




Introduction
Age-related macular degeneration (AMD) is one of the leading causes of irreversible vision loss among the elderly in industrialized countries, and its prevalence is projected to rise globally due to population aging. Epidemiological studies have suggested possible associations between AMD and cancer risk, but findings have been inconsistent and often did not distinguish between dry and neovascular forms [1–4]. Neovascular AMD (nAMD), characterized by choroidal neovascularization, represents the most vision-threatening form of AMD and is uniquely dependent on vascular endothelial growth factor (VEGF)-driven angiogenesis. While the ocular consequences of nAMD are well-established, mounting evidence suggests potential links between AMD and systemic diseases, including cancer [5–10]. AMD and cancer may share several common risk factors and biological mechanisms, such as advanced age, smoking, oxidative stress, chronic inflammation, and dysregulated angiogenic pathways, notably involving VEGF [1, 11–14].
Beyond angiogenesis, nAMD may also reflect broader systemic aging biology. Increasing evidence suggests that nAMD is associated with processes such as chronic low-grade inflammation (“inflammaging”), immune dysregulation, and extracellular matrix remodeling [15–17]. Cellular senescence, while an important component of aging, has been suggested to play dual roles: tumor-suppressive early via growth arrest, but tumor-promoting later through the senescence-associated secretory phenotype (SASP) [18]. In the context of AMD, several studies have demonstrated involvement of senescent retinal pigment epithelial cells and their SASP signatures [15, 16]. These mechanistic lines of evidence provide a framework in which nAMD might not only share angiogenic pathways with cancer but also intersect with systemic aging processes, potentially helping to explain its selective associations with certain malignancies. Recent genome-wide studies have revealed that both AMD and various cancer types exhibit polygenic susceptibility involving complement activation, lipid metabolism, and extracellular matrix regulation—pathways that are also implicated in tumor microenvironments and cancer progression—raising the possibility that such systemic vulnerability could extend beyond the eye.
Previous population-based studies have primarily evaluated AMD as a whole and reported mixed results, with some showing null or even inverse associations and others suggesting elevated risks for specific cancer types [2–4, 19]. However, the unique biology of nAMD and the widespread use of anti-VEGF therapies raise distinct questions about potential links between nAMD and cancer incidence, which remain incompletely addressed [2–4, 19].
We therefore carried out a nationwide cohort analysis using the Korean National Health Insurance Service (NHIS) database, aiming to examine the relationship between neovascular AMD and both overall and site-specific cancer incidence. Utilizing this large-scale, longitudinal dataset and validated diagnostic codes for both nAMD and various cancers, our study aimed to determine whether nAMD independently increases cancer risk and to identify which cancer types are most strongly linked to nAMD.
Materials and Methods
Study design and population
This nationwide population-based cohort study utilized data from the Korean National Health Insurance Service (NHIS) database. The study was approved by the NHIS of Korea and the Institutional Review Board of Konkuk University Medical Center (No. KUMC IRB 2024-01-024). The NHIS database provides comprehensive nationwide health information covering more than 97% of the Korean population, including demographics, medical histories, and prescription records. All diagnoses are coded according to the International Classification of Diseases, 10th Revision (ICD-10).
Cancer cases were defined by the presence of ICD-10 codes beginning with “C” and admission history with cancer as the principal diagnosis. Additionally, cancer patients were identified through the national cancer registration program to ensure accuracy. For neovascular age-related macular degeneration, patients were identified using the special copayment reduction program code V201, which is assigned specifically for confirmed nAMD diagnoses in Korea. This registration code requires confirmation by board-certified ophthalmologists through comprehensive examination including fundus photography, optical coherence tomography, and fluorescein angiography.
The NHIS database also provides baseline demographic and comorbidity information, including body mass index, diabetes mellitus, hypertension, dyslipidemia, cardiovascular diseases, stroke, chronic kidney disease, alcohol consumption, smoking status, income status, and annual number of hospital visits. Alcohol consumption was categorized as none, mild (<15 g/day), moderate (15-29.9 g/day), and heavy (≥30 g/day). Smoking status was classified as never, former, or current smoker.
From an initial population of 1,513,912 patients aged 50 years or older who underwent NHIS retinal examinations and cancer treatments during the 10-year study period (January 1, 2010, to December 31, 2019), we excluded patients with prior cancer diagnoses (n=288,546) and those with missing data (n=761,387). The study population comprised 463,979 individuals: 83,742 patients with nAMD and 380,237 patients without nAMD. Then, 1:3 matched controls were analyzed, final 250,349 matched patients without nAMD (Figure 1).
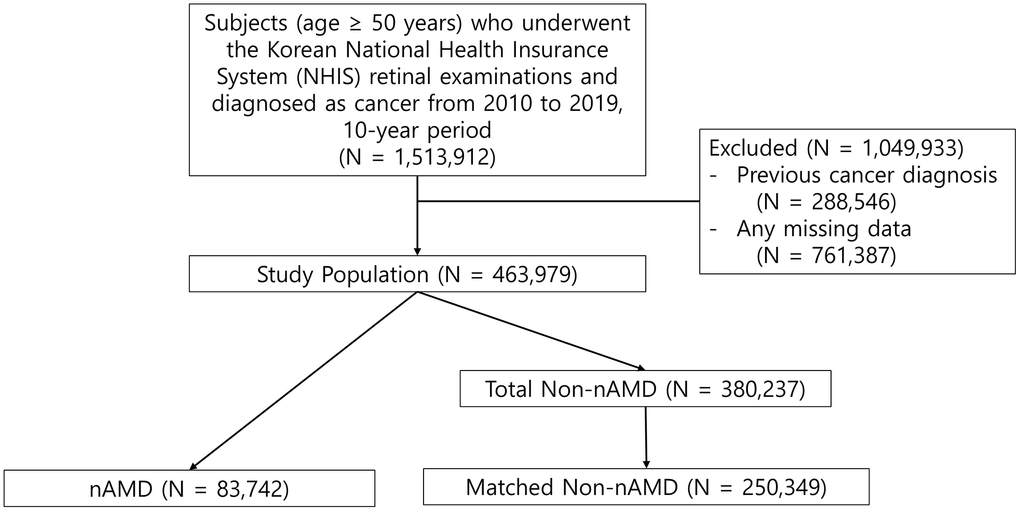
Figure 1. Flow chart of the study population. nAMD, neovascular age-related macular degeneration.
Statistical analysis
To minimize potential selection bias and balance baseline characteristics between the groups, we performed 1:3 propensity score matching. Baseline characteristics of the matched cohort were summarized as means with standard deviations (SDs) for continuous variables and as frequencies with percentages for categorical variables. Group comparisons were performed using the Student’s t test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed variables. Categorical variables were compared using the χ2 test or Fisher’s exact test, as appropriate.
Cox proportional hazards models were used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs) for time-to-event outcomes. Multivariable models were adjusted for age, sex, smoking history, alcohol consumption, income status, annual number of hospital visits, and baseline comorbidities to account for potential confounding. The proportional hazards assumption was assessed using Schoenfeld residuals. Kaplan–Meier survival curves were generated to estimate cancer-free survival, and differences between groups were evaluated with the log-rank test.
Because older patients are at an increased risk of death from other age-related conditions, a competing risk analysis was additionally conducted. We utilized the Fine and Gray subdistribution hazard model, treating all-cause mortality as a competing event, to prevent the potential overestimation of cancer incidence.
All statistical analyses were two-sided. To account for the risk of Type I error associated with evaluating multiple site-specific cancers, P-values were adjusted for multiple testing using the Benjamini-Hochberg False Discovery Rate (FDR) method. An adjusted P-value < .05 was considered statistically significant. Analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC, USA) and R version 4.0.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The final analysis included 334,091 eligible individuals aged 50 years and older who underwent retinal examinations. This cohort consisted of 83,742 patients with nAMD and 250,349 matched controls without nAMD. As detailed in Table 1, the two groups were well-balanced, demonstrating no statistically significant differences in baseline demographics (age, sex, and body mass index) or major comorbidities, including diabetes, hypertension, dyslipidemia, cardiovascular diseases, and stroke, with the sole exception of chronic kidney disease. Additionally, no significant differences were observed between the groups concerning alcohol intake, smoking status, or income level.
Table 1. Demographics and clinical characteristics of study population.
| nAMD (N = 83,742) | Non-nAMD (N=250,349) | P-value | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Age, years | 67.37±10.46 | 67.34±9.86 | 0.551 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gender (women) | 37,287 (44.52%) | 111,857 (44.68%) | 0.443 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BMI, kg/m2 | 24.14±3.07 | 24.14±3.14 | 0.862 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diabetes mellitus | 24,553 (29.32%) | 72,485 (28.95%) | 0.438 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypertension | 44,809 (53.51%) | 134,348 (53.66%) | 0.379 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dyslipidemia | 35,145 (41.97%) | 104,619 (41.78%) | 0.368 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heart diseases | 53,661 (64.08%) | 160,777 (64.22%) | 0.465 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stroke | 9,228 (11.02%) | 27,657 (11.05%) | 0.837 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chronic kidney diseases | 1,728 (2.06%) | 4,364 (1.18%) | <0.001 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Alcohol consumption, g/day | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| None | 56,108 (67.01%) | 167,746 (67.01%) | 0.963 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Mild (<15) | 16,879 (20.15%) | 50,442 (20.14%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Moderate (15-29.9) | 6,160 (7.36%) | 18,522 (7.40%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Heavy (≥30) | 4,595 (5.48%) | 13,659 (5.45%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Smoking status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Never smoker | 51,283 (61.24%) | 153,694 (61.39%) | 0.588 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Former smoker | 19,426 (23.20%) | 57,646 (23.03%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Current smoker | 13,033 (15.56%) | 39,009 (15.58%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Income status | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Top third | 17,855 (21.32%) | 53,231 (21,26%) | 0.897 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Middle third | 21,320 (25.46%) | 63,913 (25.53%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bottom third | 44,567 (53.22%) | 133,205 (53.21%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P-values in boldface indicate statistical significance. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| nAMD, neovascular age-related macular degeneration; BMI, body mass index. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
During the 10-year follow-up period, the overall incidence rate (IR) of cancer was higher among patients with nAMD compared to controls (23.55 vs. 21.01 per 1,000 person-years). Adjusted Cox proportional hazards models demonstrated that nAMD was significantly associated with an increased risk of developing any cancer (adjusted hazard ratio [aHR], 1.084; 95% CI, 1.060-1.107; P < .001) (Table 2).
Table 2. Association between neovascular age-related macular degeneration and risk of cancers.
| Cancer | Patients | IR | aHR | 95% CI | P-value | P-value False Discovery Rate | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Any Cancer | nAMD | 17,053 | 23.55 | 1.084 | 1.060-1.107 | <0.001 | 0.0005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 71,028 | 21.01 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stomach | nAMD | 2,096 | 2.66 | 0.993 | 0.934-1.055 | 0.811 | 0.9531 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 9,420 | 0.26 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Colorectal | nAMD | 2,391 | 3.04 | 1.006 | 0.950-1.065 | 0.843 | 0.9190 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 10,614 | 2.92 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Liver | nAMD | 1,944 | 2.46 | 1.057 | 0.992-1.127 | 0.087 | 0.1922 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 8,261 | 2.26 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pancreatic | nAMD | 1,544 | 1.95 | 1.155 | 1.074-1.244 | <0.001 | 0.0005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 5,916 | 1.62 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lung | nAMD | 2,873 | 3.64 | 1.128 | 1.070-1.190 | <0.001 | 0.0005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 11,158 | 3.06 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thyroid | nAMD | 967 | 1.22 | 1.241 | 1.129-1.364 | <0.001 | 0.0005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 3,495 | 0.96 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lymphoma | nAMD | 321 | 0.40 | 1.053 | 0.927-1.196 | 0.423 | 0.6936 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 1,366 | 0.37 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oral | nAMD | 196 | 0.25 | 1.112 | 0.906-1.364 | 0.310 | 0.5223 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 808 | 0.22 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Esophagus | nAMD | 220 | 0.28 | 1.021 | 0.882-1.182 | 0.781 | 0.9304 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 983 | 0.27 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gallbladder | nAMD | 339 | 0.43 | 1.098 | 0.969-1.244 | 0.142 | 0.1802 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 1,332 | 0.36 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Biliary | nAMD | 465 | 0.58 | 0.914 | 0.826-1.010 | 0.079 | 0.1643 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 2,269 | 0.62 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Laryngeal | nAMD | 123 | 0.15 | 0.998 | 0.821-1.213 | 0.984 | 0.9531 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 550 | 0.15 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Renal | nAMD | 443 | 0.56 | 1.177 | 1.059-1.309 | 0.002 | 0.0133 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 1,640 | 0.45 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bladder | nAMD | 887 | 1.12 | 1.121 | 1.041-1.207 | 0.002 | 0.0178 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 3,476 | 0.95 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nerves | nAMD | 6 | 0.01 | 0.780 | 0.326-1.864 | 0.575 | 0.8195 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 36 | 0.01 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multiple myeloma | nAMD | 203 | 0.26 | 1.008 | 0.865-1.174 | 0.920 | 0.9531 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 875 | 0.24 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leukemia | nAMD | 197 | 0.25 | 1.058 | 0.904-1.237 | 0.483 | 0.8195 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 830 | 0.23 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Skin | nAMD | 741 | 0.93 | 1.060 | 0.977-1.149 | 0.161 | 0.4446 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 3,095 | 0.84 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prostate | nAMD | 3,400 | 4.36 | 1.085 | 1.045-1.127 | <0.001 | 0.0005 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 13,817 | 3.82 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testicular | nAMD | 23 | 0.03 | 1.040 | 0.659-1.640 | 0.866 | 0.9531 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 99 | 0.03 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Breast | nAMD | 504 | 0.63 | 1.071 | 0.972-1.180 | 0.167 | 0.4063 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 2,185 | 0.60 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cervical | nAMD | 117 | 0.15 | 1.038 | 0.849-1.269 | 0.719 | 0.9304 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 530 | 0.14 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Corpus | nAMD | 105 | 0.13 | 0.964 | 0.780-1.192 | 0.737 | 0.9304 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 509 | 0.14 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ovarian | nAMD | 250 | 0.31 | 1.084 | 0.945-1.245 | 0.249 | 0.4446 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Non-nAMD | 1,070 | 0.29 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P-values in boldface indicate statistical significance. nAMD, neovascular age-related macular degeneration; IR, Incidence Rate; CI, Confidence Interval; aHR, Adjusted Hazard Ratio. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Site-specific analyses revealed significantly elevated risks for pancreatic cancer (aHR, 1.145; 95% CI, 1.074-1.244; P < 0.001), lung cancer (aHR, 1.128; 95% CI, 1.070-1.190; P < 0.001), thyroid cancer (aHR, 1.241 95% CI, 1.129-1.364; P < 0.001), renal cancer (aHR, 1.177; 95% CI, 1.059-1.309; P = 0.002), bladder cancer (aHR, 1.121; 95% CI, 1.041-1.207; P = 0.002), and prostate cancer (aHR, 1.085; 95% CI, 1.045-1.127; P < 0.001). No statistically significant associations were observed for other cancer types (Table 2).
Kaplan-Meier survival analyses further supported these findings, demonstrating decreased cancer-free survival among patients with nAMD compared to controls for pancreatic, lung, thyroid, renal, bladder, and prostate cancers (Figure 2), with log-rank tests showing significant differences across these cancer types.
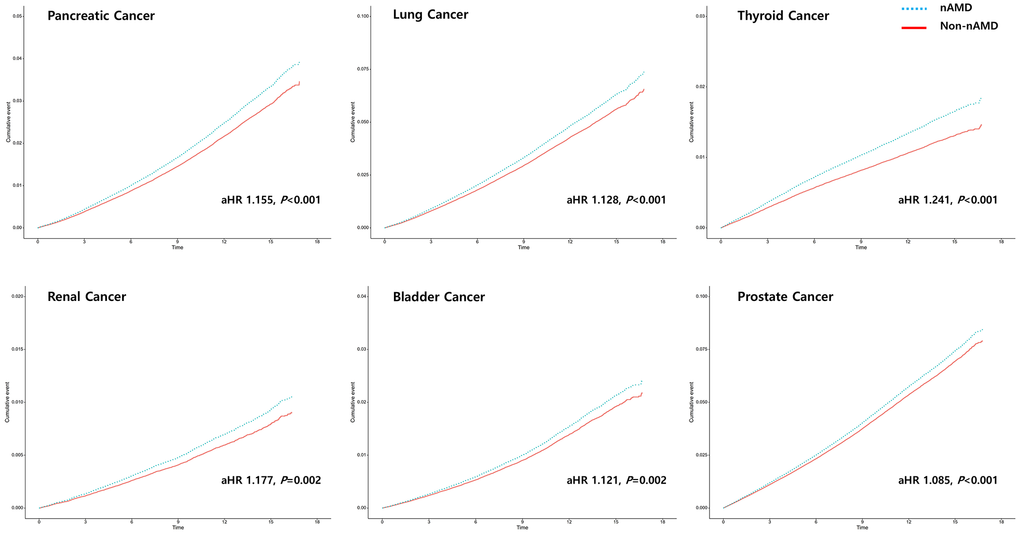
Figure 2. Association between nAMD with risk of cancer by Kaplan-Meier curves. Increased risk of pancreatic cancer (aHR 1.155, P < 0.001), lung cancer (aHR 1.128, P < 0.001), thyroid cancer (aHR 1.241, P < 0.001), renal cancer (aHR 1.177, P = 0.002), bladder cancer (aHR 1.121, P = 0.002), and prostate cancer (aHR 1.085, P < 0.001) were described.
Discussion
In this nationwide, population-based cohort study, we found that patients with nAMD had a significantly increased risk of developing cancer compared with matched controls, even after adjustment for key demographic and clinical covariates. Notably, the elevated risk was not uniform across all cancer types; it was restricted to pancreatic, lung, thyroid, renal, bladder, and prostate cancers, whereas no associations were observed for gastrointestinal, gynecologic, hematologic, or other malignancies.
Beyond angiogenesis: aging, inflammation, and senescence
While angiogenesis provides a strong biological rationale, it does not fully explain why many cancers with significant angiogenic components (gastric, colorectal, hepatic, ovarian, hematologic malignancies) showed no significant relationship with nAMD. This points to a potential overlap in a broader “aging-inflammation-vasculature” axis. However, it is important to note that the hazard ratios observed in our study are modest. Therefore, rather than serving as a definitive systemic marker, nAMD may reflect a more subtle shared epidemiological susceptibility to certain aging-related processes. Cellular senescence represents one facet of aging biology and has been proposed to be tumor-suppressive early through proliferative arrest, but tumor-promoting later through SASP [18]. The selective association of nAMD with only certain cancers may thus reflect the context-dependent duality of senescence and aging protective in some tissues, tumor-promoting in others.
Several explanations are possible for the null findings. First, competing risks and lethality: fatal tumors such as gastric or hepatic cancer in Korea may obscure associations due to shortened survival. Second, screening and detection patterns: thyroid cancer may be over-detected in Korea, inflating associations, while colorectal or gastric cancers, which rely more on alternative angiogenic pathways (e.g., PlGF, PDGF, FGF, angiopoietins), may appear null [42–44]. Third, distinct tumor biology: hematologic malignancies are primarily driven by clonal hematopoiesis and marrow niche alterations, with limited reliance on VEGF-mediated angiogenesis. Moreover, breast cancer illustrates how angiogenesis mechanisms differ: intracrine VEGF signaling predominates rather than paracrine VEGF, and angiogenic activity is strongly influenced by hormone receptor status, with heterogeneity across subtypes such as triple-negative, luminal, and HER2-positive tumors [45–47]. Similarly, ovarian cancer exhibits highly variable angiogenic patterns by histological subtype, with OVA66-mediated autocrine VEGF-VEGFR2 signaling representing a distinct pathway compared to nAMD [48, 49]. Hepatocellular carcinoma also demonstrates extensive angiogenic heterogeneity and resistance to VEGF blockade, driven by hypoxia-inducible factor activation and compensatory angiogenic pathways including FGF, PDGF, and angiopoietins, explaining the lack of association with nAMD [50, 51].
Taken together, these cancer-specific examples highlight that VEGF-dependent angiogenesis alone cannot fully account for the observed selective associations. Rather, our findings underscore the importance of considering aging, inflammation, and vascular biology in an integrated framework when interpreting the relationship between nAMD and cancer risk. The absence of association with other malignancies may suggest that cellular senescence and aging exert context-dependent effects, which could be tumor-suppressive or tumor-promoting depending on tissue and biology. However, given the observational nature of our study, these interpretations remain speculative and warrant further mechanistic validation. Collectively, while the effect sizes are modest, our findings suggest a potential epidemiological link between nAMD and specific cancers that may share pathways within the aging–inflammation–vasculature axis. Rather than indicating a profound systemic vulnerability, these results highlight a subtle shared biology. Clinically, while this modest increase in risk may not currently justify the implementation of aggressive, targeted cancer screening protocols, awareness of this selective association supports the importance of comprehensive general health monitoring in nAMD patients.
Study limitations and conclusion
Several limitations should be acknowledged. While we adjusted for key lifestyle factors such as smoking and alcohol consumption, the administrative nature of the NHIS database did not allow us to adjust for specific environmental exposures or individual genetic backgrounds, which may significantly influence population-specific cancer risk profiles. Misclassification of cancer diagnoses may also have occurred, although our identification of nAMD was strengthened by use of a specialized national registration code and further anchored by the requirement for anti-VEGF treatment, which makes our cohort highly reflective of real-world nAMD patients. By the same reasoning, dry AMD was not included in this analysis; while this could be considered a limitation, it also allowed us to specifically focus on nAMD with high diagnostic validity and clinical relevance. Furthermore, the NHIS database lacks detailed clinical information regarding cancer staging or severity at the time of diagnosis, precluding our ability to evaluate whether nAMD is differentially associated with early-stage versus progressive malignancies. Finally, as the study population comprises individuals within the Korean healthcare system and demographic context, results may not be directly generalizable to populations with different genetic backgrounds or healthcare structures.
In summary, our findings from this large, nationwide cohort indicate that nAMD is associated with an elevated risk of developing selected cancers, including pancreas, lung, thyroid, kidney, bladder, and prostate cancer. While shared dysregulated angiogenesis provides one biological explanation, our data also support a broader aging-inflammation-vasculature axis as a potential common ground. Clinically, these results emphasize the importance of recognizing systemic health concerns in individuals with nAMD. However, given the modest magnitude of the observed risk, these findings should be interpreted with clinical caution; they primarily underscore shared biological susceptibility rather than an immediate need for targeted cancer screening or novel preventive oncologic strategies. Future investigations should further elucidate the biological pathways underlying the observed associations and assess their implications for both ophthalmic and oncologic care. Moreover, as diagnostic coding becomes more standardized, expanding analyses to include dry AMD as well as nAMD will provide a more comprehensive understanding of the relationship between AMD as a whole and systemic cancer risk.
Author Contributions
Drs. Hyeong Min Kim and Hyewon Chung had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis; Concept and design: H.M. Kim and H. Chung; Acquisition, analysis, or interpretation of data: H.M. Kim, Y. Bae, M. Kim, H. Lee; Drafting of the manuscript: H.M. Kim and H. Chung; Critical revision of the manuscript for important intellectual content: H.M. Kim and H. Chung; Statistical analysis: Y. Bae, M. Kim; Administrative, technical, or material support: H. Lee; Supervision: H. Chung.
Acknowledgements
Corresponding Authors: Hyewon Chung MD, PhD; Department of Ophthalmology, Konkuk University Medical Center, 120-1, Neungdon-ro, Gwangjin-gu, Seoul, 05030, Republic of Korea.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement and Consent
This study was approved by the National Health Insurance Service (NHIS) of Korea and the Institutional Review Board (IRB) of Konkuk University Medical Center (Approval No. KUMC IRB 2024-01-024). The requirement for informed patient consent was waived by the Institutional Review Board of Konkuk University Medical Center due to the retrospective nature of the study and the use of fully anonymized, de-identified administrative claims data provided by the NHIS. All study procedures were conducted in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
This study was supported by the National Research Foundation of Korea and funded by the Ministry of Science and ICT (RS-2025-00553501, RS-2025-02213465, and RS-2025-16063013). This study was supported by 2025 fund of the Korean Retina Foundation.
References
- 1. Keizman D, Yang YX, Gottfried M, Dresler H, Leibovitch I, Haynes K, Mamtani R, Boursi B. The Association between Age-Related Macular Degeneration and Renal Cell Carcinoma: A Nested Case-Control Study. Cancer Epidemiol Biomarkers Prev. 2017; 26:743–7. https://doi.org/10.1158/1055-9965.EPI-16-0759 [PubMed]
- 2. Lin SY, Lin CL, Chang CH, Wu HC, Lin CH, Kao CH. Risk of age-related macular degeneration in patients with prostate cancer: a nationwide, population-based cohort study. Ann Oncol. 2017; 28:2575–80. https://doi.org/10.1093/annonc/mdx402 [PubMed]
- 3. Lin SY, Hsu WH, Lin CL, Lin CC, Lin JM, Chang YL, Hsu CY, Kao CH. Evidence for an Association between Macular Degeneration and Thyroid Cancer in the Aged Population. Int J Environ Res Public Health. 2018; 15:902. https://doi.org/10.3390/ijerph15050902 [PubMed]
- 4. Park J, Jung W, Han K, Kim B, Lee SY, Yoon JM, Lim DH, Shin DW. Association between age-related macular degeneration and risk of incident cancer. Br J Ophthalmol. 2024; 108:1249–56. https://doi.org/10.1136/bjo-2023-323874 [PubMed]
- 5. Chakravarthy U, Peto T. Current Perspective on Age-Related Macular Degeneration. JAMA. 2020; 324:794–5. https://doi.org/10.1001/jama.2020.5576 [PubMed]
- 6. Guymer RH, Campbell TG. Age-related macular degeneration. Lancet. 2023; 401:1459–72. https://doi.org/10.1016/S0140-6736(22)02609-5 [PubMed]
- 7. Klaver CC, Assink JJ, van Leeuwen R, Wolfs RC, Vingerling JR, Stijnen T, Hofman A, de Jong PT. Incidence and progression rates of age-related maculopathy: the Rotterdam Study. Invest Ophthalmol Vis Sci. 2001; 42:2237–41. [PubMed]
- 8. Lambert NG, ElShelmani H, Singh MK, Mansergh FC, Wride MA, Padilla M, Keegan D, Hogg RE, Ambati BK. Risk factors and biomarkers of age-related macular degeneration. Prog Retin Eye Res. 2016; 54:64–102. https://doi.org/10.1016/j.preteyeres.2016.04.003 [PubMed]
- 9. Mitchell P, Smith W, Attebo K, Wang JJ. Prevalence of age-related maculopathy in Australia. The Blue Mountains Eye Study. Ophthalmology. 1995; 102:1450–60. https://doi.org/10.1016/s0161-6420(95)30846-9 [PubMed]
- 10. Wong WL, Su X, Li X, Cheung CM, Klein R, Cheng CY, Wong TY. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014; 2:e106–16. https://doi.org/10.1016/S2214-109X(13)70145-1 [PubMed]
- 11. Cheung N, Shankar A, Klein R, Folsom AR, Couper DJ, Wong TY, and Atherosclerosis Risk in Communities (ARIC) Study Investigators. Age-related macular degeneration and cancer mortality in the atherosclerosis risk in communities study. Arch Ophthalmol. 2007; 125:1241–7. https://doi.org/10.1001/archopht.125.9.1241 [PubMed]
- 12. Goel HL, Mercurio AM. VEGF targets the tumour cell. Nat Rev Cancer. 2013; 13:871–82. https://doi.org/10.1038/nrc3627 [PubMed]
- 13. Kahn BM, Lucas A, Alur RG, Wengyn MD, Schwartz GW, Li J, Sun K, Maurer HC, Olive KP, Faryabi RB, Stanger BZ. The vascular landscape of human cancer. J Clin Invest. 2021; 131:e136655. https://doi.org/10.1172/JCI136655 [PubMed]
- 14. Shahidatul-Adha M, Zunaina E, Aini-Amalina MN. Evaluation of vascular endothelial growth factor (VEGF) level in the tears and serum of age-related macular degeneration patients. Sci Rep. 2022; 12:4423. https://doi.org/10.1038/s41598-022-08492-7 [PubMed]
- 15. Blasiak J. Senescence in the pathogenesis of age-related macular degeneration. Cell Mol Life Sci. 2020; 77:789–805. https://doi.org/10.1007/s00018-019-03420-x [PubMed]
- 16. Chae JB, Jang H, Son C, Park CW, Choi H, Jin S, Lee HY, Lee H, Ryu JH, Kim N, Kim C, Chung H. Targeting senescent retinal pigment epithelial cells facilitates retinal regeneration in mouse models of age-related macular degeneration. Geroscience. 2021; 43:2809–2833. https://doi.org/10.1007/s11357-021-00457-4 Erratum in: Geroscience. 2022; 44:1885. DOI: 10.1007/s11357-022-00523-5 PMID: 34601706.
- 17. Choi YJ, Lim D, Byeon SH, Shin EC, Chung H. Chemokine Receptor Profiles of T Cells in Patients with Age-Related Macular Degeneration. Yonsei Med J. 2022; 63:357–64. https://doi.org/10.3349/ymj.2022.63.4.357 [PubMed]
- 18. Campisi J. Aging, cellular senescence, and cancer. Annu Rev Physiol. 2013; 75:685–705. https://doi.org/10.1146/annurev-physiol-030212-183653 [PubMed]
- 19. Ha JS, Kim DK, Lee HS, Jeon S, Jeon J, Kim D, Kim JS, Kim B, Kim M, Cho KS. Androgen Deprivation Therapy and Newly Developed Neovascular Age-Related Macular Degeneration Risk in Patients with Prostate Cancer. J Clin Med. 2024; 13:2978. https://doi.org/10.3390/jcm13102978 [PubMed]
- 20. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011; 473:298–307. https://doi.org/10.1038/nature10144 [PubMed]
- 21. Hicklin DJ, Ellis LM. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol. 2005; 23:1011–27. https://doi.org/10.1200/JCO.2005.06.081 [PubMed]
- 22. Lugano R, Ramachandran M, Dimberg A. Tumor angiogenesis: causes, consequences, challenges and opportunities. Cell Mol Life Sci. 2020; 77:1745–70. https://doi.org/10.1007/s00018-019-03351-7 [PubMed]
- 23. Roudsari LC, West JL. Studying the influence of angiogenesis in in vitro cancer model systems. Adv Drug Deliv Rev. 2016; 97:250–9. https://doi.org/10.1016/j.addr.2015.11.004 [PubMed]
- 24. Saman H, Raza SS, Uddin S, Rasul K. Inducing Angiogenesis, a Key Step in Cancer Vascularization, and Treatment Approaches. Cancers (Basel). 2020; 12:1172. https://doi.org/10.3390/cancers12051172 [PubMed]
- 25. Annese T, Tamma R, Ruggieri S, Ribatti D. Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies. Cancers (Basel). 2019; 11:381. https://doi.org/10.3390/cancers11030381 [PubMed]
- 26. Elayat G, Punev I, Selim A. An Overview of Angiogenesis in Bladder Cancer. Curr Oncol Rep. 2023; 25:709–28. https://doi.org/10.1007/s11912-023-01421-5 [PubMed]
- 27. Guillaume Z, Auvray M, Vano Y, Oudard S, Helley D, Mauge L. Renal Carcinoma and Angiogenesis: Therapeutic Target and Biomarkers of Response in Current Therapies. Cancers (Basel). 2022; 14:6167. https://doi.org/10.3390/cancers14246167 [PubMed]
- 28. Melegh Z, Oltean S. Targeting Angiogenesis in Prostate Cancer. Int J Mol Sci. 2019; 20:2676. https://doi.org/10.3390/ijms20112676 [PubMed]
- 29. Ngaha TY, Zhilenkova AV, Essogmo FE, Uchendu IK, Abah MO, Fossa LT, Sangadzhieva ZD, D Sanikovich V, S Rusanov A, N Pirogova Y, Boroda A, Rozhkov A, Kemfang Ngowa JD, et al. Angiogenesis in Lung Cancer: Understanding the Roles of Growth Factors. Cancers (Basel). 2023; 15:4648. https://doi.org/10.3390/cancers15184648 [PubMed]
- 30. Rajabi S, Dehghan MH, Dastmalchi R, Jalali Mashayekhi F, Salami S, Hedayati M. The roles and role-players in thyroid cancer angiogenesis. Endocr J. 2019; 66:277–93. https://doi.org/10.1507/endocrj.EJ18-0537 [PubMed]
- 31. Fus ŁP, Górnicka B. Role of angiogenesis in urothelial bladder carcinoma. Cent European J Urol. 2016; 69:258–63. https://doi.org/10.5173/ceju.2016.830 [PubMed]
- 32. Narayanan S, Srinivas S. Incorporating VEGF-targeted therapy in advanced urothelial cancer. Ther Adv Med Oncol. 2017; 9:33–45. https://doi.org/10.1177/1758834016667179 [PubMed]
- 33. Suzuki K, Morita T, Tokue A. Vascular endothelial growth factor-C (VEGF-C) expression predicts lymph node metastasis of transitional cell carcinoma of the bladder. Int J Urol. 2005; 12:152–8. https://doi.org/10.1111/j.1442-2042.2005.01010.x [PubMed]
- 34. Huang YJ, Qi WX, He AN, Sun YJ, Shen Z, Yao Y. Prognostic value of tissue vascular endothelial growth factor expression in bladder cancer: a meta-analysis. Asian Pac J Cancer Prev. 2013; 14:645–9. https://doi.org/10.7314/apjcp.2013.14.2.645 [PubMed]
- 35. Duque JL, Loughlin KR, Adam RM, Kantoff PW, Zurakowski D, Freeman MR. Plasma levels of vascular endothelial growth factor are increased in patients with metastatic prostate cancer. Urology. 1999; 54:523–7. https://doi.org/10.1016/s0090-4295(99)00167-3 [PubMed]
- 36. Stewart RJ, Panigrahy D, Flynn E, Folkman J. Vascular endothelial growth factor expression and tumor angiogenesis are regulated by androgens in hormone responsive human prostate carcinoma: evidence for androgen dependent destabilization of vascular endothelial growth factor transcripts. J Urol. 2001; 165:688–93. https://doi.org/10.1097/00005392-200102000-00095 [PubMed]
- 37. Strohmeyer D, Rössing C, Bauerfeind A, Kaufmann O, Schlechte H, Bartsch G, Loening S. Vascular endothelial growth factor and its correlation with angiogenesis and p53 expression in prostate cancer. Prostate. 2000; 45:216–24. https://doi.org/10.1002/1097-0045(20001101)45:3<216::aid-pros3>3.0.co;2-c [PubMed]
- 38. Zhao Y, Guo S, Deng J, Shen J, Du F, Wu X, Chen Y, Li M, Chen M, Li X, Li W, Gu L, Sun Y, et al. VEGF/VEGFR-Targeted Therapy and Immunotherapy in Non-small Cell Lung Cancer: Targeting the Tumor Microenvironment. Int J Biol Sci. 2022; 18:3845–58. https://doi.org/10.7150/ijbs.70958 [PubMed]
- 39. Esposito I, Menicagli M, Funel N, Bergmann F, Boggi U, Mosca F, Bevilacqua G, Campani D. Inflammatory cells contribute to the generation of an angiogenic phenotype in pancreatic ductal adenocarcinoma. J Clin Pathol. 2004; 57:630–6. https://doi.org/10.1136/jcp.2003.014498 [PubMed]
- 40. Masamune A, Kikuta K, Watanabe T, Satoh K, Hirota M, Shimosegawa T. Hypoxia stimulates pancreatic stellate cells to induce fibrosis and angiogenesis in pancreatic cancer. Am J Physiol Gastrointest Liver Physiol. 2008; 295:G709–17. https://doi.org/10.1152/ajpgi.90356.2008 [PubMed]
- 41. Whatcott CJ, Diep CH, Jiang P, Watanabe A, LoBello J, Sima C, Hostetter G, Shepard HM, Von Hoff DD, Han H. Desmoplasia in Primary Tumors and Metastatic Lesions of Pancreatic Cancer. Clin Cancer Res. 2015; 21:3561–8. https://doi.org/10.1158/1078-0432.CCR-14-1051 [PubMed]
- 42. Chen CN, Hsieh FJ, Cheng YM, Cheng WF, Su YN, Chang KJ, Lee PH. The significance of placenta growth factor in angiogenesis and clinical outcome of human gastric cancer. Cancer Lett. 2004; 213:73–82. https://doi.org/10.1016/j.canlet.2004.05.020 [PubMed]
- 43. Macedo F, Ladeira K, Longatto-Filho A, Martins SF. Gastric Cancer and Angiogenesis: Is VEGF a Useful Biomarker to Assess Progression and Remission? J Gastric Cancer. 2017; 17:1–10. https://doi.org/10.5230/jgc.2017.17.e1 [PubMed]
- 44. Oh JM, Kim S, Tsung C, Kent E, Jain A, Ruff SM, Zhang H. Comprehensive review of the resistance mechanisms of colorectal cancer classified by therapy type. Front Immunol. 2025; 16:1571731. https://doi.org/10.3389/fimmu.2025.1571731 [PubMed]
- 45. Yan JD, Liu Y, Zhang ZY, Liu GY, Xu JH, Liu LY, Hu YM. Expression and prognostic significance of VEGFR-2 in breast cancer. Pathol Res Pract. 2015; 211:539–43. https://doi.org/10.1016/j.prp.2015.04.003 [PubMed]
- 46. Zhu X, Zhou W. The Emerging Regulation of VEGFR-2 in Triple-Negative Breast Cancer. Front Endocrinol (Lausanne). 2015; 6:159. https://doi.org/10.3389/fendo.2015.00159 [PubMed]
- 47. Zhang J, Liu C, Shi W, Yang L, Zhang Q, Cui J, Fang Y, Li Y, Ren G, Yang S, Xiang R. The novel VEGF receptor 2 inhibitor YLL545 inhibits angiogenesis and growth in breast cancer. Oncotarget. 2016; 7:41067–80. https://doi.org/10.18632/oncotarget.9392 [PubMed]
- 48. Bamberger ES, Perrett CW. Angiogenesis in epithelian ovarian cancer. Mol Pathol. 2002; 55:348–59. https://doi.org/10.1136/mp.55.6.348 [PubMed]
- 49. Song F, Chen Q, Rao W, Zhang R, Wang Y, Ge H, Wei Q. OVA66 promotes tumour angiogenesis and progression through enhancing autocrine VEGF-VEGFR2 signalling. EBioMedicine. 2019; 41:156–66. https://doi.org/10.1016/j.ebiom.2019.02.051 [PubMed]
- 50. Zheng J, Wang S, Xia L, Sun Z, Chan KM, Bernards R, Qin W, Chen J, Xia Q, Jin H. Hepatocellular carcinoma: signaling pathways and therapeutic advances. Signal Transduct Target Ther. 2025; 10:35. https://doi.org/10.1038/s41392-024-02075-w [PubMed]
- 51. Zou Y, Wan X, Zhou Q, Zhu G, Lin S, Tang Q, Yang X, Wang S. Mechanisms of drug resistance in hepatocellular carcinoma. Biol Proced Online. 2025; 27:19. https://doi.org/10.1186/s12575-025-00281-6 [PubMed]
- 52. Sim RZ, Tham YC, Betzler BK, Zhou L, Wang X, Sabanayagam C, Cheung GC, Wong TY, Cheng CY, Nusinovici S. Relationships between Lipid-Related Metabolites and Age-Related Macular Degeneration Vary with Complement Genotype. Ophthalmol Sci. 2022; 2:100211. https://doi.org/10.1016/j.xops.2022.100211 [PubMed]
- 53. Tang S, Yang J, Xiao B, Wang Y, Lei Y, Lai D, Qiu Q. Aberrant Lipid Metabolism and Complement Activation in Age-Related Macular Degeneration. Invest Ophthalmol Vis Sci. 2024; 65:20. https://doi.org/10.1167/iovs.65.12.20 [PubMed]
- 54. Zhang YD, Hurson AN, Zhang H, Choudhury PP, Easton DF, Milne RL, Simard J, Hall P, Michailidou K, Dennis J, Schmidt MK, Chang-Claude J, Gharahkhani P, et al., Breast Cancer Association Consortium (BCAC), Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON), Colon Cancer Family Registry (CCFR), Transdisciplinary Studies of Genetic Variation in Colorectal Cancer (CORECT), Endometrial Cancer Association Consortium (ECAC), Genetics and Epidemiology of Colorectal Cancer Consortium (GECCO), Melanoma Genetics Consortium (GenoMEL), Glioma International Case-Control Study (GICC), International Lung Cancer Consortium (ILCCO), Integrative Analysis of Lung Cancer Etiology and Risk (INTEGRAL) Consortium, International Consortium of Investigators Working on Non-Hodgkin’s Lymphoma Epidemiologic Studies (InterLymph), Ovarian Cancer Association Consortium (OCAC), Oral Cancer GWAS, Pancreatic Cancer Case-Control Consortium (PanC4), Pancreatic Cancer Cohort Consortium (PanScan), Prostate Cancer Association Group to Investigate Cancer Associated Alterations in the Genome (PRACTICAL), Renal Cancer GWAS, and Testicular Cancer Consortium (TECAC). Assessment of polygenic architecture and risk prediction based on common variants across fourteen cancers. Nat Commun. 2020; 11:3353. https://doi.org/10.1038/s41467-020-16483-3 [PubMed]
- 55. Rebbeck TR, Mitra N, Wan F, Sinilnikova OM, Healey S, McGuffog L, Mazoyer S, Chenevix-Trench G, Easton DF, Antoniou AC, Nathanson KL, Laitman Y, Kushnir A, et al., and CIMBA Consortium. Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. JAMA. 2015; 313:1347–61. https://doi.org/10.1001/jama.2014.5985 [PubMed]