



Introduction
As the most common malignancy of the male urogenital system, prostate cancer (PCa) has become an increasingly serious threat to male patients. [1, 2]. In the United States, it was reported that PCa is one of the most common cancer diagnosed in men, with 1,746,50 new cases and 31,620 deaths expected in 2019 [1]. PCa is the most frequently diagnosed cancer among the male population in more than half (105/185) of the countries globally and has become the major reason for tumor-related mortality among men in 46 countries [2]. Fortunately, the mortality rate of PCa has become stabilized, even decreasing recently, which is attributed to earlier diagnosis and advanced treatments [1, 3, 4]. The 5-year relative survival rate for all stages of PCa is approximately 98% [1], while for only patients with advanced tumor stage, it decreases to 28% [5].
Immunotherapy, as an important part of cancer treatment, has garnered increasing attention in recent years with further understanding of the immune escape mechanism of tumor cells [6, 7]. It has been demonstrated that the immune checkpoint signaling pathway constituted by PD-L1 and programmed cell death 1 (PD-1) promotes immune evasion of tumors [8–10]. Previous studies illustrated that high PD-L1 expression indicates poor prognosis in numerous cancers, including breast cancer [11], lung cancer [12], renal cell carcinoma [13], esophageal squamous cell carcinoma [14], biliary tract cancer [15] and gastric cancer [16]. By blocking the interaction of PD-L1 and PD-1 to prevent immune evasion of tumors, anti-PD-L1 therapy with monoclonal antibodies such as avelumab has been proven effective for cancers like Merkel cell carcinoma and non-small cell lung cancer [17, 18].
Several pilot studies have revealed PD-L1 expression features in PCa, while the clinicopathological characteristics and the prognostic value of PD-L1 still remains unclear. Therefore, we conducted this study to determine whether PD-L1 affects the prognosis of PCa. In addition, we also explored the correlation between PD-L1 and clinicopathological factors.
Results
Search results
The literature retrieval process is displayed in Figure 1. A total of 3264 studies were acquired from the initial search. After duplicates were removed, 1680 articles were screened. After removal according to titles and abstracts, 127 studies remained. When assessing the full text, 79 articles were excluded for lacking data on prognosis or clinicopathological characteristics, and 34 studies were excluded for not distinguishing high and low PD-L1 expression. Ultimately, a total of 14 studies with 3133 patients published from 2009 to 2019 were included in the final analysis [19–23, 24–32]. Table 1 shows the baseline characteristics of all included studies. The assays used to detect PD-L1, evaluation methods and cutoff values are summarized in Supplementary Table 1. Among the final studies, 5 studies were included in the analysis of the effect of PD-L1 expression or PD-L1 DNA methylation (mPD-L1) on BCR-FS, and studies ranged from 1 to 10 in the analysis of the relationship of PD-L1 and various clinicopathologic factors. The quality of all qualified studies was high with the NOS scores ranging from 6 to 7. More details are displayed in Tables 2, 3.
Table 1. Characteristics of studies included in the meta-analysis.
| Study | Country | PD-L1 detection assay | PD-L1 positive (%) | Patient characteristics | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tumor status | Patients, n | Median age, yr (range) | Gleason score, n (%) | Tumor stage, n (%) | Surgical margin, n (%) | Nodal status, n (%) | Median PSA, ng/ml (range) | Median follow-up, month (range) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ness 2017 | Norway | IHC | 236/402 (58.7) | PCa following RP | 535 | 62(47-75) | >8, 35(6.5) ≤8, 500(93.5) | pT1/pT2, 374(69.9) pT3/pT4, 161(30.1) | Positive, 286(53.5) Negative, 249(46.5) | NA | PSA<10, 308(57.6) PSA>10, 221(41.3) U, 6(1.1) | 150(17-245) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Massari 2016 | Italy | IHC | 8/16 (50.0) | CRPC | 16 | 64(53-70) | >8, 10(62.5) ≤8, 6(37.5) | NA | NA | NA | NA | at least 5 years | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Calagua 2017 | USA | IHC | 18/130 (13.8) | hormone-naive primary cancer and prostate cancer underwent RP after Neo-AAPL | 130 | 61(NA)‡ | ≥8, 34(26.0) ≤8, 96(74.0) | pT1/pT2, 64(49.2) pT3/pT4, 66(50.8) | Positive, 40(30.8) Negative, 90(69.2) | pN0, 98(75.4) pN1, 8(6.1) U, 24(18.5) | 6(4.4, 9.1) | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Baas 2017 | USA | IHC | 2/25 (8.0) | high-grade Gleason 8-10 cancer | 25 | 64±7.2 (50-79)§ | >8, 8(32.0) ≤8, 17(68.0) | NA | NA | NA | 13.9±14.3(2.4-68.9)§ | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fankhauser 2018-localized prostate cancer | Switzerland | IHC | 0/96 (0.0) | localized prostate cancer | 96 | NA | NA | NA | NA | NA | NA | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fankhauser 2018-CRPC | Switzerland | IHC | 5/81 (6.2) | CRPC | 81 | 75(54-86) | NA | NA | NA | NA | NA | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Haffner 2018-Primary Tumors | USA | IHC | 39/508 (7.7) | primary cancer | 508 | NA | ≥8, 111(21.9) ≤8, 397(78.1) | T1/T2, 195(38.4) T3/T4, 297(58.5) U, 16(3.1) | NA | N0, 467(91.9) N1, 36(7.1) U, 5(1) | NA | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Haffner 2018-CRPC | USA | IHC | 18/57 (31.6) | metastatic CRPC | 57 | NA | NA | NA | NA | NA | NA | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Petitprez 2018 | Italy | IHC | 7/51 (13.7) | node-positive PCa treated with RP and ePLND | 51 | 65(60-72) | >8, 17(33.0) ≤8, 34(67.0) | pT1/pT2, 8(16) pT3/pT4, 43(84) | Positive, 22(43) Negative, 29(57) | pN0, 50(98) pN1, 1(2) | 9.9(6.6–15.3) | 51(30–77)¶ | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ebelt 2009-PCa | Germany | IHC | 3/17 (17.6) | PCa following RP | 17 | 66(59–75) | >8, 1(5.9) ≤8, 16(94.1) | pT1/pT2, 11(64.7) pT3/pT4, 6(35.3) | NA | NA | NA | NA | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gevensleben 2016a-PD-L1 training cohort | Germany | IHC | 109/209 (52.2) | PCa following RP | 209 | 65(45-83) | >8, 14(6.7) ≤8, 190(90.9) U, 5(2.4) | pT1/pT2, 124(59.3) pT3/pT4, 85(40.7) | Positive, 83(39.7) Negative, 124(59.3) U, 2(1.0) | pN0, 192(91.9) pN1, 16(7.7) U, 1(0.5) | 7.5(0.7-163) | 61.0(0-140) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gevensleben 2016a-PD-L1 test cohort | Germany | IHC | 377/611 (61.7) | PCa following RP | 611 | 62(43-74) | >8, 40(6.5) ≤8, 571(93.5) | pT1/pT2, 418(68.4) pT3/pT4, 193(31.6) | Positive, 169(27.7) Negative, 439(71.8) U, 3(0.5) | pN0, 299(48.9) pN1, 9(1.5) U, 303(49.6) | 7.1(0.8-39.0) | 49.6(0-129) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gevensleben 2016a-mPD-L1 training cohort | Germany | qPCR | 101/498 (20.3) | PCa following RP | 498 | 61(NA) | >8, 141(28.3) ≤8, 357(71.7) | pT2, 188(37.8) pT3, 303(60.8) U, 7(1.4) | Positive, 152(30.5) Negative, 316(63.5) U, 30(6.0) | pN0, 346(69.5) pN1, 79(15.9) U, 73(14.7) | PSA≤10, 339(68.0) PSA>10, 156(31.3) U, 3(0.6) | 16(1-133) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gevensleben 2016b-mPD-L1 validation cohort | Germany | qPCR | 102/299 (34.1) | PCa following RP | 299 | NA | >8, 16(5.4) ≤8, 281(93.9) U, 2(0.7) | pT2, 205(68.6) pT3, 94(31.4) U, 1(0.3) | Positive, 98(32.8) Negative, 197(65.9) U, 4(1.3) | pN0, 278(93.0) pN1, 20(6.7) U, 1(0.3) | PSA≤10, 200(66.9) PSA>10, 86(28.8) U, 13(4.3) | 63(1-145) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iacovelli-2019-mCSPC | Italy | IHC | 15/32 (46.9) | mCSPC | 32 | 71.4(NA) | ≥8, 29(90.6) <8, 3(9.4) | NA | NA | N0, 17(91.9) N1, 15(7.1) | 170.0(NA) | 83.4(NA) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Li 2019 | China | IHC | 63/127 (49.6) | high risk PCa received AHT after RP | 127 | 66(48-76) | ≥8, 63(50.4) <8, 64(49.6) | pT1/pT2, 54(42.5) pT3/pT4, 73(57.5) | Positive, 47(63.0) Negative, 80(37.0) | pN0, 86(67.7) pN1, 41(32.3) | 49.74(1.98-408.21) | 40(29-53)¶ | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sharma 2019 | USA | IHC | 29/220 (13.2) | PCa following RP | 220 | 60.3(42-78) | ≥8, 24(10.9) <8, 196(89.1) | pT1/pT2, 166(75.5) pT3/pT4, 54(24.5) | NA | pN0, 138(62.7) pN1, 11(5.0) pNX, 71(32.3) | NA | 48.2(3-116) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Xian 2019 | USA | IHC | 50/279 (17.9) | PCa following RP | 279 | 61.1(39-76) | ≥8, 73(26.2) <8, 206(73.8) | T1/T2, 168(69.2) T3/T4, 111(39.8) | NA | N0, 255(91.4) N1, 21(7.5) U, 3(1.0) | ≤10, 220(78.9) >10, 54(19.4) U, 5(1.8) | 106.5(3-180) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| PSA, prostate specific antigen; IHC, immunohistochemistry; PCa, prostate cancer; pT, pathological tumor stage; pN, nodal pathological status; U, unknown; NA, not available; CRPC, castration-resistant prostate cancer; RP, radical prostatectomy; Neo-AAPL, neoadjuvant abiraterone acetate plus leuprolide plus prednisone; mCSPC, metastatic castration-sensitive prostate cancer; qPCR, quantitative polymerase chain reaction. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ‡ Median age at diagnosis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| § Mean ± Standard deviation (Range) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ¶ Median (Interquartile range) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Newcastle-Ottawa scale for risk of bias assessment of the case control studies.
| Source | Selection | Comparability | Exposure | ||||||
| Study | Adequacy of case definition | Representativeness of the cases | Selection of Controls | Definition of Controls | Comparability of cases and controls on the basis of the design or analysis | Ascertainment of exposure | Same method of ascertainment for cases and controls | Non-Response rate | Overall |
| Calagua 2017 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Haffner 2018 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Ebelt 2009 | ★ | ★ | ★ | ★ | ★ | ★ | 6 | ||
| Baas 2017 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Fankhauser 2018 | ★ | ★ | ★ | ★ | ★ | ★ | 6 | ||
Table 3. Newcastle-Ottawa scale for risk of bias assessment of the cohort studies.
| Source | Selection | Comparability | Outcome | ||||||
| Study | Representativeness of exposed cohort | Selection of non-exposed cohort | Ascertainment of exposure to implants | Outcome not present at start | Comparability of cohorts on the basis of the design or analysis | Assessment of outcome | Adequate follow-up length | Adequacy of follow-up | Overall |
| Gevensleben 2016a | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Gevensleben 2016b | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Massari 2016 | ★ | ★ | ★ | ★ | ★ | ★ | 6 | ||
| Ness 2017 | ★ | ★ | ★★ | ★ | ★ | 6 | |||
| Petitprez 2017 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Iacovelli 2019 | ★ | ★ | ★ | ★ | ★ | ★ | 6 | ||
| Li 2019 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Sharma 2019 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
| Xian 2019 | ★ | ★ | ★★ | ★ | ★ | ★ | 7 | ||
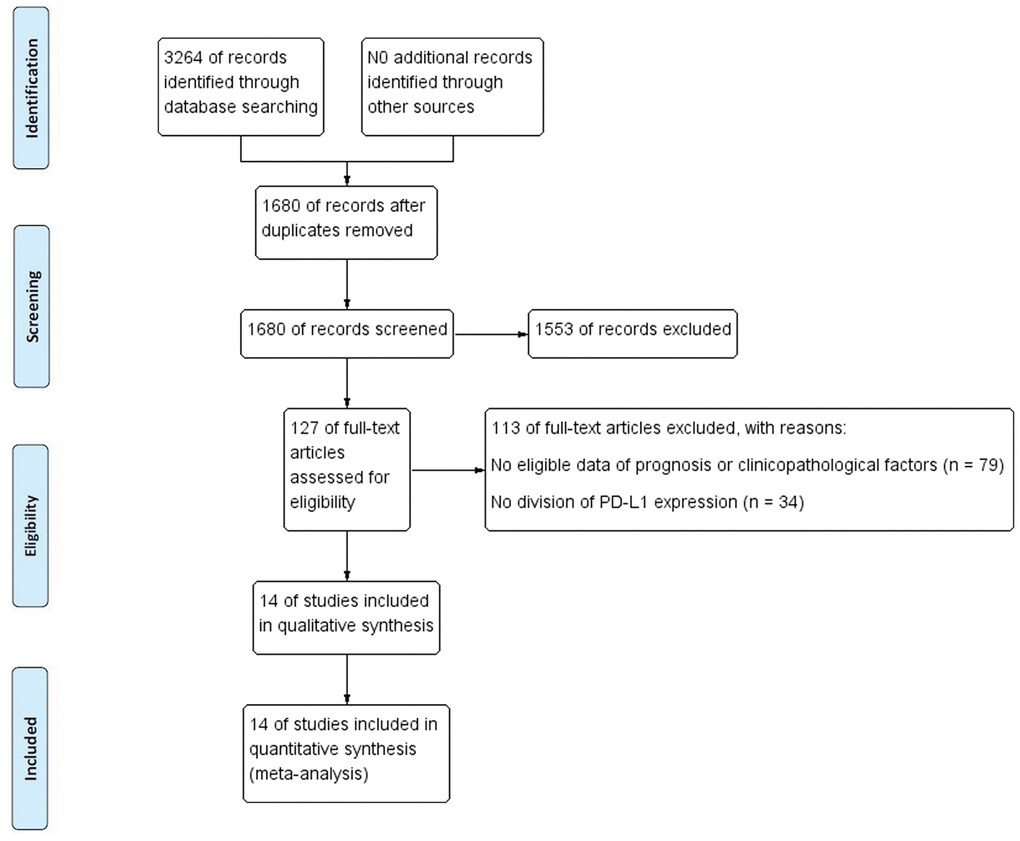
Figure 1. Flow chart of study selection process.
Prognostic significance of PD-L1 and mPD-L1 in PCa
Five studies [19–23] reported information about univariate proportional hazards analysis of PD-L1 expression or mPD-L1. The pooled results are displayed in Figure 2A and Table 4 (HR = 1.67, 95% CI = 1.38-2.06, p < 0.001), demonstrating that PD-L1 overexpression predicted poor BCR-FS. However, high heterogeneity was detected among the studies (I2 = 75.7%, p = 0.002). As seen in Figure 2B, we identified a significant association between high mPD-L1 and poor BCR-FS (HR = 2.23, 95% CI, 1.51-3.29, p < 0.001). No significant heterogeneity was present (I2 = 0.0%, p = 0.430).
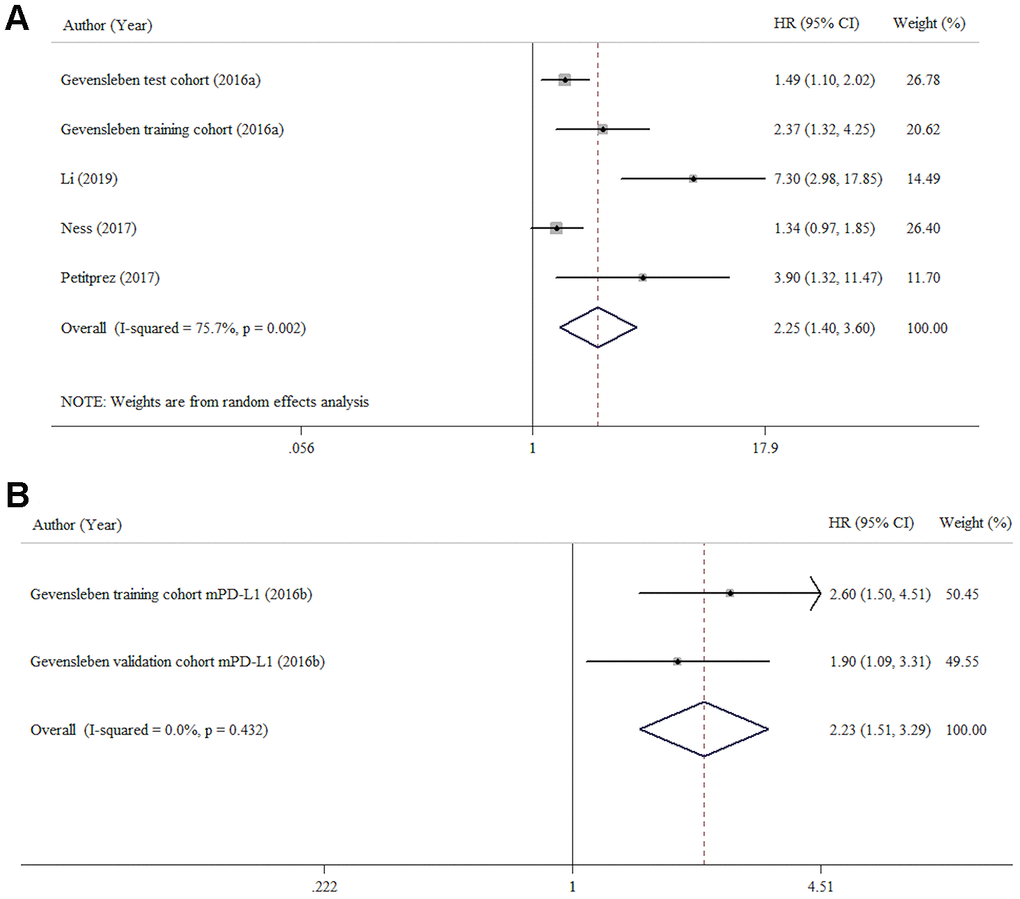
Figure 2. Forest plots HR for assessing the association between BCR-FS and PD-L1 protein expression (A) and mPD-L1 (B) in patients with prostate cancer.
Table 4. Meta-analysis results for the clinicopathological significance and prognostic value of PD-L1 in PCa.
| No. of studies | Chi² | pheterogeneity | I² (%) | Pooled OR/HR (95% CI) | Begg's test | ||||
| Fixed model | p value | Random model | p value | p value | |||||
| Age (>60 VS ≤60) | 3 | 0.37 | 0.947 | 0.0 | 1.28 (0.94-1.75) | 0.122 | 1.28 (0.94-1.75) | 0.123 | 0.734 |
| Preoperative PSA (>10 VS ≤10) | 2 | 4.92 | 0.085 | 59.3 | 1.04 (0.78-1.39) | 0.796 | 0.91 (0.54-1.55) | 0.733 | 1.000 |
| Tumor stage (pT3,4 VS pT1,2) | 7 | 10.87 | 0.144 | 35.6 | 1.40 (1.13-1.75) | 0.003 | 1.46 (1.08-1.99) | 0.015 | 0.386 |
| pN (N1 VS N0) | 7 | 15.96 | 0.025 | 56.1 | 1.37 (0.93-2.03) | 0.113 | 1.53 (0.80-2.93) | 0.199 | 0.108 |
| Surgical margin (R1 VS R0) | 3 | 5.33 | 0.149 | 43.8 | 1.36 (1.03-1.78) | 0.028 | 1.49 (0.99-2.23) | 0.055 | 0.308 |
| Gleason score (>8 VS ≤8) | 10 | 12.47 | 0.255 | 19.8 | 1.81 (1.35-2.42) | <0.001 | 1.87 (1.32-2.66) | <0.001 | 0.436 |
| AR status (AR+ VS AR-) | 1 | 1.1 | 0.294 | 9.3 | 2.20 (1.61-3.01) | <0.001 | 2.22 (1.58-3.10) | <0.001 | 1.000 |
| PD-L1 expression (CRPC VS HSPC) | 2 | 0.42 | 0.515 | 0.0 | 6.01 (3.22-11.23) | <0.001 | 5.64 (3.04-10.49) | <0.001 | 1.000 |
| BCR-FS (PD-L1 high VS PD-L1 low) | 5 | 16.49 | 0.002 | 75.7 | 1.67 (1.38-2.06) | <0.001 | 2.25 (1.40-3.61) | 0.001 | 0.221 |
| BCR-FS (mPD-L1 high VS low) | 1 | 0.52 | 0.432 | 0.0 | 2.23 (1.51-3.29) | <0.001 | 2.23 (1.51-3.29) | <0.001 | 1.000 |
PD-L1 expression in castration-resistant prostate cancer (CRPC) and primary PCa
We explored the association of PD-L1 expression with sensitivity to androgen deprivation therapy (CRPC vs primary PCa). This analysis included two studies with 819 patients. Compared with primary PCa cases (hormone-sensitive prostate cancer, HSPC), CRPC cases had a high prevalence of high or positive PD-L1 expression (OR = 6.01, 95% CI = 3.22-11.23, p < 0.001) (Figure 3). No significant heterogeneity was found (I2 =0.0%, p = 0.520).
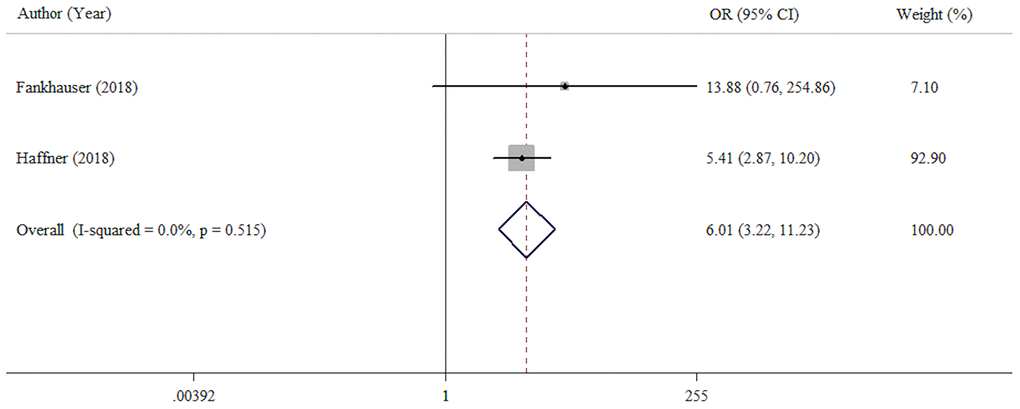
Figure 3. Forest plot assessing the association between PD-L1 expression and sensitivity of androgen deprivation therapy (CRPC VS HSPC).
The clinicopathological significance of PD-L1 expression in PCa
To find out the association between PD-L1 expression and age, preoperative PSA, tumor stage, nodal status, surgical margin, Gleason score and AR status, 3, 2, 7, 7, 3, 10 and 1 studies were analyzed, respectively. As shown in Figure 4A–4G and Table 4, the pooled ORs revealed that PD-L1 overexpression was more prevalent in PCa patients with advanced tumor stage (OR = 1.40, 95% CI = 1.13-1.75, p = 0.003), positive surgical margin (OR = 1.36, 95% CI = 1.03-1.78, p = 0.028), higher Gleason score (OR = 1.81, 95% CI = 1.35-2.42, p < 0.001) and AR positivity (OR = 2.20, 95% CI = 1.61-3.01, p < 0.001). However, the associations between PD-L1 expression and age, preoperative PSA and nodal status were not statistically significant (p = 0.122, p = 0.796, and p = 0.113, respectively).
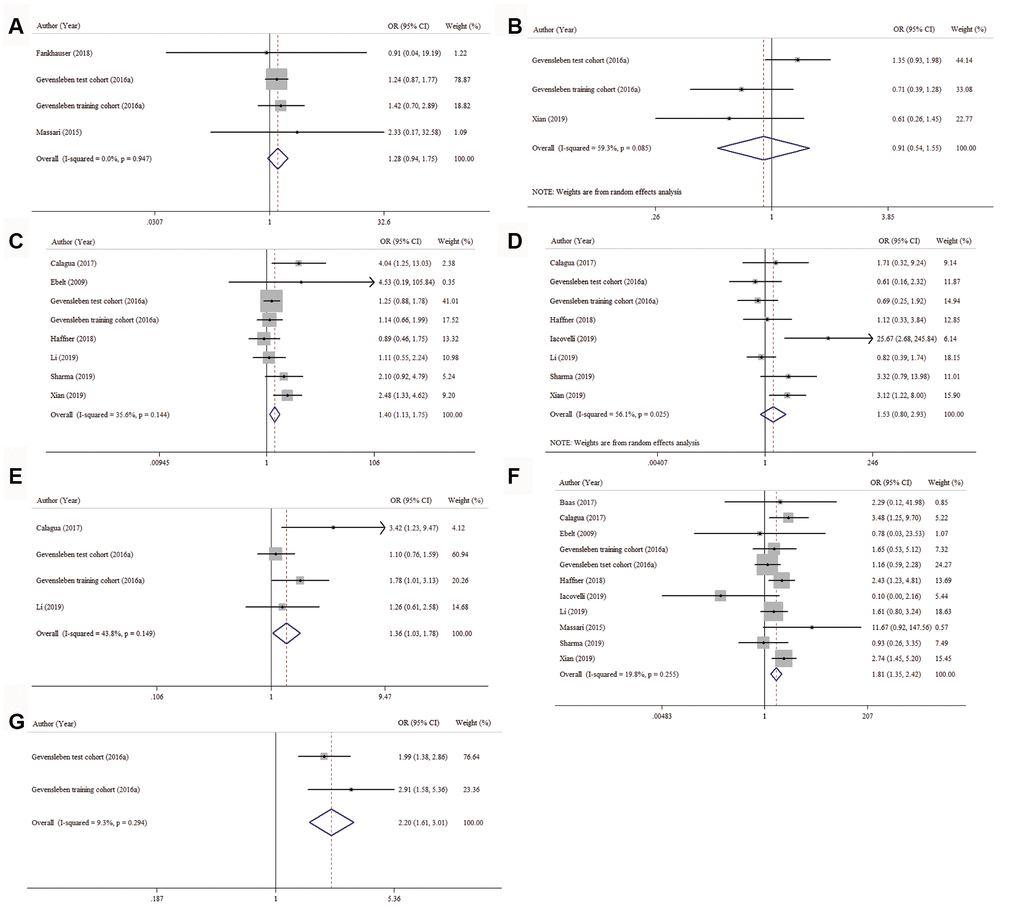
Figure 4. Forest plots for the correlation between PD-L1 expression and clinicopathologic characteristics. (A) age, (B) preoperative PSA, (C) tumor stage, (D) nodal status, (E) surgical margin, (F) Gleason score and (G) AR status.
Publication bias assessment
Begg’s test was applied to assess publication bias. The results suggested that no evidence of significant publication bias was present (Table 4 and Supplementary Figure 1A–1I).
Discussion
PD-L1 is a type 1 transmembrane protein, a member of the B7/CD28 costimulatory factor family, which was first discovered by Dong in 1999 [33]. PD-L1 is normally expressed by macrophage lineage cells with the induction of inflammatory cytokines [33–35]. PD-L1 can function as an immune checkpoint. When PD-L1 binds to its receptor PD-1, the immune system is negatively regulated to protect tissues from damage in normal physiological situations [9, 36]. However, PD-L1 is also expressed in numerous tumor cells [37–41]. Overexpression of PD-L1 in tumor cells combined with PD-1, which is mainly expressed on activated T-cells, can trigger an immunosuppression effect in the tumor microenvironment, leading to tumor immune evasion [9, 10]. It was reported that PD-L1 positivity on tumor cells of primary PCa and CRPC is ~92% and ~19%, respectively [20, 21, 26]. And the expression of PD-L1in PCa patients will up-regulate in response to inflammatory cytokines like IFN-γ or when particular signaling pathways (NF-kB) is activated [42].
Recently, some studies have verified that PD-L1 overexpression indicates poor prognosis in various cancers [15, 43–46], and several anti-PD-L1 monoclonal antibodies, including avelumab, durvalumab and atezolizumab have been approved by the FDA [47–49]. However, anti-PD-L1 therapy in PCa is not as effective as it is in other solid tumors. Few studies have explored the prognostic value of PD-L1 in PCa with disputable and unclear results.
This meta-analysis was performed to explore whether the prognosis of PCa correlates with PD-L1. The pooled data from the eligible studies revealed that overexpressed PD-L1 and mPD-L1 predicted poor BCR-FS in PCa patients, which was consistent with Li’s study [50].
Our study also explored the relationship of PD-L1 expression with clinicopathological features in PCa. The pooled results revealed that high PD-L1 expression was more likely to be observed in patients with CRPC than in patients with HSPC. This finding indicated that patients with PD-L1 overexpression show more resistance to androgen deprivation therapy (ADT) than those with low PD-L1 expression and might obtain a survival benefit from anti-PD-L1 immunotherapy. Additionally, PD-L1 overexpression was more prevalent in patients with advanced tumor stage, high GS, and positive surgical margin and positive AR status, which suggested the potential of a combined strategy featuring anti-PD-L1 immunotherapy and ADT or radiotherapy in consideration in certain situations.
Li [50] reported no statistically significant association between PD-L1 and age (OR = 1.27, 95% CI = 0.93-1.75, p = 0.14), nodal status (OR = 0.65, 95% CI = 0.35-1.21, p = 0.17) or preoperative PSA (OR = 1.13, 95% CI = 0.82-1.54, p = 0.46). A study conducted immunohistochemical staining of PD-L1/PD1 in 279 patients who underwent radical prostatectomy indicated that age (≥ 65 years), obesity (BMI ≥ 30), and advanced tumor stage, lymph node metastasis, and high Gleason score patients were related with higher PD-L1 positivity [32]. In total, 6.5 tumor-infiltrating lymphocytes per high power field were positive for PD-1 staining and 50/279 (17.9%) tumors were positive for PD-L1 staining. Interestingly, Peng’s research indicated PD-1-positive lymphocytes were significantly more expressed in PD-L1-positive tumors than PD-L1-negative.
Similarly, the correlation of PD-L1 over-expression with advanced tumor stage and higher Gleason score were also found in our study, but for age, preoperative PSA or nodal status was not significant. Moreover, we indicated that surgical margin and androgen receptor was relevant to higher PD-L1 expression. Furthermore, our study demonstrated that the prevalence of PD-L1 overexpression was higher in pT3/pT4 stage than other stages in PCa (OR = 1.40, 95% CI = 1.13-1.75, p = 0.003).
We conducted this study to uncover the prognostic and clinicopathological value of PD-L1 in PCa. Compared with previous research, we included higher numbers of qualified studies and performed more comprehensive analyses. Furthermore, this study was the first to uncover the obvious correlation between PD-L1 expression and surgical margin. However, there are several limitations in our study that should be stated. First, even though the same detection assay, immunohistochemistry, was applied to detect the expression of PD-L1, the specifics of the assays varied between studies. Second, the evaluation methods and cutoff values for dichotomization were inconsistent between eligible studies. Both of the above factors could be the origins of heterogeneity. Third, due to a lack of eligible data, subgroup analyses for BCR-FS based on tumor stage and various therapies were not be performed. Fourth, this meta-analysis included relatively few studies, and the total case number was not large enough. Fifth, most of the eligible studies included were retrospective in design.
Conclusions
In summary, our results clearly revealed that PD-L1 overexpression and mPD-L1 had value for predicting poor BCR-FS in PCa. Furthermore, the study also uncovered a significant correlation between PD-L1 overexpression and the clinicopathological features of CRPC: advanced tumor stage, higher Gleason score, positive surgical margin and positive AR status. These findings could be helpful for clinical decision making. Nevertheless, more multicenter prospective studies with large sample sizes, long observation periods and well-designed methods are required to draw a more reliable conclusion.
Materials and Methods
This meta-analysis was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) principles [51].
Literature search
The retrieve was conducted on PubMed, Cochrane Library, Web of Science and Embase to identify relevant articles published prior to March 23, 2020. The free text terms and medical subject headings (MeSH) terms used in search covered “prostate cancer” OR “prostate tumor” OR “prostate neoplasm” OR “prostate carcinoma”; “programmed death-ligand 1” OR “B7-H1” OR “programmed cell death-ligand 1” OR “CD274” OR “PD-L1”.
Inclusion and exclusion criteria
Two researchers (HS and JL) identified the titles, abstracts, and whole articles independently, with disagreements settled by discussion. The inclusion criteria were: (1) studies were published in English; (2) PCa was confirmed by histopathological examination; (3) PD-L1 protein or mPD-L1 was evaluated in PCa tissues; (4) the expression level of PD-L1 was assessed with positive (high) or negative (low) labels; (5) studies reported the relationship of PD-L1 and clinicopathological characteristics or prognosis. The exclusion criteria were: (1) studies only reported animals or in vitro experiments; (2) duplicate studies; (3) reviews, meta-analyses, meeting abstracts, expert opinions, letters, editorials, or case reports.
Data extraction
Data was collected by two reviewers (HS and JL) independently and differences were resolved by discussion. The data gathered were as follows: author name, publication year, country, size of the study population, age, preoperative PSA, Gleason score, tumor stage, nodal status, surgical margin, the expression level of PD-L1, hazard ratio (HR) and 95% confidence interval (CI) for BCR-FS, follow-up period, detection assay, evaluation method and cut-off value.
The Newcastle-Ottawa Scale (NOS) containing three domains: (1) selection; (2) comparability; (3) exposure or outcome, was implemented to evaluate the study quality [52]. High quality was considered when the score of NOS was more than 5.
Statistical analysis
Pooled HRs was calculated with 95% CIs to evaluate the PD-L1 value in prognosis of PCa patient. The odd ratios (ORs) with 95% CIs was computed to reveal the correlation between PD-L1 and clinicopathological factors. Patients were divided into two groups by age (>60 VS ≤60), preoperative PSA (>10 VS ≤10), surgical margin (R1 vs R0), tumor stage (pT3-T4 vs pT1-T2), nodal status (pN1 vs pN0), Gleason score (>8 vs ≤8) and androgen receptor (AR) expression (positive vs negative). Statistical heterogeneity of different studies was determined via employing the Chi-square-based Q statistics and I2 value [53]. If I2 > 50% and p < 0.1, the heterogeneity was considered to be high, then the random-effects model was implemented. If not, a fixed-effects model was applied.
We used Begg’s test to estimate the potential publication bias of included studies. All the statistical analyses were realized by STATA software (version 12.0, Stata Corp LP, TX77845, USA). Two-tailed p-value < 0.05 was regarded statistically significant.
Author Contributions
Study concept and design: Zhize Wang, Liping Xie; Acquisition of data: Haixiang Shen, Qinchen Li, Guoliang Sun, Libin Yan, Zhize Wang; Analysis and interpretation of data: Haixiang Shen, Jin Liu; Statistical analysis: Haixiang Shen, Jin Liu; Drafting of the manuscript: Haixiang Shen; Critical revision of the manuscript for important intellectual content: Zhize Wang, Liping Xie. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no potential conflicts of interest.
Funding
This study was not financed by any grants.
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019; 69:7–34. https://doi.org/10.3322/caac.21551 [PubMed]
- 2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. https://doi.org/10.3322/caac.21492 [PubMed]
- 3. Tsodikov A, Gulati R, Heijnsdijk EA, Pinsky PF, Moss SM, Qiu S, de Carvalho TM, Hugosson J, Berg CD, Auvinen A, Andriole GL, Roobol MJ, Crawford ED, et al. Reconciling the effects of screening on prostate cancer mortality in the ERSPC and PLCO trials. Ann Intern Med. 2017; 167:449–55. https://doi.org/10.7326/M16-2586 [PubMed]
- 4. Wong MC, Goggins WB, Wang HH, Fung FD, Leung C, Wong SY, Ng CF, Sung JJ. Global incidence and mortality for prostate cancer: analysis of temporal patterns and trends in 36 countries. Eur Urol. 2016; 70:862–74. https://doi.org/10.1016/j.eururo.2016.05.043 [PubMed]
- 5. Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, Stein KD, Alteri R, Jemal A. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016; 66:271–89. https://doi.org/10.3322/caac.21349 [PubMed]
- 6. Marin-Acevedo JA, Soyano AE, Dholaria B, Knutson KL, Lou Y. Cancer immunotherapy beyond immune checkpoint inhibitors. J Hematol Oncol. 2018; 11:8. https://doi.org/10.1186/s13045-017-0552-6 [PubMed]
- 7. Taube JM, Galon J, Sholl LM, Rodig SJ, Cottrell TR, Giraldo NA, Baras AS, Patel SS, Anders RA, Rimm DL, Cimino-Mathews A. Implications of the tumor immune microenvironment for staging and therapeutics. Mod Pathol. 2018; 31:214–34. https://doi.org/10.1038/modpathol.2017.156 [PubMed]
- 8. Finn OJ. Immuno-oncology: understanding the function and dysfunction of the immune system in cancer. Ann Oncol. 2012 (Suppl 8); 23:viii6–9. https://doi.org/10.1093/annonc/mds256 [PubMed]
- 9. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012; 12:252–64. https://doi.org/10.1038/nrc3239 [PubMed]
- 10. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu V, West AN, Carmona M, Kivork C, et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature. 2014; 515:568–71. https://doi.org/10.1038/nature13954 [PubMed]
- 11. Muenst S, Schaerli AR, Gao F, Däster S, Trella E, Droeser RA, Muraro MG, Zajac P, Zanetti R, Gillanders WE, Weber WP, Soysal SD. Expression of programmed death ligand 1 (PD-L1) is associated with poor prognosis in human breast cancer. Breast Cancer Res Treat. 2014; 146:15–24. https://doi.org/10.1007/s10549-014-2988-5 [PubMed]
- 12. Ma G, Deng Y, Jiang H, Li W, Wu Q, Zhou Q. The prognostic role of programmed cell death-ligand 1 expression in non-small cell lung cancer patients: an updated meta-analysis. Clin Chim Acta. 2018; 482:101–07. https://doi.org/10.1016/j.cca.2018.03.038 [PubMed]
- 13. Fukuda T, Kamai T, Masuda A, Nukui A, Abe H, Arai K, Yoshida K. Higher preoperative serum levels of PD-L1 and B7-H4 are associated with invasive and metastatic potential and predictable for poor response to VEGF-targeted therapy and unfavorable prognosis of renal cell carcinoma. Cancer Med. 2016; 5:1810–20. https://doi.org/10.1002/cam4.754 [PubMed]
- 14. Tsutsumi S, Saeki H, Nakashima Y, Ito S, Oki E, Morita M, Oda Y, Okano S, Maehara Y. Programmed death-ligand 1 expression at tumor invasive front is associated with epithelial-mesenchymal transition and poor prognosis in esophageal squamous cell carcinoma. Cancer Sci. 2017; 108:1119–27. https://doi.org/10.1111/cas.13237 [PubMed]
- 15. Lei C, Peng X, Gong X, Fan Y, Wu S, Liu N, Li L, Huang J, Zheng G, Long Z. Prognostic role of programmed death-ligand 1 expression in patients with biliary tract cancer: a meta-analysis. Aging (Albany NY). 2019; 11:12568–80. https://doi.org/10.18632/aging.102588 [PubMed]
- 16. Seo AN, Kang BW, Kwon OK, Park KB, Lee SS, Chung HY, Yu W, Bae HI, Jeon SW, Kang H, Kim JG. Intratumoural PD-L1 expression is associated with worse survival of patients with Epstein-Barr virus-associated gastric cancer. Br J Cancer. 2017; 117:1753–1760. https://doi.org/10.1038/bjc.2017.369 [PubMed]
- 17. Kaufman HL, Russell J, Hamid O, Bhatia S, Terheyden P, D’Angelo SP, Shih KC, Lebbé C, Linette GP, Milella M, Brownell I, Lewis KD, Lorch JH, et al. Avelumab in patients with chemotherapy-refractory metastatic merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016; 17:1374–85. https://doi.org/10.1016/S1470-2045(16)30364-3 [PubMed]
- 18. Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, Rodríguez-Abreu D, Moro-Sibilot D, Thomas CA, Barlesi F, Finley G, Kelsch C, Lee A, et al, and IMpower150 Study Group. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018; 378:2288–301. https://doi.org/10.1056/NEJMoa1716948 [PubMed]
- 19. Gevensleben H, Holmes EE, Goltz D, Dietrich J, Sailer V, Ellinger J, Dietrich D, Kristiansen G. PD-L1 promoter methylation is a prognostic biomarker for biochemical recurrence-free survival in prostate cancer patients following radical prostatectomy. Oncotarget. 2016; 7:79943–55. https://doi.org/10.18632/oncotarget.13161 [PubMed]
- 20. Gevensleben H, Dietrich D, Golletz C, Steiner S, Jung M, Thiesler T, Majores M, Stein J, Uhl B, Müller S, Ellinger J, Stephan C, Jung K, et al. The immune checkpoint regulator PD-L1 is highly expressed in aggressive primary prostate cancer. Clin Cancer Res. 2016; 22:1969–77. https://doi.org/10.1158/1078-0432.CCR-15-2042 [PubMed]
- 21. Ness N, Andersen S, Khanehkenari MR, Nordbakken CV, Valkov A, Paulsen EE, Nordby Y, Bremnes RM, Donnem T, Busund LT, Richardsen E. The prognostic role of immune checkpoint markers programmed cell death protein 1 (PD-1) and programmed death ligand 1 (PD-L1) in a large, multicenter prostate cancer cohort. Oncotarget. 2017; 8:26789–801. https://doi.org/10.18632/oncotarget.15817 [PubMed]
- 22. Li H, Wang Z, Zhang Y, Sun G, Ding B, Yan L, Liu H, Guan W, Hu Z, Wang S, Cheng F, Xu H, Zhang X, Ye Z. The immune checkpoint regulator PDL1 is an independent prognostic biomarker for biochemical recurrence in prostate cancer patients following adjuvant hormonal therapy. J Cancer. 2019; 10:3102–11. https://doi.org/10.7150/jca.30384 [PubMed]
- 23. Petitprez F, Fossati N, Vano Y, Freschi M, Becht E, Lucianò R, Calderaro J, Guédet T, Lacroix L, Rancoita PM, Montorsi F, Fridman WH, Sautès-Fridman C, et al. PD-L1 expression and CD8+ T-cell infiltrate are associated with clinical progression in patients with node-positive prostate cancer. Eur Urol Focus. 2019; 5:192–96. https://doi.org/10.1016/j.euf.2017.05.013 [PubMed]
- 24. Fankhauser CD, Schüffler PJ, Gillessen S, Omlin A, Rupp NJ, Rueschoff JH, Hermanns T, Poyet C, Sulser T, Moch H, Wild PJ. Comprehensive immunohistochemical analysis of PD-L1 shows scarce expression in castration-resistant prostate cancer. Oncotarget. 2017; 9:10284–93. https://doi.org/10.18632/oncotarget.22888 [PubMed]
- 25. Ebelt K, Babaryka G, Frankenberger B, Stief CG, Eisenmenger W, Kirchner T, Schendel DJ, Noessner E. Prostate cancer lesions are surrounded by FOXP3+, PD-1+ and B7-H1+ lymphocyte clusters. Eur J Cancer. 2009; 45:1664–72. https://doi.org/10.1016/j.ejca.2009.02.015 [PubMed]
- 26. Massari F, Ciccarese C, Caliò A, Munari E, Cima L, Porcaro AB, Novella G, Artibani W, Sava T, Eccher A, Ghimenton C, Bertoldo F, Scarpa A, et al. Magnitude of PD-1, PD-L1 and T lymphocyte expression on tissue from castration-resistant prostate adenocarcinoma: an exploratory analysis. Target Oncol. 2016; 11:345–51. https://doi.org/10.1007/s11523-015-0396-3 [PubMed]
- 27. Baas W, Gershburg S, Dynda D, Delfino K, Robinson K, Nie D, Yearley JH, Alanee S. Immune characterization of the programmed death receptor pathway in high risk prostate cancer. Clin Genitourin Cancer. 2017; 15:577–81. https://doi.org/10.1016/j.clgc.2017.04.002 [PubMed]
- 28. Calagua C, Russo J, Sun Y, Schaefer R, Lis R, Zhang Z, Mahoney K, Bubley GJ, Loda M, Taplin ME, Balk SP, Ye H. Expression of PD-L1 in hormone-naïve and treated prostate cancer patients receiving neoadjuvant abiraterone acetate plus prednisone and leuprolide. Clin Cancer Res. 2017; 23:6812–22. https://doi.org/10.1158/1078-0432.CCR-17-0807 [PubMed]
- 29. Haffner MC, Guner G, Taheri D, Netto GJ, Palsgrove DN, Zheng Q, Guedes LB, Kim K, Tsai H, Esopi DM, Lotan TL, Sharma R, Meeker AK, et al. Comprehensive evaluation of programmed death-ligand 1 expression in primary and metastatic prostate cancer. Am J Pathol. 2018; 188:1478–85. https://doi.org/10.1016/j.ajpath.2018.02.014 [PubMed]
- 30. Iacovelli R, Ciccarese C, Brunelli M, Bogina G, Munari E, Bimbatti D, Mosillo C, Fantinel E, Bria E, Martignoni G, Tortora G. PD-L1 expression in de novo metastatic castration-sensitive prostate cancer. J Immunother. 2019; 42:269–73. https://doi.org/10.1097/CJI.0000000000000287 [PubMed]
- 31. Sharma M, Yang Z, Miyamoto H. Immunohistochemistry of immune checkpoint markers PD-1 and PD-L1 in prostate cancer. Medicine (Baltimore). 2019; 98:e17257. https://doi.org/10.1097/MD.0000000000017257 [PubMed]
- 32. Xian P, Ge D, Wu VJ, Patel A, Tang WW, Wu X, Zhang K, Li L, You Z. PD-L1 instead of PD-1 status is associated with the clinical features in human primary prostate tumors. Am J Clin Exp Urol. 2019; 7:159–69. [PubMed]
- 33. Dong H, Zhu G, Tamada K, Chen L. B7-H1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nat Med. 1999; 5:1365–69. https://doi.org/10.1038/70932 [PubMed]
- 34. Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, Roche PC, Lu J, Zhu G, Tamada K, Lennon VA, Celis E, Chen L. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med. 2002; 8:793–800. https://doi.org/10.1038/nm730 [PubMed]
- 35. Mazanet MM, Hughes CC. B7-H1 is expressed by human endothelial cells and suppresses T cell cytokine synthesis. J Immunol. 2002; 169:3581–88. https://doi.org/10.4049/jimmunol.169.7.3581 [PubMed]
- 36. Chakravarti N, Prieto VG. Predictive factors of activity of anti-programmed death-1/programmed death ligand-1 drugs: immunohistochemistry analysis. Transl Lung Cancer Res. 2015; 4:743–51. https://doi.org/10.3978/j.issn.2218-6751.2015.12.10 [PubMed]
- 37. Nomi T, Sho M, Akahori T, Hamada K, Kubo A, Kanehiro H, Nakamura S, Enomoto K, Yagita H, Azuma M, Nakajima Y. Clinical significance and therapeutic potential of the programmed death-1 ligand/programmed death-1 pathway in human pancreatic cancer. Clin Cancer Res. 2007; 13:2151–57. https://doi.org/10.1158/1078-0432.CCR-06-2746 [PubMed]
- 38. Katsuya Y, Fujita Y, Horinouchi H, Ohe Y, Watanabe S, Tsuta K. Immunohistochemical status of PD-L1 in thymoma and thymic carcinoma. Lung Cancer. 2015; 88:154–59. https://doi.org/10.1016/j.lungcan.2015.03.003 [PubMed]
- 39. Karim R, Jordanova ES, Piersma SJ, Kenter GG, Chen L, Boer JM, Melief CJ, van der Burg SH. Tumor-expressed B7-H1 and B7-DC in relation to PD-1+ T-cell infiltration and survival of patients with cervical carcinoma. Clin Cancer Res. 2009; 15:6341–47. https://doi.org/10.1158/1078-0432.CCR-09-1652 [PubMed]
- 40. Berghoff AS, Kiesel B, Widhalm G, Rajky O, Ricken G, Wöhrer A, Dieckmann K, Filipits M, Brandstetter A, Weller M, Kurscheid S, Hegi ME, Zielinski CC, et al. Programmed death ligand 1 expression and tumor-infiltrating lymphocytes in glioblastoma. Neuro Oncol. 2015; 17:1064–75. https://doi.org/10.1093/neuonc/nou307 [PubMed]
- 41. Tamura H, Ishibashi M, Yamashita T, Tanosaki S, Okuyama N, Kondo A, Hyodo H, Shinya E, Takahashi H, Dong H, Tamada K, Chen L, Dan K, Ogata K. Marrow stromal cells induce B7-H1 expression on myeloma cells, generating aggressive characteristics in multiple myeloma. Leukemia. 2013; 27:464–72. https://doi.org/10.1038/leu.2012.213 [PubMed]
- 42. Jin X, Ding D, Yan Y, Li H, Wang B, Ma L, Ye Z, Ma T, Wu Q, Rodrigues DN, Kohli M, Jimenez R, Wang L, et al. Phosphorylated RB promotes cancer immunity by inhibiting NF-κB activation and PD-L1 expression. Mol Cell. 2019; 73:22–35.e6. https://doi.org/10.1016/j.molcel.2018.10.034 [PubMed]
- 43. Liu X, Shan C, Song Y, Du J. Prognostic value of programmed cell death ligand-1 expression in nasopharyngeal carcinoma: a meta-analysis of 1,315 patients. Front Oncol. 2019; 9:1111. https://doi.org/10.3389/fonc.2019.01111 [PubMed]
- 44. Wang Z, Peng S, Xie H, Guo L, Cai Q, Shang Z, Jiang N, Niu Y. Prognostic and clinicopathological significance of PD-L1 in patients with renal cell carcinoma: a meta-analysis based on 1863 individuals. Clin Exp Med. 2018; 18:165–75. https://doi.org/10.1007/s10238-018-0488-3 [PubMed]
- 45. Zeng Q, Liu Z, Liu T. Prognostic value and clinicopathological characteristics of PD-L1 overexpression in non-hodgkin lymphoma: a meta-analysis. BMC Cancer. 2020; 20:59. https://doi.org/10.1186/s12885-020-6550-z [PubMed]
- 46. Shen X, Zhao B. Efficacy of PD-1 or PD-L1 inhibitors and PD-L1 expression status in cancer: meta-analysis. BMJ. 2018; 362:k3529. https://doi.org/10.1136/bmj.k3529 [PubMed]
- 47. Patel MR, Ellerton J, Infante JR, Agrawal M, Gordon M, Aljumaily R, Britten CD, Dirix L, Lee KW, Taylor M, Schöffski P, Wang D, Ravaud A, et al. Avelumab in metastatic urothelial carcinoma after platinum failure (JAVELIN solid tumor): pooled results from two expansion cohorts of an open-label, phase 1 trial. Lancet Oncol. 2018; 19:51–64. https://doi.org/10.1016/S1470-2045(17)30900-2 [PubMed]
- 48. Powles T, O’Donnell PH, Massard C, Arkenau HT, Friedlander TW, Hoimes CJ, Lee JL, Ong M, Sridhar SS, Vogelzang NJ, Fishman MN, Zhang J, Srinivas S, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 open-label study. JAMA Oncol. 2017; 3:e172411. https://doi.org/10.1001/jamaoncol.2017.2411 [PubMed]
- 49. Balar AV, Galsky MD, Rosenberg JE, Powles T, Petrylak DP, Bellmunt J, Loriot Y, Necchi A, Hoffman-Censits J, Perez-Gracia JL, Dawson NA, van der Heijden MS, Dreicer R, et al, and IMvigor210 Study Group. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017; 389:67–76. https://doi.org/10.1016/S0140-6736(16)32455-2 [PubMed]
- 50. Li Y, Huang Q, Zhou Y, He M, Chen J, Gao Y, Wang X. The clinicopathologic and prognostic significance of programmed cell death ligand 1 (PD-L1) expression in patients with prostate cancer: a systematic review and meta-analysis. Front Pharmacol. 2019; 9:1494. https://doi.org/10.3389/fphar.2018.01494 [PubMed]
- 51. Moher D, Liberati A, Tetzlaff J, Altman DG, and PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097 [PubMed]
- 52. Stang A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25:603–05. https://doi.org/10.1007/s10654-010-9491-z [PubMed]
- 53. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–60. https://doi.org/10.1136/bmj.327.7414.557 [PubMed]