



Introduction
People around the world are living longer, so the number and proportion of people aged 60 and over in the population is growing, and this number is predicted to increase to 1.4 billion by 2030 [1, 2]. Aging is a complex phenomenon, marked by a gradual and continuous process, characterized by its wide range of dimensions and the complexity of its transformations that vary from individual to individual [3–5]. An aspect frequently experienced in old age is the gradual decrease in physical and mental capacity, which promotes a reduction in social interactions in this population, and which has the potential to significantly affect the mental health, well-being, and mood of these individuals [6–10].
Physical exercise (PE) has been investigated as an alternative to treat, prevent, and delay aging, and it has been proven that PE acts as a protective factor for chronic non-communicable diseases and in the treatment of other common diseases in aging [10–15]. In addition, several studies have demonstrated the positive effects of different types of PE on mental health, anxiety, and depression in older adults [16–20].
Furthermore, regular physical activity brings substantial benefits to older adults, acting as a protective factor against the development of mental health problems and promoting improvements in mood. Studies show that a greater investment of time in physical activities is associated with even more significant benefits [6, 21, 22].
Exergames are a new way of practicing physical exercise, leading to high adherence, and presenting considerable physiological and mental results [23–25]. Recent studies indicate that exergames are emerging as a versatile tool for interventions in various domains, due to their accessibility, low cost, and significant results [26, 27]. Other research indicates that practicing exergames can improve the mood of children and adolescents, significantly increasing vigor when practiced in a group [28–30]. In adults, an increase in happiness was observed in students and university staff when practicing individually [31], in addition to providing a lower perception of fatigue during practice among young adults when compared to traditional aerobic dance [32].
These effects may occur as a result of the mechanisms brought about by the practice of exergames, which can consequently influence mood, through engagement, social interaction when the practice is collective, and cognitive stimulation itself. Studies indicate that engagement increases experience and pleasure in the game, improves mood, and is related to a greater likelihood of wanting to practice again at another time [33–35]. In addition, social interaction is another important component of exergames, especially for older people, since the practice of exergames has been shown to improve social well-being, decrease loneliness, and increase social connection between participants, which consequently influences the improvement in mood [36]. Finally, we can consider the cognitive stimulation that occurs from exergames that combine motor and cognitive activities, which can improve cognitive functions such as memory and processing speed, also alleviating depressive symptoms [37, 38].
Exergames represent an innovative and promising alternative to traditional physical activities for older adults, offering distinct benefits in terms of adherence, accessibility, and motivation. Studies indicate that the interactive and playful nature of exergames can significantly enhance adherence to physical exercise, making it more engaging and enjoyable for this population [33, 36, 37, 39]. Additionally, the accessibility of exergames is a key factor, as they can be performed at home, eliminating barriers such as transportation and mobility limitations, which was shown to be particularly relevant during periods of social restrictions, such as the pandemic [33–35]. Thus, exergames emerge as a valuable strategy for promoting physical activity and well-being, integrating physical, cognitive, and social benefits in an accessible and effective manner.
Furthermore, recent studies indicate that participation in exergames can have positive effects in older adults, with regular practice of these games contributing to improvements in mood, increased feelings of well-being, and promoting vitality in older adults, providing a fun and stimulating way to stay active [40–42]. In this context, with the exponential growth in scientific production in various methodological approaches and the increase in clinical trials investigating the effects of exergames in older adults [26, 43–48], it becomes essential to synthesize and critically evaluate this literature, to clarify the effects of exergames on mood states and determine the best way to incorporate them into physical exercise practice for older adults. This synthesis will provide new insights for physical education and health professionals, allowing for an evidence-based approach.
With a high degree of scientific evidence, systematic reviews and meta-analyses are considered the best sources for decision-making in clinical/professional practices, and are increasingly used and cited by researchers due to the growing volume of scientific literature [49]. Thus, the aim of the current study is to analyze, through a systematic review, the impacts of exergames on the mood states of older adults.
Results
In the first stage of the database search, 651 studies were identified, of which 331 duplicates were excluded. After reading the title and abstract, 20 articles remained and were selected for full reading. At the end of the selection process, nine studies met the eligibility criteria and were selected for synthesis (Figure 1 PRISMA flowchart).
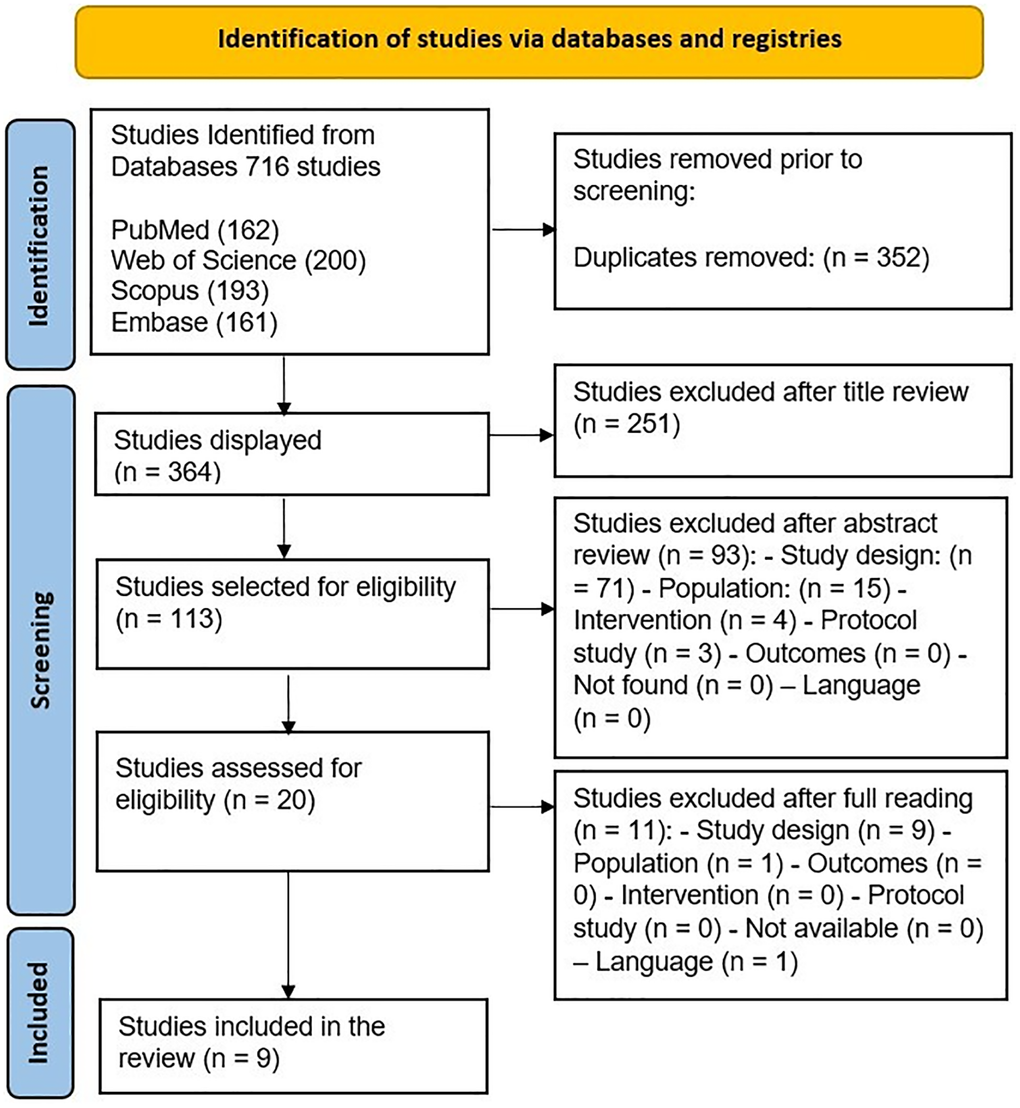
Figure 1. PRISMA flowchart illustrating the literature search and selection process.
Characteristics of included studies
Among the studies included in the review, the oldest was published in 2013 [50] and the most recent were published in 2023 [40, 41, 51] (Table 1). The studies were carried out in Brazil [40, 42, 52, 53]; Italy [45]; the United Kingdom [50], Turkey [54]; and the United States [41, 51].
Table 1. Search strategy adopted for systematic review.
| Search terms | Descriptors |
| Elderly | Elderly OR aged OR aging OR “aged, 80 and over” OR “older adults” OR “older women” OR “older men” OR senescence OR “oldest old” OR “old adults” OR nonagenarian* OR octogenarian* OR centenarian* OR elder* OR geriatr* OR “older people” OR "older person" OR senior |
| Mood | Mood OR moods OR “mood states” OR brums OR “brunel mood scale” OR poms OR “profile of mood states” OR depress* OR tense* OR tension OR irrita* OR annoyed OR hostil* OR hate* OR frustrate* OR rage OR moody OR anxious* OR temper OR vigor OR vigorous OR emotion* OR anxiety OR distress* OR anger* OR angry OR happy* OR sad OR sadness OR confus* OR upset |
| Exergames | Exergames OR exergaming OR exergame OR exergames OR “gaming, active-video” OR “virtual reality exercise” |
Participants and instruments
The 9 included studies examined psychological aspects in 325 older adults, with sample sizes ranging from 14 [41] to 83 participants [53] (Table 1). Two studies analyzed only older women [40, 52]. Ages ranged from 61 ± 6 years to 78.9 ± 8.7 years. Several instruments were adopted, among which the Profile of Mood State (POMS) was used in two studies [40, 52].
Interventions
Regarding the characteristics of the interventions, we observed several differences between the studies, making it impossible to develop a meta-analysis (Table 2). Two studies included Focus Groups, where the results were collected through interviews and group conversations [34, 35]. Regarding the comparisons performed in the selected studies, the categories identified were in relation to the level of physical activity of the individuals [44], to the control group, which practiced manual activity workshops [33], or that carried out goal setting and education on physical activity [44]. Three studies compared exergames with control groups [38, 45, 47] and two studies carried out only one intervention and compared the pre-intervention moment with the post-intervention moment [41, 44].
Table 2. Criteria for inclusion and exclusion.
| Inclusion criteria | Exclusion criteria | ||
| P | Population | Elderly ≥60 years | Studies including individuals younger than 60 years old |
| I | Intervention | Interventions using exergame | Studies not involving exergames or using non-interactive physical activities |
| C | Comparator | Among the exergame modalities, control group without exercise, with the same intervention, but different intensity, healthy individuals, other disease or disorder or not, individuals of different sexes | Studies without a comparator group or using an unrelated intervention |
| O | Outcomes | Effects of exergames on mood | Studies not assessing mood-related outcomes |
| S | Study design | Experimental, randomized, non-randomized, pre and post studies | Letters, editorials, commentaries, abstracts, conference proceedings, study protocols, case studies, review articles, non-experimental studies, cross-sectional or longitudinal studies |
The most commonly used consoles were the Xbox 360 with Kinect [40, 42, 45] and the Nintendo Wii [50, 52, 54], and the most widely used exergame was Wii Fit [50, 52, 54], however a wide variety of exergames were included.
Study quality
After assessing the quality of the studies, the studies obtained general and specific classifications of the study quality assessment criteria [55] (Table 3). The included studies obtained an average score of 8.11 (±1.05), ranging from 6 to 10. Based on this assessment, the quality of all studies was considered regular.
Table 3. Characteristics of participants and measures used to assess mood in the studies included in the review.
| References | Sample size and gender/by group | Age range/by group | Measurement (Instrument used) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [51] | S(n) = 19 SL(n) = 1 EG(n) = 10 (M = 1; F = 9) CG(n) = 9 (M = 6; F = 3) | EG = 76,4 ± 7,6 years CG = 71,4 ± 3,9 years | Patient Health Questionnaire-8 (PHQ-8) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [40] | S(n) = 22 (F) SL(n) = 9 EG(n) = 9 CG(n) = 13 | EG = 66,2 ± 4,6 years CG = 73,6 ± 8,0 years | Profile of mood state (POMS) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [41] | GF(n) = 14 SL(n) = 0 (M = 4; F = 10) | GF = 78,9 ± 8,7 years | Focus group interviews with 4–5 participants (Script included questions based on Diener et al.’s 2018 theory of subjective well-being) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [45] | S(n) = 57 SL(n) = 5 EG(n) = 38 (M = 9; F = 29) CG(n) = 19 (M = 6; F =13) | EG = 70,13 ± 3,73 years CG = 71,11 ± 3,72 years | Beck Depression Inventory II | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [54] | S(n) = 44 SL(n) = 14 EG exergame(n) = 16 (M = 7; F = 9) EG physical activity(n) = 14 (M = 6; F = 8) CG(n) = 14 (M = 9; F = 5) | EG exergame = 72,25 ± 5,95 years EG atividade física = 75,14 ± 5,50 years CG = 73,86 ± 4,63 years | Hamilton Rating Scale for Depression (HRSD) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [53] | S(n) = 83 SL(n) = 0 AG(n) = 41 (M = 5; F = 36) SG(n) = 42 (M = 26; F = 16) | AG = 69,37 ± 5,56 years SG = 74,17 ± 8,6 years | Brunel Mood Scale (BRUMS) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [42] | S(n) = 36 SL(n) = 14 EG exergame(n) = 14 (M = 5; F = 9) CG aerobic exercise(n) = 22 (M = NI; F = NI) | EG = 61,7 ± 5,7* years CG = NI | Focus group interviews | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [52] | S(n) = 30 (F with chronic low back pain) SL(n) = 4 CG physical activity(n) = 14 EG exergame(n) = 16 | S = 68 ± 4 years | Profile of Mood States (POMS) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [50] | S(n) = 20 SL(n) = 0 (M = 6 F = 14) | S = 61 ± 6 years** | Positive and Negative Affect Schedule (PANAS) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: n: number; S: samples; SL: sample loss; EG: experimental group; CG: control group; AG: active group; SG: sedentary group; M: masculine; F: female, NI: Not informed. *This study enrolled 6 individuals aged 55 to 59 years. **This study included individuals in its sample who were between 55 and 59 years old. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Most of the included studies presented common limitations, such as blinding of evaluators and the design of interrupted time series. This included the use of individual-level data to determine group-level effects, especially when the intervention was related to a specific group. Interobserver agreement for all items was 95.8%.
Effects of exergames on the mood of older people
It was found that the effects of exergames on mood varied among positive, negative, or null, depending on the characteristics of the studies analyzed and the profiles of the participants. Six studies showed that the practice of exergames by older adults produced positive effects on mood [40, 42, 50, 51, 53, 54] (Figure 2), in three studies, no significant effects were observed [41, 45, 52], and positive effects in only one aspect of mood were observed in the study by [40]. The practice of exergames did not present a negative effect in any of the studies analyzed (Frame 1).
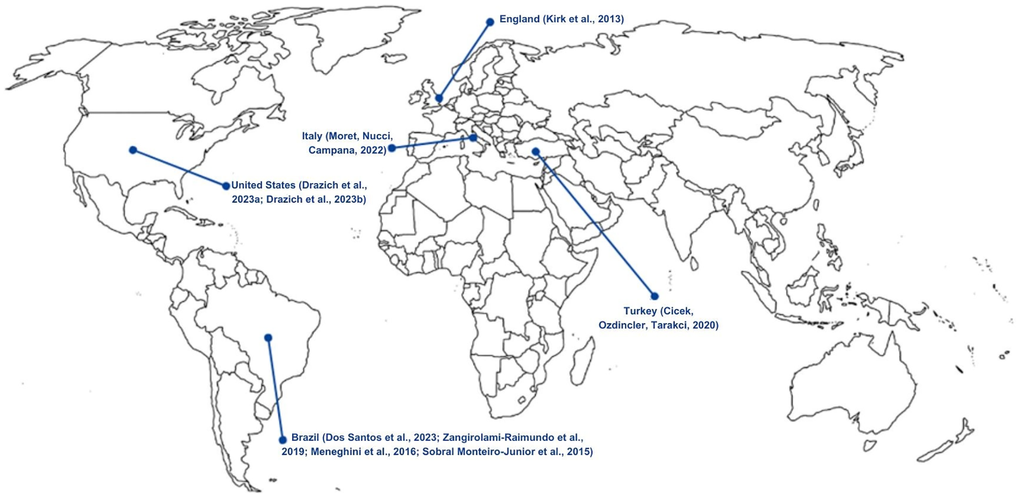
Figure 2. Global geographic distribution of studies on the effects of exergames on mood states in older adults. Country (Article references).
Frame 1. Effects of exergames on the mood of older people.
| References | Positive effects | It had no effect | Negative effects | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [51] | − | There was a positive, but not significant, influence of the program in reducing depressive symptoms in both groups. | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [40] | Tension, depression, anger, fatigue and confusion | Vigor | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [41] | Improved mood (game activity, feelings of immersion and socialization) | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [45] | − | There was no statistical evidence of a beneficial effect of exergames on mood | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [54] | Decrease in depression score in both experimental groups | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [53] | Depressive symptoms influence exergame performance | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [42] | There was a positive influence of the program on mood and emotions | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [52] | − | There was no statistical evidence of a beneficial effect of exergames on mood | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [50] | A single session of Wii activity can result in positive mood changes (mood improved before and after the session) | − | − | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Regarding the results related to sex, there was no distinction of results by this variable in any of the studies analyzed that evaluated both sexes. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
When analyzing mood variables, it is possible to observe that only two studies analyzed the variables tension, anger, fatigue, mental confusion, depressive symptoms, and vigor [40, 52], four studies analyzed only depressive mood symptoms [45, 51, 53, 54], three studies analyzed mood more comprehensively, related to positive and negative effects [50], and one in a qualitative way [42, 51], described as general mood (Frame 2).
Only two studies incorporated focus groups into their methodology (Frame 3). The interviews conducted to collect data brought a variety of enriching concepts to the research, since they were self-reported by the participants. In addition to presenting an improvement in mood, the interviews also highlighted other aspects, such as socialization, well-being, and the duration of the effects of exergames on mood.
Frame 3. Studies that used focus groups in their outcome assessments.
| References | Intervention | Results |
| [41] | The exercise practiced was “I Am Dolphin”, which lasted 15 sessions of 60 minutes. | Playing exergames improved the mood of the older adults through the game activity, but after the activity ended, the participants reported that this improvement was short-lived. The feelings of immersion gave the individuals a perception that time did not pass during the practice and did not cause boredom during the activity. The socialization that the game brought went beyond the practice, as the older adults had the opportunity to comment on the game with their friends and family. |
| [42] | The practice was carried out in pairs and was made up of 36 sessions of 50 minutes. The games played included: athletics, bowling, boxing, skiing, football, tennis, table tennis, and some mini-games. | Playing exergames was compared by the older adults to “emotional therapy”, in addition to providing well-being to individuals. Thus, it was possible to observe that the practice of exergames positively influenced the mood and emotions of the older adults. |
Although the practice of exergames produced effects on several mood variables, some studies focused specifically on the effects of exergames on depressive symptoms in older adults (Frame 4). Of these, only one study presented results that exergames provide a significant positive effect on the depression score [54], while the other two studies did not find significance in their results, but confirmed a positive trend.
Frame 4. Effects of exergames on depressive mood symptoms in older individuals.
| References | Intervention | Results |
| [51] | The EG practice was carried out on a recumbent bicycle with virtual reality glasses. The CG received classes on the practice and importance of physical activity. The intervention included 16 sessions of 40 minutes. | On average, participants reported mild depressive symptoms. After the intervention, both groups presented reductions in their depressive symptoms by an average of one point, but this result was not significant. The program therefore had a positive influence on reducing depressive symptoms in both groups. |
| [45] | The EG only performed the exergame practice (Dr Kawashima: brain and body exercises) while the CG maintained their daily routine, the duration of the intervention was 8 sessions of 45 minutes. | A positive trend was observed in the measurement of depressive symptoms, showing that the practice of exergames reduces depressive symptoms, but there was no statistical proof of this evidence. |
| [54] | There were three groups in this intervention: the exergame group (Wii Fit Plus), the physical activity group (stationary bike cycling and treadmill walking), and the CG, who maintained their daily routine. The intervention included 16 30-minute sessions. | There was a significant positive effect on depression scores in both active groups, but the effects of Nintendo Wii Fit video games were more significant than conventional physical activity. |
Discussion
The aim of the current study was to analyze the effects of exergames on the mood states of older individuals, by analyzing mood variables related to mental health and recommendations. In total, nine studies met the inclusion criteria. The main results showed that the practice of exergames provided positive effects on mood. Recent studies evaluated other psychological aspects, such as reductions in depression, anxiety, and apathy [56], which also presented positive results for the mental health of older individuals and which corroborate the results of the studies reviewed in the current work [57, 58]. These findings are summarized in Figure 3.
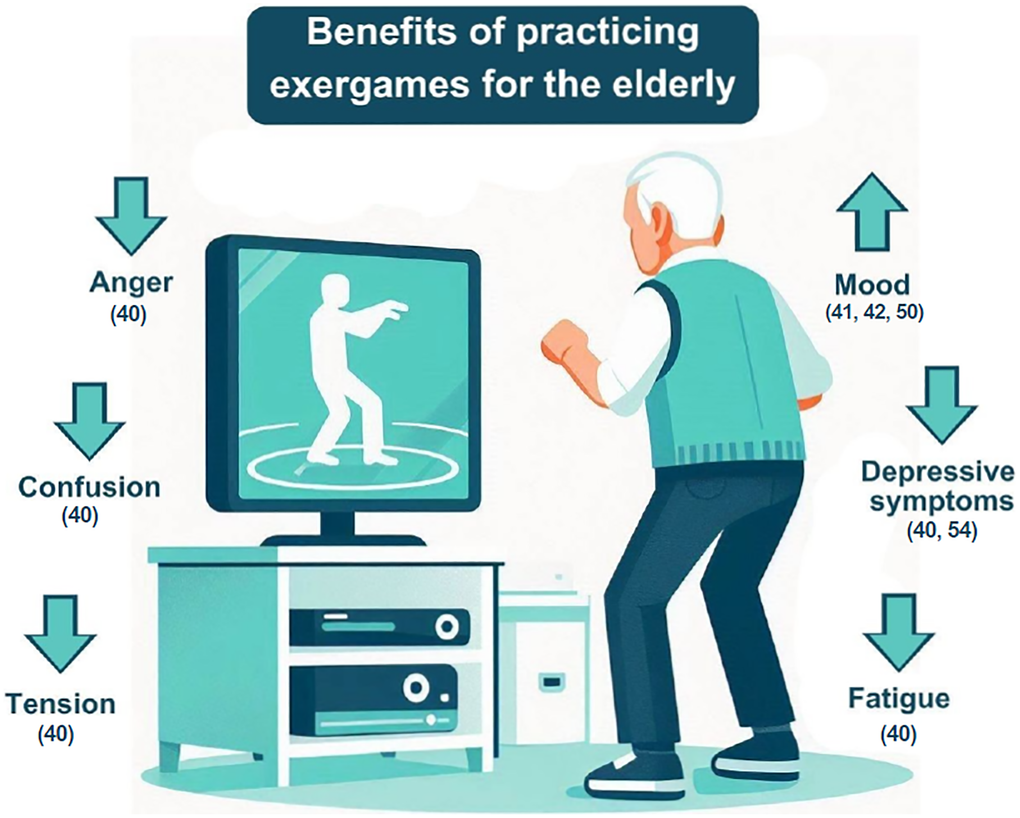
Figure 3. Benefits of practicing exergames on mood variables in the elderly.
Potential mechanisms underlying the effects of exergames on mood
The social interaction facilitated by exergames can help improve mood. Studies show that social engagement can reduce loneliness and increase social connection among participants, especially in older populations [64]. The social interaction fostered by these games can create a supportive environment that is beneficial for mood and overall mental health [57, 64]. Furthermore, practicing exergames in a group can foster positive attitudes towards others, contributing to a richer and more satisfying emotional experience [64].
Cognitive engagement is another potential mechanism that may explain the positive effects of exergames on mood. Playing exergames requires attention, decision-making, and problem-solving, which can stimulate cognitive activity and, consequently, improve mood [38, 65]. Studies show that engaging in cognitively challenging activities, such as exergames, can lead to greater feelings of vigor and happiness [29, 66]. Additionally, cognitive engagement can increase immersion and enjoyment during gameplay, which is associated with more positive mood experiences [30, 67].
Thus, both social interaction and cognitive engagement are potential mechanisms that could explain the positive effects of exergames on mood. Social interaction can improve emotional well-being by fostering social connections and support, while cognitive engagement may increase satisfaction and vigor through mental challenges. Exploring these mechanisms in greater depth can enrich the discussion on the benefits of exergames for mental health.
Sex differences in experimental studies with exergames in older individuals
Regarding the characteristics of the participants, the majority (6 out of 9 studies) conducted the experiments with the participation of female individuals [41, 45, 50, 51, 53], including two studies that only selected female participants [40, 52].
Although there was greater female participation in the included studies, only two articles reported sex as an analysis variable in their data analysis [51, 53]. In addition, only one study addressed the result of this analysis [53], while none of the other studies explored differences in results when comparing sexes, even though these data were part of the characterization of participants in all studies, and considering that differences and physiological needs between sexes have already been reported in research [68, 69]. In this sense, future studies should prioritize analyzing results by gender to provide a more comprehensive understanding of how exergames influence mood. This approach would help identify potential differences in the effects experienced by men and women, offering valuable information about whether sex-specific factors play a role in the observed outcomes.
The participation of older women has been observed in other studies [70–73]. This phenomenon can be explained by the fact that women tend to take better care of their health compared to men, which may contribute to their greater representation in related studies.
Researchers [74] conducted a cross-sectional study based on 118,199 European individuals over 50 years of age and showed that women reported a slightly lower quality of life and more depressive symptoms than men. Furthermore, it was possible to conclude that the differences between the sexes increased with advancing age, regarding quality of life, while the differences in depressive symptoms between the sexes, remained stable between age groups. Thus, it should be noted that the differences between the sexes should be explored in future studies in order to cover a wider range of variables, such as understanding sex disparities in the context of quality of life and psychological factors, which could provide valuable insights for the development of new scientific research aimed at improving the general well-being of this population.
Instruments used to assess the mood of the older adults
The selected studies used a variety of instruments to assess mood and its constructs, among them, only three used questionnaires that assess mood through various variables, which is the case of the Profile of Mood States (POMS) and BRUMS questionnaire [40, 52, 53].
The POMS instrument was developed by [75, 76] and has been shown to be reliable in assessing emotional states in different populations [77, 78]. The BRUMS is an adaptation of the POMS and was developed with the aim of allowing a rapid measurement of mood state [79]. The validations of this instrument for different populations attest to its quality [79, 80].
Considering the few studies that have investigated the mood profile, it is necessary for more articles to use gold standard instruments to assess mood, seeking to obtain more detailed results on the effects of exergames on the mood of older people, and subsequently, to evaluate the samples according to the new mood profiles [81, 82].
Protocols and exergames used
The intervention protocols varied in time, session duration, relationship between control groups, consoles, and games applied. Therefore, it is crucial to discuss these differences and understand whether there is any predominant factor or one that should be further explored in future research.
The total duration of the sessions varied between 44 minutes on average [50] and 30 total hours of intervention [42], the session times varied between 30 [51, 54] and 60 minutes, and the number of sessions varied from 1 [50, 53] to 36 sessions [42]. In this way, the great diversity of protocols, together with the different mood assessments used, limit correlations between the results of the studies.
The most widely used consoles were the Xbox 360 with Kinect [40, 42, 45] and the Nintendo Wii [50, 52, 54], which are the two reference devices in the area of exergames and which are used in research in various areas, proving their efficiency [83, 84].
The most widely used exergame was the Wii Fit [50, 52, 54]. Other types of games that were recurrent among the studies were games that simulate sports, such as Wii Sports and Kinect Sports [42, 50]. These three exergames have a common characteristic, which is the variety of game styles that each one offers, which can vary between aerobic games, yoga, muscle exercises on the Wii Fit, and games inspired by tennis, baseball, bowling, golf, boxing, and athletics on Wii Sports and Kinect Sports, reducing the possibility that the player will lose interest in the game in the long term.
Recommendations for the practice of exergames for older adults
Considering the nine included studies, experimental studies that verified the effects of practicing exergames on the mood states of the older adults and the summary of the evidence and knowledge developed from the analysis of the results, we can point out some recommendations and care recommendations for older adults. Thus, according to the authors’ recommendations, the practice of exergames is indicated for the older population and can serve as an alternative tool for the practice of physical exercises and rehabilitation of this population, and can be especially used in residential environments [51, 52, 54]. The main recommendations identified in the included studies are summarized in Frame 5.
Frame 5. Recommendations for the practice of exergames for the elderly.
| References | Recommendations |
| [51] | It is recommended that the practice of moderate to vigorous intensity exergames be further explored as a tool to reduce health disparities experienced by the elderly population. |
| [40] | They did not present any recommendations. |
| [41] | The practice should be adapted to each player profile, and can be competitive, cooperative, more or less challenging; Researchers should ensure rest periods to help alleviate fatigue or pain in older adult participants. |
| [45] | Cognitive training simultaneously with exergames in the elderly is indicated. |
| [54] | It is recommended to use alternative physical activity tools in residential environments, such as nursing homes and care centers, for the practice of physical exercises and/or rehabilitation. |
| [53] | They did not present any recommendations. |
| [42] | They did not present any recommendations. |
| [52] | Training with exergames is recommended for the elderly population as it increases pleasure, promoting greater adherence and, consequently, effectiveness resulting from continuity. |
| [50] | Assess the appropriate level of in-game exertion and heart rate through appropriate sensor devices to ensure users are working at an intensity necessary for health benefit. |
When playing, it is recommended that the practice be adapted to each player profile, which can be competitive or cooperative, and more or less challenging, thus favoring a more enjoyable environment for the player and promoting greater adherence and effectiveness resulting from the continuity of the practice [41, 52].
Considering the practical application of exergames in mental health disciplines, it is important to mention the accessibility and adaptability of these devices. They can be integrated into existing mental health interventions as a form of complementary therapy, particularly as an important complement to programs that target mood disorders, or as a preventive tool to maintain social well-being, reduce loneliness, and increase social connection in community or clinical settings [64], as the inclusion of the interactive and adaptive elements of the games can increase engagement and the effectiveness of interventions with this population [85, 86].
The implementation of exergames in clinical or community settings faces several barriers, such as the infrastructure needed to support exergames, including virtual reality equipment, which can be a challenge in terms of cost and maintenance, in addition to the lack of acceptance and familiarity of older adults with the technology, which can be overcome with adequate training and ongoing support. For this reason, the participation of health professionals and the adaptation of games to the specific needs of patients are crucial for the success of the implementation. [86–88].
It is also necessary for health professionals to take certain precautions in order to ensure the safety of practitioners. Some suggestions are that rest periods should be applied to help alleviate participants’ fatigue or pain [41]. In addition, simultaneous cognitive training with exergames in older adults is indicated [45]. Another precaution that should be considered is the assessment of the effort rate and heart rate during the practice of the game, which should ensure that users are working at an adequate and safe intensity, from moderate to vigorous, that provides better health benefits [50].
The authors’ recommendations for the production of new studies raise several relevant issues that should be emphasized. A recurring point is to conduct studies that include longer interventions, in order to be able to evaluate the long-term effects of the practice of exergames, and to be able to provide equipment so that older adults can practice exergames in their homes, reducing the barriers to practice and in the future enabling the generalization of the results found for the effects of interactive video games on healthy aging [41, 45, 50, 51, 54]. Obtaining a larger sample of older adults with greater racial and ethnic diversity and with a greater variety of depressive symptoms was also a recurring recommendation among studies [41, 42, 51]. A structured summary of these recommendations is presented in Frame 6.
Frame 6. Recommendations from the studies for future research.
| References | Recommendations |
| [51] | Use methods to distribute interventional attention more evenly across groups (such as assigning twice-weekly check-in phone calls to the control group); Obtain a sample of older adults with more variation in depressive symptoms; Develop studies of the effectiveness of fully immersive virtual reality physical activity interventions among older adults; In future, larger trials that determine the effectiveness of the intervention in increasing physical activity, residents may be able to receive their virtual reality headset upon completion of the study. |
| [40] | They did not present any recommendations. |
| [41] | Explore how to generate more lasting effects from exergaming, such as increasing exergame accessibility at home; Consider recruiting more racially and ethnically diverse older participants. |
| [45] | Use accelerometers and heart rate monitors to quantify energy consumption and perceived subjective effort, and may also use self-report questionnaires to better interpret the results; Implement longer-lasting interventions; Explore the impact of this innovative technology, also comparing it with personalized training and conventional exercises, using a robust methodology to improve the quality of evidence and provide clear and reliable guidelines. |
| [54] | Studies with larger samples are needed to generalize the effects of interactive video games on healthy aging. |
| [53] | They did not present any recommendations. |
| [42] | Developing studies with a larger number of participants is necessary to demonstrate the perception of benefits from practicing exergames. |
| [52] | Develop studies that explore the relationship between training volume and control of body stability and balance |
| [50] | Develop research that explores the degree of variation in physical intensity (and therefore associated health benefits) of Wii Sport and Wii Fit games; Develop interventions that determine the effects of Wii use with repeated exposure on health and adherence; Develop longitudinal studies. |
In addition to issues related to sample characteristics, the studies provided recommendations regarding data collection, such as the use of methods to disperse interventionist attention more equally between groups, such as assigning a routine of check-in telephone calls to the control group, which could be an effective solution for the intervention and control groups to receive more equal care [51]. Another suggestion is the use of equipment and methods that measure energy consumption and perceived subjective effort, in order to quantify the degree of variation in physical intensity [45, 50].
The recommendations consider the specificities of each study and their different objectives, and thus it is suggested that future studies address the effectiveness of fully immersive virtual reality physical activity interventions among older adults [51], compare personalized training and conventional exercises with exergames [45], explore the relationship between training volume and body stability and balance control [52], and determine the effects of Wii use on health and adherence [50].
Methods
This systematic review followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses literature search extension (PRISMA-S) [89, 90] and was registered in the Prospective Register of Systematic Reviews (PROSPERO), under number (CRD42024526448), before the completion of the selection of studies based on the eligibility criteria [91].
Research strategy
The literature search was performed using the following electronic databases: PubMed (National Library of Medicine and National Institutes of Health), Embase, Web of Science, and Scopus. In the search for studies, the search terms were included in the “all fields” option of each database, except for Scopus, where the search filter “Article title, abstract, keywords” was used. The search terms used are described in Table 4.
Table 4. Characteristics of the studies and interventions performed in the included studies.
| References | Place of publication | Objective of the study | Study design | Groups | Protocol | Console | Exergame | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [51] | United States | To determine the feasibility of a virtual reality physical activity intervention among older adults, and to test the preliminary efficacy of the intervention in increasing physical activity and decreasing depressive symptoms. | Randomized pilot study | EG = exergame, goal setting and physical activity education CG = goal setting and physical activity education | Duration: 16 sessions of 40 minutes Frequency: 2x per week for 8 weeks | Recumbent bike Nordic Track R35™ and virtual reality headset Oculus Quest 2™ | Holofit by Holidia™ | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [40] | Brazil | To evaluate the effects of a 12-week training program with Dance Exergames on the mood and functional fitness profile of elderly women. | Non-randomized experimental | EG = exergame only CG = manual activities workshops (cutting and sewing, painting and embroidery). | Duration: 24 sessions of 50 minutes Frequency: 2x per week for 12 weeks | XBOX 360 Kinect | Dance Central 3 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [41] | United States | To understand older adults’ perceptions of the connections between an exergame intervention, “I Am Dolphin”, and their subjective well-being. | Non-randomized Qualitative Descriptive | FG = just exergame | Duration: 15 sessions of 60 minutes Frequency: 3x per week for 5 weeks | Bandit (motion detection sensor based on Kinect) | I Am Dolphin | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [45] | Italy | To investigate the effects of cognitive-motor training with exergame on cognitive functions and mood in healthy elderly people. | Randomized controlled pilot study | EG = only exergame CG = kept daily routine | Duration: 8 sessions of 45 minutes Frequency: 3 to 4 times a week for 2 to 3 weeks | XBOX 360 Kinect | Fruit Ninja (habituation) Dr Kawashima: brain and body exercises | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [54] | Turkey | To evaluate the effectiveness of interactive video games on mobility, general mood and quality of life and compare them with physical activity approaches in older adults. | Non-randomized controlled clinical trial | EG exergame = only exergame EG physical activity = training (cycling on a stationary bike and walking on a treadmill) CG = maintained daily routine | Duration: 16 sessions of 30 minutes Frequency: 2x per week for 8 weeks | Nintendo Wii | “Wii Fit Plus” (Wii Fit™ and Wii Balance Board™, Nintendo of Europe GmBH Grossostheim, Deutschland) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [53] | Brazil | To compare the performance of physically active and sedentary elderly people in exergames. | Non-randomized cross-sectional | AG = just exergame SG = just exergame | Duration: 1 session (time varies depending on performance) | Computer or Notebook with webcam | MoviLetrando | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [42] | Brazil | To investigate the perception of people aged 55 or over regarding the benefits of an exercise program with exergames. | Qualitative Randomized exploratory | FG = just exergame performed in pairs | Duration: 36 sessions of 50 minutes Frequency: 3x per week for 12 weeks | Xbox 360 Kinect | Kinect Sports Ultimate Collection (athletics, bowling, boxing, skiing, football, tennis, table tennis and some mini games) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [52] | Brazil | To verify the effect of exercises with Nintendo Wii on chronic low back pain, functional capacity and mood of elderly women. | Double-blind randomized controlled trial | CG physical activity = strength exercises and core training EG exergame = strength exercises and core training and exergame | Duration: 24 sessions, general minutes NF, the exergame lasted 30 minutes. Frequency: 3x per week for 8 weeks | Nintendo Wii | “Wii Fit Plus” (Wii Fit™ and Wii Balance Board™) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| [50] | England | Reports the results of an exploratory study that examined the suitability and potential benefit of the Nintendo Wii as a tool for promoting physical activity for older adults. | Non-randomized exploratory | EG = exergame | Duration: 1 session (time varies, average 44±5.0 minutes) | Nintendo Wii | Wii Sports and Wii Fit (aerobic step, bowling, hula hooping, running, torso and waist twisting, squat with rowing, leg extension, yoga breathing and half-moon yoga pose) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Abbreviations: n: number; S: samples; EG: experimental group; CG: control group; AG: active group; SG: sedentary group; FC: Focus Group; M: masculine; F: female. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Manual search
In addition, the authors searched the reference lists of all identified studies to find any further relevant articles [92].
Eligibility criteria
The search was carried out in August 2024. To obtain a greater number of publications, there was no time limit for searching for published articles. The eligibility and exclusion criteria are described in Table 5 and were based on the PICOS strategy: Population, Intervention, Comparator, Outcome, and Study Design [48].
Table 5. Quality assessment for experimental study.
| ID Studies | Criteria* | Total score | Quality rating | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 51 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 9 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 40 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 41 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 45 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 54 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 53 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 42 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 6 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 52 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 10 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 50 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 8 | Regular | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Agreement % (Kappa) | 100 | 100 | 100 | 100 | 75 | 100 | 100 | 100 | 75 | 100 | 100 | 100 | 95.83 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Kappa interpretation (agreement) | Almost perfect | Almost perfect | Almost perfect | Almost perfect | Moderate | Almost perfect | Almost perfect | Almost perfect | Moderate | Almost perfect | Almost perfect | Almost perfect | Strong | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No or cannot determine or not applicable or not reported (0); Yes (1); The quality of the studies was classified as poor (0–4 out of 12 questions), Regular (5–10 out of 12 questions), or good (11–12 out of 12 questions). *Criteria: (1) Was the study question or objective clearly stated? (2) Were eligibility/selection criteria for the study population prespecified and clearly described? (3) Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? (4) Were all eligible participants that met the prespecified entry criteria enrolled? (5) Was the sample size sufficiently large to provide confidence in the findings? (6) Was the test/service/intervention clearly described and delivered consistently across the study population? (7) Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants? (8) Were the people assessing the outcomes blinded to the participants' exposures/interventions? (9) Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis? (10) Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests done that provided p values for the pre-to-post changes? (11) Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? (12) If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.) did the statistical analysis take into account the use of individual-level data to determine effects at the group level? | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Studies that met all of the following criteria were included in the review: (a) Population: Older adults; (b) Study design: Experimental, randomized, non-randomized, pre- and post-treatment studies; (c) Subjects: Older individuals aged 60 years or older; (d) Outcomes: Effects of exergames on mood state; (e) Country/area: Any country and region; (e) Type of article: Peer-reviewed publications; (f) Language: Restricted to publications of articles written in English, Portuguese, and Spanish.
The following studies were included: Experimental, randomized, non-randomized, pre and post studies. The following studies were excluded from the review: Reviews, letters, editorials, comments, abstracts, conference proceedings, study protocols, and articles not available in full after request by email contact with the authors.
The exclusion of non-experimental, cross-sectional, and longitudinal studies strengthens the internal validity of the current study by minimizing bias and confounding factors. Cross-sectional studies capture only short-term effects within a single session, limiting causal inference, while longitudinal designs may introduce variability due to differing follow-up periods and external factors [93]. Our study sought to prioritize experimental designs, including randomized and non-randomized trials, with the intention of ensuring a controlled evaluation of the effects of exergames on mood, reducing heterogeneity and enhancing the comparability of results [61, 71].
Study selection
After the searches, two independent researchers (CBG and WMC) selected potentially relevant studies based on the titles. The selected studies went through the phases of reading the abstract, followed by reading in full, when the inclusion/exclusion criteria were applied. If there was a divergence of opinion among the researchers in any of the phases, this was decided through discussion among them, and if no agreement was reached, the third researcher (AA) made the final decision in a consensus meeting. The selection was performed using Rayyan CRQI [94]. The references of the included articles were reviewed to identify potentially relevant articles.
Data extraction
Data extraction and synthesis were performed by analyzing the characteristics of the participants (sample, sex and age group), the instrument used to assess mood and data extraction and synthesis were performed by analyzing the characteristics of the participants (sample, sex, and age group), the instrument used to assess mood, and the experimental protocol (intervention time, weekly frequency, number of sessions, console, and exergame). Regarding mood assessment, the results of the studies were organized into categories: positive effects, no effects, and negative effects.
Evaluation of study quality
The quality of the included studies was assessed using the Quality Assessment Tool for Before-After (Pre-Post) from the National Institutes of Health – [55]. In the present study, this tool was used for the methodological evaluation of the studies. At the end of the evaluation, the instrument presents a final, based on each criterion answered; for a “yes” answer, one point is added, and for “no”, “not applicable”, “not reported” or “cannot determine” answers, the value assigned is zero. The experimental studies tool (pre-post) contains 12 criteria, thus the overall score ranges from 0–12. A higher score indicates better study quality [55].
The assessment was performed independently by two reviewers (CBG and WMC). Disagreements were resolved by consensus. When necessary, a third author (AA) was asked to decide the final opinion. The quality of the studies was not considered as an inclusion or exclusion criterion. Previous studies have used these tools, demonstrating satisfactory applicability [95, 96]. In addition, the degree of agreement between the two evaluators was analyzed using Cohen’s Kappa test. For interpretation, the agreement classification approach was used, as follows: None 0–4%; minimum 4–15%; weak 15–35%; moderate 35–63%; strong 64–81%; and almost perfect 82–100% [97].
Limitations and Future Studies
Despite the significant findings, our evidence is limited by the variations in mood assessment instruments used, heterogeneity across intervention durations and types, limited information regarding the participants’ characteristics, and small number of studies. These factors made it impossible to determine whether any specific exergame is more effective in improving the mood of older adults and whether there are differences in the effects of different durations and frequencies of exergame practice in this population. To obtain more reliable results, future studies should focus their database searches on a single type of exergame or console, in order to analyze the specific effects of these instruments on mood and evaluate whether different games or consoles influence study outcomes.
Additionally, we encourage the use of validated and standardized tools to assess mood in future research, as this would enhance the robustness and consistency of result comparisons between studies. Future research could also consider mental health factors, sex, race, and ethnicity to explore whether these variables influence the effects of exergames on mood. Moreover, studies should aim to identify which types of exergames are most beneficial for different individuals, and include interventions with longer durations and/or higher frequencies, to address this gap in the literature and provide insights into the long-term effects of exergames on the mood of older adults. To strengthen the representativeness and external validity of the findings, it is crucial to include larger and more diverse samples, as well as to consider additional strategies to assess and mitigate publication bias. These considerations have been incorporated into our discussion of limitations to appropriately address these observations. By adopting these approaches, future studies will contribute to a more accurate and comprehensive understanding of the impacts of exergames, including personalized and effective interventions for diverse populations.
Innovations, Strengths, and Applications
The current study presents innovative aspects because it is the first systematic review to address the effects of exergames on the mood of older individuals, analyzing only experimental intervention studies, and thus allowing for more specific and controlled results to be observed. In addition, it was possible to analyze different variables that make up the mood related to the mental health of older individuals. Thus, the results reported offer an opportunity for physical education professionals or physiotherapists who work directly with older individuals to discuss and integrate exergames into their practice, possibly bringing greater motivation and interest in physical exercise for these individuals.
Conclusion
The results indicate that the practice of exergames had a positive effect on the mood of older adults, reducing depressive symptoms, anger, confusion, tension, and fatigue, and promoting engagement and immersion during practice and socialization. Among the reviewed studies, no negative effects on the mood states of the older adults were reported after participating in experiments with exergames, suggesting that this activity can be recommended for this group without known risks. However, given the number of experiments carried out to date, it is recommended that new studies involving this population be carried out, with long-term designs, aiming to increase the level of available evidence.
Author Contributions
AA and CBG conceived and designed the study. CBG and WC conducted the search, performed the screening, study selection, and data extraction. CBG, AA and WC analyzed and interpreted the data. CBG and WC wrote the manuscript draft and CBG and AA revised the manuscript. All authors have read and approved the final version.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Funding
This work has been supported by the following Brazilian research agencies: National Council for Scientific and Technological Development (CNPq), Coordination for the Improvement of Higher Education Personnel — CAPES Functional Scholarship at Doctoral level - NOTICE PPGCMH N 004/2024; Foundation for research and innovation support of the State of Santa Catarina- FAPESC, PPSUS 16/2020 e PAP 027/2020.
References
- 1. Chaput JP, Willumsen J, Bull F, Chou R, Ekelund U, Firth J, Jago R, Ortega FB, Katzmarzyk PT. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. Int J Behav Nutr Phys Act. 2020; 17:141. https://doi.org/10.1186/s12966-020-01037-z [PubMed]
- 2. World economic and social survey. Department of Economic and Social Affairs. 2007. https://www.un.org/en/development/desa/policy/wess/wess_archive/2007wess.pdf.
- 3. Alves AD da S, Araújo DM, Coimbra DGL, Leitão SMA. Envelhecimento populacional: desafios e possibilidades para saúde pública. Anais do Congresso de Geriatria e Gerontologia do UNIFACIG. 2020; 1. https://pensaracademico.unifacig.edu.br/index.php/congressogeriatria/article/view/2384.
- 4. Kennedy BK, Berger SL, Brunet A, Campisi J, Cuervo AM, Epel ES, Franceschi C, Lithgow GJ, Morimoto RI, Pessin JE, Rando TA, Richardson A, Schadt EE, et al. Geroscience: linking aging to chronic disease. Cell. 2014; 159:709–13. https://doi.org/10.1016/j.cel[0-9][a-z]014.10.039 [PubMed]
- 5. Nilsson MY, Andersson S, Magnusson L, Hanson E. Ambient assisted living technology-mediated interventions for older people and their informal carers in the context of healthy ageing: A scoping review. Health Sci Rep. 2020; 4:e225. https://doi.org/10.1002/hsr2.225 [PubMed]
- 6. Andrade A, D'Oliveira A, Dos Santos KM, Bastos ACR, Corrado S, Vilarino GT, Diotaiuti P. Impact of social isolation caused by the COVID-19 pandemic on the mood profile of active and sedentary older adults: physical activity as a protective factor. Front Public Health. 2023; 11:1221142. https://doi.org/10.3389/fpubh.2023.1221142 [PubMed]
- 7. Hülür G, Macdonald B. Rethinking social relationships in old age: Digitalization and the social lives of older adults. Am Psychol. 2020; 75:554–66. https://doi.org/10.1037/amp0000604 [PubMed]
- 8. Segel-Karpas D, Ayalon L, Lachman ME. Loneliness and depressive symptoms: the moderating role of the transition into retirement. Aging Ment Health. 2018; 22:135–40. https://doi.org/10.1080/13607863.2016.1226770 [PubMed]
- 9. Umberson D, Montez JK. Social relationships and health: a flashpoint for health policy. J Health Soc Behav. 2010 (Suppl); 51:S54–66. https://doi.org/10.1177/0022146510383501 [PubMed]
- 10. D'Oliveira A, De Souza LC, Langiano E, Falese L, Diotaiuti P, Vilarino GT, Andrade A. Home Physical Exercise Protocol for Older Adults, Applied Remotely During the COVID-19 Pandemic: Protocol for Randomized and Controlled Trial. Front Psychol. 2022; 13:828495. https://doi.org/10.3389/fpsyg.2022.828495 [PubMed]
- 11. Andrade A, Siqueira TC, D'Oliveira A, Dominski FH. Effects of Exercise in the Treatment of Alzheimer's Disease: An Umbrella Review of Systematic Reviews and Meta-Analyses. J Aging Phys Act. 2022; 30:535–51. https://doi.org/10.1123/japa.2021-0033 [PubMed]
- 12. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015; 25:1–72. https://doi.org/10.1111/sms.12581 [PubMed]
- 13. Soares-Miranda L, Siscovick DS, Psaty BM, Longstreth WT
Jr , Mozaffarian D. Physical Activity and Risk of Coronary Heart Disease and Stroke in Older Adults: The Cardiovascular Health Study. Circulation. 2016; 133:147–55. https://doi.org/10.1161/CIRCULATIONAHA.115.018323 [PubMed] - 14. Ungvari Z, Fazekas-Pongor V, Csiszar A, Kunutsor SK. The multifaceted benefits of walking for healthy aging: from Blue Zones to molecular mechanisms. Geroscience. 2023; 45:3211–39. https://doi.org/10.1007/s11357-023-00873-8 [PubMed]
- 15. Wiedenmann T, Held S, Rappelt L, Grauduszus M, Spickermann S, Donath L. Exercise based reduction of falls in communitydwelling older adults: a network meta-analysis. Eur Rev Aging Phys Act. 2023; 20:1. https://doi.org/10.1186/s11556-023-00311-w [PubMed]
- 16. Figueira HA, Figueira OA, Figueira AA, Figueira JA, Polo-Ledesma RE, Lyra da Silva CR, Dantas EHM. Impact of Physical Activity on Anxiety, Depression, Stress and Quality of Life of the Older People in Brazil. Int J Environ Res Public Health. 2023; 20:1127. https://doi.org/10.3390/ijerph20021127 [PubMed]
- 17. Noetel M, Sanders T, Gallardo-Gómez D, Taylor P, Del Pozo Cruz B, van den Hoek D, Smith JJ, Mahoney J, Spathis J, Moresi M, Pagano R, Pagano L, Vasconcellos R, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2024; 384:e075847. https://doi.org/10.1136/bmj-2023-075847 [PubMed]
- 18. Ofosu EF, de Nys L, Connelly J, Ryde GC, Whittaker AC. Dimensions of Physical Activity Are Important in Managing Anxiety in Older Adults: A Systematic Review and Meta-Analysis. J Aging Phys Act. 2023; 31:679–92. https://doi.org/10.1123/japa.2022-0098 [PubMed]
- 19. Wang L, Li S, Wei L, Ren B, Zhao M. The Effects of Exercise Interventions on Mental Health in Chinese Older Adults. J Environ Public Health. 2022; 2022:7265718. https://doi.org/10.1155/2022/7265718 [PubMed]. Retraction in: J Environ Public Health. 2023; 2023:9849045. DOI: 10.1155/2023/9849045. PMID: 37538882.
- 20. Wolf S, Seiffer B, Zeibig JM, Welkerling J, Brokmeier L, Atrott B, Ehring T, Schuch FB. Is Physical Activity Associated with Less Depression and Anxiety During the COVID-19 Pandemic? A Rapid Systematic Review. Sports Med. 2021; 51:1771–83. https://doi.org/10.1007/s40279-021-01468-z [PubMed]
- 21. da Cruz WM, D' Oliveira A, Dominski FH, Diotaiuti P, Andrade A. Mental health of older people in social isolation: the role of physical activity at home during the COVID-19 pandemic. Sport Sci Health. 2022; 18:597–602. https://doi.org/10.1007/s11332-021-00825-9 [PubMed]
- 22. White RL, Babic MJ, Parker PD, Lubans DR, Astell-Burt T, Lonsdale C. Domain-Specific Physical Activity and Mental Health: A Meta-analysis. Am J Prev Med. 2017; 52:653–66. https://doi.org/10.1016/j.amepre.2016.12.008 [PubMed]
- 23. de Souza ABC, Ferreira JS, Sinésio LEM, Pissurno FR, de Alencar GP. Exergames as a tool to promote physical activity in children: an integrative review. Res Soc Dev. 2022; 11:e43911125241. https://doi.org/10.33448/rsd-v11i1.25241
- 24. Street TD, Lacey SJ, Langdon RR. Gaming Your Way to Health: A Systematic Review of Exergaming Programs to Increase Health and Exercise Behaviors in Adults. Games Health J. 2017; 6:136–46. https://doi.org/10.1089/g4h.2016.0102 [PubMed]
- 25. Xu W, Liang HN, Baghaei N, Ma X, Yu K, Meng X, Wen S. Effects of an Immersive Virtual Reality Exergame on University Students' Anxiety, Depression, and Perceived Stress: Pilot Feasibility and Usability Study. JMIR Serious Games. 2021; 9:e29330. https://doi.org/10.2196/29330 [PubMed]
- 26. Corregidor-Sánchez AI, Polonio-López B, Martin-Conty JL, Rodríguez-Hernández M, Mordillo-Mateos L, Schez-Sobrino S, Criado-álvarez JJ. Exergames to Prevent the Secondary Functional Deterioration of Older Adults during Hospitalization and Isolation Periods during the COVID-19 Pandemic. Multidisciplinary Digital Publishing Institute. 2021; 13:7932. https://www.mdpi.com/2071-1050/13/14/7932/htm.
- 27. Tough D, Robinson J, Gowling S, Raby P, Dixon J, Harrison SL. The feasibility, acceptability and outcomes of exergaming among individuals with cancer: a systematic review. BMC Cancer. 2018; 18:1151. https://doi.org/10.1186/s12885-018-5068-0 [PubMed]
- 28. Andrade A, Correia CK, Coimbra DR. The Psychological Effects of Exergames for Children and Adolescents with Obesity: A Systematic Review and Meta-Analysis. Cyberpsychol Behav Soc Netw. 2019; 22:724–35. https://doi.org/10.1089/cyber.2019.0341 [PubMed]
- 29. Andrade A, Correia CK, Cruz WMD, Bevilacqua GG. Acute Effect of Exergames on Children's Mood States During Physical Education Classes. Games Health J. 2019; 8:250–6. https://doi.org/10.1089/g4h.2018.0083 [PubMed]
- 30. Ho SS, Lwin MO, Sng JRH, Yee AZH. Escaping through exergames: Presence, enjoyment, and mood experience in predicting children’s attitude toward exergames. Comput Human Behav. 2017; 72:381–9. https://doi.org/10.1016/j.chb.2017.03.001
- 31. Huang HC, Wong MK, Lu J, Huang WF, Teng CI. Can using exergames improve physical fitness? A 12-week randomized controlled trial. Comput Human Behav. 2017; 70:310–6. https://doi.org/10.1016/j.chb.2016.12.086
- 32. Hassan MA, Ryu S, Tao K, Wang R, Quan M, Gao Z. Young adults’ rating of perceived exertion and mood in exergaming dance and aerobic dance. Brain Behavior and Immunity Integrative. 2023; 2:100007. https://doi.org/10.1016/j.bbii.2023.100007
- 33. de Medeiros CSP, Farias LBA, Santana MCD, Pacheco TBF, Dantas RR, Cavalcanti FAD. A systematic review of exergame usability as home-based balance training tool for older adults usability of exergames as home-based balance training. PLoS One. 2024; 19:e0306816. https://doi.org/10.1371/journal.pone.0306816 [PubMed]
- 34. Seinsche J, de Bruin ED, Hinrichs T, Giannouli E. Effects of home-based interventions using exergames on physical and cognitive functions in community-dwelling older adults: a PRISMA-P-compliant protocol for a systematic review. Front Public Health. 2024; 11:1291120. https://doi.org/10.3389/fpubh.2023.1291120 [PubMed]
- 35. Kruse L, Karaosmanoglu S, Rings S, Ellinger B, Steinicke F. Enabling Immersive Exercise Activities for Older Adults: A Comparison of Virtual Reality Exergames and Traditional Video Exercises. Societies. 2021; 11:134. https://doi.org/10.3390/soc11040134
- 36. Klompstra L, Stromberg A, Jaarsma T, Rytterstrom P. Feasibility exergaming as a physical activity for older adults: a systematic literature review. Eur J Prev Cardiol. 2024 (Suppl 1); 31:zwae175.048. https://doi.org/10.1093/eurjpc/zwae175.048
- 37. Ismail NA, Hashim HA, Ahmad Yusof H. Physical Activity and Exergames Among Older Adults: A Scoping Review. Games Health J. 2022; 11:1–17. https://doi.org/10.1089/g4h.2021.0104 [PubMed]
- 38. Yen HY, Chiu HL. Virtual Reality Exergames for Improving Older Adults' Cognition and Depression: A Systematic Review and Meta-Analysis of Randomized Control Trials. J Am Med Dir Assoc. 2021; 22:995–1002. https://doi.org/10.1016/j.jamda.2021.03.009 [PubMed]
- 39. Buyle M, Jung Y, Pavlou M, Gonzalez SC, Bamiou DE. The role of motivation factors in exergame interventions for fall prevention in older adults: A systematic review and meta-analysis. Front Neurol. 2022; 13:903673. https://doi.org/10.3389/fneur.2022.903673 [PubMed]
- 40. Santos RGD, de Freitas JVR, Alcantara LM, Lopes GGC, Galvão LL, de Queiroz BM, Santos DAT, de Lira CAB, Andrade MS, Knechtle B, Nikolaidis PT, Vancini RL. Effects of twelve weeks of dance Exergames on the quality-of-life variables of elderly Brazilian women enrolled in a community program. J Bodyw Mov Ther. 2023; 36:5–13. https://doi.org/10.1016/j.jbmt.2023.04.056 [PubMed]
- 41. Drazich BF, Crane BM, Taylor JL, Szanton SL, Moored KD, Eldreth D, Ahmad O, Krakauer JW, Resnick B, Carlson MC. Older adults' subjective well-being experiencing the exergame "I am Dolphin". Int J Qual Stud Health Well-being. 2023; 18:2170013. https://doi.org/10.1080/17482631.2023.2170013 [PubMed]
- 42. Meneghini V, Barbosa AR, de Mello AL, Bonetti A, Guimarães AV. Percepção de adultos mais velhos quanto à participação em programa de exercício físico com exergames: estudo qualitativo [Perception of the elderly regarding participation inexergaming-based exercise: a qualitative study]. Cien Saude Colet. 2016; 21:1033–41. https://doi.org/10.1590/1413-81232015214.11812015 [PubMed]
- 43. Altorfer P, Adcock M, de Bruin ED, Graf F, Giannouli E. Feasibility of Cognitive-Motor Exergames in Geriatric Inpatient Rehabilitation: A Pilot Randomized Controlled Study. Front Aging Neurosci. 2021; 13:739948. https://doi.org/10.3389/fnagi.2021.739948 [PubMed]
- 44. Moreira NB, Rodacki ALF, Costa SN, Pitta A, Bento PCB. Perceptive-Cognitive and Physical Function in Prefrail Older Adults: Exergaming Versus Traditional Multicomponent Training. Rejuvenation Res. 2021; 24:28–36. https://doi.org/10.1089/rej.2020.2302 [PubMed]
- 45. Moret B, Nucci M, Campana G. Effects of exergames on mood and cognition in healthy older adults: A randomized pilot study. Front Psychol. 2022; 13:1018601. https://doi.org/10.3389/fpsyg.2022.1018601 [PubMed]
- 46. Pacheco TBF, de Medeiros CSP, de Oliveira VHB, Vieira ER, de Cavalcanti FAC. Effectiveness of exergames for improving mobility and balance in older adults: a systematic review and meta-analysis. Syst Rev. 2020; 9:163. https://doi.org/10.1186/s13643-020-01421-7 [PubMed]
- 47. Perrot A, Maillot P. Factors for optimizing intervention programs for cognition in older adults: the value of exergames. NPJ Aging. 2023; 9:4. https://doi.org/10.1038/s41514-023-00103-7 [PubMed]
- 48. Roever L, Neto MG, Durães AR, Reis PEO, Pollo-Flores P, da Silva RMF, Resende ES. ARTIGO DE REVISÃO Compreendendo o GRADE: PICO e qualidade dos estudos Understanding GRADE system: PICO and study quality. Rev Soc Bras Clin Med. 2021; 19:54–61. https://www.researchgate.net/publication/359232977_ARTIGO_DE_REVISAO_Compreendendo_o_GRADE_PICO_e_qualidade_dos_estudos_Understanding_GRADE_system_PICO_and_study_quality.
- 49. Furley P, Goldschmied N. Systematic vs. Narrative Reviews in Sport and Exercise Psychology: Is Either Approach Superior to the Other? Front Psychol. 2021; 12:685082. https://doi.org/10.3389/fpsyg.2021.685082 [PubMed]
- 50. Kirk A, MacMillan F, Rice M, Carmichael A. An exploratory study examining the appropriateness and potential benefit of the nintendo wii as a physical activity tool in adults aged ≥ 55 years. Interact Comput. 2013; 25:102–14. https://doi.org/10.1093/iwc/iws004
- 51. Drazich BF, Anokye D, Zhu S, Teleb J, Galik E, Colloca L, Resnick B. Motivating older adults through immersive virtual exercise (MOTIVE): A randomized pilot study. Geriatr Nurs. 2023; 54:229–36. https://doi.org/10.1016/j.gerinurse.2023.09.019 [PubMed]
- 52. Monteiro-Junior RS, de Souza CP, Lattari E, Rocha NB, Mura G, Machado S, da Silva EB. Wii-Workouts on Chronic Pain, Physical Capabilities and Mood of Older Women: A Randomized Controlled Double Blind Trial. CNS Neurol Disord Drug Targets. 2015; 14:1157–64. https://doi.org/10.2174/1871527315666151111120131 [PubMed]
- 53. Zangirolami-Raimundo J, Raimundo RD, da Silva TD, de Andrade PE, Benetti FA, da Silva Paiva L, do Valle JET, de Abreu LC. Contrasting performance between physically active and sedentary older people playing exergames. Medicine (Baltimore). 2019; 98:e14213. https://doi.org/10.1097/MD.0000000000014213 [PubMed]
- 54. Cicek A, Ozdincler AR, Tarakci E. Interactive video game-based approaches improve mobility and mood in older adults: A nonrandomized, controlled tri̇al. J Bodyw Mov Ther. 2020; 24:252–9. https://doi.org/10.1016/j.jbmt.2020.01.005 [PubMed]
- 55. National Institutes of Health. Study Quality Assessment Tools. NHLBI, NIH. 2021. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- 56. Jahouh M, González-Bernal JJ, González-Santos J, Fernández-Lázaro D, Soto-Cámara R, Mielgo-Ayuso J. Impact of an Intervention with Wii Video Games on the Autonomy of Activities of Daily Living and Psychological-Cognitive Components in the Institutionalized Elderly. Int J Environ Res Public Health. 2021; 18:1570. https://doi.org/10.3390/ijerph18041570 [PubMed]
- 57. Fernandes CS, Magalhães B, Lima A, Nóbrega P, Silva M, Santos C. Impact of Exergames on the Mental Health of Older Adults: A Systematic Review and GRADE Evidence Synthesis. Games Health J. 2022. [Epub ahead of print]. https://doi.org/10.1089/g4h.2021.0229 [PubMed]
- 58. Cacciata M, Stromberg A, Lee JA, Sorkin D, Lombardo D, Clancy S, Nyamathi A, Evangelista LS. Effect of exergaming on health-related quality of life in older adults: A systematic review. Int J Nurs Stud. 2019; 93:30–40. https://doi.org/10.1016/j.ijnurstu.2019.01.010 [PubMed]
- 59. Rica RL, Shimojo GL, Gomes MC, Alonso AC, Pitta RM, Santa-Rosa FA, Pontes Junior FL, Ceschini F, Gobbo S, Bergamin M, Bocalini DS. Effects of a Kinect-based physical training program on body composition, functional fitness and depression in institutionalized older adults. Geriatr Gerontol Int. 2020; 20:195–200. https://doi.org/10.1111/ggi.13857 [PubMed]
- 60. Cavalli AS, Rota PA, Antonio J, Ribeiro B, Costa CP, Magalhães AB, Vaghetti CAO, Cavalli MO. Motivação e interesse de idosos em jogar Exergames relacionados à atividade física. 2014.
- 61. Andrade A, Cruz WMD, Correia CK, Santos ALG, Bevilacqua GG. Effect of practice exergames on the mood states and self-esteem of elementary school boys and girls during physical education classes: A cluster-randomized controlled natural experiment. PLoS One. 2020; 15:e0232392. https://doi.org/10.1371/journal.pone.0232392 [PubMed]
- 62. Ochi G, Kuwamizu R, Fujimoto T, Ikarashi K, Yamashiro K, Sato D. The Effects of Acute Virtual Reality Exergaming on Mood and Executive Function: Exploratory Crossover Trial. JMIR Serious Games. 2022; 10:e38200. https://doi.org/10.2196/38200 [PubMed]
- 63. Lee JE, Xiang P, Gao Z. Acute effect of active video games on older children's mood change. Comput Human Behav. 2017; 70:97–103. https://doi.org/10.1016/j.chb.2016.12.060
- 64. Li J, Erdt M, Chen L, Cao Y, Lee SQ, Theng YL. The Social Effects of Exergames on Older Adults: Systematic Review and Metric Analysis. J Med Internet Res. 2018; 20:e10486. https://doi.org/10.2196/10486 [PubMed]
- 65. Li J, Theng YL, Foo S. Effect of Exergames on Depression: A Systematic Review and Meta-Analysis. Cyberpsychol Behav Soc Netw. 2016; 19:34–42. https://doi.org/10.1089/cyber.2015.0366 [PubMed]
- 66. Huang HC, Wong MK, Yang YH, Chiu HY, Teng CI. Impact of Playing Exergames on Mood States: A Randomized Controlled Trial. Cyberpsychol Behav Soc Netw. 2017; 20:246–50. https://doi.org/10.1089/cyber.2016.0322 [PubMed]
- 67. Lee S, Kim W, Park T, Peng W. The Psychological Effects of Playing Exergames: A Systematic Review. Cyberpsychol Behav Soc Netw. 2017; 20:513–32. https://doi.org/10.1089/cyber.2017.0183 [PubMed]
- 68. Domaszewski P, Konieczny M, Dybek T, Łukaniszyn-Domaszewska K, Anton S, Sadowska-Krępa E, Skorupska E. Comparison of the effects of six-week time-restricted eating on weight loss, body composition, and visceral fat in overweight older men and women. Exp Gerontol. 2023; 174:112116. https://doi.org/10.1016/j.exger.2023.112116 [PubMed]
- 69. Gordon EH, Hubbard RE. Differences in frailty in older men and women. Med J Aust. 2020; 212:183–8. https://doi.org/10.5694/mja2.50466 [PubMed]
- 70. Ditchburn JL, van Schaik P, Dixon J, MacSween A, Martin D. The effects of exergaming on pain, postural control, technology acceptance and flow experience in older people with chronic musculoskeletal pain: a randomised controlled trial. BMC Sports Sci Med Rehabil. 2020; 12:63. https://doi.org/10.1186/s13102-020-00211-x [PubMed]
- 71. Zheng H, Li J, Salmon CT, Theng YL. The effects of exergames on emotional well-being of older adults. Comput Human Behav. 2020; 110:106383. https://doi.org/10.1016/j.chb.2020.106383
- 72. Xu X, Li J, Pham TP, Salmon CT, Theng YL. Improving Psychosocial Well-Being of Older Adults Through Exergaming: The Moderation Effects of Intergenerational Communication and Age Cohorts. Games Health J. 2016; 5:389–97. https://doi.org/10.1089/g4h.2016.0060 [PubMed]
- 73. Da Silva Júnior JLA, Biduski D, Bellei EA, Becker OHC, Daroit L, Pasqualotti A, Tourinho Filho H, De Marchi ACB. A Bowling Exergame to Improve Functional Capacity in Older Adults: Co-Design, Development, and Testing to Compare the Progress of Playing Alone Versus Playing With Peers. JMIR Serious Games. 2021; 9:e23423. https://doi.org/10.2196/23423 [PubMed]
- 74. Olsen CDH, Möller S, Ahrenfeldt LJ. Sex differences in quality of life and depressive symptoms among middle-aged and elderly Europeans: results from the SHARE survey. Aging Ment Health. 2023; 27:35–42. https://doi.org/10.1080/13607863.2021.2013434 [PubMed]
- 75. McNair DM, Lorr M, Droppleman LF. Manual for Profile of Mood States. Educational and Industrial Testing Service. 1992.
- 76. McNair DM, Lorr M, Droppleman LF. EITS Manual for the Profile of Mood States. Educational and Industrial Testing Service. 1971.
- 77. Hassmén P, Koivula N, Hansson T. Precompetitive mood states and performance of elite male golfers: do trait characteristics make a difference? Percept Mot Skills. 1998; 86:1443–57. https://doi.org/10.2466/pms.1998.86.3c.1443 [PubMed]
- 78. Terry PC, Lane AM, Lane HJ, Keohane L. Development and validation of a mood measure for adolescents. J Sports Sci. 1999; 17:861–72. https://doi.org/10.1080/026404199365425 [PubMed]
- 79. Rohlfs ICP, Rotta TM, Luft CDB, Andrade A, Krebs RJ, De Carvalho T. A Escala de Humor de Brunel (Brums): instrumento para detecção precoce da síndrome do excesso de treinamento. Revista Brasileira de Medicina do Esporte. Sociedade Brasileira de Medicina do Exercício e do Esporte. 2008; 14:176–81. https://www.scielo.br/j/rbme/a/hBHhQpZ7QqPNJywV3DCtRNs/.
- 80. Lew PCF, Parsons-Smith RL, Lamont-Mills A, Terry PC. Cross-Cultural Validation of the Malaysian Mood Scale and Tests of Between-Group Mood Differences. Int J Environ Res Public Health. 2023; 20:3348. https://doi.org/10.3390/ijerph20043348 [PubMed]
- 81. Parsons-Smith RL, Terry PC, Machin MA. Identification and Description of Novel Mood Profile Clusters. Front Psychol. 2017; 8:1958. https://doi.org/10.3389/fpsyg.2017.01958 [PubMed]
- 82. Terry P, Parsons-Smith R. Identification and Incidence of Mood Profile Clusters Among Sport Participants. J Sci Med Sport. 2019; 22:S100. http://www.jsams.org/article/S1440244019310321/fulltext.
- 83. Baldaia CP da S, Fernandes C, Ferreira L. Exergames na reabilitação da pessoa mastectomizada: uma scoping review. Associação de Enfermagem Oncológica Portuguesa (AEOP). Onco News. 2023; e072. https://doi.org/10.31877/on.2023.47.03
- 84. Marotta N, Demeco A, Indino A, de Scorpio G, Moggio L, Ammendolia A. Nintendo WiiTMversus Xbox KinectTM for functional locomotion in people with Parkinson's disease: a systematic review and network meta-analysis. Disabil Rehabil. 2022; 44:331–6. https://doi.org/10.1080/09638288.2020.1768301 [PubMed]
- 85. Ge L, Su TT, An Y, Mejía ST. The effectiveness of exergames on fear of falling in community-dwelling older adults: a systematic review. Aging Ment Health. 2022; 26:1306–17. https://doi.org/10.1080/13607863.2021.1950615 [PubMed]
- 86. Zhao C, Zhao C, Zhao M, Wang L, Guo J, Zhang L, Li Y, Sun Y, Zhang L, Li Z, Zhu W. Effect of Exergame Training on Working Memory and Executive Function in Older Adults. Multidisciplinary Digital Publishing Institute. 2022; 14:10631. https://www.mdpi.com/2071-1050/14/17/10631/htm.
- 87. Stojan R, Voelcker-Rehage C. A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. J Clin Med. 2019; 8:734. https://doi.org/10.3390/jcm8050734 [PubMed]
- 88. Manser P, Adcock-Omlin M, de Bruin ED. Design Considerations for an Exergame-Based Training Intervention for Older Adults With Mild Neurocognitive Disorder: Qualitative Study Including Focus Groups With Experts and Health Care Professionals and Individual Semistructured In-depth Patient Interviews. JMIR Serious Games. 2023; 11:e37616. https://doi.org/10.2196/37616 [PubMed]
- 89. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. https://doi.org/10.1136/bmj.n71 [PubMed]
- 90. Rethlefsen ML, Kirtley S, Waffenschmidt S, Ayala AP, Moher D, Page MJ, Koffel JB, and PRISMA-S Group. PRISMA-S: an extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst Rev. 2021; 10:39. https://doi.org/10.1186/s13643-020-01542-z [PubMed]
- 91. Schiavo JH. PROSPERO: An International Register of Systematic Review Protocols. Med Ref Serv Q. 2019; 38:171–80. https://doi.org/10.1080/02763869.2019.1588072 [PubMed]
- 92. Horsley T, Dingwall O, Sampson M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst Rev. 2011; 2011:MR000026. https://doi.org/10.1002/14651858.MR000026.pub2 [PubMed]
- 93. Wang X, Cheng Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest. 2020; 158:S65–71. https://doi.org/10.1016/j.chest.2020.03.012 [PubMed]
- 94. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016; 5:210. https://doi.org/10.1186/s13643-016-0384-4 [PubMed]
- 95. Hayes C, Simmons M, Simons C, Hopwood M. Evaluating effectiveness in adolescent mental health inpatient units: A systematic review. Int J Ment Health Nurs. 2018; 27:498–513. https://doi.org/10.1111/inm.12418 [PubMed]
- 96. Sarkies MN, Bowles KA, Skinner EH, Haas R, Lane H, Haines TP. The effectiveness of research implementation strategies for promoting evidence-informed policy and management decisions in healthcare: a systematic review. Implement Sci. 2017; 12:132. https://doi.org/10.1186/s13012-017-0662-0 [PubMed]
- 97. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012; 22:276–82. [PubMed]