



Introduction
Werner syndrome is an autosomal recessive adult-onset progeroid disorder that affects approximately 700-2,000 individuals in Japan [1–4]. Patients with Werner syndrome present with various aging phenotypes from a young age. Graying and/or loss of hair presents in their third decade of life; bilateral cataracts and diabetes, around their fourth decade of life; and atherosclerotic diseases and malignant neoplasms, around their fifth decade of life [5]. These patients also develop a high proportion of skin ulcers, often requiring amputation of the lower extremities. Although it was previously reported that patients with Werner syndrome die at 46 years of age on average [6], recent evidence indicates the average age of death is 59 years [7]. In Werner syndrome, quality of life (QOL) and activities of daily living (ADL) decline due to the various symptoms [8].
Since it is a rare disease, there is often a long period between the disease onset and the diagnosis [9]. Therefore, early detection and therapeutic intervention are important. Recently, the number of long-term survivors has increased due to therapeutic advances; however, new complications have also been observed. Although detailed and long-term involvement in medical care is essential for maintaining QOL and ADL, few reports have followed the changes over time in patients with Werner syndrome.
The Werner Syndrome Registry was established in 2017 to investigate the disease, recruit participants for clinical trials, and provide information to patients and physicians. In this report, the updated cross-sectional and longitudinal analyses of the Werner Syndrome Registry database were performed to reveal the current status and natural course in patients with Werner syndrome.
Results
Werner Syndrome Registry cross-sectional analysis
Twelve facilities and fifty-one diagnosed patients were enrolled in the registry. Table 1 shows the patients’ characteristics; the percentage of baseline major signs, clinical symptoms, and comorbidities in patients with Werner syndrome; the drugs administered for diabetes, dyslipidemia, and hypertension; and the blood examination results at the point of enrollment to the registry. The patients’ mean registered age was 49.0 ± 7.2 years. Although the mean age of onset, inferred from the interviews or medical histories, was 25.8 ± 9.2 years, the mean age at diagnosis was 41.8 ± 8.2 years. Patients with Werner syndrome were lower in height, weight, and body mass index (BMI) than the average Japanese adults [10, 11]. Despite having a low BMI, the mean waist circumference was 77.2 ± 11.1 cm, and the mean visceral fat area measured by computed tomography was 97.5 ± 57.5 cm2. The mean skeletal muscle index (SMI) on dual-energy X-ray absorptiometry was 5.36 ± 1.61 kg/m2 for men and 3.99 ± 0.98 kg/m2 for women, the grip strength (in the right hand) was 22.8 ± 8.6 kg for men and 12.9 ± 5.5 kg for women, and the average gait speed was 0.96 ± 0.56 m/sec. The grip strength and SMI met the diagnostic criteria for sarcopenia. Approximately 30% of patients’ parents had consanguineous marriages.
Table 1. Patients’ characteristics at baseline.
| Na | % (n patients with this characteristic) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Major signs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Graying and/or loss of hair | 51 | 98.0 (50) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral cataracts | 51 | 100 (51) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin changes | 51 | 98.0 (50) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intractable skin ulcers | 51 | 66.7 (34) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Soft tissue calcification | 49 | 93.9 (46) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bird-like face | 51 | 92.2 (47) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High-pitched voice | 51 | 82.4 (42) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes, IGT | 51 | 68.6 (35) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 51 | 66.7 (34) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 48 | 39.6 (19) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fatty liver | 49 | 59.2 (29) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebral bleeding | 51 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebral infarction | 51 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AP or MI | 51 | 2.0 (1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAD | 51 | 11.8 (6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Malignant neoplasm | 51 | 25.5 (13) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Amputation | 51 | 11.8 (6) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (1) For diabetes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DPP-4 inhibitor | 35 | 34.3 (12) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Biguanide | 35 | 34.3 (12) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazolidine | 35 | 42.9 (15) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alpha GI | 35 | 5.7 (2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sulfonylurea | 35 | 8.6 (3) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Glinide | 35 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SGLT2 inhibitor | 35 | 2.9 (1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GLP-1 analog | 35 | 5.7 (2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Insulin | 35 | 14.3 (5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (2) For dyslipidemia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 34 | 58.8 (20) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrate | 34 | 2.9 (1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ezetimibe | 34 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPA | 34 | 14.7 (5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ion exchange resin | 34 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nicotinic acids | 34 | 14.7 (5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (3) For hypertension, among others | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ca blocker | 19 | 47.4 (9) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ARB | 19 | 36.8 (7) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ACE inhibitor | 19 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alpha1 blocker | 19 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta blocker | 19 | 10.5 (2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diuretics | 19 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Eplerenone | 19 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nitrate | 48 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 48 | 4.2 (2) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 47 | 10.6 (5) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Warfarin | 48 | 0 (0) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anticoagulant | 47 | 2.1 (1) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total | Male | Female | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Patients’ backgrounds | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Registered age (years) | 51 | 49.0 ± 7.2 | 27 | 48.3 ± 7.1 | 24 | 49.7 ± 7.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Onset age (years) | 41 | 25.8 ± 9.2 | 21 | 28.0 ± 8.1 | 20 | 23.4 ± 9.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diagnosed age (years) | 50 | 41.8 ± 8.2 | 26 | 41.8 ± 6.0 | 24 | 41.8 ± 10.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Consanguineous marriage (%) | 14/48 | 29.2 | 7/24 | 29.2 | 7/24 | 29.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical findings/function | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Height (cm) | 51 | 154.2 ± 10.5 | 27 | 160.1 ± 8.2 | 24 | 147.6 ± 8.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Average 40s Japanese height (cm) | 171.5 ± 5.8 | 158.1 ± 5.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body weight (kg) | 51 | 43.7 ± 9.6 | 27 | 49.6 ± 8.6 | 24 | 37.1 ± 5.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Average 40s Japanese body weight (kg) | 72.8 ± 12.8 | 55.6 ± 10.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 51 | 18.3 ± 3.1 | 27 | 19.4 ± 3.2 | 24 | 17.1 ± 2.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Average 40s Japanese BMI (kg/m2) | 24.7 ± 4.0 | 22.3 ± 4.0 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg) | 45 | 123 ± 19 | 23 | 128 ± 19 | 22 | 118 ± 18 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg) | 45 | 69 ± 13 | 23 | 73 ± 11 | 22 | 65 ± 13 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse (/min) | 43 | 87 ± 14 | 22 | 88 ± 14 | 21 | 85 ± 13 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference (cm) | 30 | 77.2 ± 11.1 | 17 | 80.2 ± 11.3 | 13 | 73.2 ± 9.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Visceral fat area (cm2) | 14 | 97.5 ± 57.5 | 6 | 117.3 ± 63.6 | 8 | 82.7 ± 51.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skeletal muscle mass index (kg/m2) | 18 | 4.60 ± 1.44 | 8 | 5.36 ± 1.61 | 10 | 3.99 ± 0.98 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grip strength (right) (kg) | 32 | 18.1 ± 8.8 | 17 | 22.8 ± 8.6 | 15 | 12.9 ± 5.5 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Grip strength (left) (kg) | 32 | 16.6 ± 7.8 | 17 | 21.0 ± 7.4 | 15 | 11.5 ± 4.6 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Walking speed (m/sec) | 16 | 0.96 ± 0.56 | 8 | 1.03 ± 0.60 | 8 | 0.88 ± 0.55 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Blood examinations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC (/μL) | 50 | 7504 ± 2268 | 27 | 7486 ± 2605 | 23 | 7525 ± 1855 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBC (x104/μL) | 50 | 414 ± 85 | 27 | 429 ± 70 | 23 | 397 ± 99 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 50 | 12.6 ± 2.1 | 27 | 13.2 ± 2.1 | 23 | 12.0 ± 1.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plt (x104/μL) | 50 | 28.6 ± 9.1 | 27 | 26.0 ± 7.2 | 23 | 31.7 ± 10.2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST (U/L) | 51 | 31.6 ± 17.5 | 27 | 34.9 ± 19.6 | 24 | 27.8 ± 14.4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT (U/L) | 51 | 41.2 ± 32.9 | 27 | 48.6 ± 38.2 | 24 | 33.0 ± 23.9 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| γGTP (U/L) | 49 | 98.3 ± 103.6 | 27 | 95.1 ± 96.4 | 22 | 102.2 ± 114.1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDH (U/L) | 48 | 223 ± 161 | 27 | 234 ± 208 | 21 | 210 ± 65 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALP (U/L) | 45 | 272 ± 173 | 26 | 273 ± 149 | 19 | 271 ± 205 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ChE (U/L) | 35 | 368 ± 98 | 18 | 374 ± 114 | 17 | 361 ± 82 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T-Bil (mg/dL) | 44 | 0.55 ± 0.25 | 25 | 0.57 ± 0.26 | 19 | 0.52 ± 0.24 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP (g/dL) | 47 | 7.77 ± 0.57 | 26 | 7.78 ± 0.51 | 21 | 7.74 ± 0.65 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alb (g/dL) | 48 | 4.25 ± 0.72 | 25 | 4.32 ± 0.84 | 23 | 4.17 ± 0.59 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA (mg/dL) | 46 | 5.39 ± 1.32 | 25 | 5.59 ± 1.24 | 21 | 5.15 ± 1.40 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BUN (mg/dL) | 48 | 16.4 ± 7.4 | 27 | 16.4 ± 8.0 | 21 | 16.3 ± 6.7 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cre (mg/dL) | 50 | 0.77 ± 0.86 | 27 | 0.96 ± 1.13 | 23 | 0.54 ± 0.19 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcre (mL/min/1.73 m2) | 50 | 98.3 ± 36.3 | 27 | 92.3 ± 28.5 | 23 | 105.3 ± 43.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 50 | 77.8 ± 27.0 | 27 | 79.6 ± 24.8 | 23 | 75.5 ± 29.8 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcys (mL/min/1.73 m2) | 15 | 83.2 ± 29.5 | 10 | 86.1 ± 30.3 | 5 | 77.4 ± 30.3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Na (mEq/L) | 48 | 140 ± 3 | 26 | 139 ± 3 | 22 | 140 ± 3 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| K (mEq/L) | 48 | 4.27 ± 0.39 | 26 | 4.26 ± 0.43 | 22 | 4.27 ± 0.36 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cl (mEq/L) | 47 | 104 ± 3 | 25 | 104 ± 3 | 22 | 104 ± 4 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mg/dL) | 43 | 193 ± 32 | 25 | 196 ± 33 | 18 | 189 ± 31 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG (mg/dL) | 49 | 161 ± 96 | 26 | 178 ± 98 | 23 | 143 ± 92 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (direct) (mg/dL) | 39 | 119 ± 27 | 20 | 121 ± 28 | 19 | 117 ± 26 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C (mg/dL) | 46 | 57 ± 21 | 23 | 56 ± 20 | 23 | 59 ± 21 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c (%) | 46 | 6.42 ± 1.25 | 23 | 6.29 ± 0.98 | 23 | 6.55 ± 1.49 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FPG (mg/dL) | 21 | 118 ± 29 | 10 | 123 ± 36 | 11 | 112 ± 21 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PPG (mg/dL) | 24 | 142 ± 55 | 13 | 151 ± 47 | 11 | 132 ± 63 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aN denotes the number of patients who had data. Regarding medications for diabetes, dyslipidemia, and hypertension, N means the patients with diabetes, dyslipidemia, and hypertension. Abbreviations: IGT: Impaired glucose tolerance; AP: Angina pectoris; MI: Myocardial infarction; PAD: peripheral artery disease; DPP-4: Dipeptidyl peptidase-4; alpha GI: alpha glucosidase inhibitor; SGLT2: Sodium-glucose cotransporter-2; GLP-1: Glucagon-like peptide-1; EPA: Eicosapentaenoic acid; Ca: Calcium; ARB: Angiotensin- II receptor blocker; ACE: Angiotensin-converting enzyme inhibitor; BMI: body mass index; SMI: skeletal muscle mass index; WBC: white blood cell; RBC: red blood cell; Hgb: hemoglobin; Plt: platelet; AST: aspartate aminotransferase; ALT: alanine aminotransferase; γ-GTP: gamma-glutamyl transpeptidase; LDH: lactate dehydrogenase; ALP: alkaline phosphatase; ChE: cholinesterase; T-Bil: total bilirubin; TP: total protein; Alb: albumin; UA: uric acid; BUN: blood urea nitrogen; Cre: creatinine; BSA: body surface are; eGFR: estimated glomerular filtration rate; Na: natrium; K: potassium; Cl: chlorine; TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; HbA1c: glycated hemoglobin; FPG: fasting plasma glucose; PPG: postprandial plasma glucose; SD: standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Regarding comorbidities, the malignant neoplasm was found in about 25% of the patients. The specific types identified were as follows: breast cancer, thyroid cancer (follicular and papillary), colon cancer, bladder cancer, lung cancer, meningioma, malignant melanoma, undifferentiated polymorphic sarcoma, osteosarcoma, and soft tissue sarcoma.
Regarding the drugs, the most commonly used drug for diabetes mellitus was thiazolidine in 42.9% (15/35), followed by dipeptidyl peptidase-4 inhibitor (DPP4i) and metformin in 34.3% (12/35) of the patients with diabetes. Approximately 58.8% (20/34) of the patients with dyslipidemia were administered a statin. As for hypertension, calcium channel blockers followed by angiotensin II receptor blockers (ARBs) were the two most common types of drugs administered.
Regarding the blood examination, the gamma-glutamyl transpeptidase (γGTP) level was twice higher than the upper normal limit (for males 13-64, females 9-32 U/L). As for lipid profile, the mean low-density lipoprotein cholesterol (LDL-C) level was 121 ± 28 mg/dL for men and the mean triglyceride (TG) level was 161 ± 96 mg/dL, which were both slightly higher values than the normal range (for patients with diabetes, LDL-C 120 mg/dL, TG 150 mg/dL). Concerning the glucose profile, the mean glycated hemoglobin (HbA1c) was 6.42 ± 1.25%, the mean fasting plasma glucose was 118 ± 29 mg/dL, and the mean postprandial plasma glucose was 142 ± 55 mg/dL, which were all values within the target range (HbA1c 6.5%, fasting plasma glucose 126 mg/dL, postprandial plasma glucose 200 mg/dL). As for renal function, while the estimated glomerular filtration rate calculated from serum creatinine (eGFRcre) was 98.3 ± 36.3 mL/min/1.73 m2, the body surface area (BSA)-uncorrected eGFRcre was 77.8 ± 27.0 mL/min. The GFR calculated from cystatin C (eGFRcys) was 83.2 ± 29.5 mL/min/1.73 m2. Dissociation was observed between eGFRcre, BSA-uncorrected eGFRcre, and eGFRcys (P = 0.0017).
Werner Syndrome Registry longitudinal analysis
Table 2 shows the comparison between the point of registration and one year later. Although there were no significant changes in physical examination findings compared to the baseline regarding major signs, the proportion of patients with intractable skin ulcers tended to increase (62.5% vs. 75.0%, P = 0.350). Regarding comorbidities, the percentage of patients with malignant neoplasms tended to increase (20.8% vs. 25.0%, P = 1.000); four patients died from malignant neoplasms (lung cancer and undifferentiated polymorphic sarcoma, osteosarcoma, soft tissue sarcoma, and malignant melanoma), and one patient died from renal failure.
Table 2. Comparison between the point of registration and one year later.
| N | % (n patients with this characteristic) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | one year later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Major signs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Graying and/or loss of hair | 24 | 100 (24) | 100 (24) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral cataracts | 24 | 100 (24) | 100 (24) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin changes | 24 | 95.8 (23) | 95.8 (23) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intractable skin ulcers | 24 | 62.5 (15) | 75.0 (18) | 0.350 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Soft tissue calcification | 22 | 86.4 (19) | 90.9 (20) | 0.635 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bird-like face | 24 | 83.3 (20) | 87.5 (21) | 0.683 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High-pitched voice | 24 | 83.3 (20) | 83.3 (20) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes, IGT | 24 | 70.8 (17) | 79.2 (19) | 0.505 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 24 | 79.2 (19) | 83.3 (20) | 0.712 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 22 | 45.5 (10) | 36.4 (8) | 0.540 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fatty liver | 22 | 54.5 (12) | 50.0 (11) | 0.763 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AP or MI | 24 | 4.2 (1) | 8.3 (2) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAD | 24 | 4.2 (1) | 4.2 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Malignant neoplasm | 24 | 20.8 (5) | 25.0 (6) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (1) For diabetes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DPP-4 inhibitor | 23 | 21.7 (5) | 26.1 (6) | 0.730 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Biguanide | 23 | 26.1 (6) | 34.8 (8) | 0.522 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazolidine | 23 | 34.8 (8) | 30.4 (7) | 0.753 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alpha GI | 24 | 8.3 (2) | 4.2 (1) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sulfonylurea | 24 | 8.3 (2) | 4.2 (1) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SGLT2 inhibitor | 24 | 4.2 (1) | 0 (0) | 0.312 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GLP-1 analog | 24 | 4.2 (1) | 8.3 (2) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Insulin | 24 | 12.5 (3) | 12.5 (3) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (2) For dyslipidemia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 23 | 21.7 (5) | 26.1 (6) | 0.730 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrate | 23 | 26.1 (6) | 34.8 (8) | 0.522 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ezetimibe | 23 | 34.8 (8) | 30.4 (7) | 0.753 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPA | 24 | 8.3 (2) | 4.2 (1) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ion exchange resin | 24 | 8.3 (2) | 4.2 (1) | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (3) For hypertension and others | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ca blocker | 24 | 20.8 (5) | 20.8 (5) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ARB | 24 | 12.5 (3) | 8.3 (2) | 0.637 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta blocker | 24 | 8.3 (2) | 8.3 (2) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diuretics | 24 | 0 (0) | 4.2 (1) | 0.312 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 24 | 4.2 (1) | 4.2 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 23 | 8.7 (2) | 13.0 (3) | 0.636 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anticoagulant | 23 | 4.3 (1) | 4.3 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | Mean ± SD | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | one year later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical findings/function | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body weight (kg) | 21 | 45.1 ±9.7 | 44.9 ± 10.0 | 0.383 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 21 | 18.4 ± 2.8 | 18.0 ± 2.9 | 0.279 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg) | 19 | 124.0 ± 16.7 | 127.0± 18.0 | 0.628 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg) | 19 | 72.3 ± 9.5 | 73.7 ± 11.3 | 0.571 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse (/min) | 13 | 87.1 ± 14.3 | 88.7 ± 13.4 | 0.570 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference (cm) | 8 | 80.3 ± 15.6 | 79.4 ± 15.3 | 0.500 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean grip strength (right) (kg) | 8 | 18.6 ± 7.8 | 19.6 ± 7.9 | 0.469 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean grip strength (left) (kg) | 7 | 17.3 ± 7.4 | 17.4 ± 6.9 | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Blood examinations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC (/μL) | 19 | 7266 ± 1838 | 6300 ± 1988 | 0.003 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBC (x104/μL) | 19 | 455.2 ± 60.1 | 435.2 ± 75.4 | 0.447 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 19 | 13.42 ± 1.88 | 13.05 ± 2.27 | 0.574 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plt (x104/μL) | 19 | 28.3 ± 6.8 | 26.5 ± 9.9 | 0.050 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST (U/L) | 20 | 30.3 ± 12.2 | 30.7 ± 13.4 | 0.958 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT (U/L) | 20 | 44.4 ± 29.2 | 37 ± 25.5 | 0.383 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| γGTP (U/L) | 20 | 96.6 ± 141.9 | 61.3 ± 80.3 | 0.010 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDH (U/L) | 18 | 195.9 ± 36.7 | 191.7 ± 39.6 | 0.827 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALP (U/L) | 17 | 269.9 ± 197.8 | 207.9 ± 67.4 | 0.289 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ChE (U/L) | 16 | 395.1 ± 78.0 | 376.9 ± 71.6 | 0.323 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T-Bil (mg/dL) | 13 | 0.57 ± 0.14 | 0.43 ± 0.25 | 0.043 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP (g/dL) | 19 | 8.02 ± 0.51 | 7.84 ± 0.49 | 0.172 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alb (g/dL) | 18 | 4.54 ± 0.58 | 4.47 ± 0.48 | 0.510 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA (mg/dL) | 18 | 5.37 ± 1.42 | 5.23 ± 1.36 | 0.641 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BUN (mg/dL) | 20 | 17.2 ± 7.5 | 16.5 ± 6.9 | 0.595 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cre (mg/dL) | 20 | 0.775 ± 0.284 | 0.801 ± 0.293 | 0.157 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcre (mL/min/1.73 m2) | 20 | 85.4 ± 24.1 | 82.8 ± 27.6 | 0.408 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 17 | 70.8 ± 23.2 | 69.4 ± 26.6 | 0.109 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Na (mEq/L) | 20 | 139.7 ± 1.3 | 140 ± 1.7 | 0.486 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| K (mEq/L) | 20 | 4.39 ± 0.31 | 4.37 ± 0.39 | 0.624 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cl (mEq/L) | 20 | 104.5 ± 2.2 | 104.9 ± 2.7 | 0.123 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mg/dL) | 16 | 187.4 ± 29.1 | 164.1 ± 26.2 | 0.021 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG (mg/dL) | 19 | 172.3 ± 93.2 | 153 ± 74.4 | 0.390 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (direct) (mg/dL) | 13 | 118.4 ± 28.5 | 97.5 ± 20.4 | 0.033 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C (mg/dL) | 18 | 54.0 ± 10.6 | 56.1 ± 13.1 | 0.424 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c (%) | 18 | 6.43 ± 0.84 | 6.08 ± 0.63 | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FPG (mg/dL) | 5 | 115.4 ± 40.1 | 105.4 ± 10.5 | 0.625 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PPG (mg/dL) | 8 | 142.9 ± 29.9 | 152.4 ± 38.7 | 0.641 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: IGT: Impaired glucose tolerance; AP: Angina pectoris; MI: Myocardial infarction; PAD: peripheral artery disease; DPP-4: Dipeptidyl peptidase-4; alpha GI: alpha glucosidase inhibitor; SGLT2: Sodium-glucose cotransporter-2; GLP-1: Glucagon-like peptide-1; EPA: Eicosapentaenoic acid; Ca: Calcium; ARB: Angiotensin- II receptor blocker; ACE: Angiotensin-converting enzyme inhibitor; BMI: body mass index; SMI: skeletal muscle mass index; WBC: white blood cell; RBC: red blood cell; Hgb: hemoglobin; Plt: platelet; AST: aspartate aminotransferase; ALT: alanine aminotransferase; γ-GTP: gamma-glutamyl transpeptidase; LDH: lactate dehydrogenase; ALP: alkaline phosphatase; ChE: cholinesterase; T-Bil: total bilirubin; TP: total protein; Alb: albumin; UA: uric acid; BUN: blood urea nitrogen; Cre: creatinine; BSA: body surface are; eGFR: estimated glomerular filtration rate; Na: natrium; K: potassium; Cl: chlorine; TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; HbA1c: glycated hemoglobin; FPG: fasting plasma glucose; PPG: postprandial plasma glucose; SD: standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Blood examinations showed significant decreases in the white blood cell count (7266/μL vs. 6300/μL, P = 0.003), γGTP (96.6 mg/dL vs. 61.3 mg/dL, P = 0.010), and total bilirubin (T-Bil; 0.57 mg/dL vs. 0.43 mg/dL, P = 0.043). Significant decreases in total cholesterol (TC; 187.4 mg/dL vs. 164.1 mg/dL, P = 0.021), LDL-C (118.4 mg/dL vs. 97.5 mg/dL, P = 0.033), and HbA1c (6.43% vs. 6.08%, P = 0.030) were also observed.
Table 3 shows the comparison between the point of registration and two years later. Due to the difference in patients’ enrolled period, the number of observed patients decreased by the end of the study. The mean body weight decreased significantly (44.4 kg vs. 43.0 kg, P = 0.029). One patient died from brainstem hemorrhage caused by a myelodysplastic syndrome with overt acute myeloid leukemia infiltration to the central nervous system.
Table 3. Comparison between the point of registration and two years later.
| N | % (n patients with this characteristic) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | two years later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Major signs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Graying and/or loss of hair | 20 | 100 (20) | 100 (20) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral cataracts | 20 | 100 (20) | 100 (20) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin changes | 20 | 95 (19) | 100 (20) | 0.311 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intractable skin ulcers | 20 | 60 (12) | 75 (15) | 0.311 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Soft tissue calcification | 20 | 85 (17) | 85 (17) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bird-like face | 20 | 85 (17) | 80 (16) | 0.677 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High-pitched voice | 20 | 80 (16) | 80 (16) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes, IGT | 20 | 75 (15) | 80 (16) | 0.705 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 20 | 75 (15) | 80 (16) | 0.705 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 19 | 42.1 (8) | 42.1 (8) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fatty liver | 19 | 47.4 (9) | 52.6 (10) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebral bleeding | 20 | 0 (0) | 5 (1) | 0.311 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cerebral infarction | 20 | 0 (0) | 5 (1) | 0.311 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AP or MI | 20 | 5 (1) | 5 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAD | 20 | 0 (0) | 5 (1) | 0.311 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Malignant neoplasm | 20 | 25.0 (5) | 35.0 (7) | 0.731 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (1) For diabetes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DPP-4 inhibitor | 19 | 31.6 (6) | 26.3 (5) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Biguanide | 19 | 21.1 (4) | 36..8 (7) | 0.476 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazolidine | 19 | 47.4 (9) | 31.6 (6) | 0.508 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alpha GI | 19 | 5.3 (1) | 0 (0) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sulfonylurea | 19 | 10.5 (2) | 5.3 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GLP-1 analog | 19 | 5.3 (1) | 10.5 (2) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Insulin | 19 | 15.8 (3) | 15.8 (3) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (2) For dyslipidemia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 19 | 63.2 (12) | 52.6 (10) | 0.743 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrate | 19 | 5.3 (1) | 10.5 (2) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPA | 19 | 5.3 (1) | 5.3 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nicotinic acids | 19 | 10.5 (2) | 5.3 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (3) For hypertension, and others | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ca blocker | 19 | 21.1 (4) | 31.6 (6) | 0.714 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ARB | 19 | 15.8 (3) | 5.3 (1) | 0.604 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta blocker | 19 | 10.5 (2) | 10.5 (2) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspirin | 19 | 5.3 (1) | 5.3 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 18 | 5.6 (1) | 5.6 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anticoagulant | 18 | 5.6 (1) | 0 (0) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | Mean ± SD | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | two years later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical findings/function | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body weight (kg) | 19 | 44.4 ±9.5 | 43.0 ± 10.3 | 0.029 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 18 | 18.0 ± 2.9 | 17.5 ± 3.3 | 0.056 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg) | 15 | 123.9 ± 15.9 | 119.1± 17.3 | 0.482 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg) | 15 | 72.5 ± 10.4 | 70.3 ± 8.9 | 0.270 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse (/min) | 6 | 84.7 ± 17.3 | 81.5 ± 17.2 | 0.719 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Waist circumference (cm) | 6 | 74.6 ± 11.0 | 74.9 ± 10.2 | 0.625 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean grip strength (right) (kg) | 5 | 16.5 ± 6.9 | 15.0 ± 4.1 | 0.438 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mean grip strength (left) (kg) | 4 | 13.5 ± 6.5 | 12.1 ± 3.1 | 0.625 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Blood examinations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC (/μL) | 16 | 6859 ± 1696 | 7186 ± 2261 | 0.836 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBC (x104/μL) | 16 | 442.6 ± 52.8 | 412.6 ± 89.3 | 0.298 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 16 | 13.05 ± 1.79 | 12.66 ± 2.85 | 0.850 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plt (x104/μL) | 16 | 28.33 ± 6.64 | 64.53 ± 106.3 | 0.744 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST (U/L) | 17 | 26.4 ± 9.6 | 28.3 ± 9.9 | 0.551 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT (U/L) | 17 | 35.8 ± 27.4 | 31.6 ± 20.8 | 0.923 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| γGTP (U/L) | 16 | 82.4 ± 129.3 | 71.1 ± 78.4 | 0.536 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDH (U/L) | 14 | 195.9 ± 39.6 | 202.4 ± 46.6 | 0.366 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALP (U/L) | 13 | 248.8 ± 215.0 | 205.0 ± 111.2 | 0.906 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ChE (U/L) | 12 | 374.7 ± 70.8 | 373.8 ± 90.5 | 0.733 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T-Bil (mg/dL) | 9 | 0.55 ± 0.16 | 0.34 ± 0.29 | 0.039 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP (g/dL) | 16 | 7.96 ± 0.54 | 7.78 ± 0.61 | 0.774 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alb (g/dL) | 15 | 4.44 ± 0.59 | 4.27 ± 0.68 | 0.668 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA (mg/dL) | 15 | 5.38 ± 1.45 | 4.72 ± 0.88 | 0.089 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BUN (mg/dL) | 16 | 17.7 ± 8.0 | 17.2 ± 6.7 | 0.657 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cre (mg/dL) | 17 | 0.766 ± 0.311 | 0.788 ± 0.386 | 0.451 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcre (mL/min/1.73 m2) | 17 | 84.5 ± 25.6 | 87.6 ± 41.6 | 0.644 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 15 | 68.5 ± 22.8 | 70.6 ± 33.6 | 0.639 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Na (mEq/L) | 16 | 139.7 ± 1.4 | 138.8 ± 3.6 | 0.461 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| K (mEq/L) | 16 | 4.33 ± 0.33 | 5.48 ± 3.65 | 0.022 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cl (mEq/L) | 16 | 104.7 ± 2.2 | 97.9 ± 26.2 | 0.892 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mg/dL) | 12 | 182.0 ± 23.6 | 173.6 ± 26.5 | 0.531 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG (mg/dL) | 15 | 146.1 ± 79.1 | 141.2 ± 53.4 | 0.836 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (direct) (mg/dL) | 11 | 113.2 ± 27.9 | 101.4 ± 27.3 | 0.182 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C (mg/dL) | 14 | 57.1 ± 10.7 | 55.2 ± 11.1 | 0.726 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c (%) | 16 | 6.26 ± 0.65 | 6.31 ± 1.02 | 0.550 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PPG (mg/dL) | 7 | 137.0 ± 26.9 | 148.1 ± 34.3 | 0.375 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: IGT: Impaired glucose tolerance; AP: Angina pectoris; MI: Myocardial infarction; PAD: peripheral artery disease; DPP-4: Dipeptidyl peptidase-4; alpha GI: alpha glucosidase inhibitor; SGLT2: Sodium-glucose cotransporter-2; GLP-1: Glucagon-like peptide-1; EPA: Eicosapentaenoic acid; Ca: Calcium; ARB: Angiotensin- II receptor blocker; ACE: Angiotensin-converting enzyme inhibitor; BMI: body mass index; SMI: skeletal muscle mass index; WBC: white blood cell; RBC: red blood cell; Hgb, hemoglobin; Plt: platelet; AST, aspartate aminotransferase; ALT: alanine aminotransferase; γ-GTP: gamma-glutamyl transpeptidase; LDH: lactate dehydrogenase; ALP: alkaline phosphatase; ChE: cholinesterase; T-Bil: total bilirubin; TP: total protein; Alb: albumin; UA: uric acid; BUN: blood urea nitrogen; Cre: creatinine; BSA: body surface are; eGFR: estimated glomerular filtration rate; Na: natrium; K: potassium; Cl: chlorine; TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; HbA1c: glycated hemoglobin; FPG: fasting plasma glucose; PPG: postprandial plasma glucose; SD: standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The blood examination showed that glucose and lipid metabolism were controlled within the target range, and T-Bil decreased (0.55 mg/dL vs. 0.34 mg/dL, P = 0.039), while a new increase in the mean serum potassium was observed (4.33 mEq/L vs. 5.48 mEq/L, P = 0.022). Regarding therapeutic drugs, metformin tended to increase, while thiazolidine tended to decrease in association with diabetes, and the use of ARBs as antihypertensive drugs were discontinued in two patients using them.
Table 4 shows the comparison between the point of registration and three years later. A significant decrease in renal function was observed over time. At the point of registration, the mean eGFRcre was 74.8 mL/min/1.73/m2, and the mean BSA-uncorrected eGFRcre was 59.3 mL/min, whereas three years later, the mean eGFRcre was 63.4 mL/min/1.73 m2 (P = 0.078) and the mean BSA-uncorrected eGFRcre was 50.2 mL/min (P = 0.047), which correlated to a decrease of approximately 3 mL/min (/1.73 m2) per a year on average.
Table 4. Comparison between the point of registration and three years later.
| N | % (n patients with this characteristic) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | three years later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Major signs | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Graying and/or loss of hair | 9 | 100 (9) | 100 (9) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bilateral cataracts | 9 | 100 (9) | 100 (9) | − | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin changes | 9 | 88.9 (8) | 100 (9) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intractable skin ulcers | 9 | 66.7 (6) | 77.8 (7) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Soft tissue calcification | 9 | 100 (9) | 100 (9) | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bird-like face | 9 | 77.8 (7) | 77.8 (7) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| High-pitched voice | 9 | 77.8 (7) | 88.9 (8) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Clinical symptoms | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes, IGT | 9 | 55.6 (5) | 66.7 (6) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 9 | 66.7 (6) | 77.8 (7) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 8 | 50.0 (4) | 62.5 (5) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fatty liver | 9 | 55.6 (5) | 66.7 (6) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAD | 9 | 0 (0) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Malignant neoplasm | 9 | 44.4 (4) | 44.4 (4) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Medications | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (1) For diabetes | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DPP-4 inhibitor | 9 | 22.2 (2) | 33.3 (3) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Biguanide | 9 | 11.1 (1) | 22.2 (2) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiazolidine | 9 | 22.2 (2) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GLP-1 analog | 9 | 11.1 (1) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Insulin | 9 | 11.1 (1) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (2) For dyslipidemia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Statin | 9 | 55.6 (5) | 55.6 (5) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrate | 9 | 11.1 (1) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EPA | 9 | 11.1 (1) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nicotinic acids | 9 | 22.2 (2) | 11.1 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| (3) For hypertension and others | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ca blocker | 8 | 37.5 (3) | 50.0 (4) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ARB | 8 | 12.5 (1) | 0 (0) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Beta blocker | 8 | 12.5 (1) | 12.5 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antiplatelet | 8 | 12.5 (1) | 12.5 (1) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anticoagulant | 8 | 12.5 (1) | 0 (0) | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | Mean ± SD | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| at registration | three years later | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physical findings/function | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Body weight (kg) | 7 | 45.29 ±4.62 | 44.30 ± 4.57 | 0.281 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI (kg/m2) | 3 | 18.06 ± 1.43 | 17.35 ± 1.69 | 0.500 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Systolic blood pressure (mmHg) | 5 | 132.8 ± 21.6 | 138.4± 15.8 | 0.625 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diastolic blood pressure (mmHg) | 5 | 74.0 ± 10.77 | 76.6 ± 12.54 | 0.875 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulse (/min) | 4 | 92.5 ± 12.0 | 93.5 ± 22.2 | 0.875 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Blood examinations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| WBC (/μL) | 6 | 7517 ± 1699 | 8550 ± 2671 | 0.313 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RBC (x104/μL) | 6 | 424.8 ± 69.7 | 394.7 ± 63.2 | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hb (g/dL) | 6 | 12.05 ± 2.02 | 12.15 ± 1.82 | 0.688 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plt (x104/μL) | 6 | 29.23 ± 5.44 | 33.27 ± 7.01 | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AST (U/L) | 7 | 24.7 ± 4.2 | 24.3 ± 9.6 | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALT (U/L) | 8 | 28.6 ± 14.5 | 27.8 ± 17.4 | 0.734 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| γGTP (U/L) | 8 | 43.5 ± 32.3 | 58.4 ± 55.9 | 0.398 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDH (U/L) | 7 | 195.9 ± 39.9 | 194.9 ± 26.5 | 0.563 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ALP (U/L) | 6 | 204.5 ± 100.9 | 241.2 ± 69.4 | 0.156 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ChE (U/L) | 6 | 374.2 ± 98.0 | 376.0 ± 102.2 | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TP (g/dL) | 7 | 7.94 ± 0.20 | 8.14 ± 0.59 | 0.641 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alb (g/dL) | 7 | 4.34 ± 0.69 | 4.36 ± 0.29 | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| UA (mg/dL) | 8 | 5.56 ± 1.40 | 4.91 ± 1.03 | 0.109 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BUN (mg/dL) | 7 | 23.1 ± 9.1 | 25.6 ± 12.3 | 0.438 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cre (mg/dL) | 7 | 0.904 ± 0.425 | 1.133 ± 0.747 | 0.078 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcre (mL/min/1.73 m2) | 7 | 74.8 ± 33.5 | 63.4 ± 31.9 | 0.078 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 7 | 59.3 ± 25.2 | 50.2 ± 26.9 | 0.047 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Na (mEq/L) | 7 | 139.3 ± 1.6 | 139.7 ± 2.0 | 0.531 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| K (mEq/L) | 7 | 4.51 ± 0.37 | 4.96 ± 0.82 | 0.141 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cl (mEq/L) | 7 | 104.6 ± 2.9 | 105.0 ± 3.8 | 0.922 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TC (mg/dL) | 6 | 179.8 ± 16.7 | 189.7 ± 25.9 | 0.563 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TG (mg/dL) | 7 | 114.1 ± 25.8 | 126.6 ± 55.6 | 0.578 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LDL-C (direct) (mg/dL) | 4 | 115.0 ± 17.9 | 103.3 ± 11.9 | 0.375 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HDL-C (mg/dL) | 6 | 52.3 ± 8.8 | 54.2 ± 8.9 | 0.375 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HbA1c (%) | 7 | 6.20 ± 0.70 | 6.17 ± 0.91 | 0.875 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PPG (mg/dL) | 3 | 144.0 ± 24.8 | 139.0 ± 11.1 | 1.000 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: IGT: Impaired glucose tolerance; AP: Angina pectoris; MI: Myocardial infarction; PAD: peripheral artery disease; DPP-4: Dipeptidyl peptidase-4; alpha GI: alpha glucosidase inhibitor; SGLT2: Sodium-glucose cotransporter-2; GLP-1: Glucagon-like peptide-1; EPA: Eicosapentaenoic acid; Ca: Calcium; ARB: Angiotensin- II receptor blocker; ACE: Angiotensin-converting enzyme inhibitor; BMI: body mass index; SMI: skeletal muscle mass index; WBC: white blood cell; RBC: red blood cell; Hgb: hemoglobin; Plt: platelet; AST: aspartate aminotransferase; ALT: alanine aminotransferase; γ-GTP: gamma-glutamyl transpeptidase; LDH: lactate dehydrogenase; ALP: alkaline phosphatase; ChE: cholinesterase; T-Bil: total bilirubin; TP: total protein; Alb: albumin; UA: uric acid; BUN: blood urea nitrogen; Cre: creatinine; BSA: body surface are; eGFR: estimated glomerular filtration rate; Na: natrium; K: potassium; Cl: chlorine; TC: total cholesterol; TG: triglyceride; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; HbA1c: glycated hemoglobin; FPG: fasting plasma glucose; PPG: postprandial plasma glucose; SD: standard deviation. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The results of the survey covering the entire period regarding malignant neoplasms, renal function, and aspiration pneumonia are described below.
Regarding malignant neoplasms, the morbidity due to malignant neoplasms at baseline was 25.5% (out of 51 patients) and 31.4% in the entire survey period. Table 5 shows the type of malignant neoplasms and the age of onset. The breakdown of the malignant neoplasm types revealed epithelial neoplasms in eight patients (15.7%), non-epithelial in four patients (7.8%), and both in three patients (5.9%). Multiple neoplasms were found in 3/51 (5.9%) of all the patients enrolled, and 3/16 (18.8%) of the patients with malignant neoplasms.
Table 5. Type of malignant neoplasms and age of onset.
| Patient No. | Age of onset (years) | Type of malignant neoplasm | Age during reporting or die (years) | Status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 32 | Bladder cancer | 61 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | 36 | Breast cancer | 44 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | 42 | Colon cancer | 56 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 | 48, 49 | Papillary thyroid cancer, meningiomaa | 49 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 | 48 | Myelodysplastic syndromea, acute myeloid leukemiaa | 48 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 6 | 50 | Papillary thyroid cancer | 50 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 7 | 52 | Lung adenocarcinoma | 53 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 8 | 52 | Breast cancer | 55 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 9 | 56 | Melanomaa | 58 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 10 | 57, 60, 64 | Meningiomaa, breast cancer, lung cancer | 65 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 11 | Unknown | Osteosarcomaa | 45 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 12 | Unknown | Thyroid follicular carcinoma | 53 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 13 | Unknown, unknown | Lung cancer, undifferentiated pleomorphic sarcomaa | 55 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 14 | Unknown | Soft tissue sarcomaa | 56 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 15 | Unknown | Lung adenocarcinoma | 64 | Alive | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 16 | Unknown | Unknown | 64 | Dead | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| aShows non-epithelial neoplasm. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Regarding renal function, Figure 1 shows the age group and the mean renal function during the entire survey period. Of the three indices of renal function, there was a discrepancy between eGFRcre and BSA-uncorrected eGFRcre/eGFRcys. The mean eGFRcre, BSA-uncorrected eGFRcre, and eGFRcys for each age decile were as follows: 30s, 129.9/108.5/121.6; 40s, 93.7/74.5/69.0; 50s, 88.2/72.8/79.8; and 60s, 50.2/36.9/33.1.
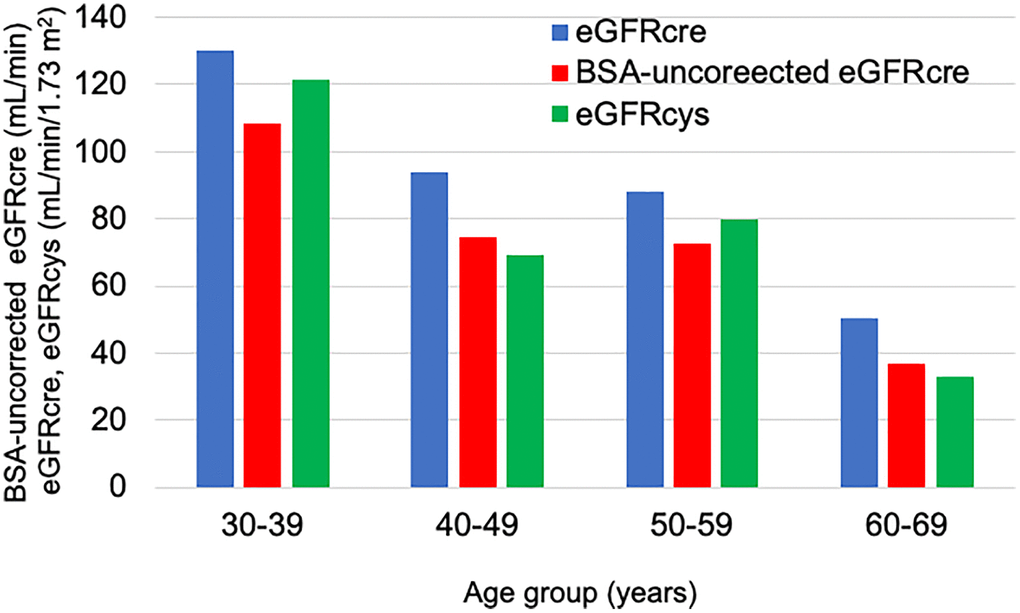
Figure 1. Average renal function in each age group over the entire survey period. The blue bar shows the eGFRcre. The red bar shows the BSA-uncorrected eGFRcre. The green bar shows the eGFRcys.
Many patients with Werner syndrome have painful leg ulcers and frequently use non-steroidal anti-inflammatory drugs (NSAIDs). Frequent use of NSAIDs is connected with an observed decrease in renal function. Table 6 shows that in the relationship between the presence of leg ulcers and renal function, renal function tended to be low in patients with leg ulcers, and eGFRcre, BSA-uncorrected eGFRcre, and eGFRcys were as follows: patients with leg ulcers, 91.5 ± 30.5 mL/min/1.73 m2 vs. without leg ulcers, 112.9 ± 43.9 mL/min/1.73 m2, P = 0.121; 73.7 ± 25.2 mL/min vs. 86.3 ± 29.4 mL/min, P = 0.228; and 77.0 ± 27.5 mL/min/1.73 m2 vs. 100.1 ± 32.2 mL/min/1.73 m2, P = 0.240, respectively. In relation to the usage of NSAIDs, there was no difference in renal function between the users and non-users, as follows: NSAIDs user 94.0 ± 28.7 mL/min/1.73 m2 vs. non-user 99.2 ± 38.0 mL/min/1.73 m2, P = 0.830; 74.5 ± 26.3 mL/min vs. 78.5 ± 27.4 mL/min, P = 0.910, and 75.0 ± 9.2 mL/min/1.73 m2 vs. 85.2 ± 32.7 mL/min/1.73 m2, P = 0.471, respectively.
Table 6. Relationship between renal function and the presence of leg ulcers/the usage of NSAIDs.
| N | Patients with ulcer (mean ± SD) | N | Patients without ulcer (mean ± SD) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR (mL/min/1.73 m2) | 34 | 91.5 ± 30.5 | 16 | 112.9 ± 43.9 | 0.121 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 34 | 73.7 ± 25.2 | 16 | 86.3 ± 29.4 | 0.228 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcys (mL/min/1.73 m2) | 11 | 77.0 ± 27.5 | 4 | 100.1 ± 32.2 | 0.240 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N | Patients with NSAIDs (mean ± SD) | N | Patients without NSAIDs (mean ± SD) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFR (mL/min/1.73 m2) | 9 | 94.0 ± 28.7 | 41 | 99.2 ± 38.0 | 0.830 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BSA-uncorrected eGFRcre (mL/min) | 9 | 74.5 ± 26.3 | 41 | 78.5 ± 27.4 | 0.910 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| eGFRcys (mL/min/1.73 m2) | 3 | 75.0 ± 9.2 | 12 | 85.2 ± 32.7 | 0.471 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: NSAIDs: non-steroidal anti-inflammatory drugs; eGFR: estimated glomerular filtration rate; BSA: body surface area. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Two patients (4.9%) were hospitalized with aspiration pneumonia; the age at onset was 67 years and 63 years, respectively.
During the four-year follow-up, deaths could be confirmed in six patients, of whom five died from malignant neoplasms and one from renal failure. The average age of death was 54.2 years (52.4 years for malignant neoplasms and 63.0 years for renal failure).
Discussion
Data from the registry described in this study revealed the occurrence of changes over time for up to four years after registration in patients with Werner syndrome in Japan. Notably, a novel finding was that the index of renal function may greatly deviate from the actual state of renal function and that the rate of decline in renal function may be rapid. Although there were case reports regarding declining renal function in a patient with Werner syndrome [12–15], there was no report with a large sample size and long-term follow-up. Moreover, it was clarified that the morbidity due to malignant neoplasms is higher than that of the general population, the age of onset is younger, and both epithelial and non-epithelial neoplasms exist in similar ratios. In addition, aspiration pneumonia was observed in patients in their sixties.
The life expectancy of patients with Werner syndrome is extending [7] due to improvements in understanding the pathology of Werner syndrome and the development of medical treatments for diabetes and dyslipidemia [9]. Therefore, longer-term, more detailed follow-ups and medical interventions are needed. Atherosclerotic cardiovascular diseases (ASCVD), malignant neoplasms, sarcopenia, and leg ulcers were mentioned as the main pathological conditions affecting the prognosis of patients with Werner syndrome. The medical intervention seems to be effective for improving life quality [16–18]. Each important comorbidity is now discussed as follows.
Malignant neoplasms
In this study, the morbidity due to malignant neoplasms at baseline was 25.5% (13/51 patients). The morbidity due to malignant neoplasms in patients with Werner syndrome is increasing, and aging is a possible contributing factor [19]. In other words, patients with Werner syndrome are no longer dying from cardiovascular diseases at a young age; therefore, the morbidity due to malignant neoplasms may be increasing as a result.
Moreover, the ratio of epithelial neoplasms to non-epithelial neoplasms is generally approximately 10:1, while patients with Werner syndrome have very high morbidity associated with non-epithelial neoplasms [19, 20]. Similarly, the ratio of epithelial neoplasms to non-epithelial neoplasms was 12:7 for the entire study period.
Although the prevalence of epithelial neoplasms has been reported to be significantly higher in patients with diabetes compared to patients without diabetes [19], Lauper et al. reported no association between diabetes and epithelial or non-epithelial neoplasms [21]. In our study, the prevalence of epithelial neoplasms in patients with diabetes was 18.9%, and that in patients without diabetes was 28.6%.
Furthermore, reportedly, the age of onset for malignant neoplasm was low in patients with Werner syndrome, with the predominant onset age for malignant neoplasms being 25–65 years. In particular, the morbidity due to non-epithelial neoplasms, in other words, those of mesenchymal origin (sarcoma), is particularly high (20%) in patients with Werner syndrome before the age of 41 years [22]. In other reports, the average age of malignant neoplasm onset was 47.2 years for epithelial neoplasms, 45.2 years for non-epithelial neoplasms, and 45.8 years for all malignant neoplasms [19]. Figure 2 shows the percentage of malignant neoplasms by onset in each age group. Epithelial neoplasms developed at a younger age, and the incidence of non-epithelial neoplasms increased during the late 40s. The average age of onset was 48.4 years for epithelial neoplasms, 52.5 years for non-epithelial neoplasms, and 49.7 years for all malignant neoplasms. Therefore, the age of onset of non-epithelial neoplasms is higher than in previous reports as well. This may be due to the fact that the patients’ lifespan has been prolonged by cardiovascular disease prevention and epithelial neoplasm treatment.
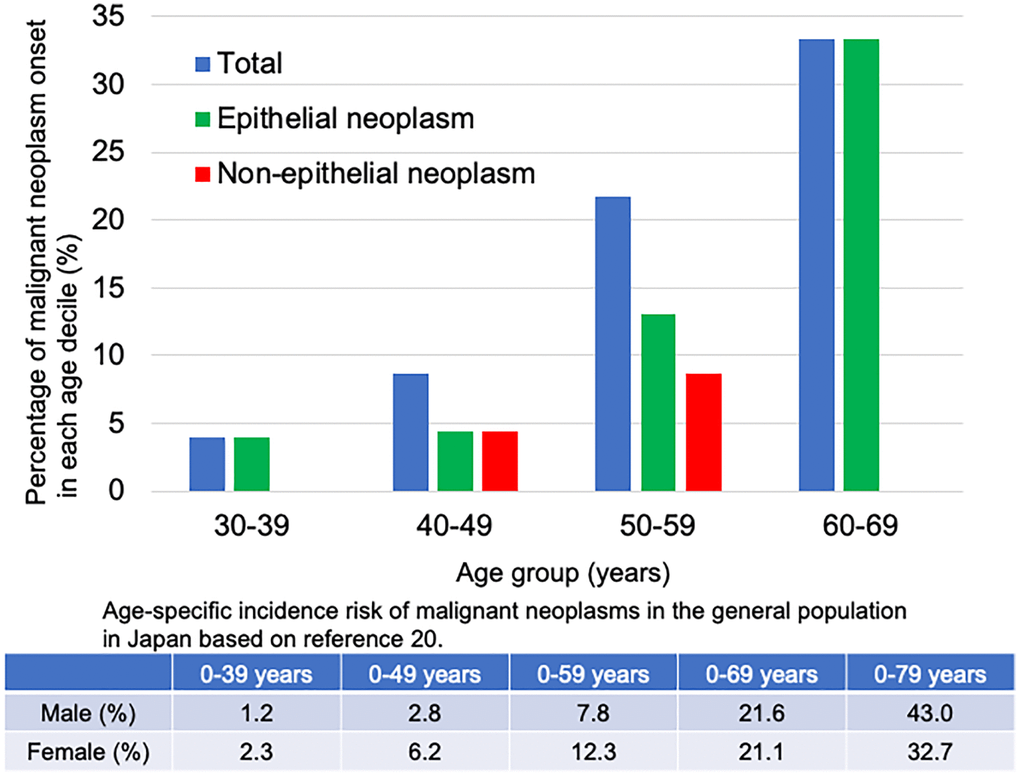
Figure 2. Percentage of malignant neoplasms onset in each age decile in the patients with Werner syndrome. The blue bar shows the percentage of total malignant neoplasms in each age group. The green bar shows the percentage of epithelial neoplasms in each age group. The red bar shows the percentage of non-epithelial neoplasms in each age group. Patients with thyroid follicular cancer, osteosarcoma, lung cancer/undifferentiated polymorphic sarcoma, and soft tissue sarcoma were excluded because the exact age of onset was unknown.
The table in Figure 2 shows the age-specific incidence risk of malignant neoplasms in the general population in Japan. Since the probability of malignant neoplasms in the 30s and 60s of the general population is 1.2–21.6%, the morbidity due to malignant neoplasms is higher in the same age group of patients with Werner syndrome. Malignant neoplasms onset is approximately 10 years earlier in patients with Werner syndrome than in the general population [23].
A high percentage of multiple neoplasms is also characteristic of patients with Werner syndrome. In other reports, there were multiple neoplasms in 5.3% of all patients and 15–20% of patients with malignant neoplasms [19, 24]. A similar tendency was observed in this study.
Reportedly, two-thirds of neoplasms in the Werner syndrome population were thyroid neoplasms, malignant melanomas, meningiomas, soft tissue sarcomas, leukemia and preleukemic conditions, and osteosarcoma and bone neoplasms; in our study, half of the patients with malignant neoplasms had these neoplasms, and the incidence of breast and lung cancers in the epithelial neoplasm group was also high [25]. Regarding osteosarcoma, X-ray screening of long bones may be useful. Therefore, screening of these neoplasms should be prioritized.
Currently, the main cause of death in patients with Werner syndrome is malignant neoplasms development, and malignant neoplasms greatly influence prognosis; therefore, early detection and treatment by regular screening from a younger age are both very important to ameliorate their prognosis.
There are some cautions to be considered regarding cancer treatment for patients with Werner syndrome. Reportedly, a patient with a heterozygous mutation in the WRN gene and a retroperitoneal liposarcoma had dramatic renal and hematological toxicity after cytotoxic chemotherapy [26]. For patients with a WRN mutation, close monitoring of the hematologic profile and renal function is needed to avoid severe toxicities. Furthermore, it was reported that radiotherapy is contraindicated in most homozygous patients with recessive radiosensitivity syndromes, including Werner syndrome [27]. Therefore, safer and more effective new cancer treatments for patients with Werner syndrome are needed.
Recently, the mechanism of high morbidity and treatment strategies for malignant neoplasm in patients with Werner syndrome have been getting clear. The Werner syndrome ATP-dependent helicase (WRN) is a RecQ enzyme involved in the maintenance of genome integrity. WRN is associated with Werner syndrome and a predisposition to multiple cancers, such as multiple myeloma [28], myelodysplastic syndrome/acute myeloid leukemia [29], colorectal cancer [30], breast cancer [31], and ovarian cancer [32]. WRN contributes to chromosomal stability for survival in both normal and cancer cells [33]. WRN is also required for DNA damage repair and the survival of cancer cells with microsatellite instability (MSI) [34]. WRN depletion induces double-strand DNA breaks and promotes apoptosis and cell cycle arrest selectively in MSI models. Loss of WRN leads to synthetic lethality in mismatch repair-deficient/high MSI cells [35].
Genome-wide screening studies have reported that WRN inhibition induces massive chromosome disruption [36] and synthetic lethality in cancer cells with high MSI [37, 38]. The development possibility of novel therapeutic agents that target WRN for MSI-associated cancers by pharmacological inhibition of WRN helicase function has been reported [35, 36, 38]. Reportedly, exposure to small-molecule compounds, such as NSC 19630 (N-(1-(4-((4-methoxyphenyl) amino) quinazolin-6-yl) ethyl)-3-(pyridin-3-yl) acrylamide) and NSC 617145 (5-(4-chlorophenyl)-4-(4-methylphenyl)-4,5-dihydro-1H-imidazol-2-amine N-(4-methylphenyl) sulfonylacetamide), which inhibits WRN helicase activity, sensitizes cancer cells to DNA-damaging agents [39] and DNA cross-linking agents [40]. Sublethal dosage of small-molecule compounds and the chemotherapy drug act synergistically to inhibit cell proliferation and induce DNA damage in cancer cells. These studies are still in progress and thus the results are highly awaited.
Renal function
According to the renal function index, the discrepancy was observed in patients with Werner syndrome. It may be because patients with Werner syndrome have a smaller body size and less muscle mass than those without Werner syndrome.
The calculation of eGFRcre (mL/min/1.73 m2) requires the serum creatinine level, age, and sex. The calculation of BSA-uncorrected eGFRcre (mL/min) requires five items: serum creatinine level, age, sex, height, and weight. In other words, it considers the physique. The calculation of eGFRcys (mL/min/1.73 m2) requires three items: serum cystatin C level, age, and sex. Therefore, it is not affected by muscle mass.
Since creatinine is easily affected by muscle mass, diet, and exercise, eGFRcre is often higher in older adults with less muscle mass, and discrepancies are likely to be observed. The situation is similar to that in patients with Werner syndrome. Therefore, in the patients with Werner syndrome, it is considered that eGFRcre dissociates from BSA-uncorrected eGFRcre and eGFRcys.
It can be observed from Figure 1 that the eGFRcys/eGFRcre ratios are <1.0. Reportedly, the presence of low eGFRcys/eGFRcre ratios (<1.0) is associated with sarcopenia [41]. In Figure 1, the eGFRcys/eGFRcre ratio is also low in non-elderly people, which may reflect that patients with Werner syndrome are small and have low muscle mass even at a young age. Therefore, there are concerns due to the dissociation of the renal function indices. Side effects may likely occur when using medicines such as antibiotics and NSAIDs for patients with poor renal function. For patients with extremely small body size and decreased renal function, the use of BSA-uncorrected eGFRcre or eGFRcys is preferable to eGFRcre. It is important to carefully consider which renal function index to use before deciding the amount of medicine to be used.
The other problem is that when there is a worse eGFRcys than eGFRcre, it is associated with a higher risk of death and end-stage renal disease [42, 43]. Therefore, it is necessary to carefully follow the course of a patient’s renal function.
Renal function (eGFRcre, BSA-uncorrected eGFRcre) tended to decrease over three years, and BSA-uncorrected eGFRcre showed a significant decrease. The average rate of decline in BSA-uncorrected eGFRcre in the patients with Werner syndrome was 9.1 mL/min for three years, that is, approximately 3 mL/min in a year. In addition, as Figure 1 shows, the decrease in renal function is remarkable in the 30s and after the 50s. The average rate of decline in eGFR for general Japanese people aged 40 and above is 0.36 mL/min/1.73 m2 (males 40–49 years: 0.35 mL/min/1.73 m2; 50–59 years: 0.31 mL/min/1.73 m2; 60–69 years: 0.37 mL/min/1.73 m2; 70–79 years: 0.42 mL/min/1.73 m2; females 40–49 years: 0.41 mL/min/1.73 m2; 50–59 years: 0.31 mL/min/1.73 m2; 60–69 years: 0.32 mL/min/1.73 m2; and 70–79 years: 0.39 mL/min/1.73 m2) [44]. Therefore, this suggests that the rate of renal function decline was faster than that of the general population of the same age.
While the management of diabetes and hypertension was appropriate, the use of analgesics such as NSAIDs was considered one of the reasons that the rate of renal function decline was rapid. Approximately 70% of patients with Werner syndrome develop painful intractable ulcers, and NSAIDs are frequently used. Although there was no relationship between leg ulcers or NSAIDs and renal function in this three-year follow-up, various factors, such as the presence of peripheral angiopathy, also affect the results; therefore, it may be necessary to pay attention to the dose of NSAIDs in patients with painful intractable ulcers. The use of NSAIDs in older adults is often noted, and similar caution is needed in patients with Werner syndrome, even the non-elderly, whose renal dysfunction cannot be predicted by eGFRcre alone. For other medicines, such as antibiotics, anti-cancer drugs, and ARBs, it is also necessary to care about drug-induced renal damage or side effects due to overdose.
Atherosclerotic cardiovascular diseases and metabolic diseases
ASCVDs, such as myocardial infarction, angina pectoris, and atherothrombotic cerebral infarction, were not common during the study period. The reduction of ASCVD appears to be extending the life expectancy of patients with Werner syndrome. This is presumed to be associated with the improved management of metabolic diseases such as diabetes, dyslipidemia, and hypertension. Regarding diabetes treatments, similar to findings in a previous report [9], pioglitazone, metformin, and insulin sensitizers were often used. While, longitudinally, the percentage of metformin use has increased more than that of pioglitazone, suggesting that the negative effects of pioglitazone on osteoporosis may be considered. Among those with dyslipidemia, statins were used in 58.8% of patients. Although the baseline data were generally within the control target range over four years, the LDL-C level decreased more from baseline, suggesting suitable interventions took place. Hypertriglyceridemia should also be noted. It was reported that a 29-year-old patient with Werner syndrome and hypertriglyceridemia (triglyceride level of 3900 mg/dL) had advanced three-vessel disease requiring coronary artery bypass graft surgery [45]. Therefore, in addition to statins, management of hypertriglyceridemia may also be needed. Regarding antihypertensive medications, the use of ARBs decreased in patients over the four years, and eventually, there were no patients using ARBs. Hyperkalemia was cited as one of the reasons for medication discontinuation, suggesting a relationship with impaired renal function. Although metabolic diseases were sufficiently controlled overall, as life expectancy prolongs, appropriate medications must be selected to address potential side effects. Moreover, patients with severe aortic stenosis [46, 47] and heart failure due to impaired coronary microcirculation with no coronary artery stenosis have been reported [48]. Therefore, a comprehensive evaluation of arteriosclerosis in patients with Werner syndrome is still needed.
Sarcopenia
The sarcopenia diagnostic criteria by the Asian Working Group for Sarcopenia 2019 [49] has three indicators, of them, the following three indicators were used in this survey: 1) grip strength (male/female) <28 kg/<18 kg, 2) walking speed <1.0 m/s, and 3) SMI dual-energy X-ray absorptiometry <7.0 kg/m2 (male) and <5.4 kg/m2 (female), SMI bioimpedance, <7.0 kg/m2 (male) and <5.7 kg/m2 (female). As Table 1 shows, the mean values of grip strength and SMI in the present registry met the criteria of 1) and 3), and sarcopenia was suspected. The patients with Werner syndrome tended to have sarcopenia obesity (visceral fat increase despite low BMI). It was reported that sarcopenia tended to appear before visceral fat accumulation [50]. Moreover, over the years, body weight, BMI, and grip strength tended to decrease in this study. The adipogenic and chondrogenic differentiation capacity was significantly decreased in the foot fibroblasts of patients when Werner syndrome in vitro. It may partially explain the underlying mechanism of sarcopenia in patients with Werner syndrome [51]. The presence of sarcopenia may be related not only to QOL reduction but also to renal function evaluation, as aforementioned, suggesting that sarcopenia prevention is needed. Measures such as leucine intake [52, 53] and strength training [54, 55], which have general preventive effects on sarcopenia, should be considered. Ghrelin receptor agonist has been shown to increase body weight, muscle mass, and appetite in patients with cancer cachexia [56, 57]. These findings suggest that ghrelin receptor agonist also may be effective in patients with Werner syndrome, in whom skeletal muscle mass is significantly reduced.
Other complications associated with aging
As lifespans prolong, complications such as aspiration pneumonia, which are often seen in late older adults, are increasing. Two patients with aspiration pneumonia were reported in this survey. They were aged in their 60s and were thus younger than the average age group that generally experienced aspiration pneumonia. Vaccinations to prevent pneumonia in those aged in their early 60s and oral care may be useful preventive measures. Further, the use of benzodiazepine should be avoided.
This study is limited because the evaluated registry does not cover all patients with Werner syndrome in Japan. However, almost half of the patients confirmed in a previous national survey registered; therefore, the clinical evidence was established based on a highly universal (and the largest) database of Werner syndrome in Japan.
Although the overall prognosis of patients with Werner syndrome is improving, new opportunities for early diagnosis and treatment intervention are still needed. It has been suggested that the inclusion of the WRN gene in genetic analyses for early-onset diabetes, lipodystrophy, or dyslipidemia may offer an opportunity to diagnose patients with Werner syndrome long before the presentation of the full spectrum of symptoms and complications, enabling earlier interventions, including malignant neoplasm screenings and prevention of diseases listed in the clinical criteria [58]. Recently, novel senescent markers, ATP6V0D1 and RTN4, were shown to be increased in cells derived from patients with Werner syndrome, raising a possibility that they may serve as markers of disease progression [59]. Similarly, ribonuclease H2 subunit A (RNaseH2A) was shown to be downregulated in Werner syndrome cells as well as selected cancer cells [60]. Therefore, it may also be used as a diagnosis and severity marker. It was reported that patients with Werner syndrome have thinning of the retinal nerve fiber layer, ganglion cell complex, and choroidal thickness and the loss of visual field [61]. It may be useful for early diagnosis to have retinal and choroidal check-ups with the optical coherence tomography images when patients present with juvenile cataracts of unknown cause. For early detection of complications, genetic testing for complications, such as malignant neoplasms, may also be useful, when Werner syndrome is diagnosed. Early detection makes it possible to reduce risk factors such as smoking and to do early prevention and treatment.
Regarding renal protection, renin-angiotensin system inhibitors are hard to use, since many patients stopped their usage due to hyperkalemia. Additionally, sodium-glucose cotransporter 2 inhibitors are also difficult to use due to concern of sarcopenia in patients with Werner syndrome. However, a mineralocorticoid receptor antagonist, finerenone, may be a good candidate, since it is less likely to cause hyperkalemia.
Regarding intractable skin ulcers, treatment with a functional peptide SR-0379 was found to be safe, well-tolerated, and effective for leg ulcers in patients with Werner syndrome in clinical trials [62, 63].
Reportedly, p38 inhibitors reduced the accelerated cell senescence in primary fibroblasts from patients with Werner syndrome [64]. It is believed that in the near future, p38 inhibitors may be used in in vivo studies. Nicotinamide adenine dinucleotide (NAD) is important for the activation of sirtuin, a type of protein involved in regulating cellular processes including the aging and death of cells. NAD levels decrease in patients with Werner syndrome [65], therefore supplementation with NAD precursors may be effective. A clinical trial with nicotinamide riboside, a precursor of NAD, which may be effective for intractable ulcers, sarcopenia, and ASCVD, is investigating the safety and efficacy in patients with Werner syndrome [66]. Using state-of-the-art technologies, such as genome, transcriptome, and epigenome analyses [67], study of the generation of iPS cells from patients with Werner syndrome and the correction of the WRN gene by the CRISPR/Cas9-mediated methods [68] will create new treatments for patients with Werner syndrome.
In conclusion, this study clarified secular changes in multiple patients with Werner syndrome. The morbidity due to malignant neoplasms is high even in those of young age; therefore, it is necessary to carry out active and detailed screening examinations for malignant neoplasms. Renal function declines rapidly; therefore, evaluation based on BSA-uncorrected eGFRcre or eGFRcys and attention to the type and amount of drugs used are needed.
Materials and Methods
Werner Syndrome Registry (patient registration system)
To reveal the disease profile and prognosis and to seek suitable medical intervention methods, the Werner Syndrome Registry was established. Based on the results of a nationwide primary survey, the patients were recruited to the registry from facilities with patients definitively diagnosed with Werner syndrome according to the diagnostic criteria [20].
The study complied with the ethical rules for human experimentation as specified in the Declaration of Helsinki. The study received approval from the Ethics Board of Chiba University on 27th July 2016 (approval number: 278) and from the Ethics Board of Kyoto University on 29th January 2020 (approval number: R2370). The study was registered at the UMIN Clinical Trial Registry (https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000034058) on 3rd November 2017 (ID: UMIN000029812). Written informed consent was obtained from patients before registration.
The key inclusion criteria for the registry were as follows: 1) patients with confirmed Werner syndrome based on the diagnostic criteria [20], and 2) patients who provided written informed consent prior to their participation in the registry. There were no exclusion criteria. The registry data included patient background (age at the time of onset, diagnosis, and registration; height, weight, BMI, abdominal circumference, and presence of consanguineous marriage), characteristic major signs and clinical symptoms, comorbidities (diabetes mellitus, impaired glucose tolerance, dyslipidemia, hypertension, fatty liver, cerebrovascular diseases, cardiovascular diseases, peripheral artery disease, foot amputation, and malignant neoplasms), the pattern of gene mutation, blood examination (blood cell count, biochemistry, liver and renal functions, and glucose and lipid profiles), visceral fat area, SMI, physical function (grip strength and walking speed), and treatment content. Renal function was evaluated using the following three indices: eGFRcre, BSA-uncorrected eGFRcre, and eGFRcys.
The calculation formula of each eGFR index was as follows:
(1) eGFRcre (mL/min/1.73 m2)
Male: eGFRcre (mL/min/1.73 m2) = 194 × Cr−1.094 × Age−0.287
Female: eGFRcre (mL/min/1.73 m2) = 194 × Cr−1.094 × Age−0.287 × 0.739
(2) BSA-uncorrected eGFRcre (mL/min) = eGFRcre × (BSA/1.73)
BSA can be calculated using the Du Bois method. BSA (m2) = Height (cm)0.725 × Weight (kg)0.425 × 0.007184.
(3) eGFRcys (mL/min/1.73 m2)
Male: eGFRcys (mL/min/1.73 m2) = {104 × CysC−1.019 × 0.996Age} −8
Female: eGFRcys (mL/min/1.73 m2) = {104 × CysC−1.019 × 0.996Age × 0.929} −8
The datasheets were collected from the facilities annually. The collected data were subsequently inputted into the registration system Fountayn (previously named DATATRACK ONE) (NTT DATA, Tokyo, Japan) [9].
Cross-sectional analysis and longitudinal analysis
The data were extracted on May 12, 2022. Data obtained at the registration time of each patient were analyzed through a cross-sectional analysis study model. For longitudinal analysis of the data in the Werner Syndrome Registry, the data at the time of initial registration and after one, two, and three years were compared in the patients with such data. For continuous variables, the paired t-test was used for items with a normal distribution, and the Wilcoxon signed-rank test was used for items with a non-normal distribution. For binary variables, Pearson’s chi-squared test was used for items with 20 patients and more, and Fisher’s exact test was used for items with less than 20 patients included. All data were analyzed with JMP pro 15 (SAS Institute, Cary, NC, USA). A p-value less than 0.05 was considered statistically significant.
The prevalence of malignant neoplasms and aspiration pneumonia was also investigated for the entire period from registration to three years later. Regarding malignant neoplasms, the presence or absence of malignant neoplasms, categorization of epithelial or non-epithelial neoplasms, and type of neoplasms were investigated.
Moreover, the association between renal function and leg ulcers/NSAIDs was also investigated. The relationship between renal function (eGFRcre, BSA-uncorrected eGFRcre, and eGFRcys) and both the presence or absence of leg ulcers and the use of NSAIDs were investigated using the baseline data.
Author Contributions
MKoshizaka, MS, YMaeda, HKaneko, HKato, YMaezawa, MT, and KYokote managed the project. MKoshizaka, MS, YMaeda, HKato, YM, JK, KYoshinaga, MI, AS, SM, HN, YY, ST, AT, KS, YT, YS, KHashimoto, TYoshimura, AK, DS, NO, TYoshida, KW, MKuzuya, and KYokote recruited the patients and carried out examinations. MKoshizaka, YMaeda and MS analyzed data. YMaeda and MKoshizaka drafted the manuscript. MKoshizaka, YMaeda, MS, HKaneko, HKato, YMaezawa, JO, and KYokote edited and revised the manuscript. KYokote acted as the “principal investigator.” All authors contributed significantly, read, and approved the final manuscript.
Acknowledgments
The authors would like to thank all additional staff, and the patients who participated in the present study.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
The study complied with the ethical rules for human experimentation as specified in the Declaration of Helsinki. The study received approval from the Ethics Board of Chiba University on 27th July 2016 (approval number: 278) and from the Ethics Board of Kyoto University on 29th January 2020 (approval number: R2370). Written informed consent was obtained from patients before registration.
Funding
This work was supported by JSPS KAKENHI Grant Number JP21K19437, JP20H00524, and MHLW Research on rare and intractable diseases Program Grant Number 21FC2001, and AMED under Grant Number 20ek0109353h0003 and 23ek0109622h0001.
References
- 1. Matsumoto T, Imamura O, Yamabe Y, Kuromitsu J, Tokutake Y, Shimamoto A, Suzuki N, Satoh M, Kitao S, Ichikawa K, Kataoka H, Sugawara K, Thomas W, et al. Mutation and haplotype analyses of the Werner's syndrome gene based on its genomic structure: genetic epidemiology in the Japanese population. Hum Genet. 1997; 100:123–30. https://doi.org/10.1007/s004390050477 [PubMed]
- 2. Satoh M, Imai M, Sugimoto M, Goto M, Furuichi Y. Prevalence of Werner's syndrome heterozygotes in Japan. Lancet. 1999; 353:1766. https://doi.org/10.1016/S0140-6736(98)05869-3 [PubMed]
- 3. Yokote K, Chanprasert S, Lee L, Eirich K, Takemoto M, Watanabe A, Koizumi N, Lessel D, Mori T, Hisama FM, Ladd PD, Angle B, Baris H, et al. WRN Mutation Update: Mutation Spectrum, Patient Registries, and Translational Prospects. Hum Mutat. 2017; 38:7–15. https://doi.org/10.1002/humu.23128 [PubMed]
- 4. Yamaga M, Takemoto M, Takada-Watanabe A, Koizumi N, Kitamoto T, Sakamoto K, Ishikawa T, Koshizaka M, Maezawa Y, Yokote K. Recent Trends in WRN Gene Mutation Patterns in Individuals with Werner Syndrome. J Am Geriatr Soc. 2017; 65:1853–6. https://doi.org/10.1111/jgs.14906 [PubMed]
- 5. Goto M, Matsuura M. Secular trends towards delayed onsets of pathologies and prolonged longevities in Japanese patients with Werner syndrome. Biosci Trends. 2008; 2:81–7. [PubMed]
- 6. Goto M. Hierarchical deterioration of body systems in Werner's syndrome: implications for normal ageing. Mech Ageing Dev. 1997; 98:239–54. https://doi.org/10.1016/s0047-6374(97)00111-5 [PubMed]
- 7. Kato H, Koshizaka M, Kaneko H, Maezawa Y, Yokote K. Lifetime extension and the recent cause of death in Werner syndrome: a retrospective study from 2011 to 2020. Orphanet J Rare Dis. 2022; 17:226. https://doi.org/10.1186/s13023-022-02383-w [PubMed]
- 8. Kitagawa Y, Amemiya A, Ogata H, Koshizaka M, Shoji M, Maezawa Y, Akita S, Mitsukawa N, Yokote K. Quality of life in Werner syndrome and associated subjective foot/ankle symptoms: A cross-sectional survey. Geriatr Gerontol Int. 2023; 23:188–93. https://doi.org/10.1111/ggi.14541 [PubMed]
- 9. Koshizaka M, Maezawa Y, Maeda Y, Shoji M, Kato H, Kaneko H, Ishikawa T, Kinoshita D, Kobayashi K, Kawashima J, Sekiguchi A, Motegi SI, Nakagami H, et al. Time gap between the onset and diagnosis in Werner syndrome: a nationwide survey and the 2020 registry in Japan. Aging (Albany NY). 2020; 12:24940–56. https://doi.org/10.18632/aging.202441 [PubMed]
- 10. e-Stat, Statistics of Japan. https://www.e-stat.go.jp/dbview?sid=0003224177&scid=wi_mny_topic_article_2112_00001_43407_02.
- 11. e-Stat, Statistics of Japan. https://www.e-stat.go.jp/dbview?sid=0003224178.
- 12. Nishihara G, Nakamoto M, Yasunaga C, Takeda K, Matsuo K, Urabe M, Goya T, Sakemi T. End-stage renal disease in a patient with Werner's syndrome. Nephron. 1997; 76:360. https://doi.org/10.1159/000190208 [PubMed]
- 13. Kawamura H, Tsuchida H, Maezawa Y, Kobayashi K, Fujimoto M, Asaumi S, Yokote K, Mori S, Saito Y. [A report of a case with Werner's syndrome suffering from end-stage renal failure]. Nihon Ronen Igakkai Zasshi. 2003; 40:282–6. https://doi.org/10.3143/geriatrics.40.282 [PubMed]
- 14. Kocabay G, Ozturk S, Ecder T. Werner syndrome associated with renal involvement. Saudi Med J. 2006; 27:1768–9. [PubMed]
- 15. Granata A, Floccari F, Mignani R, Gallieni M. Glomerular membranous nephropathy and Werner syndrome: a case report. J Am Geriatr Soc. 2011; 59:1749–50. https://doi.org/10.1111/j.1532-5415.2011.03578.x [PubMed]
- 16. Kubota Y, Takemoto M, Taniguchi T, Motegi SI, Taniguchi A, Nakagami H, Maezawa Y, Koshizaka M, Kato H, Mori S, Tsukamoto K, Kuzuya M, Yokote K. Management guideline for Werner syndrome 2020. 6. Skin ulcers associated with Werner syndrome: Prevention and non-surgical and surgical treatment. Geriatr Gerontol Int. 2021; 21:153–9. https://doi.org/10.1111/ggi.14096 [PubMed]
- 17. Motegi SI, Takemoto M, Taniguchi T, Kubota Y, Taniguchi A, Nakagami H, Maezawa Y, Koshizaka M, Kato H, Mori S, Tsukamoto K, Kuzuya M, Yokote K. Management guideline for Werner syndrome 2020. 7. Skin ulcer associated with Werner syndrome: Dermatological treatment. Geriatr Gerontol Int. 2021; 21:160–2. https://doi.org/10.1111/ggi.14077 [PubMed]
- 18. Kuzuya M, Takemoto M, Kubota Y, Taniguchi T, Motegi SI, Taniguchi A, Nakagami H, Maezawa Y, Koshizaka M, Kato H, Mori S, Tsukamoto K, Yokote K. Management guideline for Werner syndrome 2020. 2. Sarcopenia associated with Werner syndrome. Geriatr Gerontol Int. 2021; 21:139–41. https://doi.org/10.1111/ggi.14076 [PubMed]
- 19. Onishi S, Takemoto M, Ishikawa T, Okabe E, Ishibashi R, He P, Kobayashi K, Fujimoto M, Kawamura H, Yokote K. Japanese diabetic patients with Werner syndrome exhibit high incidence of cancer. Acta Diabetol. 2012 (Suppl 1); 49:S259–60. https://doi.org/10.1007/s00592-012-0424-z [PubMed]
- 20. Takemoto M, Mori S, Kuzuya M, Yoshimoto S, Shimamoto A, Igarashi M, Tanaka Y, Miki T, Yokote K. Diagnostic criteria for Werner syndrome based on Japanese nationwide epidemiological survey. Geriatr Gerontol Int. 2013; 13:475–81. https://doi.org/10.1111/j.1447-0594.2012.00913.x [PubMed]
- 21. Lauper JM, Monnat RJ
Jr . Diabetes mellitus and cancer in Werner syndrome. Acta Diabetol. 2014; 51:159–61. https://doi.org/10.1007/s00592-013-0456-z [PubMed] - 22. Goto M. Werner's syndrome: from clinics to genetics. Clin Exp Rheumatol. 2000; 18:760–6. [PubMed]
- 23. Foundation for Promotion of Cancer Research. Cancer statistics in Japan-2022. https://ganjoho.jp/public/qa_links/report/statistics/pdf/cancer_statistics_2022.pdff.
- 24. Goto M, Miller RW, Ishikawa Y, Sugano H. Excess of rare cancers in Werner syndrome (adult progeria). Cancer Epidemiol Biomarkers Prev. 1996; 5:239–46. [PubMed]
- 25. Lauper JM, Krause A, Vaughan TL, Monnat RJ
Jr . Spectrum and risk of neoplasia in Werner syndrome: a systematic review. PLoS One. 2013; 8:e59709. https://doi.org/10.1371/journal.pone.0059709 [PubMed] - 26. Awni BM, Holanda Lopes CD, Harada G, Salgues ACR, França GA, Testagrossa LA, Queiroz MA, Gonçalves E Silva A, Ferreira FO, Munhoz RR. Exacerbated Renal and Hematologic Toxicities to Ifosfamide and Doxorubicin-Based Chemotherapy in a Patient with Retroperitoneal Liposarcoma Harboring a Germline Mutation in the WRN Gene. Case Rep Oncol. 2022; 15:170–5. https://doi.org/10.1159/000521624 [PubMed]
- 27. Lohynská R, Pechačová Z, Mazaná E, Čejková J, Nováková-Jirešová A, Hornová J, Langová M. Radiotherapy and radiosensitivity syndromes in DNA repair gene mutations. Klin Onkol. 2022; 35:119–27. https://doi.org/10.48095/ccko2022119 [PubMed]
- 28. Akcora-Yildiz D, Ozkan T, Ozen M, Gunduz M, Sunguroglu A, Beksac M. Werner helicase is required for proliferation and DNA damage repair in multiple myeloma. Mol Biol Rep. 2023; 50:1565–73. https://doi.org/10.1007/s11033-022-08178-3 [PubMed]
- 29. Kato H, Maezawa Y, Nishijima D, Iwamoto E, Takeda J, Kanamori T, Yamaga M, Mishina T, Takeda Y, Izumi S, Hino Y, Nishi H, Ishiko J, et al. A high prevalence of myeloid malignancies in progeria with Werner syndrome is associated with p53 insufficiency. Exp Hematol. 2022; 109:11–7. https://doi.org/10.1016/j.exphem.2022.02.005 [PubMed]
- 30. Sobol RW. WRN suppresses p53/PUMA-induced apoptosis in colorectal cancer with microsatellite instability/mismatch repair deficiency. Proc Natl Acad Sci U S A. 2023; 120:e2219963120. https://doi.org/10.1073/pnas.2219963120 [PubMed]
- 31. Datta A, Biswas K, Sommers JA, Thompson H, Awate S, Nicolae CM, Thakar T, Moldovan GL, Shoemaker RH, Sharan SK, Brosh RM
Jr . WRN helicase safeguards deprotected replication forks in BRCA2-mutated cancer cells. Nat Commun. 2021; 12:6561. https://doi.org/10.1038/s41467-021-26811-w [PubMed] - 32. Datta A, Brosh RM
Jr . WRN rescues replication forks compromised by a BRCA2 deficiency: Predictions for how inhibition of a helicase that suppresses premature aging tilts the balance to fork demise and chromosomal instability in cancer. Bioessays. 2022; 44:e2200057. https://doi.org/10.1002/bies.202200057 [PubMed] - 33. Tsuge K, Shimamoto A. Research on Werner Syndrome: Trends from Past to Present and Future Prospects. Genes (Basel). 2022; 13:1802. https://doi.org/10.3390/genes13101802 [PubMed]
- 34. Kategaya L, Perumal SK, Hager JH, Belmont LD. Werner Syndrome Helicase Is Required for the Survival of Cancer Cells with Microsatellite Instability. iScience. 2019; 13:488–97. https://doi.org/10.1016/j.isci.2019.02.006 [PubMed]
- 35. Lieb S, Blaha-Ostermann S, Kamper E, Rippka J, Schwarz C, Ehrenhöfer-Wölfer K, Schlattl A, Wernitznig A, Lipp JJ, Nagasaka K, van der Lelij P, Bader G, Koi M, et al. Werner syndrome helicase is a selective vulnerability of microsatellite instability-high tumor cells. Elife. 2019; 8:e43333. https://doi.org/10.7554/eLife.43333 [PubMed]
- 36. van Wietmarschen N, Sridharan S, Nathan WJ, Tubbs A, Chan EM, Callen E, Wu W, Belinky F, Tripathi V, Wong N, Foster K, Noorbakhsh J, Garimella K, et al. Repeat expansions confer WRN dependence in microsatellite-unstable cancers. Nature. 2020; 586:292–8. https://doi.org/10.1038/s41586-020-2769-8 [PubMed]
- 37. Chan EM, Shibue T, McFarland JM, Gaeta B, Ghandi M, Dumont N, Gonzalez A, McPartlan JS, Li T, Zhang Y, Bin Liu J, Lazaro JB, Gu P, et al. WRN helicase is a synthetic lethal target in microsatellite unstable cancers. Nature. 2019; 568:551–6. https://doi.org/10.1038/s41586-019-1102-x [PubMed]
- 38. Behan FM, Iorio F, Picco G, Gonçalves E, Beaver CM, Migliardi G, Santos R, Rao Y, Sassi F, Pinnelli M, Ansari R, Harper S, Jackson DA, et al. Prioritization of cancer therapeutic targets using CRISPR-Cas9 screens. Nature. 2019; 568:511–6. https://doi.org/10.1038/s41586-019-1103-9 [PubMed]
- 39. Aggarwal M, Sommers JA, Shoemaker RH, Brosh RM
Jr . Inhibition of helicase activity by a small molecule impairs Werner syndrome helicase (WRN) function in the cellular response to DNA damage or replication stress. Proc Natl Acad Sci U S A. 2011; 108:1525–30. https://doi.org/10.1073/pnas.1006423108 [PubMed] - 40. Aggarwal M, Banerjee T, Sommers JA, Brosh RM
Jr . Targeting an Achilles' heel of cancer with a WRN helicase inhibitor. Cell Cycle. 2013; 12:3329–35. https://doi.org/10.4161/cc.26320 [PubMed] - 41. Kusunoki H, Tsuji S, Kusukawa T, Wada Y, Tamaki K, Nagai K, Itoh M, Sano K, Amano M, Maeda H, Sugita H, Hasegawa Y, Kishimoto H, et al. Relationships between cystatin C- and creatinine-based eGFR in Japanese rural community- dwelling older adults with sarcopenia. Clin Exp Nephrol. 2021; 25:231–9. https://doi.org/10.1007/s10157-020-01981-x [PubMed]
- 42. Shlipak MG, Matsushita K, Ärnlöv J, Inker LA, Katz R, Polkinghorne KR, Rothenbacher D, Sarnak MJ, Astor BC, Coresh J, Levey AS, Gansevoort RT, and CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013; 369:932–43. https://doi.org/10.1056/NEJMoa1214234 [PubMed]
- 43. Lin YL, Chang IC, Liou HH, Wang CH, Lai YH, Kuo CH, Hsu BG. Serum indices based on creatinine and cystatin C predict mortality in patients with non-dialysis chronic kidney disease. Sci Rep. 2021; 11:16863. https://doi.org/10.1038/s41598-021-96447-9 [PubMed]
- 44. Imai E, Horio M, Yamagata K, Iseki K, Hara S, Ura N, Kiyohara Y, Makino H, Hishida A, Matsuo S. Slower decline of glomerular filtration rate in the Japanese general population: a longitudinal 10-year follow-up study. Hypertens Res. 2008; 31:433–41. https://doi.org/10.1291/hypres.31.433 [PubMed]
- 45. Kaur A, Grover P, Albawaliz A, Chauhan M, Barthel B. Growing Old Too Fast: A Rare Case of Werner Syndrome. Cureus. 2019; 11:e4743. https://doi.org/10.7759/cureus.4743 [PubMed]
- 46. Handa K, Fukui S, Shirakawa Y, Sakamoto T, Kitahara M, Kakizawa Y, Nishi H. Aortic valve replacement with annular patch enlargement for a patient with Werner's syndrome and severe aortic stenosis. J Cardiothorac Surg. 2020; 15:174. https://doi.org/10.1186/s13019-020-01219-7 [PubMed]
- 47. Masada K, Kuratani T, Maeda K, Torikai K, Sawa Y. Transcatheter aortic valve replacement in a patient with Werner syndrome. J Card Surg. 2017; 32:414–5. https://doi.org/10.1111/jocs.13164 [PubMed]
- 48. Yamamoto M, Yamamoto E, Yasuda O, Yasuda H, Sakamoto K, Tsujita K, Izumiya Y, Kaikita K, Hokimoto S, Ogawa H. A case of Werner's syndrome with cardiac syndrome X and heart failure with preserved ejection fraction. J Cardiol Cases. 2015; 12:195–8. https://doi.org/10.1016/j.jccase.2015.08.009 [PubMed]
- 49. Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, Jang HC, Kang L, Kim M, Kim S, Kojima T, Kuzuya M, Lee JSW, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc. 2020; 21:300–7.e2. https://doi.org/10.1016/j.jamda.2019.12.012 [PubMed]
- 50. Yamaga M, Takemoto M, Shoji M, Sakamoto K, Yamamoto M, Ishikawa T, Koshizaka M, Maezawa Y, Kobayashi K, Yokote K. Werner syndrome: a model for sarcopenia due to accelerated aging. Aging (Albany NY). 2017; 9:1738–44. https://doi.org/10.18632/aging.101265 [PubMed]
- 51. Kato H, Maezawa Y, Takayama N, Ouchi Y, Kaneko H, Kinoshita D, Takada-Watanabe A, Oshima M, Koshizaka M, Ogata H, Kubota Y, Mitsukawa N, Eto K, et al. Fibroblasts from different body parts exhibit distinct phenotypes in adult progeria Werner syndrome. Aging (Albany NY). 2021; 13:4946–61. https://doi.org/10.18632/aging.202696 [PubMed]
- 52. Borack MS, Volpi E. Efficacy and Safety of Leucine Supplementation in the Elderly. J Nutr. 2016; 146:2625S–9S. https://doi.org/10.3945/jn.116.230771 [PubMed]
- 53. Martínez-Arnau FM, Fonfría-Vivas R, Buigues C, Castillo Y, Molina P, Hoogland AJ, van Doesburg F, Pruimboom L, Fernández-Garrido J, Cauli O. Effects of Leucine Administration in Sarcopenia: A Randomized and Placebo-controlled Clinical Trial. Nutrients. 2020; 12:932. https://doi.org/10.3390/nu12040932 [PubMed]
- 54. Grgic J, Garofolini A, Orazem J, Sabol F, Schoenfeld BJ, Pedisic Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2020; 50:1983–99. https://doi.org/10.1007/s40279-020-01331-7 [PubMed]
- 55. Mayer F, Scharhag-Rosenberger F, Carlsohn A, Cassel M, Müller S, Scharhag J. The intensity and effects of strength training in the elderly. Dtsch Arztebl Int. 2011; 108:359–64. https://doi.org/10.3238/arztebl.2011.0359 [PubMed]
- 56. Katakami N, Uchino J, Yokoyama T, Naito T, Kondo M, Yamada K, Kitajima H, Yoshimori K, Sato K, Saito H, Aoe K, Tsuji T, Takiguchi Y, et al. Anamorelin (ONO-7643) for the treatment of patients with non-small cell lung cancer and cachexia: Results from a randomized, double-blind, placebo-controlled, multicenter study of Japanese patients (ONO-7643-04). Cancer. 2018; 124:606–16. https://doi.org/10.1002/cncr.31128 [PubMed]
- 57. Hamauchi S, Furuse J, Takano T, Munemoto Y, Furuya K, Baba H, Takeuchi M, Choda Y, Higashiguchi T, Naito T, Muro K, Takayama K, Oyama S, et al. A multicenter, open-label, single-arm study of anamorelin (ONO-7643) in advanced gastrointestinal cancer patients with cancer cachexia. Cancer. 2019; 125:4294–302. https://doi.org/10.1002/cncr.32406 [PubMed]
- 58. Atallah I, McCormick D, Good JM, Barigou M, Fraga M, Sempoux C, Superti-Furga A, Semple RK, Tran C. Partial lipodystrophy, severe dyslipidaemia and insulin resistant diabetes as early signs of Werner syndrome. J Clin Lipidol. 2022; 16:583–90. https://doi.org/10.1016/j.jacl.2022.06.004 [PubMed]
- 59. Misawa T, Hitomi K, Miyata K, Tanaka Y, Fujii R, Chiba M, Loo TM, Hanyu A, Kawasaki H, Kato H, Maezawa Y, Yokote K, Nakamura AJ, et al. Identification of Novel Senescent Markers in Small Extracellular Vesicles. Int J Mol Sci. 2023; 24:2421. https://doi.org/10.3390/ijms24032421 [PubMed]
- 60. Sugawara S, Okada R, Loo TM, Tanaka H, Miyata K, Chiba M, Kawasaki H, Katoh K, Kaji S, Maezawa Y, Yokote K, Nakayama M, Oshima M, et al. RNaseH2A downregulation drives inflammatory gene expression via genomic DNA fragmentation in senescent and cancer cells. Commun Biol. 2022; 5:1420. https://doi.org/10.1038/s42003-022-04369-7 [PubMed]
- 61. Nagai T, Yokouchi H, Miura G, Koshizaka M, Maezawa Y, Oshitari T, Yokote K, Baba T. Optical coherence tomography findings in three patients with Werner syndrome. BMC Ophthalmol. 2022; 22:448. https://doi.org/10.1186/s12886-022-02660-z [PubMed]
- 62. Nakagami H, Sugimoto K, Ishikawa T, Fujimoto T, Yamaoka T, Hayashi M, Kiyohara E, Ando H, Terabe Y, Takami Y, Yamamoto K, Takeya Y, Takemoto M, et al. Physician-initiated clinical study of limb ulcers treated with a functional peptide, SR-0379: from discovery to a randomized, double-blind, placebo-controlled trial. NPJ Aging Mech Dis. 2018; 4:2. https://doi.org/10.1038/s41514-018-0021-7 [PubMed]
- 63. Nakagami H, Sugimoto K, Ishikawa T, Koshizaka M, Fujimoto T, Kiyohara E, Hayashi M, Nakagawa Y, Ando H, Terabe Y, Takami Y, Yamamoto K, Takeya Y, et al. Investigator-initiated clinical study of a functional peptide, SR-0379, for limb ulcers of patients with Werner syndrome as a pilot study. Geriatr Gerontol Int. 2019; 19:1118–23. https://doi.org/10.1111/ggi.13782 [PubMed]
- 64. Davis T, Brook AJ, Rokicki MJ, Bagley MC, Kipling D. Evaluating the Role of p38 MAPK in the Accelerated Cell Senescence of Werner Syndrome Fibroblasts. Pharmaceuticals (Basel). 2016; 9:23. https://doi.org/10.3390/ph9020023 [PubMed]
- 65. Fang EF, Hou Y, Lautrup S, Jensen MB, Yang B, SenGupta T, Caponio D, Khezri R, Demarest TG, Aman Y, Figueroa D, Morevati M, Lee HJ, et al. NAD(+) augmentation restores mitophagy and limits accelerated aging in Werner syndrome. Nat Commun. 2019; 10:5284. https://doi.org/10.1038/s41467-019-13172-8 [PubMed]
- 66. Prospective, single-center, cross-over trial to verify safety and effectiveness of nicotinamide riboside for patients with Werner syndrome (EMPOWER). https://jrct.niph.go.jp/en-latest-detail/jRCTs031190141. .
- 67. Kato H, Maezawa Y. Atherosclerosis and Cardiovascular Diseases in Progeroid Syndromes. J Atheroscler Thromb. 2022; 29:439–47. https://doi.org/10.5551/jat.RV17061 [PubMed]
- 68. Kato H, Maezawa Y, Ouchi Y, Takayama N, Sone M, Sone K, Takada-Watanabe A, Tsujimura K, Koshizaka M, Nagasawa S, Saitoh H, Ohtaka M, Nakanishi M, et al. Generation of disease-specific and CRISPR/Cas9-mediated gene-corrected iPS cells from a patient with adult progeria Werner syndrome. Stem Cell Res. 2021; 53:102360. https://doi.org/10.1016/j.scr.2021.102360 [PubMed]