



Introduction
Lung cancer is a major contributor to cancer-related deaths worldwide [1]. Specifically, non-Small Cell Lung Cancer (NSCLC) accounts for approximately 85.0% of all new lung cancer cases, [2] with roughly 30% of these NSCLC patients being diagnosed with stage III disease [3, 4]. Stage III NSCLC encompasses a diverse range of diseases, [5] resulting in a variety of treatment approaches [6–11]. Currently, the standard treatment for unresectable epidermal growth factor receptor (EGFR) wild-type cases is concurrent chemoradiotherapy (CCRT) plus adjuvant durvalumab [12–15]. However, for EGFR-mutated patients, adjuvant durvalumab is not recommended, and CCRT remains the standard care.
Despite its status as the standard treatment, several studies have reported that CCRT may lead to poorer survival outcomes in EGFR-mutated patients [16, 17]. Conversely, in clinical practice, EGFR-tyrosine kinase inhibitor (TKI) is often recommended for stage III cases based on survival data from trials designed for stage IV EGFR-mutated NSCLC [18–24]. To date, the optimal treatment strategy for unresectable stage III EGFR-mutated NSCLC patients remains unclear. Therefore, this study aims to investigate the treatment patterns and survival rates in this specific patient population.
Results
Patient characteristics
The selection process of patients is visually represented in Figure 1. Out of the 5,477 patients tested for EGFR status, 88 were deemed eligible for the study. A comprehensive summary of these patients’ characteristics can be found in Table 1. Notably, the median follow-up time for these patients was 19 months, with an interquartile range of 11-29 months.
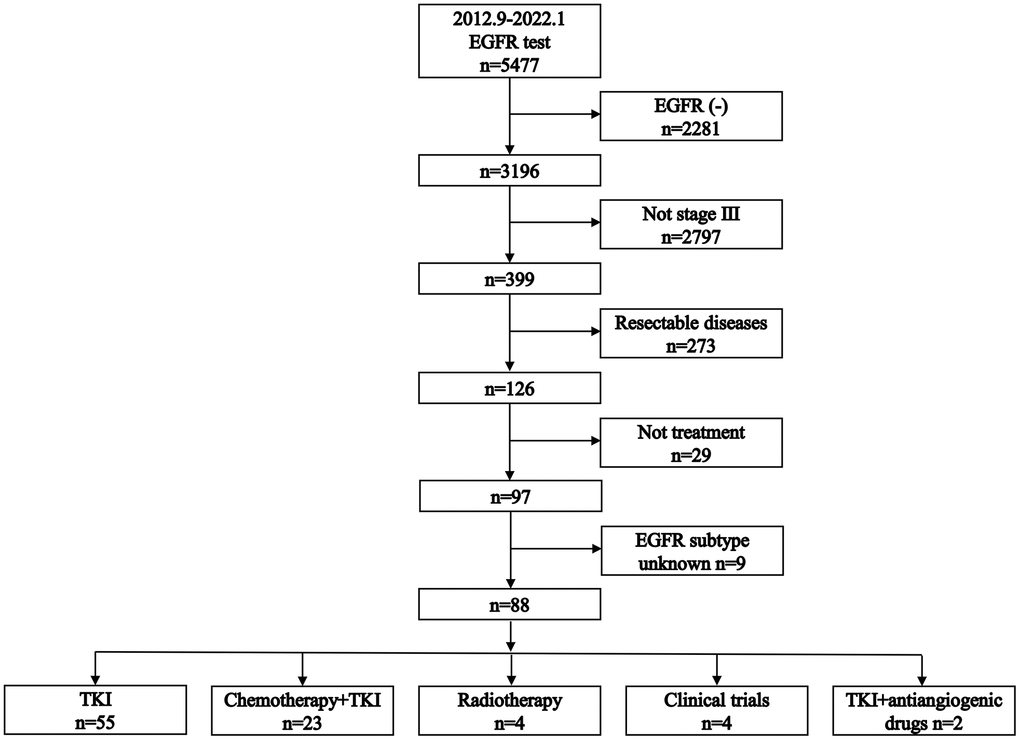
Figure 1. Flowchart of patient selection process.
Table 1. Patient characteristics.
| Characteristics | Total (n=88) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age (year) median (IQR) | 63 (54-70) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | 42 (47.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 46 (52.3%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 4 (4.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 19 (21.6%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | 65 (73.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | 44 (50.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 43 (48.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≥2 | 1 (1.1%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | 20 (22.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 32 (36.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 15 (17.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 21 (23.9%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | 2 (2.2%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 3 (3.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 32 (36.4%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 51 (58.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AJCC stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIa | 22 (25.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIb | 51 (58.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIc | 15 (17.0%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR mutation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | 49 (55.7%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R mutation | 33 (37.5%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 6 (6.8%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IQR, interquartile range; ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer; EGFR, epidermal growth factor receptor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Treatment patterns
The various treatment approaches administered to the patients are detailed in Figure 2. Overall, 62.5% of the patients received TKI alone, while 26.1% received TKI+chemotherapy. Radiotherapy was administered to 4.5% of the patients, 4.5% participated in clinical trials, and 2.4% received a regimen consisting of TKI+antiangiogenic drugs.
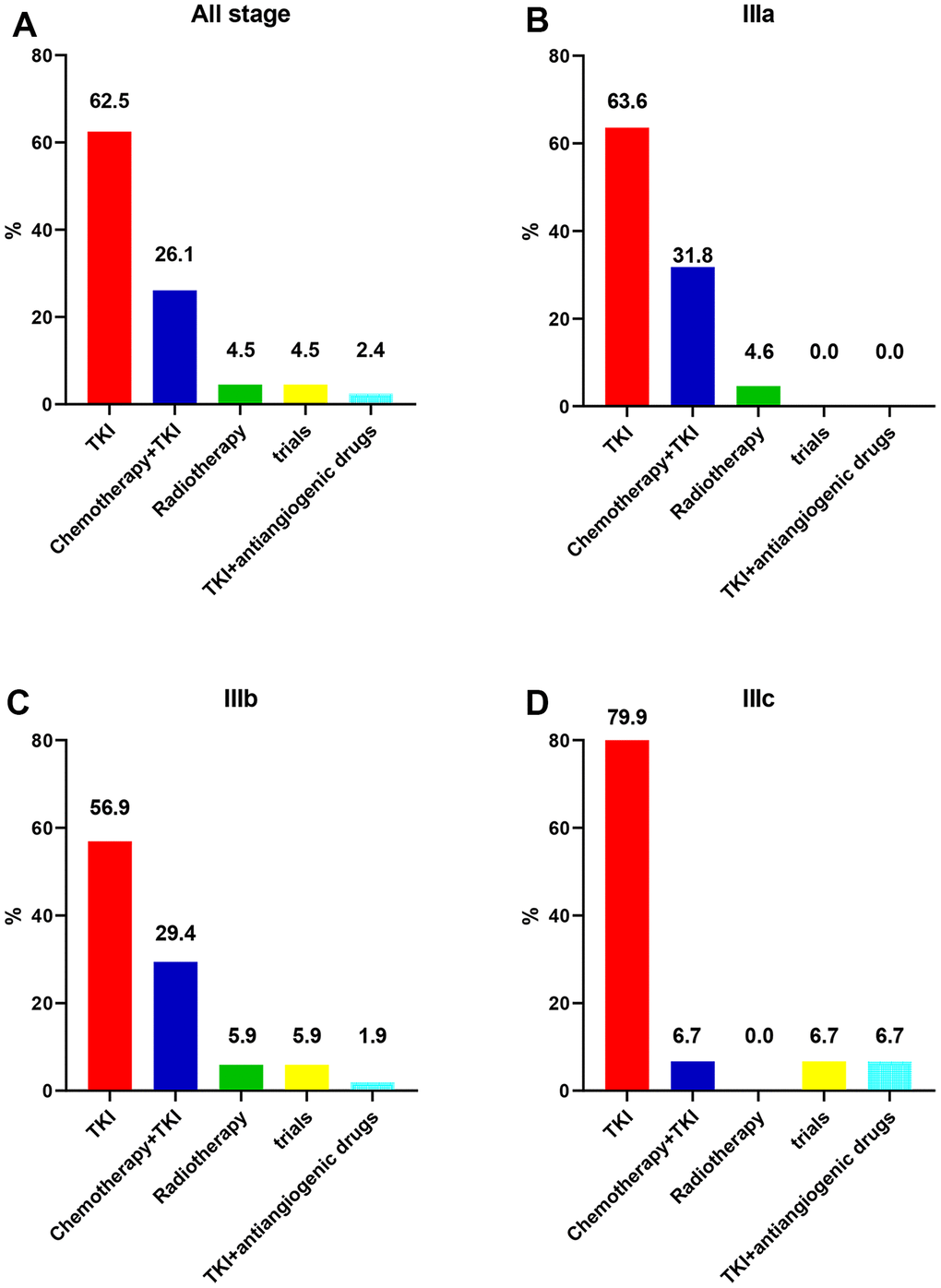
Figure 2. Initial treatment patterns for unresectable stage III EGFR-mutated non-small cell lung cancer. (A) Stage III. (B) Stage IIIa. (C) Stage IIIb. (D) Stage IIIc.
Due to the small numbers of patients in the radiotherapy, antiangiogenic therapy, and clinical trials subgroups, the survival analysis primarily compared the outcomes between the TKI alone group and the TKI+chemotherapy group. The specific characteristics of patients in these two subgroups before and after PSM are detailed in Table 2.
Table 2. Patient characteristics between TKI alone and TKI+chemotherapy groups.
| The unmatched cohort | P | The PSM cohort | P | |||
| TKI alone (n=55) | TKI+chemotherapy (n=23) | TKI alone (n=20) | TKI+chemotherapy (n=20) | |||
| Age (year) | 0.019 | 0.999 | ||||
| ≤63 | 23 (41.8%) | 17 (73.9%) | 13 (65.0%) | 14 (70.0%) | ||
| >63 | 32 (58.2%) | 6 (26.1%) | 7 (35.0%) | 6 (30.0%) | ||
| Sex | 0.005 | 0.740 | ||||
| Male | 20 (36.4%) | 17 (73.9%) | 12 (60.0%) | 14 (70.0%) | ||
| Female | 35 (63.6%) | 6 (26.1%) | 8 (40.0%) | 6 (30.0%) | ||
| Smoking status | 0.064 | 0.780 | ||||
| Current smoker | 1 (1.8%) | 3 (13.0%) | 1 (5.0%) | 3 (15.0%) | ||
| Former smoker | 10 (18.2%) | 6 (26.1%) | 5 (25.0%) | 4 (20.0%) | ||
| Never smoker | 44 (80.0%) | 14 (60.9%) | 14 (70.0%) | 13 (65.0%) | ||
| ECOG | 0.954 | 0.999 | ||||
| 0 | 29 (52.7%) | 13 (56.5%) | 11 (55.0%) | 11 (55.0%) | ||
| 1 | 26 (47.3%) | 10 (43.5%) | 9 (45.0%) | 9 (45.0%) | ||
| T stage | 0.012 | 0.382 | ||||
| T1 | 9 (16.4%) | 9 (39.1%) | 6 (30.0%) | 9 (45.0%) | ||
| T2 | 19 (34.5%) | 10 (43.5%) | 12 (60.0%) | 7 (35.0%) | ||
| T3 | 13 (23.6%) | 0 (0.0%) | / | / | ||
| T4 | 14 (25.5%) | 4 (17.4%) | 2 (10.0%) | 4 (20.0%) | ||
| N stage | 0.821 | 0.341 | ||||
| N0 | 2 (3.7%) | 0 (0.0%) | / | / | ||
| N1 | 1 (1.8%) | 1 (4.3%) | 0 (0.0%) | 1 (5.0%) | ||
| N2 | 22 (40.0%) | 8 (34.8%) | 11 (55.0%) | 7 (35.0%) | ||
| N3 | 30 (54.5%) | 14 (60.9%) | 9 (45.0%) | 12 (60.0%) | ||
| AJCC stage | 0.181 | 0.514 | ||||
| IIIa | 14 (25.5%) | 7 (30.4%) | 9 (45.0%) | 6 (30.0%) | ||
| IIIb | 29 (52.7%) | 15 (65.2%) | 11 (55.0%) | 13 (65.0%) | ||
| IIIc | 12 (21.8%) | 1 (4.4%) | 0 (0.0%) | 1 (5.0%) | ||
| EGFR mutation | 0.373 | 0.715 | ||||
| Exon 19 deletion | 28 (50.9%) | 16 (69.6%) | 14 (70.0%) | 16 (80.0%) | ||
| L858R mutation | 22 (40.0%) | 6 (26.1%) | 6 (30.0%) | 4 (20.0%) | ||
| Other | 5 (9.1%) | 1 (4.3%) | / | / | ||
PFS
In the unmatched cohort, the median PFS for the TKI alone group was 17 months, compared to 11 months for the TKI plus chemotherapy group (Figure 3A). The 1-year PFS rates were 62.8% and 41.6%, respectively, for the two groups. Similarly, the 2-year PFS rates were 41.3% and 31.2%, respectively. The univariable regression analysis revealed no statistically significant difference in PFS between the two groups (HR = 1.56, 95% CI: 0.87-2.80; P = 0.134; Table 3). Furthermore, multivariable Cox regression analysis confirmed that TKI+chemotherapy was not an independent prognostic factor for PFS (HR = 1.47, 95% CI: 0.73-2.97; P = 0.276; Table 3).
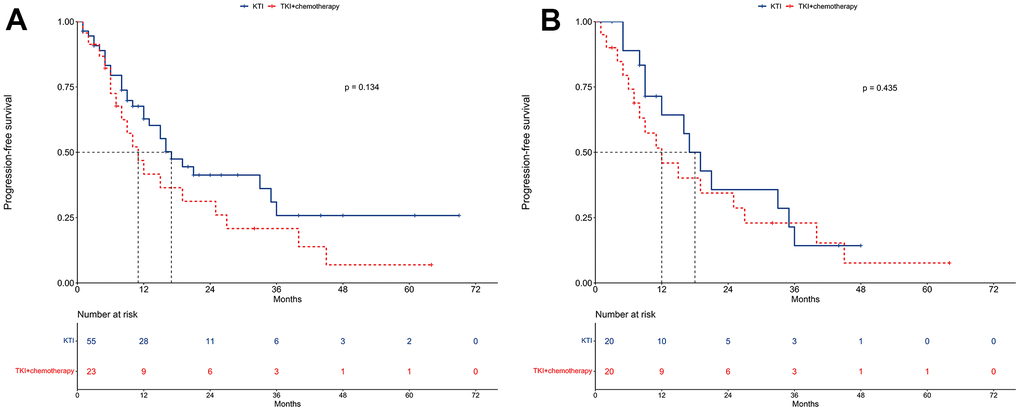
Figure 3. Progression-free survival between TKI alone and TKI+chemotherapy groups. (A) The unmatched cohort. (B) The propensity score matching cohort.
Table 3. Univariable and multivariable Cox regressions of progression-free survival.
| Univariable analysis | Multivariable analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤63 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63 | 0.54 | 0.30-0.97 | 0.043 | 0.54 | 0.25-1.13 | 0.099 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 0.87 | 0.49-1.54 | 0.633 | 0.67 | 0.30-1.46 | 0.306 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 0.77 | 0.36-1.66 | 0.510 | 0.54 | 0.18-1.53 | 0.235 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 2.21 | 0.52-9.41 | 0.284 | 1.83 | 0.08-3.66 | 0.534 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 0.66 | 0.36-1.18 | 0.158 | 0.58 | 0.26-1.25 | 0.160 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 1.31 | 0.61-2.83 | 0.493 | 1.54 | 0.69-3.53 | 0.295 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 1.14 | 0.54-3.00 | 0.796 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 1.87 | 0.79-4.43 | 0.155 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 4.17 | 0.38-46.25 | 0.245 | 7.96 | 0.49-142.27 | 0.144 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 1.52 | 0.20-11.43 | 0.684 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 1.73 | 0.23-12.80 | 0.591 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AJCC stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIa | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIb | 1.10 | 0.57-2.11 | 0.775 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIc | 1.47 | 0.62-3.53 | 0.384 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR mutation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R mutation | 0.83 | 0.44-1.55 | 0.549 | 0.99 | 0.48-2.13 | 0.977 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.53 | 0.13-2.24 | 0.298 | 0.54 | 0.10-2.86 | 0.468 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatments | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI+chemotherapy | 1.56 | 0.87-2.80 | 0.134 | 1.47 | 0.73-2.97 | 0.276 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer; TKI, tyrosine kinase inhibitor; EGFR, epidermal growth factor receptor; HR, hazard ratio; CI, confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the PSM cohort, the median PFS for the TKI alone group and the TKI+chemotherapy group was 18 months and 12 months, respectively (Figure 3B). The corresponding 1-year PFS rates were 64.3% and 45.9%, while the 2-year PFS rates were 35.7% and 34.4%.
OS
In the unmatched cohort, the median OS was 29 months for the TKI alone group and 28 months for the TKI+chemotherapy group (Figure 4A). The 1-year OS rates were 77.7% and 82.0%, respectively, for the two groups, while the 2-year OS rates were 63.7% and 63.2%. According to the univariable regression analysis, no significant difference in OS was observed between the two groups (HR = 1.12, 95% CI: 0.59-2.13; P = 0.733; Table 4). Furthermore, the multivariable Cox regression analysis also supported this finding by showing that TKI+chemotherapy was not an independent prognostic factor for OS (HR = 1.57, 95% CI: 0.69-3.54; P = 0.280; Table 4).
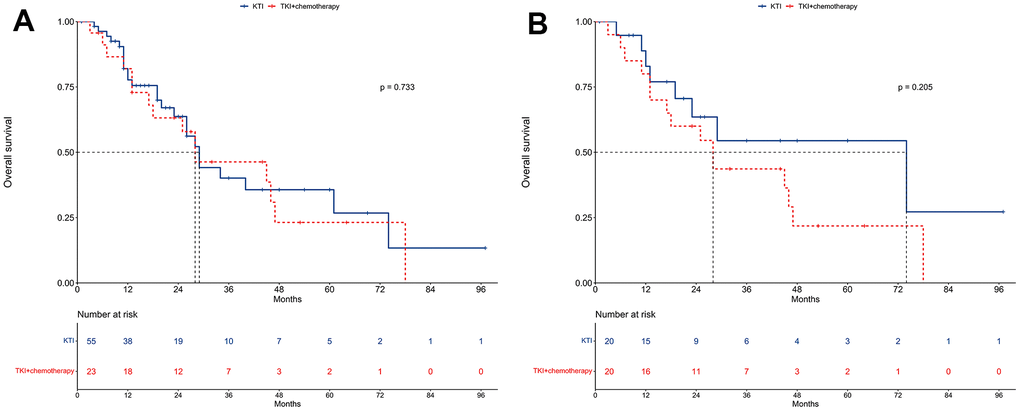
Figure 4. Overall survival between TKI alone and TKI+chemotherapy groups. (A) The unmatched cohort. (B) The propensity score matching cohort.
Table 4. Univariable and multivariable Cox regressions of overall survival.
| Univariable analysis | Multivariable analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤63 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63 | 1.35 | 0.72-2.55 | 0.347 | 2.09 | 0.93-4.68 | 0.073 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 1.13 | 0.59-2.14 | 0.715 | 1.38 | 0.56-2.03 | 0.477 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 0.72 | 0.28-1.86 | 0.496 | 0.46 | 0.10-2.05 | 0.307 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 6.62 | 2.15-20.41 | 0.001 | 10.19 | 2.15-48.33 | 0.003 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 0.76 | 0.39-1.45 | 0.400 | 0.88 | 0.38-2.03 | 0.761 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 0.85 | 0.35-2.10 | 0.729 | 0.73 | 0.28-1.93 | 0.526 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 1.53 | 0.55-4.29 | 0.416 | 21.60 | 1.78-262.79 | 0.016 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 1.93 | 0.76-4.87 | 0.164 | 24.34 | 1.48-400.73 | 0.026 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 1.42 | 0.09-22.97 | 0.804 | 0.18 | 0.01-4.34 | 0.287 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 0.73 | 0.09-5.57 | 0.758 | 4.68 | 0.17-126.98 | 0.359 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 0.85 | 0.11-6.42 | 0.878 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AJCC stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIa | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIb | 1.86 | 0.86-4.03 | 0.114 | 0.14 | 0.01-2.43 | 0.177 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIc | 1.71 | 0.61-4.94 | 0.302 | 0.02 | 0.01-1.18 | 0.058 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR mutation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R mutation | 1.04 | 0.53-2.04 | 0.912 | 1.24 | 0.52-2.95 | 0.630 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.41 | 0.06-3.00 | 0.390 | 0.24 | 0.03-2.35 | 0.222 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatments | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI+chemotherapy | 1.12 | 0.59-2.13 | 0.733 | 1.57 | 0.69-3.54 | 0.280 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer; TKI, tyrosine kinase inhibitor; EGFR, epidermal growth factor receptor; HR, hazard ratio; CI, confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the PSM cohort, the median OS was 74 months for the TKI alone group and 28 months for the TKI+chemotherapy group (Figure 4B). The 1-year OS was 82.9% and 80.0%, respectively, for these two groups, while the 2-year OS was 63.5% and 60.0%, respectively.
LRFS
In the unmatched cohort, the median LRFS for the TKI alone group was 21 months, compared to 11 months for the TKI+chemotherapy group (Figure 5A). The 1-year LRFS rates were 69.9% and 44.2%, and the 2-year LRFS rates were 45.4% and 33.1%, respectively for the two groups. The univariable regression analysis did not reveal any significant differences in LRFS between the two treatment approaches (HR = 1.46, 95% CI: 0.75-2.81; P = 0.267; Table 5). Additionally, the multivariable Cox regression analysis further solidified that TKI+chemotherapy was not an independent prognosticator for LRFS (HR = 1.32, 95% CI: 0.58-2.79; P = 0.547; Table 5).
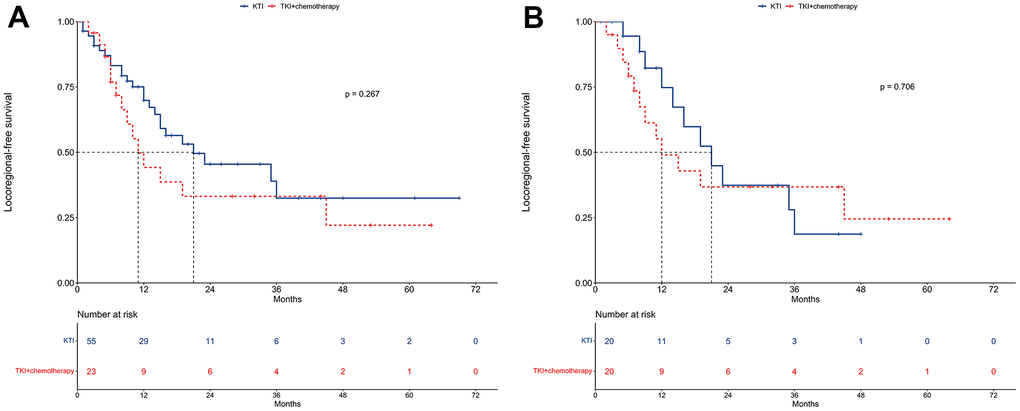
Figure 5. Locoregional-free survival between TKI alone and TKI+chemotherapy groups. (A) The unmatched cohort. (B) The propensity score matching cohort.
Table 5. Univariable and multivariable Cox regressions of locoregional-free survival.
| Univariable analysis | Multivariable analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤63 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63 | 0.54 | 0.28-1.04 | 0.065 | 0.61 | 0.20-1.07 | 0.070 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 0.74 | 0.40-1.40 | 0.360 | 0.46 | 0.18-1.10 | 0.081 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 0.76 | 0.32-1.81 | 0.531 | 0.45 | 0.11-1.33 | 0.132 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 2.78 | 0.64-12.01 | 0.172 | 1.26 | 0.12-5.44 | 0.815 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 0.63 | 0.33-1.22 | 0.169 | 0.55 | 0.23-1.31 | 0.175 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 1.53 | 0.63-3.73 | 0.348 | 1.65 | 0.68-4.42 | 0.245 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 1.18 | 0.37-3.74 | 0.778 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 2.31 | 0.88-6.04 | 0.089 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 2.05 | 0.13-32.86 | 0.613 | 4.18 | 0.17-113.51 | 0.374 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 1.43 | 0.19-10.84 | 0.729 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 1.45 | 0.19-10.79 | 0.719 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AJCC stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIa | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIb | 1.07 | 0.51-2.21 | 0.863 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIc | 1.57 | 0.60-4.07 | 0.356 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR mutation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R mutation | 1.01 | 0.51-1.99 | 0.979 | 1.41 | 0.63-3.26 | 0.387 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 0.75 | 0.18-3.20 | 0.699 | 1.10 | 0.16-5.07 | 0.915 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatments | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI+chemotherapy | 1.46 | 0.75-2.81 | 0.267 | 1.32 | 0.58-2.79 | 0.547 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer; TKI, tyrosine kinase inhibitor; EGFR, epidermal growth factor receptor; HR, hazard ratio; CI, confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the PSM cohort, the median LRFS for the TKI alone group was 75 months, compared to 49 months for the TKI+chemotherapy group (Figure 5B). The respective 1-year LRFS rates were 74.7% and 49.0%, while the 2-year LRFS rates were 37.4% and 36.8%.
DMFS
In the unmatched cohort, the median DMFS was not reached for the TKI alone group, while it was 25 months for the TKI+chemotherapy group (Figure 6A). The 1-year DMFS rates were 82.0% and 60.8%, and the 2-year DMFS rates were 70.7% and 54.7%, respectively for the two groups. The univariable regression analysis indicated a decreased DMFS with TKI+chemotherapy compared to TKI alone (HR = 2.39, 95% CI: 1.11-5.18; P = 0.022; Table 6). However, upon conducting a multivariable Cox regression analysis, TKI+chemotherapy did not emerge as an independent prognostic factor for DMFS (HR = 4.07, 95% CI: 0.97-6.22; P = 0.057; Table 6).
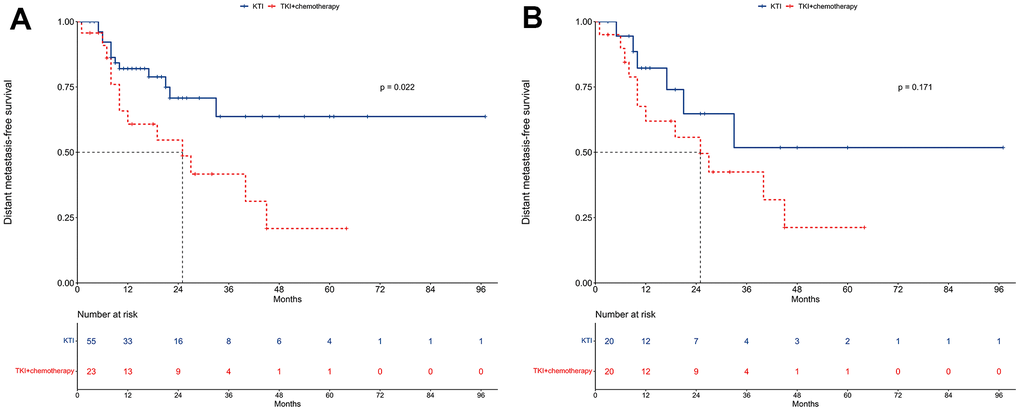
Figure 6. Distant metastasis-free survival between TKI alone and TKI+chemotherapy groups. (A) The unmatched cohort. (B) The propensity score matching cohort.
Table 6. Univariable and multivariable Cox regressions of distant metastasis-free survival.
| Univariable analysis | Multivariable analysis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HR | 95% CI | P | HR | 95% CI | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ≤63 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| >63 | 0.37 | 0.15-0.87 | 0.024 | 1.98 | 0.72-5.20 | 0.192 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sex | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Male | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Female | 1.20 | 0.55-2.63 | 0.639 | 1.33 | 0.42-4.02 | 0.644 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 0.75 | 0.25-2.19 | 0.593 | 1.60 | 0.14-2.85 | 0.543 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 3.46 | 0.78-15.40 | 0.104 | 2.10 | 0.38-35.79 | 0.259 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 0.61 | 0.27-1.37 | 0.229 | 0.49 | 0.17-1.39 | 0.170 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T1 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T2 | 1.31 | 0.48-3.56 | 0.596 | 1.51 | 0.50-4.40 | 0.482 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T3 | 1.19 | 0.33-4.23 | 0.789 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| T4 | 0.97 | 0.29-3.21 | 0.959 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N0 | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N1 | 1.31 | 0.48-3.56 | 0.998 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N2 | 1.19 | 0.33-4.23 | 0.998 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| N3 | 0.97 | 0.29-3.21 | 0.998 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AJCC stage | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIa | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIb | 1.00 | 0.42-2.36 | 0.995 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIIc | 0.68 | 0.18-2.56 | 0.568 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EGFR mutation | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exon 19 deletion | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| L858R mutation | 1.05 | 0.42-2.16 | 0.913 | 1.17 | 0.46-3.27 | 0.683 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Treatments | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI | reference | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI+chemotherapy | 2.39 | 1.11-5.18 | 0.022 | 4.07 | 0.97-6.22 | 0.057 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ECOG, Eastern Cooperative Oncology Group; AJCC, American Joint Committee on Cancer; TKI, tyrosine kinase inhibitor; EGFR, epidermal growth factor receptor; HR, hazard ratio; CI, confidence interval. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In the PSM cohort, similar trends were observed with median DMFS not being reached for the TKI alone group and being 25 months for the TKI+chemotherapy group (Figure 6B). For the TKI alone and TKI+chemotherapy groups, the respective 1-year DMFS rates were 82.2% and 61.9%, while the respective 2-year DMFS rates were 64.7% and 55.7%.
Adverse events
A comprehensive overview of the adverse events is presented in Table 7. The TKI+chemotherapy group was associated with a higher occurrence of hematological events compared to TKI alone group. Specifically, a higher incidence of leukopenia (Grade 1-2: 52.2% vs. 5.5%, P < 0.001), neutropenia (Grade 1-2: 56.5% vs. 5.5%, P < 0.001), anemia (Grade 1-2: 17.4% vs. 3.6%, P = 0.038), and thrombocytopenia (Grade 1-2: 13.0% vs. 0.0%, P = 0.006) was observed in the TKI+chemotherapy group.
Table 7. Adverse events between TKI alone and TKI+chemotherapy groups.
| Grade 1-2 | P | Grade 3-4 | P | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI alone (n=55) | TKI+chemotherapy (n=23) | TKI alone (n=55) | TKI+chemotherapy (n=23) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hematological events | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leukopenia | <0.001 | 0.006 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 52 (94.5%) | 11 (47.8%) | 55 (100.0%) | 20 (87.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 3 (5.5%) | 12 (52.2%) | 0 (0.0%) | 3 (13.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Neutropenia | <0.001 | 0.027 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 52 (94.5%) | 10 (43.5%) | 55 (100.0%) | 21 (91.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 3 (5.5%) | 13 (56.5%) | 0 (0.0%) | 2 (8.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anemia | 0.038 | 0.295 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 53 (96.4%) | 19 (82.6%) | 55 (100.0%) | 22 (95.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 2 (3.6%) | 4 (17.4%) | 0 (0.0%) | 1 (4.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thrombocytopenia | 0.006 | 0.999 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 55 (100.0%) | 20 (43.5%) | 55 (100.0%) | 23 (100.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 0 (0.0%) | 3 (13.0%) | 0 (0.0%) | 0 (0.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-hematological events | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver dysfunction | 0.540 | 0.999 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 45 (81.8%) | 17 (73.9%) | 55 (100.0%) | 23 (100.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 10 (18.2%) | 6 (26.1%) | 0 (0.0%) | 0 (0.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Rash or acne | 0.805 | 0.999 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 29 (52.7%) | 11 (47.8%) | 51 (92.7%) | 21 (91.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 26 (47.3%) | 12 (52.2%) | 4 (7.3%) | 2 (8.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diarrhea | 0.805 | 0.999 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 33 (60.0%) | 13 (56.5%) | 53 (96.4%) | 22 (95.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 22 (40.0%) | 10 (43.5%) | 2 (3.6%) | 1 (4.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Vomiting | 0.258 | 0.295 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 49 (89.1%) | 18 (78.3%) | 55 (100.0%) | 22 (95.7%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 6 (10.9%) | 5 (21.7%) | 0 (0.0%) | 1 (4.3%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nail changes | 0.999 | 0.999 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| no | 47 (85.5%) | 20 (87.0%) | 54 (98.2%) | 23 (100.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| yes | 8 (14.5%) | 3 (13.0%) | 1 (1.8%) | 0 (0.0%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TKI, tyrosine kinase inhibitor. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Moreover, a higher prevalence of Grade 3-4 leukopenia (13.0% vs. 0.0%, P = 0.006) and neutropenia (8.7% vs. 0.0%, P = 0.027) was noted among patients receiving TKI+chemotherapy. In contrast, non-hematological events did not show any significant differences between the TKI alone and TKI plus chemotherapy groups (all P > 0.05).
Discussion
The findings of this study revealed two important insights. Firstly, it highlighted the prevailing trend in clinical practice where the majority of patients with unresectable stage III EGFR-mutated NSCLC were primarily treated with TKI monotherapy, as opposed to chemoradiotherapy. Secondly, our data suggested that the addition of chemotherapy to TKI therapy as an initial treatment strategy did not provide survival benefits over TKI alone.
The current standard of care for unresectable stage III EGFR-mutated NSCLC patients is CCRT [6–11]. Surprisingly, our study found that only a small proportion (4.5%) of patients received radiotherapy, while a significant majority (91.0%) were initially treated with TKI. There could be several explanations for this observation. One possible explanation was the evidence from various clinical trials that have demonstrated the efficacy of TKI as a standard treatment for stage IV EGFR-mutated NSCLC patients [18–24]. These trials had also included a subset of stage III patients, who achieved superior PFS with TKI monotherapy compared to CCRT [16, 17]. Another explanation could be the lack of difference in OS (HR = 0.71, 95% CI: 0.34-1.47) and cancer-specific survival (HR = 0.65, 95% CI: 0.31-1.35) between TKI monotherapy and CCRT, as reported in a previous study [25]. Additionally, the absence of radiation oncologists in defining treatment strategies could also contribute to the low utilization of radiotherapy [26].
While TKI monotherapy has shown better PFS than CCRT, it is crucial to recognize that it is not a curative treatment. TKI alone did not improve OS for stage III patients compared to stage IV patients [27]. Moreover, patients who experienced recurrences after CCRT had the option of salvage TKI therapy, which had shown significant OS improvement [28–30]. Therefore, recommending EGFR-TKI monotherapy as the initial treatment for all stage III patients may not be appropriate.
The FLAURA2 study had emphasized the improved PFS in stage IV patients receiving TKI plus chemotherapy [31, 32]. This raises the intriguing possibility of whether similar advantages could be observed in patients with stage III disease. Currently, however, there is a paucity of evidence addressing this question directly. In our study, we observed that the median PFS was 17.0 months in the TKI alone group and 11.0 months in the TKI+chemotherapy group, with no statistically significant difference between the two groups (HR = 1.56, 95% CI: 0.87-2.80; P = 0.134). This finding was consistent with several other studies that had reached similar conclusions [25, 29, 33, 34].
While these findings contribute valuable insights, it is crucial to interpret them with caution. A majority of participants in our study (89.7%) received first-generation TKIs, which had not demonstrated improved PFS when combined with chemotherapy in stage III patients [35]. It is noteworthy that third-generation TKIs have shown greater efficacy compared to their first-generation counterparts [18–20]. Therefore, there is a compelling rationale to investigate the therapeutic potential of combining third-generation TKIs with chemotherapy in stage III EGFR-mutated NSCLC patients.
It is important to acknowledge the limitations of our study. The retrospective design inherently results in potential confounders, such as age, sex, and T stage, being imbalanced between the treatment groups. Although we attempted to account for these factors through multivariable analysis and PSM, the possibility of unmeasured confounders remains. Moreover, the relatively small sample size of the TKI+chemotherapy group may have limited our ability to detect subtle differences in survival outcomes between the two treatment strategies.
In conclusion, our findings suggested that the addition of chemotherapy to TKI therapy did not improve survival outcomes in unresectable stage III EGFR-mutated NSCLC patients compared to TKI alone. However, given the limitations of our study, including its small sample size, these results should be interpreted cautiously. Larger prospective studies and clinical trials are essential to validate these findings and provide more definitive guidance on the optimal treatment approach for these patients.
Materials and Methods
Patient selection
We conducted a comprehensive search to identify NSCLC patients at Guangxi Medical University Cancer Hospital between September 2012 and January 2022. The inclusion criteria for patient selection were as follows: (1) histologically or cytologically confirmed NSCLC, (2) EGFR testing performed and mutation confirmed, (3) definitive EGFR subtypes identified for the EGFR mutation, (4) staging according to the 8th edition of the American Joint Committee on Cancer (AJCC) criteria confirming stage III disease, and (5) presence of unresectable disease. Patients meeting any of the following criteria were excluded from the study: (1) those who did not receive any treatment, (2) patients who underwent surgery as their initial treatment modality, and (3) individuals with incomplete or missing clinical information.
Endpoint
The primary endpoint of the study was progression-free survival (PFS). The secondary endpoints included overall survival (OS), locoregional-free survival (LRFS), and distant metastasis-free survival (DMFS).
Statistical analysis
The continuous factor of age was transformed to categorical factor according to the median value. Categorical variables were assessed using the χ2 test or Fisher’s exact test. To compare PFS, OS, LRFS, and DMFS across different treatment modalities, the Kaplan-Meier method coupled with log-rank test statistics was utilized. Univariable regression analysis was performed to pinpoint potential prognostic indicators. Furthermore, multivariable Cox regression analysis was conducted to identify independent prognostic factors after adjusting for variables. The results were presented in terms of hazard ratios (HRs) along with corresponding 95% confidence intervals (CIs).
To minimize the impact of selection bias when comparing outcomes between different treatment modalities, a matched case-control analysis via propensity score matching (PSM) was executed. During the calculation of propensity scores, one-to-one matching without replacement was achieved within a logistic regression model. The nearest-neighbor matching algorithm based on the propensity score was applied for factors with a caliper of 0.8 on the logistic regression model.
The statistical analyses for this study were carried out using SPSS Statistics Version 26.0 software (IBM Co., Armonk, NY, USA) and R software (version 4.2.1). A two-tailed P-value of less than 0.05 was deemed statistically significant.
Data availability statement
The data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Author Contributions
Conceptualization: Xin-Bin Pan; Methodology: Huan-Wei Liang; Formal Analysis: Yang Liu; Investigation: Yang Liu; Resources: Huan-Wei Liang; Validation: Huan-Wei Liang and Yang Liu; Writing-Original Draft Preparation: Huan-Wei Liang; Writing-Review and Editing: Xin-Bin Pan.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement
The ethical approval and consent were waived by the Ethics Committee and Institutional Review Board of Guangxi Medical University Cancer Hospital due to the retrospective nature of this study.
Funding
No funding was provided for this study.
References
- 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71:209–49. https://doi.org/10.3322/caac.21660 [PubMed]
- 2. McKeage MJ, Jameson MB, and AS1404-201 Study Group Investigators. Comparative outcomes of squamous and non-squamous non-small cell lung cancer (NSCLC) patients in phase II studies of ASA404 (DMXAA) - retrospective analysis of pooled data. J Thorac Dis. 2010; 2:199–204. https://doi.org/10.3978/j.issn.2072-1439.2010.02.04.1 [PubMed]
- 3. Aupérin A, Le Péchoux C, Rolland E, Curran WJ, Furuse K, Fournel P, Belderbos J, Clamon G, Ulutin HC, Paulus R, Yamanaka T, Bozonnat MC, Uitterhoeve A, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010; 28:2181–90. https://doi.org/10.1200/JCO.2009.26.2543 [PubMed]
- 4. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, Nicholson AG, Groome P, Mitchell A, Bolejack V, International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions, and International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee Advisory Boards and Participating Institutions. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016; 11:39–51. https://doi.org/10.1016/j.jtho.2015.09.009 [PubMed]
- 5. Huber RM, De Ruysscher D, Hoffmann H, Reu S, Tufman A. Interdisciplinary multimodality management of stage III nonsmall cell lung cancer. Eur Respir Rev. 2019; 28:190024. https://doi.org/10.1183/16000617.0024-2019 [PubMed]
- 6. Postmus PE, Kerr KM, Oudkerk M, Senan S, Waller DA, Vansteenkiste J, Escriu C, Peters S, and ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017; 28:iv1–21. https://doi.org/10.1093/annonc/mdx222 [PubMed]
- 7. Miller ED, Fisher JL, Haglund KE, Grecula JC, Xu-Welliver M, Bertino EM, He K, Shields PG, Carbone DP, Williams TM, Otterson GA, Bazan JG. The Addition of Chemotherapy to Radiation Therapy Improves Survival in Elderly Patients with Stage III Non-Small Cell Lung Cancer. J Thorac Oncol. 2018; 13:426–35. https://doi.org/10.1016/j.jtho.2017.11.135 [PubMed]
- 8. Davidoff AJ, Gardner JF, Seal B, Edelman MJ. Population-based estimates of survival benefit associated with combined modality therapy in elderly patients with locally advanced non-small cell lung cancer. J Thorac Oncol. 2011; 6:934–41. https://doi.org/10.1097/JTO.0b013e31820eed00 [PubMed]
- 9. Curran WJ
Jr , Paulus R, Langer CJ, Komaki R, Lee JS, Hauser S, Movsas B, Wasserman T, Rosenthal SA, Gore E, Machtay M, Sause W, Cox JD. Sequential vs. concurrent chemoradiation for stage III non-small cell lung cancer: randomized phase III trial RTOG 9410. J Natl Cancer Inst. 2011; 103:1452–60. https://doi.org/10.1093/jnci/djr325 [PubMed] - 10. Bradley JD, Paulus R, Komaki R, Masters G, Blumenschein G, Schild S, Bogart J, Hu C, Forster K, Magliocco A, Kavadi V, Garces YI, Narayan S, et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015; 16:187–99. https://doi.org/10.1016/S1470-2045(14)71207-0 [PubMed]
- 11. Yoon SM, Shaikh T, Hallman M. Therapeutic management options for stage III non-small cell lung cancer. World J Clin Oncol. 2017; 8:1–20. https://doi.org/10.5306/wjco.v8.i1.1 [PubMed]
- 12. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M, Cho BC, Bourhaba M, Quantin X, et al, and PACIFIC Investigators. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N Engl J Med. 2017; 377:1919–29. https://doi.org/10.1056/NEJMoa1709937 [PubMed]
- 13. Spigel DR, Faivre-Finn C, Gray JE, Vicente D, Planchard D, Paz-Ares L, Vansteenkiste JF, Garassino MC, Hui R, Quantin X, Rimner A, Wu YL, Özgüroğlu M, et al. Five-Year Survival Outcomes From the PACIFIC Trial: Durvalumab After Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. J Clin Oncol. 2022; 40:1301–11. https://doi.org/10.1200/JCO.21.01308 [PubMed]
- 14. Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, Kurata T, Chiappori A, Lee KH, de Wit M, Cho BC, Bourhaba M, Quantin X, et al, and PACIFIC Investigators. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N Engl J Med. 2018; 379:2342–50. https://doi.org/10.1056/NEJMoa1809697 [PubMed]
- 15. Gray JE, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, Kurata T, Chiappori A, Lee KH, Cho BC, Planchard D, Paz-Ares L, Faivre-Finn C, et al. Three-Year Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC-Update from PACIFIC. J Thorac Oncol. 2020; 15:288–93. https://doi.org/10.1016/j.jtho.2019.10.002 [PubMed]
- 16. Park SE, Noh JM, Kim YJ, Lee HS, Cho JH, Lim SW, Ahn YC, Pyo H, Choi YL, Han J, Sun JM, Lee SH, Ahn JS, et al. EGFR Mutation Is Associated with Short Progression-Free Survival in Patients with Stage III Non-squamous Cell Lung Cancer Treated with Concurrent Chemoradiotherapy. Cancer Res Treat. 2019; 51:493–501. https://doi.org/10.4143/crt.2018.125 [PubMed]
- 17. Ishihara M, Igawa S, Sasaki J, Otani S, Fukui T, Ryuge S, Katono K, Hiyoshi Y, Kasajima M, Mitsufuji H, Kubota M, Yokoba M, Katagiri M, et al. Evaluation of concurrent chemoradiotherapy for locally advanced NSCLC according to EGFR mutation status. Oncol Lett. 2017; 14:885–90. https://doi.org/10.3892/ol.2017.6231 [PubMed]
- 18. Lu S, Dong X, Jian H, Chen J, Chen G, Sun Y, Ji Y, Wang Z, Shi J, Lu J, Chen S, Lv D, Zhang G, et al. AENEAS: A Randomized Phase III Trial of Aumolertinib Versus Gefitinib as First-Line Therapy for Locally Advanced or MetastaticNon-Small-Cell Lung Cancer With EGFR Exon 19 Deletion or L858R Mutations. J Clin Oncol. 2022; 40:3162–71. https://doi.org/10.1200/JCO.21.02641 [PubMed]
- 19. Shi Y, Chen G, Wang X, Liu Y, Wu L, Hao Y, Liu C, Zhu S, Zhang X, Li Y, Liu J, Cao L, Cheng Y, et al, and FURLONG investigators. Furmonertinib (AST2818) versus gefitinib as first-line therapy for Chinese patients with locally advanced or metastatic EGFR mutation-positive non-small-cell lung cancer (FURLONG): a multicentre, double-blind, randomised phase 3 study. Lancet Respir Med. 2022; 10:1019–28. https://doi.org/10.1016/S2213-2600(22)00168-0 [PubMed]
- 20. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A, Imamura F, Nogami N, Kurata T, Okamoto I, Zhou C, Cho BC, et al, and FLAURA Investigators. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018; 378:113–25. https://doi.org/10.1056/NEJMoa1713137 [PubMed]
- 21. Wu YL, Cheng Y, Zhou X, Lee KH, Nakagawa K, Niho S, Tsuji F, Linke R, Rosell R, Corral J, Migliorino MR, Pluzanski A, Sbar EI, et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017; 18:1454–66. https://doi.org/10.1016/S1470-2045(17)30608-3 [PubMed]
- 22. Park K, Tan EH, O’Byrne K, Zhang L, Boyer M, Mok T, Hirsh V, Yang JC, Lee KH, Lu S, Shi Y, Kim SW, Laskin J, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016; 17:577–89. https://doi.org/10.1016/S1470-2045(16)30033-X [PubMed]
- 23. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, Fujita Y, Okinaga S, Hirano H, et al, and North-East Japan Study Group. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010; 362:2380–8. https://doi.org/10.1056/NEJMoa0909530 [PubMed]
- 24. Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, Asami K, Katakami N, Takada M, et al, and West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010; 11:121–8. https://doi.org/10.1016/S1470-2045(09)70364-X [PubMed]
- 25. Hsia TC, Liang JA, Li CC, Chien CR. Comparative effectiveness of concurrent chemoradiotherapy versus EGFR-tyrosine kinase inhibitors for the treatment of clinical stage IIIb lung adenocarcinoma patients with mutant EGFR. Thorac Cancer. 2018; 9:1398–405. https://doi.org/10.1111/1759-7714.12847 [PubMed]
- 26. Van Dao T, Diep TB, Le Phuong T, Huggenberger R, Kumar A. Real-World Treatment Patterns and Clinical Outcomes in Patients With Stage III Non-Small-Cell Lung Cancer: Results of KINDLE-Vietnam Cohort. Front Oncol. 2022; 12:842296. https://doi.org/10.3389/fonc.2022.842296 [PubMed]
- 27. Liu Y, Liang HW, Pan XB. Efficacy of first-line tyrosine kinase inhibitor between unresectable stage III and stage IV EGFR-mutated non-small cell lung cancer patients. Aging (Albany NY). 2023; 15:5066–74. https://doi.org/10.18632/aging.204781 [PubMed]
- 28. Jazieh AR, Onal HC, Tan DSW, Soo RA, Prabhash K, Kumar A, Huggenberger R, Robb S, Cho BC. Real-World Treatment Patterns and Clinical Outcomes in Patients With Stage III NSCLC: Results of KINDLE, a Multicountry Observational Study. J Thorac Oncol. 2021; 16:1733–44. https://doi.org/10.1016/j.jtho.2021.05.003 [PubMed]
- 29. Su PL, Chang GC, Hsiao SH, Hsia TC, Lin MC, Lin MH, Shih JY, Yang CT, Yang SH, Chen YM. An Observational Study on Treatment Outcomes in Patients With Stage III NSCLC in Taiwan: The KINDLE Study. JTO Clin Res Rep. 2022; 3:100292. https://doi.org/10.1016/j.jtocrr.2022.100292 [PubMed]
- 30. Jazieh AR, Onal HC, Tan DS, Soo RA, Prabhash K, Kumar A, Huggenberger R, Cho BC. Real-world global data on targeting epidermal growth factor receptor mutations in stage III non-small-cell lung cancer: the results of the KINDLE study. Ther Adv Med Oncol. 2022; 14:17588359221122720. https://doi.org/10.1177/17588359221122720 [PubMed]
- 31. Asahina H, Tanaka K, Morita S, Maemondo M, Seike M, Okamoto I, Oizumi S, Kagamu H, Takahashi K, Kikuchi T, Isobe T, Sugio K, Kobayashi K. A Phase II Study of Osimertinib Combined With Platinum Plus Pemetrexed in Patients With EGFR-Mutated Advanced Non-Small-cell Lung Cancer: The OPAL Study (NEJ032C/LOGIK1801). Clin Lung Cancer. 2021; 22:147–51. https://doi.org/10.1016/j.cllc.2020.09.023 [PubMed]
- 32. Wu YL, Tsuboi M, He J, John T, Grohe C, Majem M, Goldman JW, Laktionov K, Kim SW, Kato T, Vu HV, Lu S, Lee KY, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med. 2020; 383:1711–23. https://doi.org/10.1056/NEJMoa2027071 [PubMed]
- 33. Wu R, Yu S, Ye J, Wang Y, Zhao Z, Liu H, Song Y. A Multicenter Retrospective Study on the Prognosis of Stage III Unresectable Mutant Non-Small Cell Lung Cancer With Tyrosine Kinase Inhibitors Therapy. Front Oncol. 2021; 11:692703. https://doi.org/10.3389/fonc.2021.692703 [PubMed]
- 34. Sun Y, Wu M, Zhou M, Luo X, Guo Y, Bai H, Zhang Z, Tian W, Wang X, Bai Y, Zhu X, Pan H, Deng Y, et al. Management of medically inoperable and tyrosine kinase inhibitor-naïve early-stage lung adenocarcinoma with epidermal growth factor receptor mutations: a retrospective multi-institutional analysis. BMC Cancer. 2020; 20:646. https://doi.org/10.1186/s12885-020-07122-7 [PubMed]
- 35. Xu L, Qi Q, Zhang Y, Cui J, Liu R, Li Y. Combination of icotinib and chemotherapy as first-line treatment for advanced lung adenocarcinoma in patients with sensitive EGFR mutations: A randomized controlled study. Lung Cancer. 2019; 133:23–31. https://doi.org/10.1016/j.lungcan.2019.05.008 [PubMed]