



Introduction
Lung cancer is the second most commonly diagnosed cancer and the leading cause of cancer-related death worldwide, with an estimated 2.2 million new cases and 1.8 million deaths in 2020 [1]. Non-small-cell lung cancer (NSCLC) represents 80%–85% of all lung cancer cases and is often diagnosed at an advanced stage [2]. There is significant geographical variation in epidermal growth factor receptor (EGFR) mutations, which are much more common in Asian (40%–60%) than in Western (10%–15%) NSCLC populations [3]. Activating EGFR mutations (e.g., exon 19 deletions and L858R) are predictive of progression-free survival (PFS), overall survival (OS), and response to tyrosine kinase inhibitors (TKIs) [4], of which afatinib, gefitinib, and erlotinib have been approved to treat EGFR-mutated NSCLC [4–6].
Lung cancer disproportionately affects older adults, with 71.1% of newly diagnosed patients being ≥65 years old and 36.2% being ≥75 years old [7]. This population often experiences physiological problems and increased comorbidities, with approximately half of those aged >75 years having two or more complications. Multiple factors, including polypharmacy, decreased social support, and limited economic resources, can affect the tolerability and effectiveness of cancer treatment for elderly patients [8]. The median age of patients was 63 years in the afatinib group and gefitinib group in the LUX-Lung 7 study [9], 61.5 years in the afatinib group in the LUX-Lung 3 study, 57 years in the gefitinib group in the IPASS study, and 65 years in the erlotinib group in the EURTAC study [4–6]. In the LUX-Lung 7 study [9], the only randomized study comparing afatinib and first-generation EGFR-TKIs, the benefit of afatinib for the subgroup (aged ≥65 years) receiving this therapy was nonsignificant, with a hazard ratio (HR) of 0.85 (95% confidence interval [CI] = 0.59–1.22) for PFS. Therefore, comparisons of the effectiveness and safety of these EGFR-TKIs approved for patients aged ≥65 years are limited.
The available real-world evidence for EGFR-TKI treatment of elderly patients is also limited. Therefore, this study aimed to describe the effectiveness and safety of afatinib, gefitinib, and erlotinib for treatment-naïve elderly patients (aged ≥65 years) with EGFR-mutated advanced NSCLC.
Materials and Methods
Patients and data collection
Patient data were obtained from the Cancer Registry System in the part of the Chang Gung Research Database [10, 11]. The selected patients were diagnosed with EGFR-mutated NSCLC and treated with first-line EGFR-TKI monotherapy (gefitinib, erlotinib, or afatinib) between May 2014, when Taiwan’s National Health Insurance began to reimburse afatinib, and January 2018. EGFR mutation status was retrospectively reviewed, and only patients with exon 19 deletions and exon 21 L858R mutations were included in the study.
The clinical data of patients who received EGFR-TKIs as first-line treatments were retrospectively reviewed. Their clinicopathological features, including age, sex, smoking history, Eastern Cooperative Oncology Group performance status (PS) score, tumor involvement, EGFR mutation (exon 19 deletion or L858R), dose adjustment (reduction/interruption), drug discontinuation, tumor response, adverse events (AEs), and subsequent treatment, were obtained. The last follow-up time point in this study was September 2021.
Treatment and response evaluation
The patients were treated with EGFR-TKIs administered once daily until disease progression determined based on radiological studies or intolerable AEs as evaluated by clinicians. The dose and schedule of the EGFR-TKIs were adjusted by clinicians according to the patient’s clinical condition and treatment-related AEs. The tumor response was evaluated most frequently with computed tomography and sometimes with chest radiography and/or additional positron emission tomography. The tumor response was evaluated according to the Response Evaluation Criteria in Solid Tumors (version 1.1). The detailed definitions of tumor response, including complete response, partial response, stable disease, progressive disease, and not assessed, as well as definitions of PFS and OS, were described in our previous study [12].
Adverse events
Data on AEs were collected from electronic medical records and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.0). Dose adjustments (reductions or interruptions) and drug discontinuations or withdrawals due to AEs were recorded.
Statistical analysis
Continuous variables were compared using the t-test or analysis of variance. Categorical variables were compared using the chi-square test or Fisher’s exact test. A series of univariate Cox proportional hazards models were applied to initially screen for potential factors associated with PFS and OS. Those variables with p-values <0.05 in the univariate Cox analysis were included in a multivariate Cox model. A two-sided p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS (2011 release; IBM Corp., Armonk, NY, USA), SPSS Statistics for Windows (version 20.0; IBM Corp.), and R statistical software (version 4.0.5) [13].
Results
Comparison of patient characteristics between younger (aged <65 years) and older (aged ≥65 years) patients
This study included 1343 treatment-naïve patients with EGFR-mutated advanced NSCLC, of whom 554 were aged <65 years and 789 were aged ≥65 years. Compared to older patients, younger patients showed better PS, were less likely to be nonsmokers, were more likely to have stage IV disease, and had a higher incidence of brain, bone, and distant lymph node metastasis. Tumor morphology did not differ significantly between younger and older patients (p = 0.273). The exon 19 deletion was more common in older patients (56.4% vs. 44.6%), while the L858R point mutation was more common in younger patients (55.4% vs. 43.6%, p < 0.0001). Younger patients were more frequently treated with afatinib than older patients (58.3% vs. 39.6%, p < 0.0001). However, afatinib remained the TKI of choice for older patients compared to erlotinib or gefitinib. The characteristics of younger and older patients are presented in Supplementary Table 1.
Progression-free survival did not differ significantly between patients aged <65 years and those aged ≥65 years treated with any of the EGFR-TKIs considered (p = 0.568; gefitinib: p = 0.459; erlotinib: p = 0.920; afatinib: p = 0.858). However, patients aged <65 years had significantly longer OS than those aged ≥65 years when treated with one of the three EGFR-TKIs (median of 25.5 vs. 20.1 months, p < 0.0001; gefitinib: median of 22.5 vs. 17.7 months, p = 0.035; erlotinib: median of 23.7 vs. 18.5 months, p = 0.049; afatinib: median of 28.5 vs. 22.2 months, p = 0.018; Supplementary Figure 1).
Characteristics of elderly patients (aged ≥65 years)
Elderly patients (aged ≥65 years) were further divided into three age groups and differences in their characteristics were examined. There were 383 patients aged 65–74 years, 323 aged 75–84 years, and 83 aged ≥85 years. The different age groups did not differ significantly in sex, smoking status, tumor morphology, and disease stage. PS worsened with age. Interestingly, the L858R point mutation was more common in patients aged ≥85 years (71.1%) than in those aged 75–84 (56.0%) or 65–74 (53.5%) years (p = 0.014). In addition, the choice of EGFR-TKI was age-dependent (p < 0.0001); gefitinib or erlotinib was prescribed more frequently as age increased, while afatinib was prescribed less frequently. The patients’ characteristics and the distribution of EGFR-TKIs among the age groups are summarized in Table 1.
Table 1. Patients’ characteristics of elderly patients (age ≥ 65 years).
| Characteristics | Age (years) | p-Value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65–74 (N=383) | 75–84 (N=323) | ≥85 (N=83) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | 0.307 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 158 (41.3%) | 115 (35.6%) | 32 (38.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 225 (58.7%) | 208 (64.4%) | 51 (61.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Performance status | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 65 (17.0%) | 36 (11.1%) | 4 (4.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 251 (65.5%) | 193 (59.8%) | 39 (47.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | 37 (9.7%) | 55 (17.0%) | 27 (32.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | 20 (5.2%) | 21 (6.5%) | 9 (10.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 | 10 (2.6%) | 18 (5.6%) | 4 (4.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 0.270 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 290 (75.7%) | 244 (75.6%) | 69 (83.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 80 (20.9%) | 64 (19.8%) | 14 (16.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 13 (3.4%) | 15 (4.6%) | 0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor morphology | 0.418 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adenocarcinoma | 376 (98.2%) | 313 (96.9%) | 82 (98.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-adenocarcinoma | 7 (1.8%) | 10 (3.1%) | 1 (1.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mutation | 0.014 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | 178 (46.5%) | 142 (44.0%) | 24 (28.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R | 205 (53.5%) | 181 (56.0%) | 59 (71.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage | 0.118 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | 35 (9.1%) | 21 (6.5%) | 11 (13.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 348 (90.9%) | 302 (93.5%) | 72 (86.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR-TKI | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Afatinib | 178 (46.5%) | 114 (35.3%) | 20 (24.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Erlotinib | 133 (34.7%) | 95 (29.4%) | 31 (37.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gefitinib | 72 (18.8%) | 114 (35.3%) | 32 (38.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver metastasis | 0.266 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 53 (13.8%) | 33 (10.2%) | 8 (9.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 330 (86.2%) | 290 (89.8%) | 75 (90.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brain metastasis | 0.152 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 119 (31.1%) | 92 (28.5%) | 17 (20.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 264 (68.9%) | 231 (71.5%) | 66 (79.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lung metastasis | 0.473 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 151 (39.4%) | 138 (42.7%) | 30 (36.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 232 (60.6%) | 185 (57.3%) | 53 (63.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bone metastasis | 0.052 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 173 (45.2%) | 125 (38.7%) | 27 (32.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 210 (54.8%) | 198 (61.3%) | 56 (67.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pleura metastasis | 0.034 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 163 (42.6%) | 169 (52.3%) | 40 (48.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 220 (57.4%) | 154 (47.7%) | 43 (51.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adrenal metastasis | 0.154 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 39 (10.2%) | 33 (10.2%) | 3 (3.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 344 (89.8%) | 290 (89.8%) | 80 (96.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Distant lymph node metastasis | 0.520 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 38 (9.9%) | 32 (9.9%) | 5 (6.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 345 (90.1%) | 291 (90.1%) | 78 (94.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pericardia metastasis | 0.347 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 4 (1.0%) | 6 (1.9%) | 0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 379 (99.0%) | 317 (98.1%) | 83 (100.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peritoneal metastasis | 0.777 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 2 (0.5%) | 2 (0.6%) | 0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 381 (99.5%) | 321 (99.4%) | 83 (100.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Footnote: Continuous variables were compared using a t-test or analysis of variance. Categorical variables were compared using a Chi-square or Fisher’s exact test. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: EGFR-TKI, epidermal growth factor receptor-tyrosine kinase inhibitor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Outcomes of EGFR-TKI therapy for elderly patients
Of the 789 elderly patients, 218 were treated with gefitinib, 259 with erlotinib, and 312 with afatinib. The effectiveness of the three EGFR-TKIs was evaluated in relation to objective response rate (ORR) and disease control rate (DCR). In the elderly patients, afatinib had a marginally higher ORR (68.6%) than gefitinib (58.7%) and erlotinib (62.2%; p = 0.054), but a significantly higher DCR (83.3%) than gefitinib (74.3%) and erlotinib (77.2%; p = 0.032). However, when the data were analyzed separately for each age subgroup, afatinib had numerically higher ORRs than gefitinib or erlotinib, although the differences were nonsignificant. Afatinib had a significantly higher DCR than gefitinib or erlotinib in patients aged 65–74 years (p = 0.027) but not in the other subgroups. The results are summarized in Table 2.
Table 2. The objective response rates (ORR) and disease control rates (DCR) of epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) among elderly patients (age ≥ 65 years).
| Characteristics | EGFR-TKIs | p-Value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gefitinib | Erlotinib | Afatinib | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Overall≥65 | (N=218) | (N=259) | (N=312) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ORR | 128 (58.7%) | 161 (62.2%) | 214 (68.6%) | 0.054 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DCR | 162 (74.3%) | 200 (77.2%) | 260 (83.3%) | 0.032 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65–75 | (N=72) | (N=133) | (N=178) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ORR | 49 (68.1%) | 84 (63.2%) | 125 (70.2%) | 0.417 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DCR | 56 (77.8%) | 102 (76.7%) | 156 (87.6%) | 0.027 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 75–55 | (N=114) | (N=95) | (N=114) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ORR | 66 (57.9%) | 62 (65.3%) | 76 (66.7%) | 0.343 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DCR | 84 (73.7%) | 74 (77.9%) | 91 (79.8%) | 0.531 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥85 | (N=32) | (N=31) | (N=20) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ORR | 13 (40.6%) | 15 (48.4%) | 13 (65.0%) | 0.229 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DCR | 22 (68.8%) | 24 (77.4%) | 13 (65.0%) | 0.591 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Footnote: The tumor response was evaluated most frequently by computed tomography and sometimes by chest radiography and/or additional positron emission tomography. The tumor response was evaluated according to the Response Evaluation Criteria in Solid Tumors (version 1.1). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The PFS and OS of patients aged ≥65 years treated with afatinib were more favorable (PFS: HR = 0.771, 95% CI = 0.656–0.907; OS: HR = 0.820, 95% CI = 0.699–0.962) than those of patients treated with erlotinib or gefitinib (Figure 1). Patients aged ≥65 years treated with afatinib had significantly longer PFS (median of 14.7 vs. 9.9 and 10.8 months, p = 0.003; Figure 2A) and OS (median of 22.2 vs. 17.7 and 18.5 months, p = 0.026; Figure 3A) than those treated with gefitinib or erlotinib. However, when the data were analyzed separately for each age subgroup (Figures 1–3), only PFS of patients aged 65–74 years differed significantly (p = 0.032; Figure 2B).
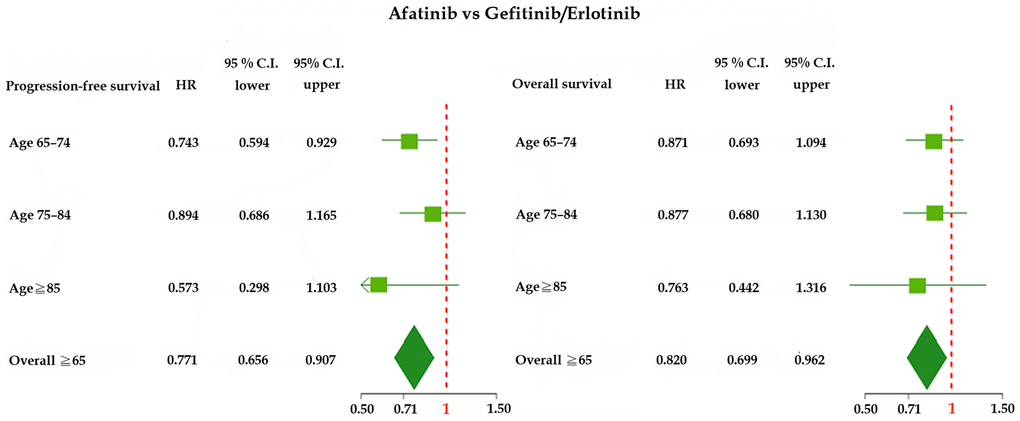
Figure 1. Forest plot of progression-free survival (PFS) and overall survival (OS) of elderly patients (age ≥65 years) treated with afatinib, gefitinib, or erlotinib. Abbreviations: HR, hazard ratio; CI, confidence interval.
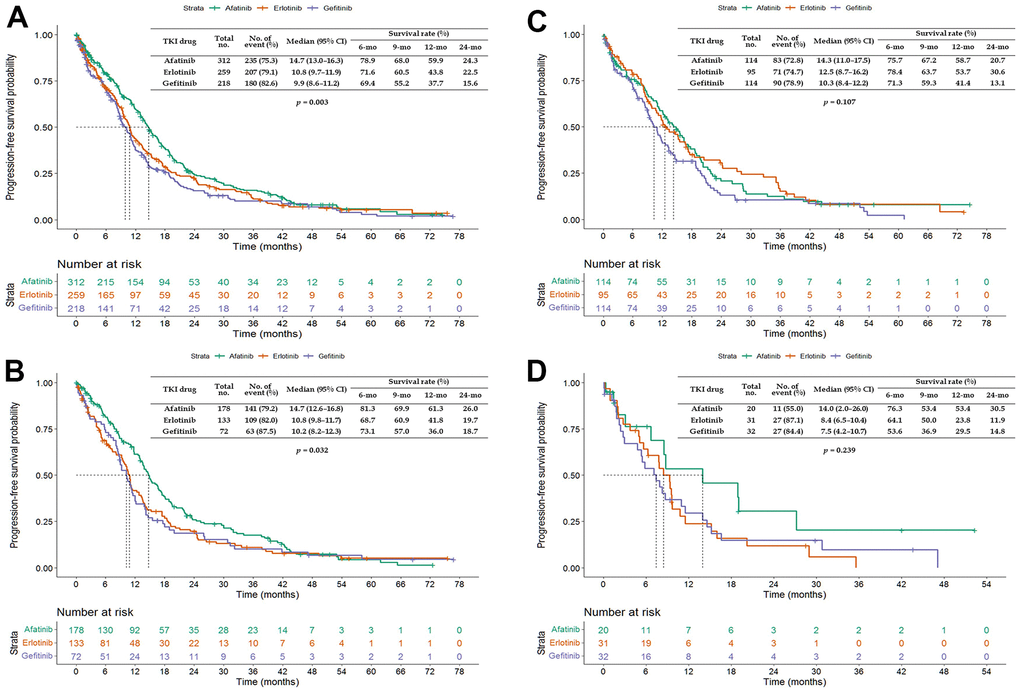
Figure 2. Kaplan–Meier curves of progression-free survival (PFS) of elderly patients treated with afatinib, erlotinib, or gefitinib. (A) Overall age ≥65 years; (B) age 65–74 years; (C) age 75–84 years; and (D) age ≥85 years. Abbreviations: TKI, tyrosine kinase inhibitor; CI, confidence interval.
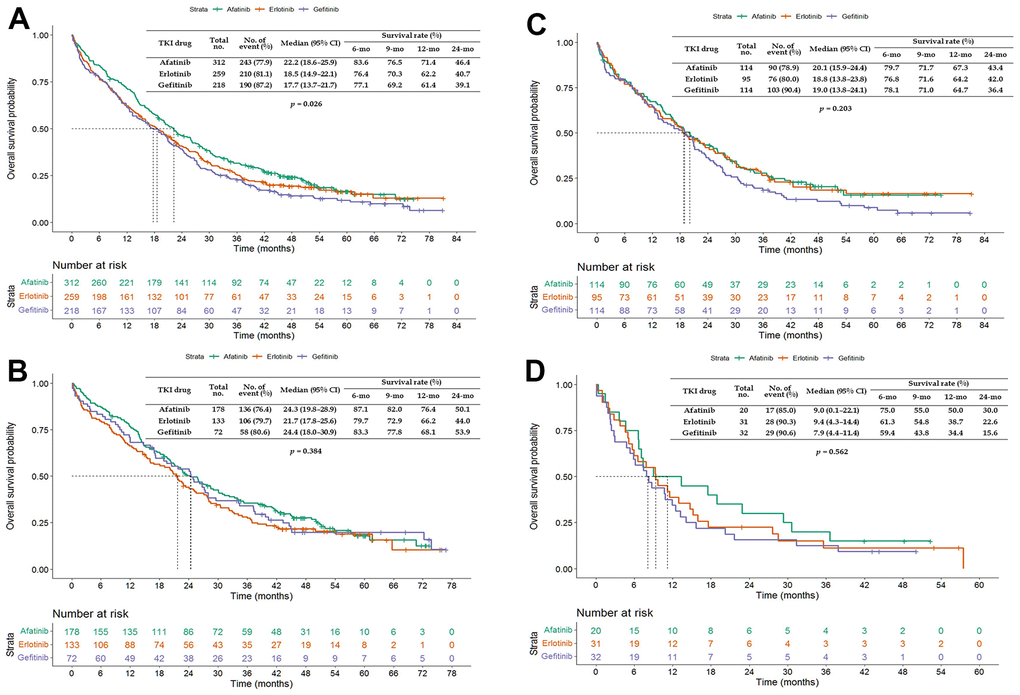
Figure 3. Kaplan–Meier curves of overall survival (OS) of elderly patients treated with afatinib, erlotinib, or gefitinib. (A) Overall age ≥65 years; (B) age 65–74 years; (C) age 75–84 years; and (D) age ≥85 years. Abbreviations: TKI, tyrosine kinase inhibitor; CI, confidence interval.
The PFS of patients aged 65–74 and 75–84 years was longer than that of patients aged ≥85 years when treated with any of the three EGFR-TKIs (p = 0.060) or erlotinib (p = 0.027) but not with gefitinib (p = 0.437) or afatinib (p = 0.803; Figure 4). The OS of patients aged 65–74 and 75–84 years was longer than that of patients aged ≥85 years when treated with any of the three EGFR-TKIs (p < 0.0001), gefitinib (p = 0.001), or erlotinib (p = 0.019; Figure 5).
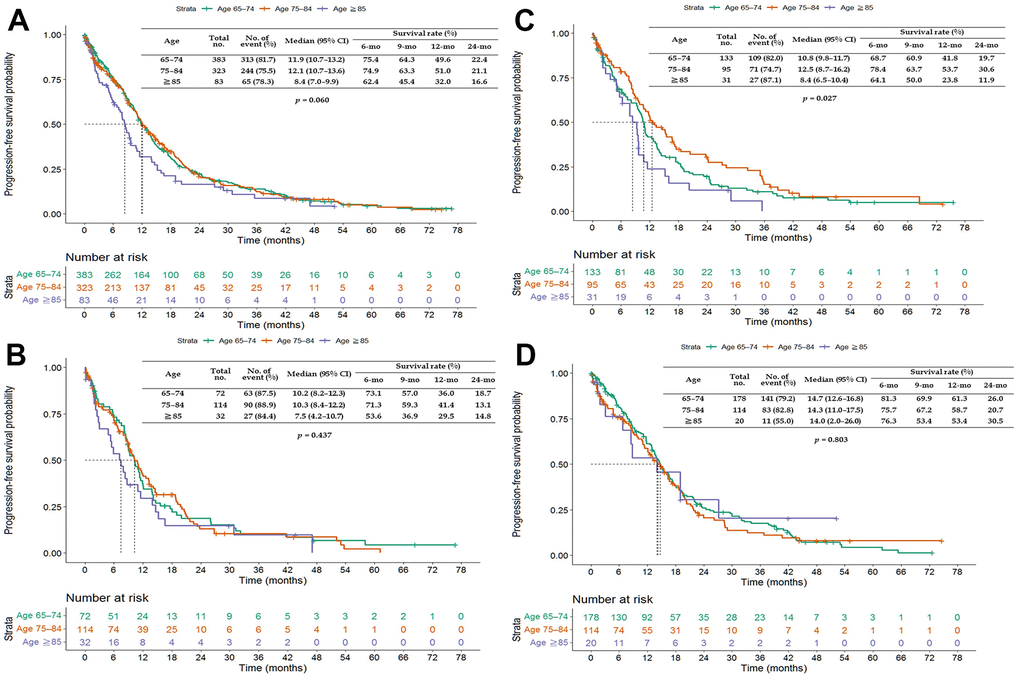
Figure 4. Kaplan–Meier curves of progression-free survival (PFS) of elderly patients (age ≥65 years) treated with epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs). (A) All EGFR-TKIs; (B) gefitinib; (C) erlotinib; and (D) afatinib. Abbreviation: CI, confidence interval.
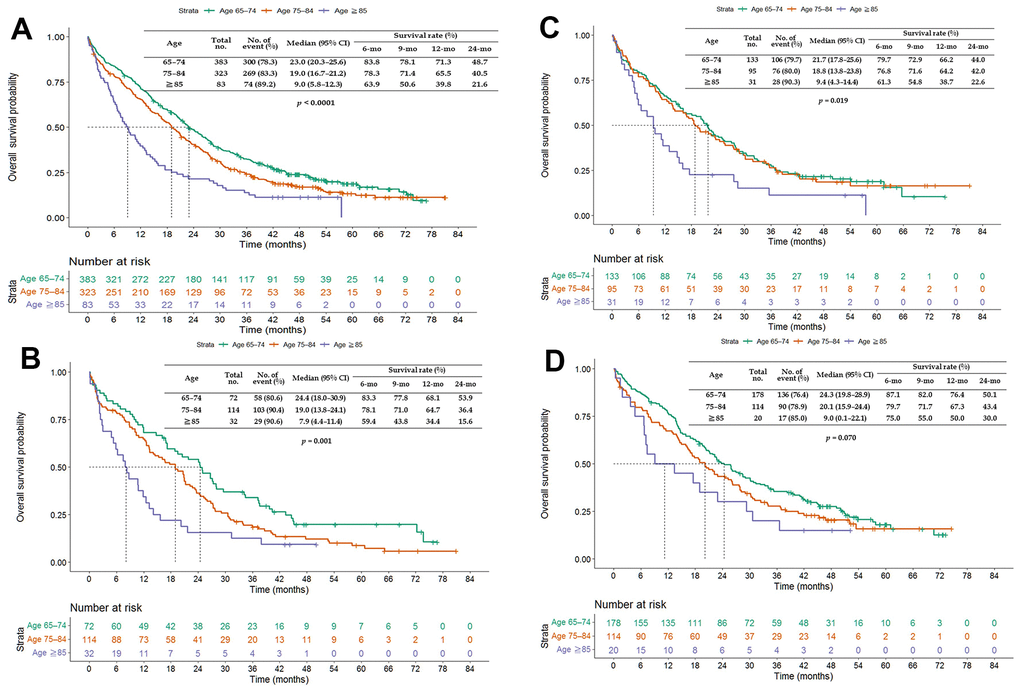
Figure 5. Kaplan–Meier curves of overall survival (OS) of elderly patients (age ≥65 years) treated with epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs). (A) All EGFR-TKIs; (B) gefitinib; (C) erlotinib; and (D) afatinib. Abbreviation: CI, confidence interval.
Adverse events of EGFR-TKIs
The AEs of EGFR-TKIs in elderly patients are presented in Table 3. The most common AEs of EGFR-TKIs, including skin toxicities, paronychia, mucositis, and diarrhea, were analyzed. The patients treated with afatinib experienced more AEs, as well as more grade ≥3 AEs, than those treated with gefitinib or erlotinib. In addition, more patients receiving afatinib required dose reductions or discontinuation compared to those treated with gefitinib or erlotinib.
Table 3. Adverse events of epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) among elderly patients (age ≥ 65 years).
| Characteristics | EGFR-TKIs | p-Value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gefitinib (N=218) | Erlotinib (N=259) | Afatinib (N=312) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dose-reduction | 25 (11.5%) | 38 (14.7%) | 122 (39.1%) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dose discontinuation | 9 (4.1%) | 27 (10.4%) | 46 (14.7%) | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥Grade 3 | 4 (1.8%) | 10 (3.9%) | 19 (6.1%) | 0.052 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any grades | 100 (45.9%) | 154 (59.5%) | 191 (61.2%) | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Paronychia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥Grade 3 | 1 (0.5%) | 6 (2.3%) | 16 (5.1%) | 0.006 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any grades | 52 (23.9%) | 67 (25.9%) | 160 (51.3%) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mucositis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥Grade 3 | 0 | 3 (1.1%) | 6 (1.9%) | 0.122 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any grades | 27 (12.4%) | 34 (13.1%) | 112 (35.9%) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diarrhea | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥Grade 3 | 5 (2.3%) | 4 (1.5%) | 29 (9.3%) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any grades | 76 (34.9%) | 90 (34.7%) | 230 (73.7%) | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Footnote: The EGFR-TKIs’ dose and schedule were adjusted by clinicians based on the patient’s clinical condition and treatment-related AEs. Data on AEs were collected from electronic medical records and graded according to National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.0). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Univariate and multivariate analysis of prognostic factors of progression-free survival of elderly patients
A univariate analysis was performed to explore the possible prognostic factors of PFS of elderly patients treated with EGFR-TKIs (Table 4). Patients with a PS score of 2–4, stage IV disease, and ≥4 metastatic sites had significantly worse PFS. Patients with liver, brain, bone, pleural, adrenal, and pericardial metastasis showed significantly worse PFS. Treatment with gefitinib also resulted in significantly worse PFS.
Table 4. Univariate and multivariate analysis of prognostic factors of progression-free survivals (PFS) for elderly patients (age ≥ 65 years).
| Parameters | No | Univariate analysis | Multivariate analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (months) | 95% CI | p-Value | Hazard ratio | 95% CI | p-Value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | 0.060 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65–74 | 383 | 11.9 | 10.7–13.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 75-84 | 323 | 12.1 | 10.7–13.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥85 | 83 | 8.4 | 7.0–9.9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | 0.474 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 305 | 11.0 | 9.3–12.8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 484 | 11.8 | 10.6–13.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Performance status | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0–1 | 588 | 13.3 | 12.2–14.4 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2–4 | 201 | 6.8 | 5.1–8.5 | 1.73 | 1.43–2.09 | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 0.078 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 158 | 9.7 | 7.4–12.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 603 | 12.0 | 10.9–13.0 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 28 | 10.3 | 8.9–11.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor morphology | 0.102 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adenocarcinoma | 771 | 11.7 | 10.8–12.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-adenocarcinoma | 18 | 4.6 | 0.1–9.4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mutation | 0.646 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 19del | 344 | 12.9 | 11.5–14.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R | 445 | 11.0 | 10.1–11.9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIB | 67 | 27.2 | 18.6–35.7 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 722 | 11.1 | 10.2–11.9 | 1.75 | 1.26–2.45 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lung metastasis | 0.113 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 319 | 11.1 | 10.1–12.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 470 | 12.0 | 10.7–13.4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 94 | 8.9 | 7.3–10.5 | 1.34 | 1.04–1.74 | 0.026 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 695 | 12.1 | 11.1–13.1 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brain metastasis | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 228 | 9.2 | 7.6–10.9 | 1.18 | 0.98–1.43 | 0.079 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 561 | 12.6 | 11.4–13.8 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bone metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 325 | 10.4 | 9.3–11.6 | 1.24 | 1.04–1.48 | 0.016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 464 | 13.0 | 11.8–14.1 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pleura metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 372 | 11.0 | 10.2–11.9 | 1.39 | 1.17–1.64 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 417 | 13.2 | 11.3–15.1 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adrenal metastasis | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 75 | 8.6 | 5.3–12.0 | 1.37 | 1.04–1.80 | 0.025 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 714 | 12.0 | 11.1–13.0 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Distant lymph node metastasis | 0.481 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 75 | 10.2 | 6.0–14.3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 714 | 11.7 | 10.8–12.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pericardia metastasis | 0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 10 | 1.8 | 1.2–2.5 | 2.39 | 1.16–4.92 | 0.018 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 779 | 11.7 | 10.8–12.6 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peritoneum metastasis | 0.102 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 4 | 3.9 | 0.1–13.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 785 | 11.7 | 10.8–12.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of metastatic sites | <0.0001 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0-1 | 348 | 14.6 | 12.3–16.9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2-3 | 354 | 11.0 | 10.2–11.9 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 or more | 87 | 7.7 | 5.8–9.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR-TKI | 0.003 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Afatinib | 312 | 14.7 | 13.0–16.3 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Erlotinib | 259 | 10.8 | 9.7–11.9 | 1.17 | 0.97–1.42 | 0.102 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gefitinib | 218 | 9.9 | 8.6–11.2 | 1.48 | 1.21–1.80 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Footnote: A series of univariate Cox proportional hazards models were performed to initially screen for potential factors associated with PFS. Those variables with p-values <0.05 in the univariate Cox analysis were further introduced into a multivariable Cox model. A two-sided p-value of <0.05 was considered statistically significant. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CI, confidence interval; EGFR-TKI, epidermal growth factor receptor-tyrosine kinase inhibitor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Multivariate analysis was performed to identify potential independent prognostic factors of PFS (Table 4). PS of 2–4, stage IV disease, liver, bone, pleural, adrenal, and pericardial metastasis, and EGFR-TKI treatment with gefitinib were independent unfavorable prognostic factors of PFS.
Univariate and multivariate analysis of prognostic factors of overall survival of elderly patients
Univariate analyses were performed to explore the possible prognostic factors of OS of patients aged ≥65 years treated with EGFR-TKIs (Table 5). The OS of patients aged ≥85 years with a PS of 2–4, non-adenocarcinoma morphology, stage IV disease, and ≥4 metastatic sites was significantly worse. In addition, the OS of patients with liver, brain, bone, pleural, adrenal, and pericardial metastasis was significantly worse. EGFR-TKI treatment with gefitinib was also associated with significantly worse OS.
Table 5. Univariate and multivariate analysis of prognostic factors of overall survivals (OS) for elderly patients (age ≥ 65 years).
| Parameters | No | Univariate analysis | Multivariate analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Median (months) | 95% CI | p-Value | Hazard ratio | 95% CI | p-Value | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (years) | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 65–74 | 383 | 23.0 | 20.3–25.6 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 75-84 | 323 | 19.0 | 16.7–21.2 | 1.17 | 0.98–1.38 | 0.077 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥85 | 83 | 9.0 | 5.8–12.3 | 1.90 | 1.45–2.48 | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | 0.512 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 305 | 20.5 | 17.8–23.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 484 | 19.5 | 17.1–21.8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Performance status | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0-1 | 588 | 24.1 | 21.8–26.5 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2–4 | 201 | 8.0 | 5.7–10.4 | 2.21 | 1.84–2.65 | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking | 0.092 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 158 | 17.7 | 12.7–22.8 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 603 | 20.3 | 18.0–22.5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unknown | 28 | 16.7 | 0.9–32.4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor morphology | 0.046 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adenocarcinoma | 771 | 20.2 | 18.3–22.1 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-adenocarcinoma | 18 | 8.0 | 0.4–15.5 | 1.11 | 0.67–1.84 | 0.697 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mutation | 0.187 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 19del | 344 | 22.0 | 18.8–25.3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R | 445 | 18.2 | 16.0–20.3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stage | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIB | 67 | 45.1 | 31.1–59.0 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IV | 722 | 18.8 | 17.0–20.5 | 1.80 | 1.25–2.59 | 0.002 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lung metastasis | 0.059 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 319 | 19.0 | 15.4–22.5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 470 | 20.7 | 18.2–23.3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 94 | 11.5 | 8.8–14.1 | 1.43 | 1.12–1.82 | 0.004 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 695 | 20.9 | 19.2–22.7 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brain metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 228 | 14.2 | 11.4–16.9 | 1.22 | 1.02–1.47 | 0.030 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 561 | 21.8 | 19.5–24.2 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bone metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 325 | 14.7 | 12.3–17.2 | 1.43 | 1.20–1.69 | <0.0001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 464 | 23.5 | 20.6–26.5 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pleura metastasis | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 372 | 17.2 | 14.9–19.6 | 1.34 | 1.13–1.57 | <0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 417 | 22.8 | 20.2–25.3 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Adrenal metastasis | <0.0001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 75 | 12.5 | 10.0–14.9 | 1.53 | 1.18–1.99 | 0.001 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 714 | 20.9 | 18.9–22.8 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Distant lymph node metastasis | 0.406 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 75 | 17.7 | 13.3–22.1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 714 | 20.3 | 18.2–22.3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pericardia metastasis | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 10 | 1.8 | 0.1–7.1 | 2.54 | 1.33–4.88 | 0.005 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 779 | 20.1 | 18.2–22.1 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Peritoneum metastasis | 0.954 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | 4 | 3.9 | 0.1–20.6 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No | 785 | 20.1 | 18.2–22.1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No. of metastatic sites | <0.0001 | - | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0-1 | 348 | 27.2 | 23.9–30.7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2-3 | 354 | 17.2 | 14.8–9.5 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 or more | 87 | 7.8 | 4.4–11.2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR-TKI | 0.026 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Afatinib | 312 | 22.2 | 18.6–25.9 | Reference | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Erlotinib | 259 | 18.5 | 14.9–22.1 | 1.05 | 0.87–1.27 | 0.623 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gefitinib | 218 | 17.7 | 13.7–21.7 | 1.27 | 1.05–1.55 | 0.016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Footnote: A series of univariate Cox proportional hazards models were performed to initially screen for potential factors associated with OS. Those variables with p-values <0.05 in the univariate Cox analysis were further introduced into a multivariable Cox model. A two-sided p-value of <0.05 was considered statistically significant. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: CI, confidence interval; EGFR-TKI, epidermal growth factor receptor-tyrosine kinase inhibitor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Multivariate analysis was performed to identify the potential independent prognostic factors of OS (Table 5). Age ≥85 years, PS of 2–4, stage IV disease, liver, brain, bone, pleural, adrenal, and pericardial metastasis, and EGFR-TKI treatment with gefitinib were independent unfavorable prognostic factors of OS.
Discussion
This large retrospective study used real-world data to determine the effectiveness and safety of EGFR-TKIs for elderly patients with EGFR-mutated advanced NSCLC. Of 789 patients aged ≥65 years, 218 were treated with gefitinib, 259 with erlotinib, and 312 with afatinib. Younger patients were more frequently treated with afatinib than older patients (58.3% vs. 39.6%; p < 0.0001). However, afatinib remained the preferred TKI for older patients compared to erlotinib or gefitinib. Afatinib as a first-line treatment was more effective, with a median PFS of 14.7 months and OS of 22.2 months, than gefitinib (9.9 and 17.7 months, respectively) and erlotinib (10.8 and 18.5 months, respectively). However, patients treated with afatinib also experienced more grade ≥3 AEs than those treated with gefitinib or erlotinib. Furthermore, PS of 2–4, stage IV disease, liver, bone, pleural, adrenal, and pericardial metastasis, and EGFR-TKI treatment with gefitinib were identified as independent unfavorable prognostic factors of PFS, while age ≥ 85 years, PS of 2–4, stage IV disease, liver, brain, bone, pleural, adrenal, and pericardial metastasis, and EGFR-TKI treatment with gefitinib were independent unfavorable prognostic factors of OS.
In the LUX-Lung 3 study, PFS of patients with EGFR-mutated advanced lung adenocarcinoma was longer with afatinib than with doublet chemotherapy (11.1 vs. 6.9 months; HR = 0.58, 95% CI = 0.43–0.78, p = 0.001) [5]. In the LUX-Lung 7 study, PFS of patients with advanced NSCLC with common EGFR mutations was longer with afatinib than with gefitinib (11.0 vs. 10.9 months; HR = 0.73, 95% CI = 0.57–0.95, p = 0.017) [9]. However, it is important to note that the results of these studies may not necessarily apply to all populations, including elderly patients. In the LUX-Lung 7 study, the only randomized study comparing afatinib and first-generation EGFR-TKIs, the median age of both groups was 63 years and 44.5% of the patients were more than 65 years old. The benefit of afatinib for this subgroup was nonsignificant with an HR of 0.85 (95% CI = 0.59–1.22), which might have been due to the small number of cases [9]. In addition, the safety of TKIs for elderly patients was rarely discussed in LUX-LUNG 7 and retrospective studies.
Real-world evidence shows that the survival outcomes of patients with advanced NSCLC with common EGFR mutations [10], uncommon EGFR mutations [12, 14, 15], or poor PS [16, 17] were better with afatinib than with gefitinib or erlotinib. In a study of 2190 patients with common EGFR mutations, univariate analysis identified EGFR-TKI use as a prognostic factor (erlotinib or gefitinib vs. afatinib; p < 0.0001). Multivariate analysis confirmed EGFR-TKI use as an independent prognostic factor (erlotinib vs. afatinib: adjusted HR [AHR] = 1.274, 95% CI = 1.117–1.454, p < 0.001; gefitinib vs. afatinib: AHR = 1.461, 95% CI = 1.307–1.633, p < 0.0001) [10]. In a study of 230 patients with uncommon EGFR mutations, PFS and OS of patients receiving afatinib were better than those of patients receiving gefitinib or erlotinib (PFS: 6.4 vs. 5.9 months, p = 0.022; OS: 13.4 vs. 13.0 months, p = 0.008) [12]. Similarly, in an investigation of 517 patients with a PS ≥2 [16], PFS and OS of patients treated with 40 mg of afatinib were better than those of patients treated with gefitinib or erlotinib (PFS: 11.6 vs. 6.8 or 6.7 months, p = 0.009; OS: 16.2 vs. 10.0 or 9.6 months, p = 0.001), although this trend was nonsignificant in multivariate analyses. Dose adjustment was an independent prognostic factor of PFS and OS, regardless of the EGFR-TKI used [16].
While most patients with EGFR-mutated NSCLC initially respond well to EGFR-TKIs, the disease eventually progresses due to acquired resistance. A secondary EGFR mutation involving a substitution of threonine for methionine at position 790 (T790M) has been identified [18]. Osimertinib can overcome treatment resistance associated with this EGFR T790M mutation, with afatinib followed by osimertinib being an effective therapeutic strategy [11, 19–21].
Patients discontinuing EGFR-TKIs due to intolerable AEs should be switched to another EGFR-TKI [22]. In a retrospective study of 2190 patients treated with first-line EGFR-TKIs, 114 experienced intolerable AEs requiring discontinuation of EGFR-TKIs. Age >65 years, female sex, body weight, and body surface area were associated with intolerable AEs in patients treated with afatinib. PFS of patients receiving subsequent first-line EGFR-TKIs (median = 14.9 months, 95% CI = 11.0–18.8 months) was better than that of patients receiving chemotherapy (median = 7.0 months, 95% CI = 1.0–12.3 months) and patients without subsequent treatment (median = 0.9 months, 95% CI = 0.6–1.2 months). In addition, OS of patients receiving subsequent EGFR-TKIs (median = 31.3 months, 95% CI = 23.9–38.7 months) was better than that of patients receiving chemotherapy (median = 19.4 months, 95% CI = 18.5–20.3 months) and patients without subsequent treatment (median = 2.4 months, 95% CI = 1.3–3.5 months) [22].
This study has several limitations. Bias might have been introduced into the study due to its retrospective nature. There might also have been selection bias since the clinician chose the EGFR-TKI. In addition, the choice of sequential treatment could have affected survival outcomes.
In conclusion, this study demonstrated the effectiveness and safety of EGFR-TKIs for elderly patients with EGFR-mutated advanced NSCLC, a population that has often been underrepresented in clinical trials and real-world evidence. For elderly patients with EGFR-mutated advanced NSCLC, clinicians were more likely to prefer gefitinib or erlotinib to afatinib as a therapy, in contrast to the treatment regimen for younger patients. Nevertheless, afatinib still emerged as the primary choice for first-line treatment for older patients compared to other EGFR-TKIs, as it is more effective than gefitinib or erlotinib in elderly patients with EGFR-mutated advanced NSCLC.
Author Contributions
Ling-Jen Hung, John Wen-Cheng Chang, and Chiao-En Wu conceived and designed the study. Ping-Chih Hsu and Chen-Yang Huang contributed to the literature search. Chih-Hsi Scott Kuo and Ching-Fu Chang performed data collection. Cheng-Ta Yang, John Wen-Cheng Chang, and Chiao-En Wu conducted data analysis and interpretation. Ling-Jen Hung drafted the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement and Consent
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (approval number: 202300775B0). Since this was a retrospective study, patient consent to participate was not required.
Funding
This study was supported by grants from Linkou Chang-Gung Memorial Hospital (Grant No. CMRPG3M0971 to C.-E. W.).
References
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71:209–49. https://doi.org/10.3322/caac.21660 [PubMed]
- 2. Planchard D, Popat S, Kerr K, Novello S, Smit EF, Faivre-Finn C, Mok TS, Reck M, Van Schil PE, Hellmann MD, Peters S, and ESMO Guidelines Committee. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 (Suppl 4); 29:iv192–237. https://doi.org/10.1093/annonc/mdy275 [PubMed]
- 3. Tan AC, Tan DSW. Targeted Therapies for Lung Cancer Patients With Oncogenic Driver Molecular Alterations. J Clin Oncol. 2022; 40:611–25. https://doi.org/10.1200/JCO.21.01626 [PubMed]
- 4. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009; 361:947–57. https://doi.org/10.1056/NEJMoa0810699 [PubMed]
- 5. Sequist LV, Yang JC, Yamamoto N, O’Byrne K, Hirsh V, Mok T, Geater SL, Orlov S, Tsai CM, Boyer M, Su WC, Bennouna J, Kato T, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013; 31:3327–34. https://doi.org/10.1200/JCO.2012.44.2806 [PubMed]
- 6. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, et al, and Spanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012; 13:239–46. https://doi.org/10.1016/S1470-2045(11)70393-X [PubMed]
- 7. Marur S, Singh H, Mishra-Kalyani P, Larkins E, Keegan P, Sridhara R, Blumenthal GM, Pazdur R. FDA analyses of survival in older adults with metastatic non-small cell lung cancer in controlled trials of PD-1/PD-L1 blocking antibodies. Semin Oncol. 2018; 45:220–5. https://doi.org/10.1053/j.seminoncol.2018.08.007 [PubMed]
- 8. Fukushima T, Oyamada Y, Ikemura S, Nukaga S, Inoue T, Arai D, Ohgino K, Kuroda A, Ishioka K, Sakamaki F, Suzuki Y, Terai H, Yasuda H, et al. Real-world clinical practice for advanced non-small-cell lung cancer in the very elderly: A retrospective multicenter analysis. Clin Lung Cancer. 2022; 23:532–41. https://doi.org/10.1016/j.cllc.2022.05.003 [PubMed]
- 9. Park K, Tan EH, O’Byrne K, Zhang L, Boyer M, Mok T, Hirsh V, Yang JC, Lee KH, Lu S, Shi Y, Kim SW, Laskin J, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016; 17:577–89. https://doi.org/10.1016/S1470-2045(16)30033-X [PubMed]
- 10. Chang JW, Huang CY, Fang YF, Chang CF, Yang CT, Kuo CS, Hsu PC, Wu CE. Risk Stratification Using a Novel Nomogram for 2190 EGFR-Mutant NSCLC Patients Receiving the First or Second Generation EGFR-TKI. Cancers (Basel). 2022; 14:977. https://doi.org/10.3390/cancers14040977 [PubMed]
- 11. Hsu PC, Chang JW, Chang CF, Huang CY, Yang CT, Kuo CS, Fang YF, Wu CE. Sequential treatment in advanced non-small cell lung cancer harboring EGFR mutations. Ther Adv Respir Dis. 2022; 16:17534666221132731. https://doi.org/10.1177/17534666221132731 [PubMed]
- 12. Chang JW, Huang CY, Fang YF, Chang CF, Yang CT, Kuo CS, Hsu PC, Wu CE. Epidermal growth factor receptor tyrosine kinase inhibitors for non-small cell lung cancer harboring uncommon EGFR mutations: Real-world data from Taiwan. Thorac Cancer. 2023; 14:12–23. https://doi.org/10.1111/1759-7714.14537 [PubMed]
- 13. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2021.
- 14. Chang JW, Huang CY, Fang YF, Chang CF, Yang CT, Kuo CS, Hsu PC, Wu CE. Epidermal growth factor receptor tyrosine kinase inhibitors for de novo T790M mutation: A retrospective study of 44 patients. Thorac Cancer. 2022; 13:1888–97. https://doi.org/10.1111/1759-7714.14272 [PubMed]
- 15. Hsu PC, Lee SH, Chiu LC, Lee CS, Wu CE, Kuo SC, Ju JS, Huang AC, Li SH, Ko HW, Yang CT, Wang CC. Afatinib in Untreated Stage IIIB/IV Lung Adenocarcinoma with Major Uncommon Epidermal Growth Factor Receptor (EGFR) Mutations (G719X/L861Q/S768I): A Multicenter Observational Study in Taiwan. Target Oncol. 2023; 18:195–207. https://doi.org/10.1007/s11523-023-00946-w [PubMed]
- 16. Wu CE, Chang CF, Huang CY, Yang CT, Kuo CS, Hsu PC, Chang JW. Comparison of Different Tyrosine Kinase Inhibitors for Treatment of Poor Performance Status Patients with EGFR-Mutated Lung Adenocarcinoma. Cancers (Basel). 2022; 14:674. https://doi.org/10.3390/cancers14030674 [PubMed]
- 17. Wu CE, Chang CF, Huang CY, Yang CT, Kuo CS, Hsu PC, Chang JW. Feasibility and effectiveness of afatinib for poor performance status patients with EGFR-mutation-positive non-small-cell lung cancer: a retrospective cohort study. BMC Cancer. 2021; 21:859. https://doi.org/10.1186/s12885-021-08587-w [PubMed]
- 18. Ohashi K, Maruvka YE, Michor F, Pao W. Epidermal growth factor receptor tyrosine kinase inhibitor-resistant disease. J Clin Oncol. 2013; 31:1070–80. https://doi.org/10.1200/JCO.2012.43.3912 [PubMed]
- 19. Wu SG, Chiang CL, Liu CY, Wang CC, Su PL, Hsia TC, Shih JY, Chang GC. An Observational Study of Acquired EGFR T790M-Dependent Resistance to EGFR-TKI Treatment in Lung Adenocarcinoma Patients in Taiwan. Front Oncol. 2020; 10:1481. https://doi.org/10.3389/fonc.2020.01481 [PubMed]
- 20. Chen CH, Chang JW, Chang CF, Huang CY, Yang CT, Kuo CS, Fang YF, Hsu PC, Wu CE. Real-world Afatinib Outcomes in Advanced Non-small Cell Lung Cancer Harboring EGFR Mutations. Anticancer Res. 2022; 42:2145–57. https://doi.org/10.21873/anticanres.15697 [PubMed]
- 21. Tang YJ, Chang JW, Chang CF, Huang CY, Yang CT, Kuo CS, Fang YF, Hsu PC, Wu CE. Impact of T790M Mutation Status on Later-Line Osimertinib Treatment in Non-Small Cell Lung Cancer Patients. Cancers (Basel). 2022; 14:5095. https://doi.org/10.3390/cancers14205095 [PubMed]
- 22. Chang JW, Chang CF, Huang CY, Yang CT, Kuo CS, Fang YF, Hsu PC, Wu CE. The survival after discontinuation of EGFR-TKIs due to intolerable adverse events in patients with EGFR-mutated non-small cell lung cancer. Thorac Cancer. 2023; 14:348–56. https://doi.org/10.1111/1759-7714.14674 [PubMed]