



Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disease. It is the most common form of dementia in the elderly, mainly characterized by the progressive decline in memory and cognitive function. AD can be classified as early-onset AD (EOAD, age at onset (AAO)<65 years) and late-onset AD (LOAD, AAO≥65 years). The etiology of AD is multifactorial and complex. Mutations in the amyloid precursor protein gene (APP), presenilin1 gene (PSEN1), and presenilin2 gene (PSEN2) are the leading causes for familial EOAD. Simultaneously, the convergence of genetic and environmental factors in aging is the primary drive for sporadic LOAD. Among multiple genetic factors associated with sporadic LOAD, apolipoprotein E (APOE) is the most critical risk factor [1, 2]. To date, genome-wide association studies have identified more than 50 AD-related genes/loci, shedding new light on the pathogenesis of AD [3].
It is well established that the Methylenetetrahydrofolate reductase (MTHFR) gene is critical for the folate cycle and homocysteine metabolism. Reduction and loss of MTHFR function lead to an elevated homocysteine level, which is considered a risk factor for AD. In addition, Hyperhomocysteinemia has also been linked to white matter signal abnormalities (WMSA) in magnetic resonance imaging (MRI), which is also recognized as a risk factor for AD [4, 5]. Recently, Hoffman et al. [6] proposed a novel mechanism leading to AD. The genetic MTHFR deficiency could enhance phosphorylation of amyloid-β protein precursor (AβPP) at Thr668, correlating with enhanced accumulation of demethylated protein phosphatase 2A (PP2A) and activation of glycogen synthase kinase-3β (GSK-3β), which was known to critically influence neuronal AβPP function and pathological amyloidogenic processing [6].
So far, three polymorphisms (C677T (rs1801133), A1298C (rs1801131), and A1793G (rs2274976)) of the MTHFR gene have been reported to be associated with AD. Among them, the C677T is the most significant polymorphism with most investigations in the clinic. The T allele prevalence (C677T) varied across ethnic groups and regions, with a range from 12% to 57% in European, Asian, American, and African populations [7, 8]. It should be pointed out that the C677T polymorphism was associated with increased susceptibility of AD in Asian and Caucasian populations [9–12]. However, there is still controversy over whether A1298C is related to the risk of AD. Previous studies have proposed that the A1298C polymorphism might play a protective role in developing AD in Indian and Japanese populations [13, 14], which was inconsistent with the Tunisian population's results reported by Mansouri et al. [15]. As for A1793G polymorphism, the protective effect was only confirmed in Japanese AD patients [13]. In the present study, we aimed to explore the genotype distributions of three polymorphisms and their associations with age at onset (AAO), homocysteine, and white matter lesions (WML) in the Chinese AD population.
Materials and Methods
Study subjects
A total of 721 patients with AD and 365 cognitively unimpaired control subjects were involved in the study (Table 1). AD patients were recruited from the Department of Neurology, Xiangya Hospital, Central South University (Hunan, China). All patients were clinically diagnosed by two experienced neurologists and met the National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer's Disease and Related Disorders Association criteria [16] for probable or definite AD. Among them, 121 AD patients performed homocysteine examinations and brain MRI scanning. Besides, 365 unaffected community-dwelling individuals without AD symptoms were recruited as healthy controls and matched for ethnicity and area of residence. The study was approved by the Ethics Committee of Xiangya Hospital, Central South University (institutional review board equivalent). Written informed consent was obtained from all participants involved in the study.
Table 1. Basic information of subjects.
| AD | Controls | P-value | |
| Numbers | 721 | 365 | |
| Age (years) | 65.80±10.91 | 70.65 ± 5.35 | 0.000 |
| Gender | |||
| Female | 426 (59.1%) | 190 (52.1%) | 0.027 |
| Male | 295 (40.9%) | 175 (48.0%) | |
| MMSE | 10.96 ± 7.30 | 27.79 ± 1.51 | 0.000 |
| APOE4 | |||
| APOE4 non-carriers | 409 (56.7%) | 293 (80.3%) | 0.000 |
| APOE4 carriers | 312 (43.3%) | 72 (19.7%) |
Genetic testing
Blood samples (10 mL per subject) were obtained by venipuncture from each subject and transferred to ethylenediaminetetraacetic acid (EDTA) tubes. Genomic DNA was isolated from peripheral blood leukocytes using a standard protocol [17]. All isolated DNA samples were measured for quality and quantity by a fluorometer and normalized to 50 ng/μL. Polymerase chain reaction (PCR) was performed on MTHFR (NM_001330358) C677T, A1298C, and A1793G polymorphisms. Primers for MTHFR and APOE genotypes amplification were shown in Supplementary Table 1. All PCR products were sequenced with Big Dye terminator v3.1 sequencing chemistry on an ABI 3730xl DNA analyzer (Applied Biosystems). DNA sequences were analyzed using the sequencing software of Mutation Surveyor (Softgenetics). Variants were checked against established databases (Genome Aggregation Database (gnomAD) and dbSNP v.150).
Homocysteine examinations
Venous blood samples were collected using standard venipuncture protocols after an overnight fast. The total plasma homocysteine level (umol/L, reference 0–20 umol/L) was measured by high-performance liquid chromatography within 3 hours of blood collection.
MRI data acquisitions and Fazekas score
Magnetic resonance imaging (MRI) data were acquired in a 3.0T Philips Achieva system (Philips Medical Systems), using a 3D T1-weighted Turbo Field Echo (TFE) sequence (RT = 7.2 ms, ET = 3.2 ms, flip angle=9°, number of slices=160, matrix size=250 × 250 mm, slice thickness=1.0 mm); and a 3D FLAIR sequence (RT = 48000 ms, ET = 280 ms, TI = 1650 ms, flip angle=90°, number of slices=140, matrix size=250 × 237 mm, slice thickness=2.0mm).
The Fazekas scale is a widely used method to visually rate hyperintense white matter signal abnormalities (WMSA) in MRI data. The Fazekas scale was applied on FLAIR MRI data on the axial plane and was scored following standard guidelines [18]. Briefly, Fazekas grades WMSA as 0 (i.e. absence of WMSA), 1 (i.e. punctate WMSA), 2 (i.e. early confluent WMSA), and 3 (i.e. WMSA in large confluent areas).
Statistical analyses
Descriptive statistics were described as the mean ± standard deviation. The Mann–Whitney U test was used to compare age and Mini-Mental State Examination (MMSE). The chi-square test was used to compare gender and the distribution of alleles and genotypes of MTHFR polymorphisms between AD patients and controls. The Bonferroni method was used to perform the pairwise test between multiple groups based on the chi-square test. Each subscript letter denotes a subset of intervention categories whose row/column proportions do not differ significantly from each other at the 0.05 level. For example, the group marked 'a' is not statistically significant from the other group marked 'a' (P > 0.05), and the group marked 'a' is statistical significantly from the group marked 'b' (P < 0.05). The Kruskal-Wallis test was used to confirm the significant difference in the AAO and homocysteine levels among different genotypes in AD patients. The chi-square test was used to determine the significant difference of Fazekas score among different genotypes in AD patients. The statistical analyses were performed by SPSS version 23.0. P < 0.05 was considered statistically significant.
Results
A total of 721 patients with AD and 365 cognitively unimpaired control subjects were involved in the study. The mean age of the AD group was 65.80 ± 10.91 years, and the proportion of females was 59.1%. The control group's mean age was 70.65 ± 5.35 years, and the ratio of females was 52.1%. In addition, the mean score of MMSE in AD patients was 10.96 ± 7.30, while in controls was 27.79 ± 1.51 (P = 0.000). The frequency of APOE4 carriers in AD patients (43.3%) was significantly higher than in controls (19.7%, P = 0.000) (Table 1). Moreover, 318 cases (44.1%) of the 721 patients were diagnosed as EOAD (AAO < 65) and 403 cases (55.9%) were LOAD (AAO ≥ 65). Among them, 121 AD patients performed homocysteine examinations and MRI data acquisition.
Distributions of MTHFR C677T, A1298C, and A1793G polymorphisms in AD patients and controls
The allele and genotype distributions of MTHFR C677T, A1298C, and A1793G polymorphisms of all participants were presented in Table 2. Allele T of the C677T polymorphism was significantly more frequent in the AD group (29.7%) than the control group (25.5%, P = 0.040). Moreover, the genotype distribution showed a significantly higher TT genotype in AD patients (6.1%) compared with controls (2.5%, P < 0.05). In terms of the A1298C polymorphism, allele C was more common in the AD group (19.0%) than the control group (16.7%), but no statistical difference was determined (P > 0.05). Furthermore, the distribution of genotypes showed a significantly higher percentage of CC genotype in the AD group (2.4%) compared with the control group (0.0%, P < 0.05). However, as for the A1793G polymorphism, no statistical difference was observed in the allele and genotype distributions between AD patients and controls (P > 0.05) (Table 2).
Table 2. Allele and genotype distributions of MTHFR polymorphisms in AD patients and controls.
| Total | C677T allele (%) | C677T genotype (%) | A1298C allele (%) | A1298C genotype (%) | A1793G allele (%) | A1793G genotype (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C | T | CC | CT | TT | A | C | AA | AC | CC | A | G | AA | AG | GG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AD | 721 | 1014 (70.3) | 428 (29.7) | 337 (46.7)a | 340 (47.2)a | 44 (6.1)b | 1168 (81.0) | 274 (19.0) | 464 (64.4)a | 240 (33.3)a | 17 (2.4)b | 1292 (89.6) | 150 (10.4) | 574 (79.6)a | 144 (20.0)a | 3 (0.4)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Controls | 365 | 544 (74.5) | 186 (25.5) | 188 (51.5)a | 168 (46.0)a | 9 (2.5)a | 608 (83.3) | 122 (16.7) | 243 (66.6)a | 122 (33.4)a | 0 (0.0)a | 665 (91.1) | 65 (8.9) | 300 (82.2)a | 65 (17.8)a | 0 (0.0)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P-value | 0.040 | 0.021 | 0.192 | 0.012 | 0.269 | 0.196 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a, b: each subscript letter denotes a subset of intervention categories whose row proportions do not differ significantly from each other at the 0.05 level (Bonferroni method). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The genotype distribution of the MTHFR gene in AD patients and controls was also determined after stratification of all samples by APOE4 status. In APOE4 carriers, the frequency for the T allele (C677T) was prominent in cases compared with controls (P = 0.039), and the distribution of the C677T genotypes was also significantly different (P = 0.047). At the same time, no statistical difference was determined in the A1298C and A1793G polymorphisms (P > 0.05). In APOE4 non-carriers, allele and genotype distributions of the A1298C polymorphism were significantly different between AD patients and controls (P = 0.044, P = 0.003, separately). Still, no statistical difference was found in C677T and A1793G polymorphisms (P > 0.05) (Table 3).
Table 3. Allele and genotype distributions of MTHFR polymorphisms in APOE4 carriers and non-carriers.
| Total | C677T allele (%) | C677T genotype (%) | A1298C allele (%) | A1298C genotype (%) | A1793G allele (%) | A1793G genotype (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C | T | CC | CT | TT | A | C | AA | AC | CC | A | G | AA | AG | GG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE4 carriers | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AD | 312 | 431 (69.1) | 193 (30.9) | 139 (44.6)a | 153 (49.7)a | 20 (9.4)a | 522 (83.7) | 102 (16.2) | 212 (67.9)a | 98 (31.4)a | 2 (0.6)a | 569 (91.2) | 55 (8.8) | 258 (82.7)a | 53 (17.0)a | 1 (0.3)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Controls | 72 | 112 (77.8) | 32 (22.2) | 41 (56.9)a | 30 (41.7)a | 1 (1.4)a | 120 (83.3) | 24 (16.7) | 48 (66.7)a | 24 (33.3)a | 0 (0.0)a | 131 (91.0) | 13 (9.0) | 59 (81.9)a | 13 (18.1)a | 0 (0.0)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P-value | 0.039 | 0.047 | 0.925 | 0.634 | 0.935 | 0.795 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE4 non-carriers | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| AD | 409 | 583 (71.3) | 235 (28.7) | 198 (48.4)a | 187 (45.7)a | 24 (5.9)b | 646 (79.0) | 172 (21.0) | 252 (61.6)a | 142 (34.7)a | 15 (3.7)b | 723 (88.4) | 95 (11.6) | 316 (77.3)a | 91 (22.2)a | 2 (0.5)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Controls | 293 | 432 (73.7) | 154 (26.3) | 147 (50.2)a | 138 (47.1)a | 8 (2.7)a | 488 (83.3) | 98 (16.7) | 195 (66.6)a | 98 (33.4)a | 0 (0.0)a | 534 (91.1) | 52 (8.9) | 241 (82.3)a | 52 (17.7)a | 0 (0.0)a | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P-value | 0.312 | 0.145 | 0.044 | 0.003 | 0.098 | 0.110 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a, b: each subscript letter denotes a subset of intervention categories whose column proportions do not differ significantly from each other at the 0.05 level (Bonferroni method). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Correlations of age at onset (AAO) with APOE4 or MTHFR polymorphisms in AD patients
After stratification of AD patients by AAO (EOAD (< 65 years) and LOAD (≥ 65 years)), AAO was significantly lower in LOAD patients carrying APOE 4/4 genotypes compared to APOE X/X genotype (lowered by 3.7 years, P = 0.015). As for MTHFR C677T polymorphism, AAO was significantly lower in LOAD patients carrying MTHFR CT/TT (C677T) genotypes compared to CC genotype (lowered by 1.2 years, P = 0.042). In terms of the A1298C polymorphism, AAO was significantly higher in LOAD patients carrying AC/CC (A1298C) genotypes (74.69 ± 5.78 years) compared to AA genotype (73.50 ± 5.93 years, P = 0.034). A similar pattern was observed in the A1793G polymorphism. AAO was significantly higher in LOAD patients carrying AG/GG (A1793G) genotypes (75.19 ± 5.56 years) compared to AA genotype (73.56 ± 5.95 years, P = 0.009). Nevertheless, no statistical difference was determined in all AD patients or EOAD patients (P > 0.05). (Figure 1A)
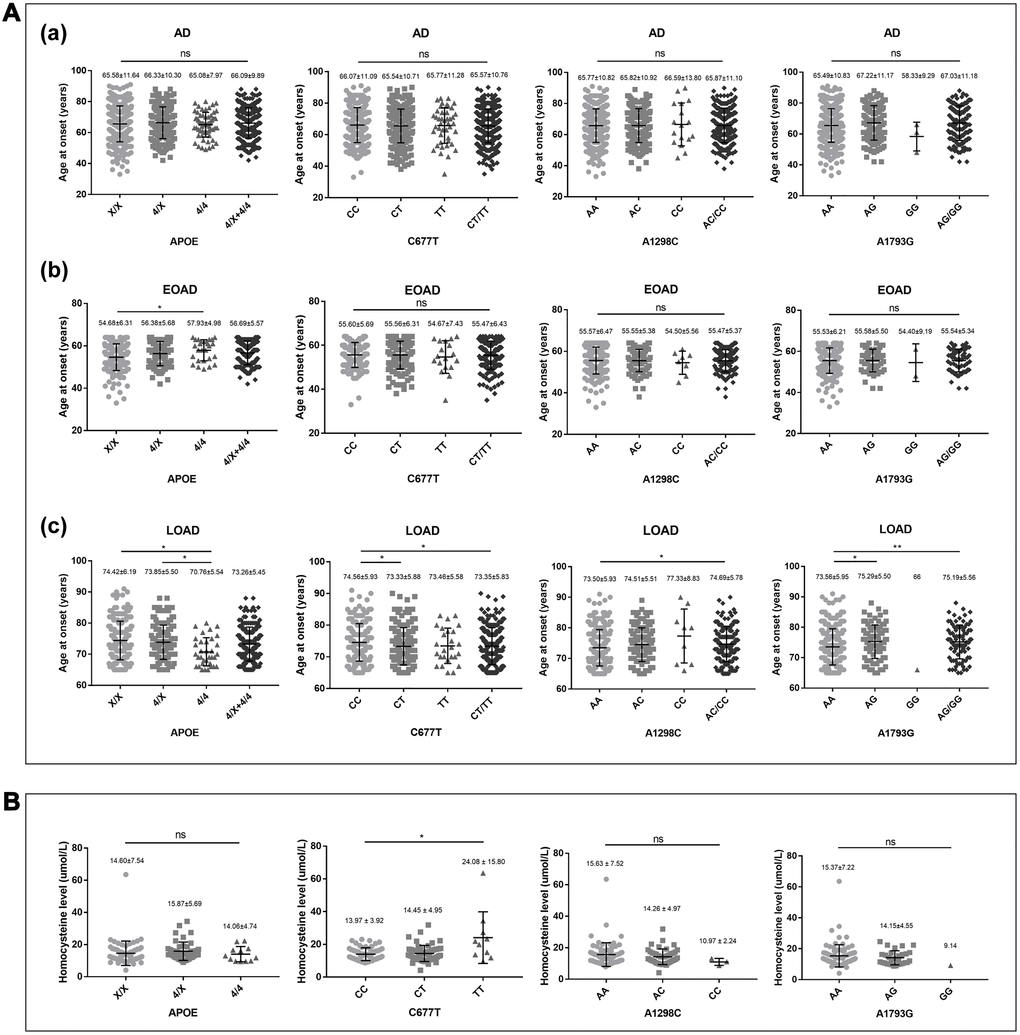
Figure 1. Correlations of AAO and homocysteine with APOE4, MTHFR C667T, A1298C, and A1793G genotypes in AD patients. (A) Correlation of AAO with APOE4, MTHFR C667T, A1298C, and A1793G genotypes in (a) AD (N = 721), (b) EOAD (N = 318), and (c) LOAD (N = 403). (B) Correlation of homocysteine with APOE4, MTHFR C667T, A1298C, and A1793G genotypes in AD (N = 121). Descriptive statistics were described as the mean ± standard deviation. Statistics performed by Kruskal-Wallis test, *p < 0.05, **p < 0.01; ns: no statistical difference.
Correlations of homocysteine with MTHFR polymorphisms in AD patients
The average level of homocysteine was 15.02 ± 6.65 umol/L in the 121 AD patients. AD patients with MTHFR TT (C677T) genotype (24.08 ± 15.60 umol/L) presented a significantly higher level of homocysteine compared to the CC genotype (13.97±3.92 umol/L, P = 0.036). Additionally, AD patients with CT (C677T) genotype (14.45 ± 4.95 umol/L) had a higher level of homocysteine compared to the CC genotype, but no statistical difference was observed (P > 0.05). In AC/CC (A1298C) carriers, the average levels of homocysteine (14.26 ± 4.97 umol/L and 10.97 ± 2.24 umol/L, respectively) were lower in comparison with AA (15.63 ± 7.52 umol/L), but no statistical difference was determined (P > 0.05). Similar to A1298C, the average levels of homocysteine were lower in AG/GG (A1793G) carriers (14.15 ± 4.55 umol/L and 9.14 umol/L, respectively) compared to AA (15.37 ± 7.22 umol/L), but no statistical difference was confirmed (P > 0.05). (Figure 1B)
Correlations of white matter lesions (WML) with MTHFR polymorphisms in AD patients
The Fazekas scale is a widely used method to visually assess white matter lesions (WML) in MRI data. The Fazekas score was significantly higher in AD patients carrying the MTHFR T allele (C677T) (P = 0.006), as well as TT (C677T) genotype (P = 0.024). In terms of the A1793G polymorphism, the Fazekas score was significantly lower in patients with AG/GG genotypes (P = 0.013). However, no statistical difference was determined in AD patients with A1298C polymorphism (P > 0.05). (Table 4)
Table 4. Correlations of WML with MTHFR C667T, A1298C and A1793G genotypes in AD patients (N = 121).
| C677T allele (%) | C677T genotype (%) | A1298C allele (%) | A1298C genotype (%) | A1793G allele (%) | A1793G genotype (%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C | T | CC | CT | TT | A | C | AA | AC | CC | A | G | AA | AG | GG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fazekas | 0 | 9 (5.4) | 1 (1.4) | 4 (7.0)a | 1 (1.9)a | 0 (0.0)a | 8 (4.2) | 2 (4.0) | 4 (5.4)a, b | 0 (0.0)b | 1 (33.3) a | 8 (3.8) | 2 (6.3) | 4 (4.4)a | 0 (0.0)a | 1 (100.0)b | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | 97 (57.7) | 29 (39.2) | 37 (64.9)a | 23 (42.6)a | 3 (30.0)a | 96 (50.0) | 30 (60.0) | 35 (47.3)a | 26 (59.1)a | 2 (66.7)a | 104 (49.5) | 22 (68.8) | 41 (45.6)a | 22 (73.3)b | 0 (0.0)a, b | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | 39 (23.2) | 31 (41.9) | 10 (17.5)a | 19 (35.2)a, b | 6 (60.0)b | 58 (30.2) | 12 (24.0) | 23 (31.1)a | 12 (27.3)a | 0 (0.0)a | 66 (31.4) | 4 (12.5) | 31 (34.4)a | 4 (13.3)a | 0 (0.0)a | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | 23 (13.7) | 13 (17.6) | 6 (10.5)a | 11 (20.4)a | 1 (10.0)a | 30 (15.6) | 6 (12.0) | 12 (16.2)a | 6 (13.6)a | 0 (0.0)a | 32 (15.2) | 4 (12.5) | 14 (15.6)a | 4 (13.3)a | 0 (0.0)a | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P value | 0.006 | 0.024 | 0.646 | 0.121 | 0.087 | 0.013 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a, b: each subscript letter denotes a subset of intervention categories whose column proportions do not differ significantly from each other at the 0.05 level (Bonferroni method). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Gene-gene interactions of MTHFR and APOE in AD patients
The allele C of the A1298C polymorphism was significantly more frequent in the APOE4 non-carriers (21.0%) than the APOE4 carriers (16.3%, P = 0.025) in AD patients. And the genotype distribution showed a significantly higher CC genotype (3.7%) in APOE4 non-carriers compared with APOE4 carriers (0.7%, P < 0.05). In terms of the C677T and A1793G polymorphisms, there was a lack of association between APOE4 and MTHFR polymorphisms in the Chinese AD population (P > 0.05). (Table 5)
Table 5. Gene-gene interactions of MTHFR and APOE in AD patients (N = 721).
| C677T allele (%) | C677T genotype (%) | A1298C allele (%) | A1298C genotype (%) | A1793G allele (%) | A1793G genotype (%) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| C | T | CC | CT | TT | A | C | AA | AC | CC | A | G | AA | AG | GG | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE4 carriers | 431 (69.1) | 193 (30.9) | 139 (44.6)a | 153 (49.0)a | 20 (6.4)a | 522 (83.7) | 102 (16.3) | 212 (67.9)a | 98 (31.4)a, b | 2 (0.7)b | 569 (91.2) | 55 (8.8) | 258 (82.7)a | 53 (17.0)a | 1 (0.3)a | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| APOE4 non-carriers | 583 (71.3) | 235 (28.7) | 198 (48.4)a | 187 (45.7)a | 24 (5.9)a | 646 (79.0) | 172 (21.0) | 252 (61.6)a | 142 (34.7)a, b | 15 (3.7)b | 723 (88.4) | 95 (11.6) | 316 (77.3)a | 91 (22.2)a | 2 (0.5)a | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| P value | 0.822 | 0.588 | 0.025 | 0.014 | 0.084 | 0.195 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| a, b: each subscript letter denotes a subset of intervention categories whose column proportions do not differ significantly from each other at the 0.05 level (Bonferroni method). | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Discussion
To our best knowledge, this is the first study to systematically analyze the genotype distribution of three MTHFR polymorphisms (C677T, A1298C, and A1793G) and their associations with AAO, homocysteine, and WML in the Chinese AD cohort. We found two polymorphisms, including C677T and A1298C, were associated with AD in Chinese populations. Moreover, in APOE4 carriers, the frequency of the allele T (C677T) was prominent in AD patients compared to controls, indicating that C677T might depend on the presence of APOE4.
Interestingly, the C677T polymorphism was associated with AAO, homocysteine, and WML, suggesting it may be a risk factor in developing AD. Several studies have documented that C677T resulted in a mildly dysfunctional thermolabile MTHFR enzyme, leading to reduced enzymatic activity and elevated blood homocysteine levels [19–21], suggesting it may play an important role in AD. In our results, we confirmed a significantly lower AAO in LOAD patients carrying CT/TT (C677T) genotypes, suggesting that C677T polymorphism was associated with susceptibility to LOAD. In contrast, AAO was significantly higher in LOAD patients carrying AC/CC (A1298C) and AG/GG (A1793G) genotypes, indicating A1298C and A1793G polymorphism may delay the onset of AD. Sutovsky et al. [22] reported that AAO in APOE4 non-carriers was higher than APOE4 carriers in AD patients (higher by 3.4 years), which was similar to our results (higher by 3.7 years in LOAD). Moreover, AAO in group of ‘APOE X/X + CC (C677T) + AA (A1298C)’ in AD patients was higher than group of ‘APOE 4/X + 4/4 + TT (C677T)’ or group of ‘APOE 4/X + 4/4 + CC (A1298C)’ (higher by 5.3 years and 2.9 years, separately). Combining the above two results, the single effect of TT (C677T) increased the difference in AAO (1.9 years), while CC (A1298C) decreased the difference in AAO (0.5 years), which was similar to our results (both 1.2 years in LOAD).
Consistent with previously reported results [23], the average level of homocysteine was significantly higher in TT (C677T) carriers in comparison with those of non-carriers (CC), suggesting that C677T polymorphism contributed to an elevated homocysteine level. In AC/CC (A1298C) and AG/GG (A1793G) carriers, the average level of homocysteine was lower in comparison with those of non-carriers (AA), but no statistical difference was determined. This trend indicated that the A1298C and A1793G might have an effect on lowering homocysteine. Moreover, the Fazekas score was higher in AD patients carrying CT/TT (C677T) genotypes, while the Fazekas score was higher in AD patients carrying AA (A1793G) genotype. These results showed that the C677T polymorphism was correlated with more severe WML, and A1793G polymorphism might contribute to milder WML. Like A1793G, the Fazekas score was higher in AD patients carrying AA (A1298C) genotype, while no statistical significance was determined. Considering that homocysteine and WML were determined by several factors in addition to MTHFR genotypes, including diet, lifestyle, and blood pressure [24, 25], more studies are required to confirm their associations in AD patients further.
There was a lack of association of the epistatic interaction between APOE4 and MTHFR C677T polymorphism, either in LOAD or EOAD (P > 0.05), which was inconsistent with previously reported results [22, 26]. These may depend on diverse characteristics of the study population, including ethnicity and geographical location. The APOE4 proportion was varied in different regions from 14.1% (lowest, Asia and Southern Europe) to 61.3% (highest, Northern Europe) [27]. The prevalence of APOE4 alleles in our AD patients was 43.3% compared with 75.2% in the reported positive study (75.2%) [22], which may explain the difference. However, a significantly higher frequency of MTHFR CC genotype (A1298C) was observed in APOE4 non-carriers in AD (p < 0.05), indicating that there may be an epistatic interaction between APOE4 and MTHFR A1298C polymorphism.
The MTHFR enzyme is a dimer where each monomer is composed of a catalytic domain that binds the FAD cofactor and folate, and a regulatory domain that binds S-adenosylmethionine. The 222 position in the polypeptide (corresponding to 677 in cDNA) resides in the catalytic domain, and the 429 position (1298 in cDNA) resides in the regulatory domain [20]. Vraneković et al. [28] reported that the 'C configuration' (formed by genotypes of 677CC and 1298CC) of the MTHFR enzyme was more stable than the 'E configuration' (formed by genotypes of 677TT and 1298AA). Our various results of the C667T and A1298C may be explained by the destabilization of the enzyme dimer, which could be caused by the altered polypeptide conformations, including the movement of polypeptide domains induced by the variants [28, 29]. Inspired by the model of C667T and A1298C discussed above, we speculated that A1793G might function in a similar way, which requires further investigation. Moreover, the N5-methyltetrahydrofolate could spontaneously release formaldehyde (FA) after a series of actions [30]. Several studies provided evidence that endogenous formaldehyde was closely related to AD, such as essential for Aβ self-aggregation [31–33]. And scavenging FA could be an effective strategy for treating AD [31]. Therefore, polymorphisms of the MTHFR gene may affect the development of AD by affecting the release of FA.
Conclusions
The genotype distributions of MTHFR C677T and A1298C polymorphisms are associated with AD in the Chinese population. Moreover, AD patients with C677T polymorphism are prone to present an earlier onset, higher homocysteine level, and more severe WML.
Supplementary Materials
Author Contributions
All authors contributed substantially to the preparation of this manuscript. Bin Jiao and Yaling Jiang were responsible for protocol design. Yaling Jiang, Xuewen Xiao, Yafei Wen, Meidan Wan, Lu Zhou, Xixi Liu, Xin Wang, Lina Guo, and Hui Liu were responsible for patients' recruitment and data acquisition. Yafang Zhou, Junling, Wang, Xinxin Liao, and Lu Shen contributed reagents and materials. Yaling Jiang and Xuewen Xiao were responsible for data analysis. All authors interpreted the data. Yaling Jiang and Bin Jiao wrote the manuscript. All authors revised and finalized the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This study was supported by the National Natural Science Foundation of China (No.81671075, 81971029 to Lu Shen, No.81701134, 82071216 to Bin Jiao, No. 81901171 to Xinxin Liao), the National Key R&D Program of China (No. 2017YFC0840100 and 2017YFC0840104 to Lu Shen, No. 2018YFC1312003 to Junling Wang), and the Youth Science Foundation of Xiangya Hospital (No. 2018Q020 to Xinxin Liao).
References
- 1. Bateman RJ, Aisen PS, De Strooper B, Fox NC, Lemere CA, Ringman JM, Salloway S, Sperling RA, Windisch M, Xiong C. Autosomal-dominant Alzheimer's disease: a review and proposal for the prevention of Alzheimer's disease. Alzheimers Res Ther. 2011; 3:1. https://doi.org/10.1186/alzrt59 [PubMed]
- 2. Lane CA, Hardy J, Schott JM. Alzheimer's disease. Eur J Neurol. 2018; 25:59–70. https://doi.org/10.1111/ene.13439 [PubMed]
- 3. Sims R, Hill M, Williams J. The multiplex model of the genetics of Alzheimer's disease. Nat Neurosci. 2020; 23:311–22. https://doi.org/10.1038/s41593-020-0599-5 [PubMed]
- 4. Hainsworth AH, Yeo NE, Weekman EM, Wilcock DM. Homocysteine, hyperhomocysteinemia and vascular contributions to cognitive impairment and dementia (VCID). Biochim Biophys Acta. 2016; 1862:1008–17. https://doi.org/10.1016/j.bbadis.2015.11.015 [PubMed]
- 5. Bilello M, Doshi J, Nabavizadeh SA, Toledo JB, Erus G, Xie SX, Trojanowski JQ, Han X, Davatzikos C. Correlating Cognitive Decline with White Matter Lesion and Brain Atrophy Magnetic Resonance Imaging Measurements in Alzheimer's Disease. J Alzheimers Dis. 2015; 48:987–94. https://doi.org/10.3233/jad-150400 [PubMed]
- 6. Hoffman A, Taleski G, Qian H, Wasek B, Arning E, Bottiglieri T, Sontag JM, Sontag E. Methylenetetrahydrofolate Reductase Deficiency Deregulates Regional Brain Amyloid-ß Protein Precursor Expression and Phosphorylation Levels. J Alzheimers Dis. 2018; 64:223–37. https://doi.org/10.3233/jad-180032 [PubMed]
- 7. Wilcken B, Bamforth F, Li Z, Zhu H, Ritvanen A, Renlund M, Stoll C, Alembik Y, Dott B, Czeizel AE, Gelman-Kohan Z, Scarano G, Bianca S, et al. Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. J Med Genet. 2003; 40:619–25. https://doi.org/10.1136/jmg.40.8.619 [PubMed]
- 8. Yang B, Liu Y, Li Y, Fan S, Zhi X, Lu X, Wang D, Zheng Q, Wang Y, Wang Y, Sun G. Geographical distribution of MTHFR C677T, A1298C and MTRR A66G gene polymorphisms in China: findings from 15357 adults of Han nationality. PLoS One. 2013; 8:e57917. https://doi.org/10.1371/journal.pone.0057917 [PubMed]
- 9. Zuin M, Cervellati C, Trentini A, Roncon L, Guasti P, Zuliani G. Methylenetetrahydrofolate reductase (MTHFR) C667T polymorphism and susceptibility to late-onset Alzheimer's disease in the Italian population. A systematic review and meta-analysis. Minerva Med. 2020. [Epub ahead of print]. https://doi.org/10.23736/s0026-4806.20.06801-9 [PubMed]
- 10. Yi J, Xiao L, Zhou SQ, Zhang WJ, Liu BY. The C677T Polymorphism of the Methylenetetrahydrofolate Reductase Gene and Susceptibility to Late-onset Alzheimer's Disease. Open Med (Wars). 2019; 14:32–40. https://doi.org/10.1515/med-2019-0006 [PubMed]
- 11. Durmaz A, Kumral E, Durmaz B, Onay H, Aslan GI, Ozkinay F, Pehlivan S, Orman M, Cogulu O. Genetic factors associated with the predisposition to late onset Alzheimer's disease. Gene. 2019; 707:212–15. https://doi.org/10.1016/j.gene.2019.05.030 [PubMed]
- 12. Rai V. Methylenetetrahydrofolate Reductase (MTHFR) C677T Polymorphism and Alzheimer Disease Risk: a Meta-Analysis. Mol Neurobiol. 2017; 54:1173–86. https://doi.org/10.1007/s12035-016-9722-8 [PubMed]
- 13. Wakutani Y, Kowa H, Kusumi M, Nakaso K, Yasui K, Isoe-Wada K, Yano H, Urakami K, Takeshima T, Nakashima K. A haplotype of the methylenetetrahydrofolate reductase gene is protective against late-onset Alzheimer's disease. Neurobiol Aging. 2004; 25:291–94. https://doi.org/10.1016/s0197-4580(03)00082-4 [PubMed]
- 14. Mansoori N, Tripathi M, Luthra K, Alam R, Lakshmy R, Sharma S, Arulselvi S, Parveen S, Mukhopadhyay AK. MTHFR (677 and 1298) and IL-6-174 G/C genes in pathogenesis of Alzheimer's and vascular dementia and their epistatic interaction. Neurobiol Aging. 2012; 33:1003.e1–8. https://doi.org/10.1016/j.neurobiolaging.2011.09.018 [PubMed]
- 15. Mansouri L, Fekih-Mrissa N, Klai S, Mansour M, Gritli N, Mrissa R. Association of methylenetetrahydrofolate reductase polymorphisms with susceptibility to Alzheimer's disease. Clin Neurol Neurosurg. 2013; 115:1693–96. https://doi.org/10.1016/j.clineuro.2013.03.015 [PubMed]
- 16. Dubois B, Feldman HH, Jacova C, Cummings JL, Dekosky ST, Barberger-Gateau P, Delacourte A, Frisoni G, Fox NC, Galasko D, Gauthier S, Hampel H, Jicha GA, et al. Revising the definition of Alzheimer's disease: a new lexicon. Lancet Neurol. 2010; 9:1118–27. https://doi.org/10.1016/s1474-4422(10)70223-4 [PubMed]
- 17. Jiang Y, Jiao B, Liao X, Xiao X, Liu X, Shen L. Analyses Mutations in GSN, CST3, TTR, and ITM2B Genes in Chinese Patients With Alzheimer's Disease. Front Aging Neurosci. 2020; 12:581524. https://doi.org/10.3389/fnagi.2020.581524 [PubMed]
- 18. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA. MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. AJR Am J Roentgenol. 1987; 149:351–56. https://doi.org/10.2214/ajr.149.2.351 [PubMed]
- 19. Hiraoka M, Kagawa Y. Genetic polymorphisms and folate status. Congenit Anom (Kyoto). 2017; 57:142–49. https://doi.org/10.1111/cga.12232 [PubMed]
- 20. Yamada K, Chen Z, Rozen R, Matthews RG. Effects of common polymorphisms on the properties of recombinant human methylenetetrahydrofolate reductase. Proc Natl Acad Sci U S A. 2001; 98:14853–58. https://doi.org/10.1073/pnas.261469998 [PubMed]
- 21. Frosst P, Blom HJ, Milos R, Goyette P, Sheppard CA, Matthews RG, Boers GJ, den Heijer M, Kluijtmans LA, van den Heuvel LP, Rozen R. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995; 10:111–13. https://doi.org/10.1038/ng0595-111 [PubMed]
- 22. Sutovsky S, Petrovic R, Fischerova M, Haverlikova V, Ukropcova B, Ukropec J, Turcani P. Allelic Distribution of Genes for Apolipoprotein E and MTHFR in Patients with Alzheimer's Disease and Their Epistatic Interaction. J Alzheimers Dis. 2020; 77:1095–105. https://doi.org/10.3233/jad-200321 [PubMed]
- 23. Ni J, Zhang L, Zhou T, Xu WJ, Xue JL, Cao N, Wang X. Association between the MTHFR C677T polymorphism, blood folate and vitamin B12 deficiency, and elevated serum total homocysteine in healthy individuals in Yunnan Province, China. J Chin Med Assoc. 2017; 80:147–53. https://doi.org/10.1016/j.jcma.2016.07.005 [PubMed]
- 24. Schneede J, Refsum H, Ueland PM. Biological and environmental determinants of plasma homocysteine. Semin Thromb Hemost. 2000; 26:263–79. https://doi.org/10.1055/s-2000-8471 [PubMed]
- 25. Nasrallah I, Pajewski N, Auchus A, Chelune G, Cheung A, Cleveland M, Coker L, Crowe M, Cushman W, Cutler J, Davatzikos C, Desiderio L, Doshi J, et al. Association of Intensive vs Standard Blood Pressure Control With Cerebral White Matter Lesions. JAMA. 2019; 322:524–34. https://doi.org/10.1001/jama.2019.10551 [PubMed]
- 26. Polito L, Poloni TE, Vaccaro R, Abbondanza S, Mangieri M, Davin A, Villani S, Guaita A. High homocysteine and epistasis between MTHFR and APOE: association with cognitive performance in the elderly. Exp Gerontol. 2016; 76:9–16. https://doi.org/10.1016/j.exger.2016.01.005 [PubMed]
- 27. Ward A, Crean S, Mercaldi CJ, Collins JM, Boyd D, Cook MN, Arrighi HM. Prevalence of apolipoprotein E4 genotype and homozygotes (APOE e4/4) among patients diagnosed with Alzheimer's disease: a systematic review and meta-analysis. Neuroepidemiology. 2012; 38:1–17. https://doi.org/10.1159/000334607 [PubMed]
- 28. Vraneković J, Babić Bozović I, Starcević Cizmarević N, Buretić-Tomljanović A, Ristić S, Petrović O, Kapović M, Brajenović-Milić B. Functional inference of methylenetetrahydrofolate reductase gene polymorphisms on enzyme stability as a potential risk factor for Down syndrome in Croatia. Dis Markers. 2010; 28:293–98. https://doi.org/10.3233/dma-2010-0704 [PubMed]
- 29. Guenther BD, Sheppard CA, Tran P, Rozen R, Matthews RG, Ludwig ML. The structure and properties of methylenetetrahydrofolate reductase from Escherichia coli suggest how folate ameliorates human hyperhomocysteinemia. Nat Struct Biol. 1999; 6:359–65. https://doi.org/10.1038/7594 [PubMed]
- 30. Thorndike J, Beck WS. Production of formaldehyde from N5-methyltetrahydrofolate by normal and leukemic leukocytes. Cancer Res. 1977; 37:1125–32. [PubMed]
- 31. Fei X, Zhang Y, Mei Y, Yue X, Jiang W, Ai L, Yu Y, Luo H, Li H, Luo W, Yang X, Lyv J, He R, et al. Degradation of FA reduces Aβ neurotoxicity and Alzheimer-related phenotypes. Mol Psychiatry. 2020. [Epub ahead of print]. https://doi.org/10.1038/s41380-020-00929-7 [PubMed]
- 32. Li ZH, He XP, Li H, He RQ, Hu XT. Age-associated changes in amyloid-β and formaldehyde concentrations in cerebrospinal fluid of rhesus monkeys. Zool Res. 2020; 41:444–48. https://doi.org/10.24272/j.issn.2095-8137.2020.088 [PubMed]
- 33. Tong Z, Han C, Qiang M, Wang W, Lv J, Zhang S, Luo W, Li H, Luo H, Zhou J, Wu B, Su T, Yang X, et al. Age-related formaldehyde interferes with DNA methyltransferase function, causing memory loss in Alzheimer's disease. Neurobiol Aging. 2015; 36:100–10. https://doi.org/10.1016/j.neurobiolaging.2014.07.018 [PubMed]