474–80. https://doi.org/10.1111/jth.13940 [PubMed]
- 32. Russo A, Cannizzo M, Ghetti G, Barbaresi E, Filippini E, Specchia S, Branzi A. Idiopathic thrombocytopenic purpura and coronary artery disease: comparison between coronary artery bypass grafting and percutaneous coronary intervention. Interact Cardiovasc Thorac Surg. 2011; 13:153–7. https://doi.org/10.1510/icvts.2011.271296 [PubMed]
- 33. Würtz M, Hvas AM, Kristensen SD, Grove EL. Platelet aggregation is dependent on platelet count in patients with coronary artery disease. Thromb Res. 2012; 129:56–61. https://doi.org/10.1016/j.thromres.2011.08.019 [PubMed]
- 34. Schulz C, Massberg S. Platelets in atherosclerosis and thrombosis. Handb Exp Pharmacol. 2012; 111–33. https://doi.org/10.1007/978-3-642-29423-5_5 [PubMed]
- 35. Fawzy A, Anderson JA, Cowans NJ, Crim C, Wise R, Yates JC, Hansel NN. Association of platelet count with all-cause mortality and risk of cardiovascular and respiratory morbidity in stable COPD. Respir Res. 2019; 20:86. https://doi.org/10.1186/s12931-019-1059-1 [PubMed]
- 36. van der Bom JG, Heckbert SR, Lumley T, Holmes CE, Cushman M, Folsom AR, Rosendaal FR, Psaty BM. Platelet count and the risk for thrombosis and death in the elderly. J Thromb Haemost. 2009; 7:399–405. https://doi.org/10.1111/j.1538-7836.2008.03267.x [PubMed]
- 37. Segal JB, Moliterno AR. Platelet counts differ by sex, ethnicity, and age in the United States. Ann Epidemiol. 2006; 16:123–30. https://doi.org/10.1016/j.annepidem.2005.06.052 [PubMed]
- 38. Biino G, Santimone I, Minelli C, Sorice R, Frongia B, Traglia M, Ulivi S, Di Castelnuovo A, Gögele M, Nutile T, Francavilla M, Sala C, Pirastu N, et al. Age- and sex-related variations in platelet count in Italy: a proposal of reference ranges based on 40987 subjects' data. PLoS One. 2013; 8:e54289. https://doi.org/10.1371/journal.pone.0054289 [PubMed]
- 39. Kim JY, Park JB, Kim DS, Kim KS, Jeong JW, Park JC, Oh BH, Chung N, and KAAS investigators. Gender Difference in Arterial Stiffness in a Multicenter Cross-Sectional Study: The Korean Arterial Aging Study (KAAS). Pulse (Basel). 2014; 2:11–7. https://doi.org/10.1159/000365267 [PubMed]
- 40. Butkiewicz AM, Kemona H, Dymicka-Piekarska V, Matowicka-Karna J, Radziwon P, Lipska A. Platelet count, mean platelet volume and thrombocytopoietic indices in healthy women and men. Thromb Res. 2006; 118:199–204. https://doi.org/10.1016/j.thromres.2005.06.021 [PubMed]
- 41. Hughes AD, Park C, Davies J, Francis D, McG Thom SA, Mayet J, Parker KH. Limitations of augmentation index in the assessment of wave reflection in normotensive healthy individuals. PLoS One. 2013; 8:e59371. https://doi.org/10.1371/journal.pone.0059371 [PubMed]
- 42. Mozos I, Borzak G, Caraba A, Mihaescu R. Arterial stiffness in hematologic malignancies. Onco Targets Ther. 2017; 10:1381–8. https://doi.org/10.2147/OTT.S126852 [PubMed]
- 43. Kim MJ, Park PW, Seo YH, Kim KH, Seo JY, Jeong JH, Park MJ, Ahn JY. Comparison of platelet parameters in thrombocytopenic patients associated with acute myeloid leukemia and primary immune thrombocytopenia. Blood Coagul Fibrinolysis. 2014; 25:221–5. https://doi.org/10.1097/MBC.0000000000000027 [PubMed]
- 44. Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. 2010; 16:2518–25. https://doi.org/10.2174/138161210792062920 [PubMed]
- 45. Lacolley P, Regnault V, Laurent S. Mechanisms of Arterial Stiffening: From Mechanotransduction to Epigenetics. Arterioscler Thromb Vasc Biol. 2020; 40:1055–62. https://doi.org/10.1161/ATVBAHA.119.313129 [PubMed]
- 46. Gresele P, Falcinelli E, Sebastiano M, Momi S. Matrix Metalloproteinases and Platelet Function. Prog Mol Biol Transl Sci. 2017; 147:133–65. https://doi.org/10.1016/bs.pmbts.2017.01.002 [PubMed]
- 47. Falcinelli E, Giannini S, Boschetti E, Gresele P. Platelets release active matrix metalloproteinase-2 in vivo in humans at a site of vascular injury: lack of inhibition by aspirin. Br J Haematol. 2007; 138:221–30. https://doi.org/10.1111/j.1365-2141.2007.06632.x [PubMed]
- 48. Iannarelli NJ, MacNeil AJ, Dempster KS, Wade TJ, O'Leary DD. Serum MMP-3 and its association with central arterial stiffness among young adults is moderated by smoking and BMI. Physiol Rep. 2021; 9:e14920. https://doi.org/10.14814/phy2.14920 [PubMed]
- 49. Yasmin, McEniery CM, Wallace S, Dakham Z, Pulsalkar P, Maki-Petaja K, Ashby MJ, Cockcroft JR, Wilkinson IB. Matrix metalloproteinase-9 (MMP-9), MMP-2, and serum elastase activity are associated with systolic hypertension and arterial stiffness. Arterioscler Thromb Vasc Biol. 2005; 25:372–8. https://doi.org/10.1161/01.ATV.0000151373.33830.41 [PubMed]
- 50. Galis ZS, Khatri JJ. Matrix metalloproteinases in vascular remodeling and atherogenesis: the good, the bad, and the ugly. Circ Res. 2002; 90:251–62. [PubMed]
- 51. Blakytny R, Ludlow A, Martin GE, Ireland G, Lund LR, Ferguson MW, Brunner G. Latent TGF-beta1 activation by platelets. J Cell Physiol. 2004; 199:67–76. https://doi.org/10.1002/jcp.10454 [PubMed]
- 52. Loppnow H, Bil R, Hirt S, Schönbeck U, Herzberg M, Werdan K, Rietschel ET, Brandt E, Flad HD. Platelet-derived interleukin-1 induces cytokine production, but not proliferation of human vascular smooth muscle cells. Blood. 1998; 91:134–41. [PubMed]
- 53. Mozos I, Malainer C, Horbańczuk J, Gug C, Stoian D, Luca CT, Atanasov AG. Inflammatory Markers for Arterial Stiffness in Cardiovascular Diseases. Front Immunol. 2017; 8:1058. https://doi.org/10.3389/fimmu.2017.01058 [PubMed]
- 54. Park S, Lakatta EG. Role of inflammation in the pathogenesis of arterial stiffness. Yonsei Med J. 2012; 53:258–61. https://doi.org/10.3349/ymj.2012.53.2.258 [PubMed]
- 55. Tunjungputri RN, Li Y, de Groot PG, Dinarello CA, Smeekens SP, Jaeger M, Doppenberg-Oosting M, Cruijsen M, Lemmers H, Toenhake-Dijkstra H, Aguirre-Gamboa R, Kumar V, Wijmenga C, et al. The Inter-Relationship of Platelets with Interleukin-1β-Mediated Inflammation in Humans. Thromb Haemost. 2018; 118:2112–25. https://doi.org/10.1055/s-0038-1675603 [PubMed]
- 56. Guo Y, Cui W, Pei Y, Xu D. Platelets promote invasion and induce epithelial to mesenchymal transition in ovarian cancer cells by TGF-β signaling pathway. Gynecol Oncol. 2019; 153:639–50. https://doi.org/10.1016/j.ygyno.2019.02.026 [PubMed]
- 57. Karolczak K, Watala C. Blood Platelets as an Important but Underrated Circulating Source of TGFβ. Int J Mol Sci. 2021; 22:4492. https://doi.org/10.3390/ijms22094492 [PubMed]
- 58. Weibrich G, Kleis WK, Hafner G, Hitzler WE. Growth factor levels in platelet-rich plasma and correlations with donor age, sex, and platelet count. J Craniomaxillofac Surg. 2002; 30:97–102. https://doi.org/10.1054/jcms.2002.0285 [PubMed]
- 59. Steven S, Dib M, Hausding M, Kashani F, Oelze M, Kröller-Schön S, Hanf A, Daub S, Roohani S, Gramlich Y, Lutgens E, Schulz E, Becker C, et al. CD40L controls obesity-associated vascular inflammation, oxidative stress, and endothelial dysfunction in high fat diet-treated and db/db mice. Cardiovasc Res. 2018; 114:312–23. https://doi.org/10.1093/cvr/cvx197 [PubMed]
- 60. Chakrabarti S, Blair P, Freedman JE. CD40-40L signaling in vascular inflammation. J Biol Chem. 2007; 282:18307–17. https://doi.org/10.1074/jbc.M700211200 [PubMed]
- 61. André P, Nannizzi-Alaimo L, Prasad SK, Phillips DR. Platelet-derived CD40L: the switch-hitting player of cardiovascular disease. Circulation. 2002; 106:896–9. https://doi.org/10.1161/01.cir.0000028962.04520.01 [PubMed]
- 62. Viallard JF, Solanilla A, Gauthier B, Contin C, Déchanet J, Grosset C, Moreau JF, Praloran V, Nurden P, Pellegrin JL, Nurden AT, Ripoche J. Increased soluble and platelet-associated CD40 ligand in essential thrombocythemia and reactive thrombocytosis. Blood. 2002; 99:2612–4. https://doi.org/10.1182/blood.v99.7.2612 [PubMed]