



Introduction
Lung cancer is a major global health problem and remains the leading cause of cancer-related mortality worldwide [1]. Most cases of lung cancer fall into one of two categories: either non-small cell lung cancer (NSCLC), which makes up 85 percent of all lung cancers, or small cell lung cancer (SCLC), which accounts for 15 percent [2]. Approximately 35,000 new cases of SCLC are identified each year, with the vast majority of patients being male [1]. Nearly 40% of all cases of SCLC are classified as limited-stage SCLC (LS-SCLC). SCLC is distinguished by its rapid progression and early onset of widespread metastases, both of which are associated with poor clinical outcomes. In this population, the disease’s estimated 5-year overall survival rate is less than 10% [3]. Those diagnosed with SCLC have a median survival time of 16–24 months [4]. Few advancements have been made in recent decades to enhance the survival rate of SCLC patients. Multimodal treatments, including surgery, chemotherapy, and radiotherapy, remains the standard management for treating this disease. Despite an early responsiveness to chemotherapy, most patients quickly develop therapy resistance, which leads to relapse and ultimately death [5]. Moreover, the surgical role in the treatment of SCLC is currently regarded as being very limited.
At the time of initial diagnosis, approximately 30% of patients with small cell lung cancer have no evidence of metastasis [6]. High rates of lung cancer mortality are often attributable to distant metastases, which occur in the vast majority of patients with SCLC [7]. Metastasis from SCLC is common in many organs, but the brain, bone, adrenals, liver, and lungs are particularly vulnerable targets [8]. For patients with SCLC, the brain is a favorable site for the disease to fail [9]. The possible reason is that most chemotherapeutic drugs are unable to reach the brain because of the blood-brain barrier [10]. Within the first two years after being diagnosed with SCLC, up to fifty percent of patients are at risk of developing brain metastases (BM) [11]. Due to SCLC’s radiosensitivity, whole brain radiotherapy has become the treatment of choice for patients with brain metastases [12]. For such patients, in addition to whole brain radiotherapy and conventional chemotherapy, there are various treatment methods, but the curative effect of these options is not ideal. In patients with brain metastases, early detection and intervention could improve clinical outcomes. Therefore, early identification of risk factors for brain metastasis in SCLC is crucial. The nomogram model integrates critical clinical and pathological features of the tumor and presents them in an intuitive graphical format, giving patients a personalized evidence-based risk assessment and assisting clinicians in choosing the best treatments. As a result, it is regarded as a trustworthy tool for visualizing and evaluating risk. To make metastatic screening easier, there is an urgent need for a predictive nomogram based on the clinicopathologic characteristics of SCLC patients.
To the best of our knowledge, there are few studies on the risk factors for brain metastasis in LS-SCLC. It is still unclear how to distinguish between patients’ risks of developing brain metastasis in LS-SCLC. LS-SCLC patients typically present in stage III [13]. Since most SCLC patients are male and at stage III, we present the first study to examine the risk factors for brain metastasis in male SCLC patients with stage III. There is no relevant prediction model has particularly been constructed to predict BM for this subgroup population till date. It represents the first attempt to develop prediction model for this specific population segment. The purpose of this research was to develop a predicted model for brain metastasis in male SCLC patients with stage III and helped in the early identification of high-risk patients and the selection of individualized therapies. This study offers theoretical direction for clinical individualization treatment in LS-SCLC.
Results
Baseline characteristics of the study cohort
Overall, 112 male SCLC patients at stage III treated with chemotherapy and radiotherapy were enrolled in our study. The clinicopathologic characteristics, demographics, and therapeutic information were shown in Table 1. Patients’ age, tumor location, smoke, concurrent chemoradiotherapy (CCRT), cycle of chemotherapy before radiotherapy, total cycle of chemotherapy, RT dose, radiotherapy time, PNI, PAR, PLR, NLR, LLR, dNLR, SII, and SIRI were collected. The optimal cut-off value for age, radiotherapy time, PNI, PAR, PLR, NLR, LLR, dNLR, SII, and SIRI was calculated to be 66, 26, 45.15, 4.03, 162.81, 2.2, 4.32, 1.69, 815.1, and 0.27, respectively. The median and average age at diagnosis was 60 years and 59 years, respectively. The majority of patients (83%) less than 66 years. Of 112 patients in the study, 61.6% had a history of smoke. During the follow-up period, of 112 patients treated with CRT, twenty-eight (25%) patients developed BM.
Table 1. Patient demographics and clinical characteristics.
| Clinicopathologic variable | Total (N) | Percentage (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <66 | 93 | 83.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥66 | 19 | 17.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor location | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left | 44 | 39.3% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Right | 68 | 60.7% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoke | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 69 | 61.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 43 | 38.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CCRT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 52 | 46.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 60 | 53.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cycle of chemotherapy before radiotherapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1–2 | 54 | 48.2% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 58 | 51.8% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total cycle of chemotherapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4–6 | 69 | 61.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 43 | 38.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RT dose (Gy) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <60 | 72 | 64.3% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥60 | 40 | 35.7% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiotherapy time (day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <26 | 9 | 8.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥26 | 103 | 92.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Targeted therapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 17 | 15.2% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 95 | 84.8% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PNI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <45.15 | 18 | 16.1% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥45.15 | 94 | 83.9% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <4.03 | 21 | 18.8% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥4.03 | 91 | 81.3% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <162.81 | 88 | 78.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥162.81 | 24 | 21.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <2.2 | 73 | 65.2% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥2.2 | 39 | 34.8% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <4.32 | 89 | 79.5% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥4.32 | 23 | 20.5% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| dNLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <1.69 | 34 | 30.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥1.69 | 78 | 69.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SII | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <815.1 | 93 | 83.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥815.1 | 19 | 17.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SIRI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <0.27 | 24 | 21.4% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥0.27 | 88 | 78.6% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brain metastases | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 28 | 25.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 84 | 75.0% | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CCRT: concurrent chemoradiotherapy; RT: radiotherapy; PNI: prognostic-nutrition index; PAR: platelet-albumin ratio; PLR: platelet-lymphocyte ratio; NLR: neutrophil-lymphocyte ratio; LLR: leukocyte-lymphocyte ratio; dNLR: derived neutrophil-lymphocyte ratio; SII: systemic immune-inflammation index; SIRI: systemic inflammation response index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Univariate and multivariate analysis of BM in LS-SCLC
Univariate and multivariate logic regression analysis were used to identify independent predictors of BM of LS-SCLC. Univariate regression analysis showed that the CCRT (p = 0.011; odds ratio (OR), 0.289; 95% confidence interval (CI), 0.111–0.752), RT dose (p = 0.008; OR, 0.300; 95% CI, 0.124–0.727), PNI (p = 0.002; OR, 0.189; 95% CI, 0.065–0.548), LLR (p = 0.025; OR, 3.034; 95% CI, 1.147–8.030), and dNLR (p = 0.011; OR, 0.313; 95% CI, 0.128–0.765) were the significant factors for a higher incidence of BM. Multivariate regression analysis further included the factors of a p < 0.05 in univariate regression analysis. Multivariate analysis showed that CCRT (p = 0.017; OR, 0.272; 95% CI, 0.093–0.795), RT dose (p = 0.011; OR, 0.262; 95% CI, 0.093–0.739), and PNI (p = 0.009; OR, 0.186; 95% CI, 0.052–0.657) were independent risk factors of BM and were included in the nomogram model. Table 2 revealed the results of univariate and multivariate analysis to identify the risk factors of BM for LS-SCLC.
Table 2. Univariable and multivariable logistic regression for analyzing the risk factors for developing BM in LS-SCLC patients.
| Clinicopathologic parameters | Univariate analysis | Multivariate analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| OR | 95% CI | p | OR | 95% CI | p | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥66 vs. <66 | 0.510 | 0.137–1.901 | 0.316 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor location | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Left vs. Right | 0.663 | 0.269–1.638 | 0.373 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoke | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes vs. No | 1.165 | 0.479–2.832 | 0.737 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CCRT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes vs. No | 0.289 | 0.111–0.752 | 0.011 | 0.272 | 0.093–0.795 | 0.017 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cycle of chemotherapy before radiotherapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1–2 vs. other | 0.750 | 0.317–1.776 | 0.513 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Total cycle of chemotherapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4–6 vs. other | 0.527 | 0.222–1.254 | 0.148 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| RT dose (Gy) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥60 vs. <60 | 0.300 | 0.124–0.727 | 0.008 | 0.262 | 0.093–0.739 | 0.011 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Radiotherapy time (day) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <26 vs. ≥26 | 0.352 | 0.042–2.945 | 0.335 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Targeted therapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes vs. No | 0.910 | 0.271–3.060 | 0.879 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PNI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥45.15 vs. <45.15 | 0.189 | 0.065–0.548 | 0.002 | 0.186 | 0.052–0.657 | 0.009 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PAR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥4.03 vs. <4.03 | 0.600 | 0.214–1.681 | 0.331 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥162.81 vs. <162.81 | 2.179 | 0.826–5.748 | 0.116 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| NLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥2.2 vs. <2.2 | 2.360 | 0.983–5.668 | 0.055 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| LLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <4.32 vs. ≥4.32 | 3.034 | 1.147–8.030 | 0.025 | 0.640 | 0.112–3.653 | 0.615 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| dNLR | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <1.69 vs. ≥1.69 | 0.313 | 0.128–0.765 | 0.011 | 0.358 | 0.075–1.717 | 0.199 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SII | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <815.1 vs. ≥815.1 | 0.377 | 0.134–1.062 | 0.065 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SIRI | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| <0.27 vs. ≥0.27 | 1.700 | 0.635–4.549 | 0.291 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: BM: brain metastases; LS-SCLC: limited-stage small cell lung cancer; OR: odds ratio; CI: confidence interval; CCRT: concurrent chemoradiotherapy; RT: radiotherapy; PNI: prognostic-nutrition index; PAR: platelet-albumin ratio; PLR: platelet-lymphocyte ratio; NLR: neutrophil-lymphocyte ratio; LLR: leukocyte-lymphocyte ratio; dNLR: derived neutrophil-lymphocyte ratio; SII: systemic immune-inflammation index; SIRI: systemic inflammation response index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Establishment and verification of predictive nomogram model
To further identify the predicted values of risk factors in the multivariable logistic regression model, we developed nomograms to predict the BM of LS-SCLC patients. The ROC curves of CCRT, RT dose, PNI, and the complex (CCRT, RT dose, and PNI) were shown in Figure 1. The ROC curves revealed the area under the ROC (AUC) of the model was 0.764 (95% CI, 0.658–0.869), which was much higher than individual variable alone (CCRT: 0.643, 95% CI: 0.528–0.758; RT dose: 0.643, 95% CI: 0.521–0.764; PNI: 0.631, 95% CI: 0.502–0.759). The prediction nomogram model for BM was conducted and shown in Figure 2A. An individual’s final score is determined by adding up the points from each factor in the nomogram based on the relative importance of those factors. The calibration curve revealed favorable consistency between the observed probability and predicted probability for brain metastases for LS-SCLC patients (Figure 2B). The C-index for the prediction nomogram was 0.764 (95% CI: 0.658–0.869), which suggested the model’s good discrimination. In addition, the DCA was generated to determine the clinical benefit and practicality of this nomogram. As a result, the DCA demonstrated that the nomogram provides a satisfactory positive net benefit across the majority of threshold probabilities (Figure 2C). The DCA indicated that LS-SCLC patients could benefit from using the nomogram to predict BM probability.
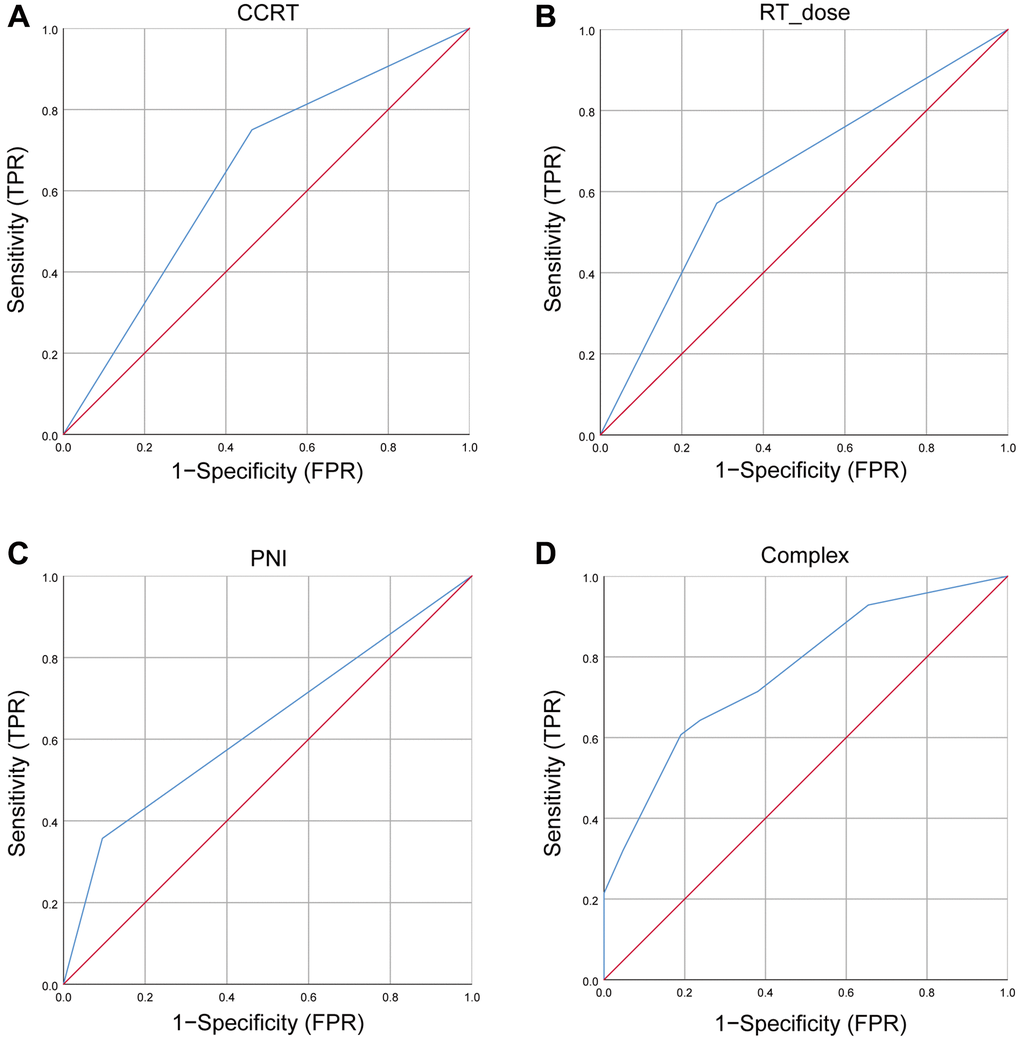
Figure 1. The ROC curves for BM. (A) The ROC curves of CCRT; (B) The ROC curves of RT dose; (C) The ROC curves of PNI; (D) The ROC curves of complex (CCRT, RT dose, and PNI). Abbreviations: ROC: receiver operating characteristic; BM: brain metastases; CCRT: concurrent chemoradiotherapy; RT: radiotherapy; PNI: prognostic-nutrition index; FPR: false positive rate; TPR: true positive rate.
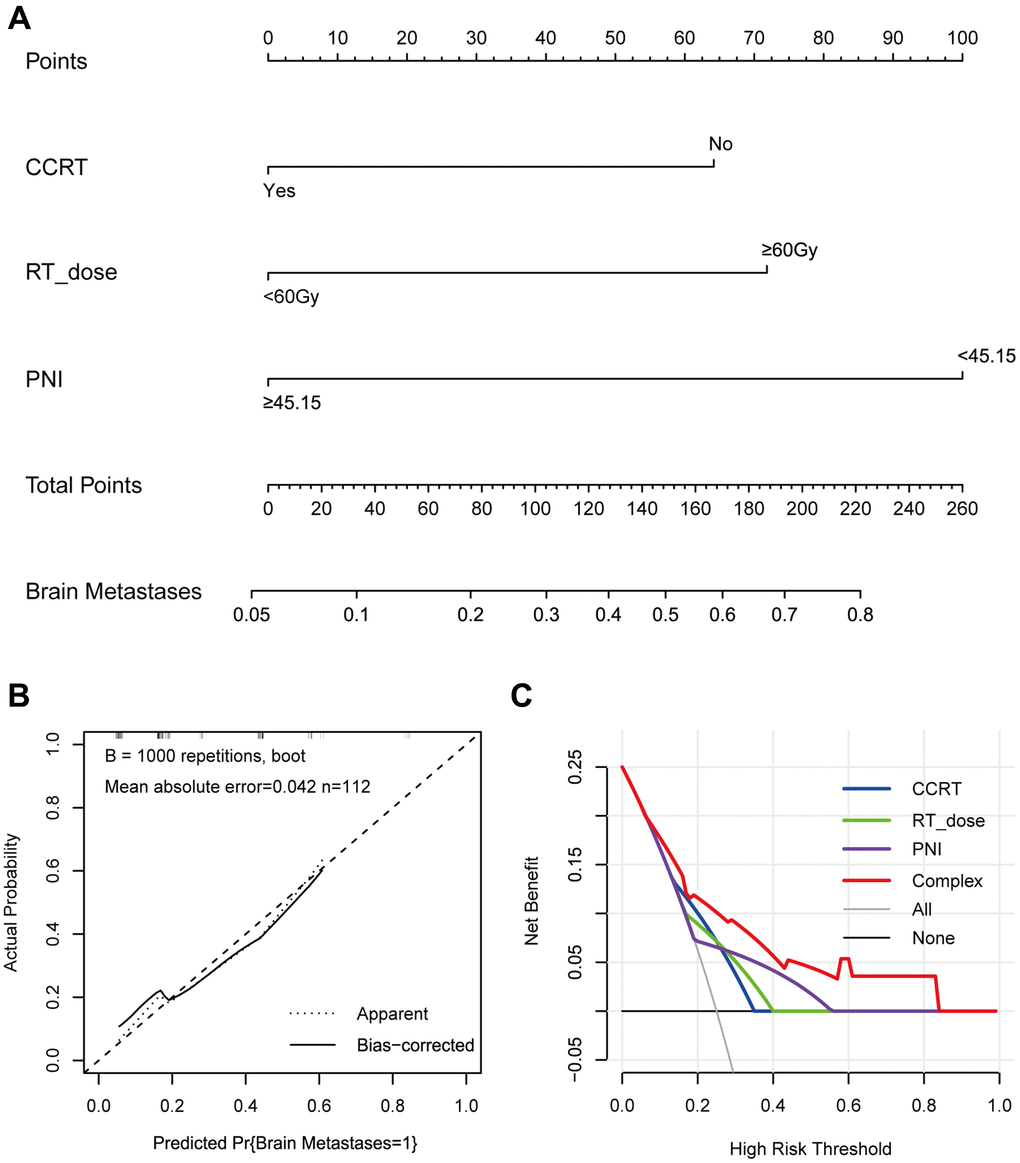
Figure 2. The nomogram, calibration curve, and decision curve for predicting the probability of BM for the whole study population. (A) A nomogram that integrates CCRT, RT dose, and PNI in LS-SCLC patients; (B) The calibration curve of the nomogram predicting the incidence of BM; (C) The decision curves of the nomogram predicting the incidence of BM. Abbreviations: BM: brain metastases; CCRT: concurrent chemoradiotherapy; RT: radiotherapy; PNI: prognostic-nutrition index; LS-SCLC: limited-stage small cell lung cancer.
Correlation between nutritional index and inflammatory index
We next performed Spearman correlation to explore the correlation between PNI, PLR, NLR, LLR, and dNLR. Spearman’s analyses revealed a negative correlation between PNI and PLR (R = −0.356, p < 0.001), PNI and NLR (R = −0.323, p < 0.001), PNI and LLR (R = −0.323, p < 0.001), PNI and dNLR (R = −0.302, p < 0.001) (Figure 3).
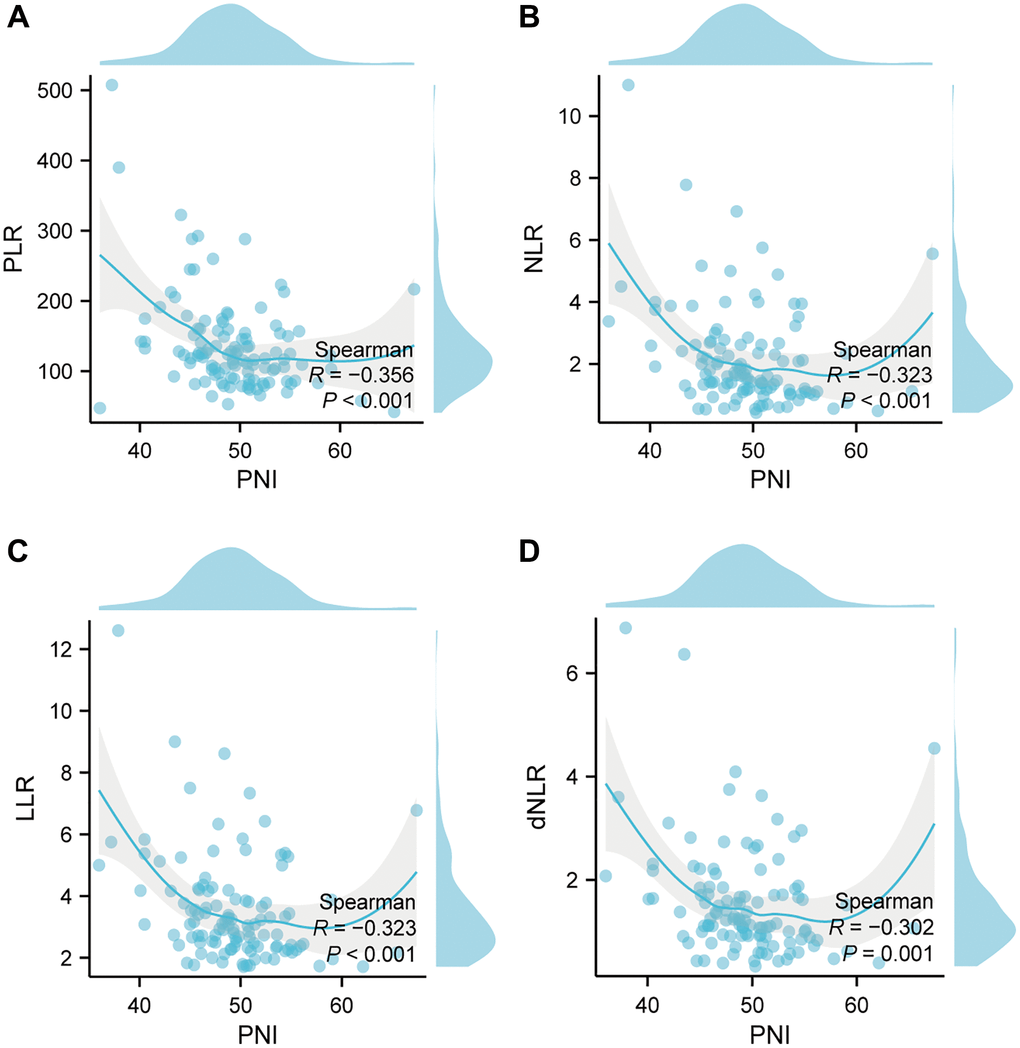
Figure 3. Correlation between nutritional index and inflammatory index in the whole study population. (A) The correlation between PNI and PLR; (B) The correlation between PNI and NLR; (C) The correlation between PNI and LLR; (D) The correlation between PNI and dNLR. Abbreviations: PNI: prognostic-nutrition index; PLR: platelet-lymphocyte ratio; NLR: neutrophil-lymphocyte ratio; LLR: leukocyte-lymphocyte ratio; dNLR: derived neutrophil-lymphocyte ratio; R: correlation.
Discussion
SCLC is a highly aggressive malignancy, poorly differentiated tumor that develops from bronchial neuroendocrine cells, with a 5-year overall survival rate of 6–7% [14]. It is a well-known fact that at an early stage, this tumor will exhibit hematogenous metastases and lymph node metastases. Nevertheless, early-stage SCLC isn’t a common clinical scenario. SCLC poses a serious threat to the lives of patients [15]. Chemoradiotherapy (CRT) is the treatment of first choice for patients with stage III LS-SCLC. Despite CRT, a proportion of patients will develop BM during the follow-up period. The central nervous system is a known refuge for SCLC, which makes it difficult to implement effective measures against the disease. BM is a common cause of death in SCLC patients. The prognosis for patients with SCLC who present with BM is generally unsatisfied [16]. These patients place a heavy burden on the nursing staff, the society, and the family members who are caring for them. The importance of BM for SCLC patients cannot be overstated. It is only through early diagnosis and prompt treatment that their chances of survival can be improved [17]. However, due to individual differences, the risk of BM is inconsistent and unclear even in male SCLC patients at the same tumor node metastasis (TNM) stage. Therefore, it is crucial to find an efficient tool that predicts the risk and probability of BM in SCLC patients with the same gender and TNM stage.
Recently, the nomogram has been widely used in cancer research and has been validated as a trustworthy instrument for evaluating the risk events in cancer patients, which may help with developing treatment strategy and conducting clinical trials. Therefore, well-established predictive models can help to better stratify treatment and risk assessment of LS-SCLC patients. In this retrospective study, we analyzed clinical data from male SCLC patients with stage III from 2008 to 2020. Our aim was to determine the independent risk factors affecting BM in LS-SCLC patients and to construct and verify a nomogram that could predict BM. To the best of our knowledge, there is currently no relevant prediction model has particularly been constructed to predict BM in male patients with stage III LS-SCLC. It represents the first attempt to develop prediction nomogram for this specific population segment.
The current study introduced a nomogram for predicting BM in LS-SCLC patients after CRT. We analyzed the impact of age, tumor location, smoke, CCRT, cycle of chemotherapy before radiotherapy, total cycle of chemotherapy, RT dose, radiotherapy time, PNI, PAR, PLR, NLR, LLR, dNLR, SII, and SIRI on the risk of BM. Our results demonstrated that CCRT, RT dose, and PNI were the independent risk factors for BM development. Next, we constructed and verified the nomogram using the significant factors in the multivariate logic analysis to predict the incidence of BM in LS-SCLC patients. The calibration curve showed an excellent consistency and discriminative ability between predicted risk and observed outcome for the nomogram. In addition, the DCA also revealed the potential clinical benefit of the model for future. These findings lend credence to the idea that this nomogram could be used in clinical practice, particularly for the purpose of developing individualized treatment plans. The nomogram is a tool that can be used by physicians to perform metastatic screening on SCLC patients who have a high risk of developing metastasis in the brain. As a result, timely treatment strategies can be implemented for these patients.
Compared with CCRT, patients without CCRT are more likely to develop BM, which was in accordance with the previous researches [18, 19]. Topkan et al. showed a significant difference (p = 0.03) between the concurrent CRT group and sequential CRT group for the occurrence of brain metastases in lung cancer, demonstrating that concurrent CRT can reduce the risk of BM [18]. Similarly, Robnett et al. demonstrated that the timing of radiotherapy can affect the risk of central nervous system recurrence, with a 27% incidence of BM in those receiving induction chemotherapy before radiotherapy and 15% in those receiving concurrent CRT. The incidence of BM within 2 years was 39% and 20%, respectively [19]. Although acute toxic effects following sequential CRT are usually well tolerated by patients, but tumor resistance is a problem that cannot be overlooked. The optimal combination of chemotherapy and radiotherapy is still controversial, but some studies have reported that the 3-year survival rate of patients with LS-SCLC is better with concurrent CRT than with sequential CRT and consolidation CRT [20]. In addition, simultaneous chemotherapy and radiotherapy can enhance the killing of tumors and reduce the accelerated re-proliferation of tumor cells during the radiotherapy process. Chemotherapy and radiotherapy act on tumor cells of different phases separately, which not only complement each other in space and time, but also enhance the sensitivity of treatment and anti-tumor efficacy, which can achieve more effective clinical treatment effect [21]. Therefore, we can be certain that CCRT treatment is a more reasonable treatment plan for patients in good condition and that it is worthy of reference and application by the majority of clinicians.
As is known to all, radiotherapy is the crucial treatment for LS-SCLC patients. Nonetheless, whether RT dose are associated with BM remains controversial. In our study, RT dose more than 60 Gy was an independent risk factor for BM. Similar findings from previous studies were reported. Compared to receiving more than 60 Gy of radiation therapy, receiving less than 60 Gy of radiation therapy significantly improved 5-year overall survival (26% vs. 16%) and decreased the risk of recurrence (36% vs. 52%) [22]. Another study showed that disease progression rates of 73% and 76% were observed in patients who received less than 60 Gy versus those who received more than 60 Gy, respectively [23]. This international phase III study, RTOG-0538, also demonstrated no significant effect on survival at doses below 60 Gy versus those above 60 Gy [23]. This also breaks the long-held theory in radiation oncology that more treatment equals better outcomes. However, in clinical practice, the majority of patients with LS-SCLC still receive radiotherapy doses in excess of 60 Gy [24]. Accordingly, patients with LS-SCLC do not necessarily benefit more from longer radiotherapy courses. In addition, the underlying mechanism behind the correlation between RT dose and BM development needs further elucidation. One possible explanation is that high radiotherapy doses cause more damage to normal tissues that comprise the blood-spinal cord barrier, causing tumor cells to more readily infiltrate the damaged blood-spinal cord barrier, which in turn produces BM through the cerebrospinal fluid circulation.
The present study also identified PNI was significantly associated with BM development in LS-SCLC patients. Our study results revealed that the optimum cutoff values for PNI was 45.15. There is a lack of consensus regarding the optimal PNI cutoff value, despite the fact that certain pieces of research have revealed that PNI may be a predictive factor of lung cancer. Recent studies have indicated that the cutoff value for PNI is 47.23–52.525 [25–27]. Due to the heterogeneity between the investigations, the cutoff values were distinct. The variation in sample size is also a significant contributor to the inconsistent research findings. PNI is an important nutritional index composed of albumin and lymphocyte. Although the relationship between PNI and BM in LS-SCLC has not been reported, a large number of studies have found that malnutrition is strongly associated with tumor metastasis and survival outcomes. Studies have revealed a high prevalence of malnutrition among cancer patients, including lung cancer patients [28]. Malnutrition interacts with tumor invasion and metastasis. Tumor metastasis is an independent factor leading to malnutrition, while the formation of tumor metastases contributes to malnutrition in patients [28]. According to the current study, the specific mechanism may be related to impaired immune function, inflammatory response, leptin level, and autophagy of tumor cells in cancer patients [29–31]. Therefore, nutritional therapy is important for SCLC patients. There is no evidence that nutritional support promotes tumor growth, and an increasing number of clinical studies have shown that nutritional therapy not only meets the nutritional needs of patients, but also enhances their immunity, improves their tolerance to radiotherapy and chemotherapy, kills tumor cells directly or indirectly, and reduces the risk of recurrence. In conclusion, timely interventions should be made to improve the nutritional status of patients with malnutrition.
Despite the fact that CRT is initially effective in treating SCLC, the central nervous system is a common location for recurrence. Our study revealed the incidence of BM in initial male SCLC patients with stage III is 25%, which was consistent with previously reported researches. In one study, the probability of BM in SCLC patients with stage I, II and III was 7% (2/30), 25% (3/12) and 27% (7/26), respectively [32]. Another study showed that the rates of BM in SCLC patients with TNM pathologic stages I, II, and III disease were 6.25% (2/32), 28.2% (11/39), and 29.1% (16/55), respectively [33]. Similar results have been reported in other studies, where BM was found in <10% of SCLC patients with pathological stage I compared to >20% of those with pathological stage II or stage III [34–36]. In patients with LS-SCLC, prophylactic cranial irradiation (PCI) can reduce the occurrence of BM and improve survival outcome [37]. However, some patients still experience BM even after implementing PCI [38]. Besides, PCI-induced neurocognitive dysfunction is a clinical issue that cannot be neglected [39]. PCI was found to be beneficial for patients at high risk of BM but not for those at low risk of BM [40]. Therefore, not all LS-SCLC patients develop BM. We need to develop a reliable predictive model to accurately evaluate the risk of BM occurrence so that patients at low BM risk do not have to undergo PCI and thus avoid neurotoxicity. The aim of this study was to construct a model for BM prediction in stage III LS-SCLC patients, and individualized treatment based on BM risk could benefit more patients. This assists in advising SCLC patients on treatment-related decisions as a way to enhance or diminish the intensity of treatment.
Although there are several studies to construct nomograms in lung cancer patients diagnosed with BM. However, it is still unclear how to distinguish between patients’ risks of developing BM in LS-SCLC. Qiu et al. developed a nomogram for predicting brain metastasis free survival in SCLC patients [27]. This study only analyzed the prognosis and did not analyze the risk factors of BM of SCLC. In a different piece of research, the researchers also focused solely on the prognostic factors of BM in SCLC, despite the fact that the sample size was quite large [41]. Although the risk factors and prognosis factors of BM were evaluated simultaneously in another study, the number of variables included was few and the staging of patients was complicated [42]. As we know, LS-SCLC patients typically present in stage III. Since most SCLC patients are male and at stage III, we present the first study to examine the risk factors for BM in male SCLC patients with stage III. There is no relevant prediction model has particularly been constructed to predict BM for this subgroup population till date. It represents the first attempt to develop prediction model for this specific population segment. The purpose of this research was to develop a predicted model for brain metastasis in male SCLC patients with stage III and helped in the early identification of high-risk patients and the selection of individualized therapies.
However, some limitations must be acknowledged in the present study. First of all, this study is a non-randomized and retrospective study, which may result in inevitable selection bias. Second, due to the rarity of SCLC and the strict inclusion criteria, the number of patients included in this study was relatively small. Therefore, more cases need to be collected in future studies. Third, several potential risk factors for BM in SCLC, including tumor markers and lactic dehydrogenase, were not included in this study due to a lack of data. In addition, the model constructed in this study is only applicable to male SCLC patients with stage III and has no reference value for predicting BM in other SCLC patients. In this study, the vast majority of our patients were not receiving immunotherapy. This prevents us from evaluating the effect of immunotherapy in brain metastases. Finally, these findings should be validated by prospective randomized controlled studies with larger data cohorts.
Conclusion
In general, the study revealed that CCRT, RT dose, and PNI were associated with BM occurrence in male SCLC patients with stage III. We established and verified a nomogram model that combines these variables to predict the incidence of BM in LS-SCLC patients. The nomogram had good performance for predicting the occurrence of BM, which aids in the early identification of high-risk SCLC patients and the selection of individualized therapies. Since the model has high reliability and clinical applicability, it can provide clinicians with theoretical guidance and treatment strategy making. Further multi-center large-scale prospective studies are necessary to validate the validity of our findings.
Materials and Methods
Patient selection
In this retrospective study, patients who were first diagnosed with stage III SCLC from 2008 to 2020 in the Fujian Provincial Cancer Hospital were included. The inclusion criteria were as follows: (1) Patients with first diagnosis of SCLC that was confirmed by cytology or pathology; (2) Male patient; (3) Age ≥ 18 years; (4) Karnofsky Performance Status (KPS) ≥ 70 points; (5) Patients received combined chemotherapy and radiotherapy (RT). The exclusion criteria were as follows: (1) Underwent surgery; (2) Patients with incomplete clinical and laboratory data; (3) Patients with BM at first diagnosis; (4) incomplete therapeutic information; (5) Patients with a history of other malignancy. The laboratory test results were collected within one week before treatment. In this study, the clinical stage was defined by the 8th American Joint Committee on Cancer (AJCC) staging system for SCLC. Following data filtering, one hundred and twelve patients who fulfilled the above criteria were included in this analysis. The Ethics Committee of Fujian Provincial Cancer Hospital reviewed and approved this study.
Treatment schedules
All patients received combined chemotherapy and radiotherapy. Etoposide, paclitaxel, or irinotecan was used in the chemotherapy regimens, and these drugs were combined with cisplatin, carboplatin, nedaplatin, or lobaplatin. The chemotherapy schedules adhered to the guidelines provided by the National Comprehensive Cancer Network (NCCN). All of the patients were scheduled to receive either three-dimensional conformal radiation therapy (3D-CRT) or intensity-modulated radiation therapy (IMRT). A 6MV medical linear accelerator was used for radiotherapy. Based on the guidelines of the NCCN, 45 Gy in 3 weeks (1.5 Gy twice daily [BID]) is superior (category 1) to 45 Gy in 5 weeks (1.8 Gy daily). When BID fractionation is used, there should be at least a 6-hour interfraction interval to allow for repair of normal tissue. If using once-daily RT, higher doses of 60–70 Gy should be used. The patients were received with a total dose of 42–69 Gy. In this study, concurrent radiotherapy within six cycles after the initiation of chemotherapy was defined as concurrent chemoradiotherapy.
Definition of nutritional and inflammatory index
The prognostic-nutrition index (PNI), platelet-albumin ratio (PAR), platelet-lymphocyte ratio (PLR), neutrophil-lymphocyte ratio (NLR), leukocyte-lymphocyte ratio (LLR), derived neutrophil-lymphocyte ratio (dNLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI) were calculated as follows: PNI = the serum albumin level + 5 × the absolute lymphocyte count; PAR = the absolute platelet count/the serum albumin level; PLR = the absolute platelet count/the absolute lymphocyte count; NLR = the absolute neutrophil count/the absolute lymphocyte count; LLR = the absolute leukocyte count/the absolute lymphocyte count; dNLR = the absolute neutrophil count/(the absolute leukocyte count-the absolute neutrophil count); SII = the absolute neutrophil count × the absolute platelet count/the absolute lymphocyte count; SIRI = the absolute neutrophil count × the absolute monocyte count/the absolute lymphocyte count.
Endpoints and follow-up
The endpoint is the development of BM in the SCLC patient. From the Electronic Medical Record System, we retrieved and reviewed the baseline clinical characteristics. Patients were followed up on at regular intervals (every 3–6 months) with a brain magnetic resonance imaging (MRI) after treatment. BM was diagnosed based on clinical manifestation and an enhanced MRI of the head. At the end of the follow-up period, all cases were censored.
Statistical analysis
All data analysis used Statistical Product and Service Solutions (SPSS) version26.0 and R software version 4.0.2 (R Foundation). The optimal cut-off values of age, radiotherapy time, PNI, PAR, PLR, NLR, LLR, dNLR, SII, and SIRI were calculated by the Receiver Operating Curve (ROC). Specifically, univariate logic regression was applied to identify the potential risk factors of BM for further analysis in multivariate logic regression. Based on univariate analysis, we included the risk factors with p < 0.05 in the multivariate analysis to identify independent predictors of BM. A ROC and nomogram for predicting the incidence of BM were then conducted based on the independent risk factors calculated by the multivariate analysis. The calibration curves (internal validation was performed using 1000 bootstrap resamples of the training cohort) were generated to evaluate the consistency between observed probability and predicted probability of BM. The perfectly calibrated curve would exhibit with a 45 degrees curve. The decision curve analysis (DCA) was performed to assess the clinical benefit of prediction models. Finally, Spearman correlation was carried out to evaluate the correlations of nutritional index and inflammatory index. All tests were two-tailed and a p-value < 0.05 was considered statistically significant.
Availability of data and materials
All relevant data are within the manuscript and its Supplementary Data Set.
Supplementary Materials
Author Contributions
BZ, BY, WZ, and JL designed this study. BY, WZ, and JQ contributed to the data collection. BY, WZ, and YY analyzed the data. BZ and JL supervised the study. BZ, BY, and WZ wrote the manuscript. All authors read and approved the final manuscript.
Acknowledgments
We thank all the investigators and patients who participated in the present study.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Ethical Statement and Consent
The current study was approved by the ethics committee of Fujian Medical University Cancer Hospital (K2021-115-01), Fuzhou, China and conducted in accordance with the principles of the Declaration of Helsinki and its amendment. All patients provided written informed consent prior to treatment, and all the information was anonymized prior to analysis.
Funding
This work was supported by the Joint Funds for the National Clinical Key Specialty Construction Program (Grant No. 2021), the Fujian Provincial Clinical Research Center for Cancer Radiotherapy and Immunotherapy (Grant No. 2020Y2012), and Fujian Clinical Research Center for Radiation and Therapy of Digestive, Respiratory and Genitourinary Malignancies (Grant No. 2021Y2014).
References
- 1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021; 71:7–33. https://doi.org/10.3322/caac.21654 [PubMed]
- 2. Oser MG, Niederst MJ, Sequist LV, Engelman JA. Transformation from non-small-cell lung cancer to small-cell lung cancer: molecular drivers and cells of origin. Lancet Oncol. 2015; 16:e165–72. https://doi.org/10.1016/S1470-2045(14)71180-5 [PubMed]
- 3. Gaspar LE, McNamara EJ, Gay EG, Putnam JB, Crawford J, Herbst RS, Bonner JA. Small-cell lung cancer: prognostic factors and changing treatment over 15 years. Clin Lung Cancer. 2012; 13:115–22. https://doi.org/10.1016/j.cllc.2011.05.008 [PubMed]
- 4. Ricotti A, Sciannameo V, Balzi W, Roncadori A, Canavese P, Avitabile A, Massa I, Berchialla P. Incidence and Prevalence Analysis of Non-Small-Cell and Small-Cell Lung Cancer Using Administrative Data. Int J Environ Res Public Health. 2021; 18:9076. https://doi.org/10.3390/ijerph18179076 [PubMed]
- 5. Kalemkerian GP, Akerley W, Bogner P, Borghaei H, Chow LQ, Downey RJ, Gandhi L, Ganti AK, Govindan R, Grecula JC, Hayman J, Heist RS, Horn L, et al. Small cell lung cancer. J Natl Compr Canc Netw. 2013; 11:78–98. https://doi.org/10.6004/jnccn.2013.0011 [PubMed]
- 6. Rudin CM, Ismaila N, Hann CL, Malhotra N, Movsas B, Norris K, Pietanza MC, Ramalingam SS, Turrisi AT
3rd , Giaccone G. Treatment of Small-Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American College of Chest Physicians Guideline. J Clin Oncol. 2015; 33:4106–11. https://doi.org/10.1200/JCO.2015.63.7918 [PubMed] - 7. Zhao H, Ren D, Liu H, Chen J. Comparison and discussion of the treatment guidelines for small cell lung cancer. Thorac Cancer. 2018; 9:769–74. https://doi.org/10.1111/1759-7714.12765 [PubMed]
- 8. Riihimäki M, Hemminki A, Fallah M, Thomsen H, Sundquist K, Sundquist J, Hemminki K. Metastatic sites and survival in lung cancer. Lung Cancer. 2014; 86:78–84. https://doi.org/10.1016/j.lungcan.2014.07.020 [PubMed]
- 9. van Oosterhout AG, van de Pol M, ten Velde GP, Twijnstra A. Neurologic disorders in 203 consecutive patients with small cell lung cancer. Results of a longitudinal study. Cancer. 1996; 77:1434–41. https://doi.org/10.1002/(SICI)1097-0142(19960415)77:8%3c1434::AID-CNCR3%3e3.0.CO;2-C [PubMed]
- 10. Svokos KA, Salhia B, Toms SA. Molecular biology of brain metastasis. Int J Mol Sci. 2014; 15:9519–30. https://doi.org/10.3390/ijms15069519 [PubMed]
- 11. Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021; 7:3. https://doi.org/10.1038/s41572-020-00235-0 [PubMed]
- 12. Ojerholm E, Alonso-Basanta M, Simone CB
2nd . Stereotactic radiosurgery alone for small cell lung cancer: a neurocognitive benefit? Radiat Oncol. 2014; 9:218. https://doi.org/10.1186/1748-717X-9-218 [PubMed] - 13. Shepherd FA, Crowley J, Van Houtte P, Postmus PE, Carney D, Chansky K, Shaikh Z, Goldstraw P, and International Association for the Study of Lung Cancer International Staging Committee and Participating Institutions. The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. J Thorac Oncol. 2007; 2:1067–77. https://doi.org/10.1097/JTO.0b013e31815bdc0d [PubMed]
- 14. Xie D, Marks R, Zhang M, Jiang G, Jatoi A, Garces YI, Mansfield A, Molina J, Yang P. Nomograms Predict Overall Survival for Patients with Small-Cell Lung Cancer Incorporating Pretreatment Peripheral Blood Markers. J Thorac Oncol. 2015; 10:1213–20. https://doi.org/10.1097/JTO.0000000000000585 [PubMed]
- 15. Morgan E, Arnold M, Rutherford MJ, Bardot A, Ferlay J, De P, Engholm G, Jackson C, Little A, Saint-Jacques N, Walsh P, Woods RR, O'Connell DL, et al. The impact of reclassifying cancers of unspecified histology on international differences in survival for small cell and non-small cell lung cancer (ICBP SurvMark-2 project). Int J Cancer. 2021; 149:1013–20. https://doi.org/10.1002/ijc.33620 [PubMed]
- 16. Cagney DN, Martin AM, Catalano PJ, Redig AJ, Lin NU, Lee EQ, Wen PY, Dunn IF, Bi WL, Weiss SE, Haas-Kogan DA, Alexander BM, Aizer AA. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol. 2017; 19:1511–21. https://doi.org/10.1093/neuonc/nox077 [PubMed]
- 17. Goncalves PH, Peterson SL, Vigneau FD, Shore RD, Quarshie WO, Islam K, Schwartz AG, Wozniak AJ, Gadgeel SM. Risk of brain metastases in patients with nonmetastatic lung cancer: Analysis of the Metropolitan Detroit Surveillance, Epidemiology, and End Results (SEER) data. Cancer. 2016; 122:1921–7. https://doi.org/10.1002/cncr.30000 [PubMed]
- 18. Topkan E, Parlak C, Kotek A, Yuksel O, Cengiz M, Ozsahin M, Pehlivan B. Impact of prophylactic cranial irradiation timing on brain relapse rates in patients with stage IIIB non-small-cell lung carcinoma treated with two different chemoradiotherapy regimens. Int J Radiat Oncol Biol Phys. 2012; 83:1264–71. https://doi.org/10.1016/j.ijrobp.2011.09.031 [PubMed]
- 19. Robnett TJ, Machtay M, Stevenson JP, Algazy KM, Hahn SM. Factors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinoma. J Clin Oncol. 2001; 19:1344–9. https://doi.org/10.1200/JCO.2001.19.5.1344 [PubMed]
- 20. Su J, Zhu S, Liu Z, Li J, Shen W, Li R. A study of elderly patients with limited-stage small-cell lung cancer after combined chemoradiotherapy. Am J Ther. 2014; 21:371–6. https://doi.org/10.1097/MJT.0b013e3182541cb3 [PubMed]
- 21. Vokes EE, Weichselbaum RR. Concomitant chemoradiotherapy: rationale and clinical experience in patients with solid tumors. J Clin Oncol. 1990; 8:911–34. https://doi.org/10.1200/JCO.1990.8.5.911 [PubMed]
- 22. Faivre-Finn C, Snee M, Ashcroft L, Appel W, Barlesi F, Bhatnagar A, Bezjak A, Cardenal F, Fournel P, Harden S, Le Pechoux C, McMenemin R, Mohammed N, et al. Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial. Lancet Oncol. 2017; 18:1116–25. https://doi.org/10.1016/S1470-2045(17)30318-2 [PubMed]
- 23. Bogart J, Wang X, Masters G, Gao J, Komaki R, Gaspar LE, Heymach J, Bonner J, Kuzma C, Waqar S, Petty W, Stinchcombe TE, Bradley JD, Vokes E. High-Dose Once-Daily Thoracic Radiotherapy in Limited-Stage Small-Cell Lung Cancer: CALGB 30610 (Alliance)/RTOG 0538. J Clin Oncol. 2023; 41:2394–402. https://doi.org/10.1200/JCO.22.01359 [PubMed]
- 24. Farrell MJ, Yahya JB, Degnin C, Chen Y, Holland JM, Henderson MA, Jaboin JJ, Harkenrider MM, Thomas CR
Jr , Mitin T. Radiation Dose and Fractionation for Limited-stage Small-cell Lung Cancer: Survey of US Radiation Oncologists on Practice Patterns. Clin Lung Cancer. 2019; 20:13–9. https://doi.org/10.1016/j.cllc.2018.08.015 [PubMed] - 25. Wang J, Liu Y, Mi X, Shao M, Liu L. The prognostic value of prognostic nutritional index (PNI) and neutrophil to lymphocyte ratio (NLR) for advanced non-small cell lung cancer treated with platinum-based chemotherapeutics. Ann Palliat Med. 2020; 9:967–78. https://doi.org/10.21037/apm.2020.04.31 [PubMed]
- 26. Li W, Qu Y, Wen F, Yu R, He X, Jia H, Liu H, Yu H. Prognostic nutritional index and systemic immune-inflammation index are prognostic biomarkers for non-small-cell lung cancer brain metastases. Biomark Med. 2021; 15:1071–84. https://doi.org/10.2217/bmm-2020-0786 [PubMed]
- 27. Qiu J, Ke D, Yu Y, Lin H, Zheng Q, Li H, Zheng H, Liu L, Wang Z, Wu Y, Liu T, Li J. A New Nomogram and Risk Stratification of Brain Metastasis by Clinical and Inflammatory Parameters in Stage III Small Cell Lung Cancer Without Prophylactic Cranial Irradiation. Front Oncol. 2022; 12:882744. https://doi.org/10.3389/fonc.2022.882744 [PubMed]
- 28. Marshall KM, Loeliger J, Nolte L, Kelaart A, Kiss NK. Prevalence of malnutrition and impact on clinical outcomes in cancer services: A comparison of two time points. Clin Nutr. 2019; 38:644–51. https://doi.org/10.1016/j.clnu.2018.04.007 [PubMed]
- 29. Dias Rodrigues V, Barroso de Pinho N, Abdelhay E, Viola JP, Correia MI, Brum Martucci R. Nutrition and Immune-Modulatory Intervention in Surgical Patients With Gastric Cancer. Nutr Clin Pract. 2017; 32:122–9. https://doi.org/10.1177/0884533616653807 [PubMed]
- 30. Inagaki-Ohara K. Gastric Leptin and Tumorigenesis: Beyond Obesity. Int J Mol Sci. 2019; 20:2622. https://doi.org/10.3390/ijms20112622 [PubMed]
- 31. Görgülü K, Diakopoulos KN, Kaya-Aksoy E, Ciecielski KJ, Ai J, Lesina M, Algül H. The Role of Autophagy in Pancreatic Cancer: From Bench to the Dark Bedside. Cells. 2020; 9:1063. https://doi.org/10.3390/cells9041063 [PubMed]
- 32. Nakamura H, Kato Y, Kato H. Outcome of surgery for small cell lung cancer -- response to induction chemotherapy predicts survival. Thorac Cardiovasc Surg. 2004; 52:206–10. https://doi.org/10.1055/s-2004-821075 [PubMed]
- 33. Gong L, Wang QI, Zhao L, Yuan Z, Li R, Wang P. Factors affecting the risk of brain metastasis in small cell lung cancer with surgery: is prophylactic cranial irradiation necessary for stage I-III disease? Int J Radiat Oncol Biol Phys. 2013; 85:196–200. https://doi.org/10.1016/j.ijrobp.2012.03.038 [PubMed]
- 34. Tsuchiya R, Suzuki K, Ichinose Y, Watanabe Y, Yasumitsu T, Ishizuka N, Kato H. Phase II trial of postoperative adjuvant cisplatin and etoposide in patients with completely resected stage I-IIIa small cell lung cancer: the Japan Clinical Oncology Lung Cancer Study Group Trial (JCOG9101). J Thorac Cardiovasc Surg. 2005; 129:977–83. https://doi.org/10.1016/j.jtcvs.2004.05.030 [PubMed]
- 35. Ogawa S, Horio Y, Yatabe Y, Fukui T, Ito S, Hasegawa Y, Mitsudomi T, Hida T. Patterns of recurrence and outcome in patients with surgically resected small cell lung cancer. Int J Clin Oncol. 2012; 17:218–24. https://doi.org/10.1007/s10147-011-0277-4 [PubMed]
- 36. Zhu H, Bi Y, Han A, Luo J, Li M, Shi F, Kong L, Yu J. Risk factors for brain metastases in completely resected small cell lung cancer: a retrospective study to identify patients most likely to benefit from prophylactic cranial irradiation. Radiat Oncol. 2014; 9:216. https://doi.org/10.1186/1748-717X-9-216 [PubMed]
- 37. Dingemans AC, Früh M, Ardizzoni A, Besse B, Faivre-Finn C, Hendriks LE, Lantuejoul S, Peters S, Reguart N, Rudin CM, De Ruysscher D, Van Schil PE, Vansteenkiste J, et al, and ESMO Guidelines Committee. Small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann Oncol. 2021; 32:839–53. https://doi.org/10.1016/j.annonc.2021.03.207 [PubMed]
- 38. Slotman BJ, van Tinteren H, Praag JO, Knegjens JL, El Sharouni SY, Hatton M, Keijser A, Faivre-Finn C, Senan S. Use of thoracic radiotherapy for extensive stage small-cell lung cancer: a phase 3 randomised controlled trial. Lancet. 2015; 385:36–42. https://doi.org/10.1016/S0140-6736(14)61085-0 [PubMed]
- 39. Yin X, Yan D, Qiu M, Huang L, Yan SX. Prophylactic cranial irradiation in small cell lung cancer: a systematic review and meta-analysis. BMC Cancer. 2019; 19:95. https://doi.org/10.1186/s12885-018-5251-3 [PubMed]
- 40. Chung JH, Kang SY, Wu HG, Seo YS, Kim DW, Kang KW, Kim HJ, Cheon GJ. Risk stratification of symptomatic brain metastases by clinical and FDG PET parameters for selective use of prophylactic cranial irradiation in patients with extensive disease of small cell lung cancer. Radiother Oncol. 2020; 143:81–7. https://doi.org/10.1016/j.radonc.2020.01.009 [PubMed]
- 41. Shan Q, Shi J, Wang X, Guo J, Han X, Wang Z, Wang H. A new nomogram and risk classification system for predicting survival in small cell lung cancer patients diagnosed with brain metastasis: a large population-based study. BMC Cancer. 2021; 21:640. https://doi.org/10.1186/s12885-021-08384-5 [PubMed]
- 42. Zhang GH, Liu YJ, De Ji M. Risk Factors, Prognosis, and a New Nomogram for Predicting Cancer-Specific Survival Among Lung Cancer Patients with Brain Metastasis: A Retrospective Study Based on SEER. Lung. 2022; 200:83–93. https://doi.org/10.1007/s00408-021-00503-0 [PubMed]