



Introduction
Cardiovascular disease (CVD) is one of the leading causes of mortality and morbidity worldwide. It has been reported that cardiovascular diseases caused 18.6 million deaths in 2019, accounting for about 30% of global deaths and imposing a huge economic burden on society [1, 2]. The major cardiovascular system diseases include myocardial infarction, heart failure, cardiomyopathy, atrial fibrillation, and valvular disease. Diabetes mellitus is an independent risk factor for the development of coronary heart disease. Long-term blood glucose abnormality leads to metabolic dysregulation, systemic inflammation, oxidative stress, and other risk factors, accelerating the development of atherosclerosis and cardiovascular disease [3, 4]. Diabetic patients often suffer from a combination of cardiovascular disease, so finding more drugs like Dagliflozin, a class of drugs that can both lower blood sugar and protect the cardiovascular system, has become the preferred choice [5–7]. Metformin, known as an AMP-activated protein kinase (AMPK) agonist, is a first-line drug for the treatment of type 2 diabetes [8, 9]. Although some existing studies have demonstrated a reduction in the incidence of heart failure and heart attacks in diabetic patients, there is still much uncertainty as to whether a direct reduction in the risk of cardiovascular disease can be achieved [10, 11]. The main reason for this is the inability to conduct a definitive placebo-controlled trial in diabetic patients with cardiovascular disease as an endpoint, especially in studies related to common valvular and cardiomyopathies, there is still a lack of clinical research trials to validate them [12].
Mendelian randomization (MR) studies use genetic variants that are strongly correlated with exposure factors as instrumental variables to assess causality between exposure factors and outcomes, are less susceptible to confounding and time-related bias, and are now increasingly used in studies of drug use and disease risk [13–15].
A two-sample Mendelian randomization analysis was used to elucidate the causal relationship between metformin treatment and common cardiovascular disease, providing new insights into the treatment of patients with diabetes combined with cardiovascular disease in clinical practice. To our knowledge, this is the first study to comprehensively explore metformin treatment and the risk of common cardiovascular disease disorders using Mendelian randomization analysis.
Materials and Methods
Study design
This study utilized metformin treatment as an exposure factor, single nucleotide polymorphisms (SNPs) with significant correlation with metformin as instrumental variables (IVs). Myocardial Infarction, Chronic Heart Failure, Atrial Fibrillation, Hypertrophic Cardiomyopathy, Dilated Cardiomyopathy, and valvular disease as outcome variables (Figure 1A). The two-sample MR applied in the present study was based on the genetic data obtained from the genome-wide association studies, which relied on three core assumptions: first, the SNPs used as IVs should be strongly associated with exposure; second, the selected SNPs must be independent of confounders; and finally, IVs are associated with the six diseases mentioned above only through metformin use (exposure) and not through direct association (Figure 1B) [16]. Meanwhile, the studies included in our analysis were approved by the relevant institutional review boards, and participants provided informed consent.
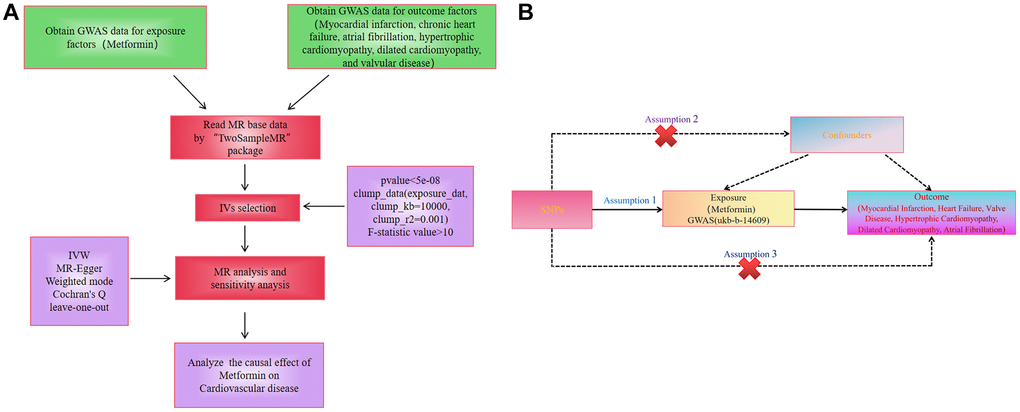
Figure 1. (A) Workflow of the study. (B) Diagram for Mendelian randomization (MR). MR is based on three hypotheses. The SNPs used as IVs should be strongly associated with exposure; second, the SNPs selected must be independent of confounders; and finally, IVs are associated with the six diseases mentioned above only through metformin use (exposure) and not through direct association.
Data sources and SNPs selection
All data covered in this study are available from genome-wide association studies (GWAS) (https://gwas.mrcieu.ac.uk/). Information related to the data can be found in Table 1. Data for metformin (ukb-b-14609) were derived from publicly available GWAS statistical outcomes data from 2018, which included 462,933 individuals, of whom 11,552 were cases and 451,381 were controls, with 9,851,867 SNPs. Myocardial Infarction (ebi-a-GCST90018877) data included 461,823 people, of whom 20,917 were cases and 440,906 controls, with 24,172,914 SNPs. Chronic Heart Failure (ebi-a-GCST90018586) data included 178,726 people, of whom 10,540 were cases and 168,186 controls, with 12,454,705 SNPs. Atrial Fibrillation (ebi-a-GCST006414) data included 1,030,836 people, of whom 11,552 were cases and 451,381 controls, with 33,519,037 SNPs. Data for Hypertrophic Cardiomyopathy (ukb-b-14609) included 489,727 people, of whom 507 were cases, 489,220 were biased people, of whom 1,444 were cases and 353,937 were controls, with 19,080,278 SNPs. The data for valvular disease (ebi-a-GCST90038612) included 484,598 people, of whom 3,742 were cases and 480,856 were controls, with 9,587,836 SNPs. The diagnostic criteria for all the diseases included in this study followed the International Classification of Diseases tenth version. The above databases include European populations and include both males and females.
Table 1. Source of the GWAS data.
| Exposure/Outcome | Database | Year | Author | Participants | Number of SNPs | Web Source if public |
| Metformin (ukb-b-14609) | UKB | 2018 | Ben Elsworth | 462,933 individuals (11,552 use cases and 451,381 controls) of European ancestry | 9,851,867 | |
| Myocardial infarction (ebi-a-GCST90018877) | EBI | 2021 | Sakaue S | 461,823 individuals (20,917 use cases and 440,906 controls) of European ancestry | 24,172,914 | |
| Chronic heart failure (ebi-a-GCST90018586) | EBI | 2021 | Sakaue S | 178,726 individuals (10,540 cases and 168,186 controls) of European ancestry | 12,454,705 | |
| Atrial fibrillation (/ebi-a-GCST006414) | EBI | 2018 | Nielsen JB | 1,030,836 individuals (60,620 cases and 970,216 controls) of European ancestry | 33,519,037 | |
| Hypertrophic cardiomyopathy (ebi-a-GCST90018861) | EBI | 2021 | Sakaue S | 489,727 individuals (507 cases and 489,220 controls) of European ancestry | 24,199,797 | |
| Dilated cardiomyopathy (ebi-a-GCST90018834) | EBI | 2021 | Sakaue S | 1,030,836 individuals (1,444 cases and 353,937 controls) of European ancestry | 19,080,278 | |
| Heart valve problem or heart murmur (/ebi-a-GCST90038612) | EBI | 2021 | NA | 484,598 individuals (3,742 cases and 480,856 controls) of European ancestry | 9,587,836 |
Instrumental variables
To avoid analysis bias caused by strong linkage disequilibrium among SNPs, the screening criteria were: (1) P < 5 × 10−8; (2) physical distance M > 10 000 kb between every two genes; (3) r2 threshold of LD between genes < 0.001. R2 is the proportion of variance in the exposure variable explained by the instrumental variable in the regression model. The R2 was calculated using the formula: R2 = β2(1−EAF) × 2EAF. EAF is the frequency of mutated genes. SNPs with F statistics >10 was defined as reliable and valid IVs. The F-statistic is calculated as: F = R2(N−K−1)/(K(1−R2)), K is the number of SNP-exposure association, and N is the sample size of the GWAS for the SNP-exposure association [17, 18].
Mendelian randomization analysis
In this study, the inverse variance weighting (IVW), MR-Egger regression, and weighted mode from the two-sample MR package were used for the analyses. IVW is the most commonly used test for calculating the weighted average of the effect values of all the instrumental variables, which provides similar estimation and precision as two-stage least squares, and therefore the results of the IVW analysis were the main focus.
Multi check calibration
This study performed multiple MR analyses, therefore Benjamini-Hochberg (BH) was chosen for multiple test correction. The BH method for multiple test correction was chosen to control the False Discovery Rate (FDR) and to be able to better maintain the efficacy of the statistical test, especially when dealing with a large number of comparisons.
Sensitivity analysis
This study used Cochran's Q statistic to test for heterogeneity. MR Egger intercept test and Mendelian randomization residual and outlier (MR-PRESSO) test were used to detect pleiotropy and remove outlier correction level pleiotropy. Leave-one-out analysis was used to assess whether the MR results were altered by a particular SNP.
Statistical analysis
All data analyses were performed using R software (version 4.3.1) and the R packages “TwosampleMR” (version 0.5.6, Mount Sinai, New York, NY, USA). MR-PRESSO test was accessed on October 8, 2023. Differences were considered statistically significant only when the p-value < 0.05.
Data availability statement
The original contributions presented in the study are included in the article, and further inquiries can be directed to the corresponding author.
Results
Genetic variant selection
Metformin was used as an exposure factor, and a total of 44 SNPs were obtained as instrumental variables by using R software to screen SNPs loci of genome-wide significance according to the screening criteria (Supplementary Table 1).
Causal effects of metformin treatment on cardiovascular diseases
IVW analysis showed a positive association between metformin treatment and myocardial infarction (OR = 22.67, 95% CI 3.22–34.01; P = 0.002). Meanwhile, IVW analysis showed that metformin treatment was positively associated with valvular disease (OR = 0.98, 95% CI 0.95–1.00; P = 0.046), whereas chronic heart failure (OR = 0.05, 95% CI 0.00–0.83; P = 0.037) and hypertrophic cardiomyopathy (OR = 0.01, 95% CI 0.00–0.22; P = 0.016) were negatively associated. The IVW also showed that metformin treatment was not significantly associated with the risk of developing atrial fibrillation (OR = 0.83, 95% CI 0.20–3.49; P = 0.798) and dilated cardiomyopathy (OR = 0.20, 95% CI 0.00–12.41; P = 0. 447) (Figure 2).
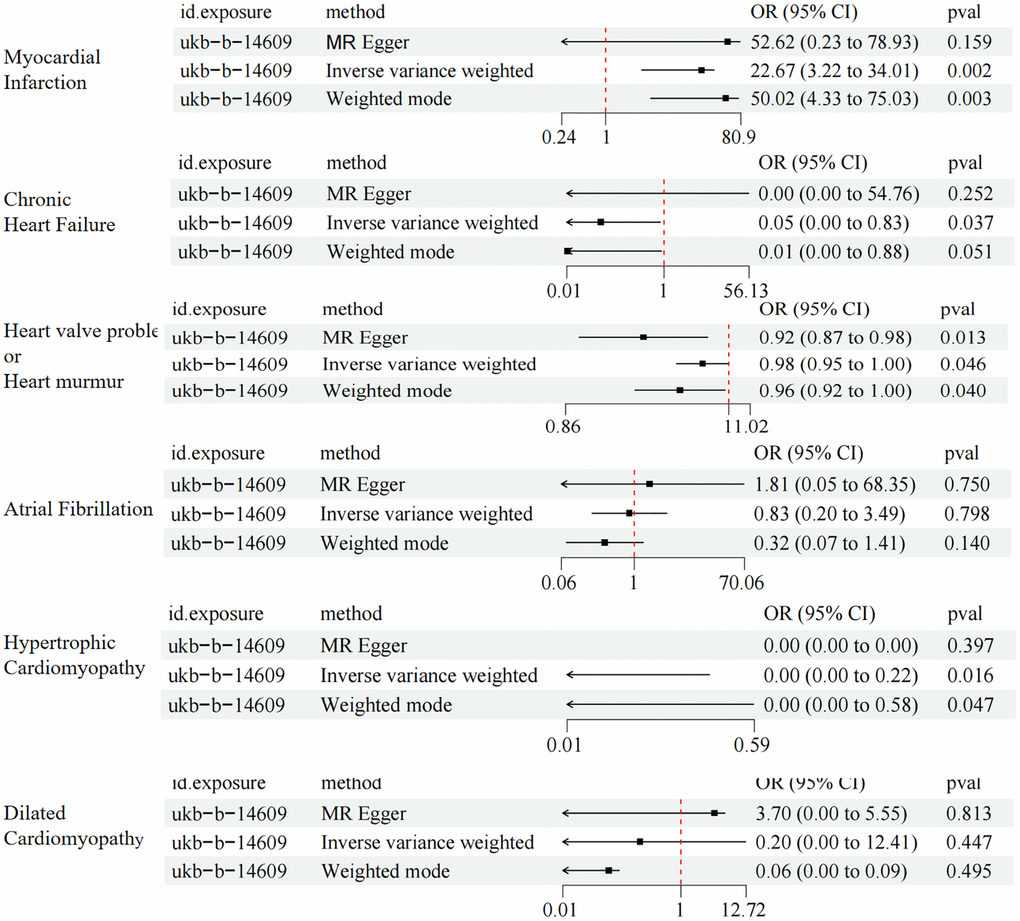
Figure 2. MR results of the causal association between metformin treatment and cardiovascular disease using three methods.
Results of multiple testing correction
After correction using the Benjamini-Hochberg method, treatment with metformin was found to have a causal relationship with the risk of developing hypertrophic cardiomyopathy (PFDR = 0.048) and myocardial infarction (PFDR = 0.012). However, there was no significant causal relationship between metformin treatment and the risk of heart failure, atrial fibrillation, valvular disease, and dilated cardiomyopathy (Table 2).
Table 2. Benjamini-Hochberg corrected.
| Outcome | P-value | Benjamini-Hochberg (PFDR) |
| Hypertrophic cardiomyopathy | 0.016 | 0.048 |
| Myocardial infarction | 0.002 | 0.012 |
| Heart valve problem or heart murmur | 0.046 | 0.069 |
| Chronic heart failure | 0.037 | 0.069 |
| Atrial fibrillation | 0.798 | 0.798 |
| Dilated cardiomyopathy | 0.447 | 0.536 |
Sensitivity analysis
The results of Cochran’s Q-test for heterogeneity are presented in Table 3. The analysis showed some heterogeneity between SNPs in metformin treatment and myocardial infarction (Q = 125, P = 0.001), chronic heart failure (Q = 60.6, P = 0.011), and atrial fibrillation (Q = 130, P = 0.001). P-value > 0.05 for all Test for directional horizontal pleiotropy. Meanwhile, in the analysis results of MR-PRESSO, it was found that there were multiple outliers when heart failure was the outcome variable, so this analysis result was excluded.
Table 3. Sensitivity analyses of the causal effect of metformin treatment on cardiovascular disease.
| Outcome | Test for directional horizontal pleiotropy | Cochran’s Q-Test | MR-PRESSO | |||
| Egger-intercept | SE | P-value | Q | Q-pval | ||
| Myocardial infarction (id: ebi-a-GCST90018877) | −0.003 | 0.008 | 0.745 | 125 | 0.001 | 0.121 |
| Chronic heart failure (id: ebi-a-GCST90018586) | 0.008 | 0.014 | 0.556 | 60.6 | 0.011 | 0.001 |
| Heart valve problem or heart murmur (id: ebi-a-GCST90038612) | 0 | 0 | 0.057 | 51.8 | 0.168 | 0.111 |
| Atrial fibrillation (id: ebi-a-GCST006414) | −0.003 | 0.005 | 0.647 | 130 | 0.001 | 0.001 |
| Hypertrophic cardiomyopathy (id: ebi-a-GCST90018861) | 0 | 0.026 | 0.993 | 27.3 | 0.962 | 0.990 |
| Dilated cardiomyopathy (id: ebi-a-GCST90018834) | −0.009 | 0.016 | 0.57 | 39.4 | 0.584 | 0.760 |
The Fixed-effect IVW analysis of the causal association of metformin treatment and cardiovascular diseases was also presented (Figure 3). The black dots and bars indicate the causal estimate and 95% CI using each SNP. Scatter plot of the effects of genetic variants on the metformin treatment and cardiovascular diseases is shown. The slopes of the solid lines denote the magnitudes of the associations estimated from the MR analysis (Figure 4). The symmetry of the funnel plot also indicated the same result (Figure 5). Furthermore, leave-one-out sensitivity testing showed that the causal effect of metformin treatment on cardiovascular diseases was not significantly affected by the omission of any single SNP (Figure 6). The results of the causal effect of metformin treatment on cardiovascular diseases can be shown to be stable and reliable.
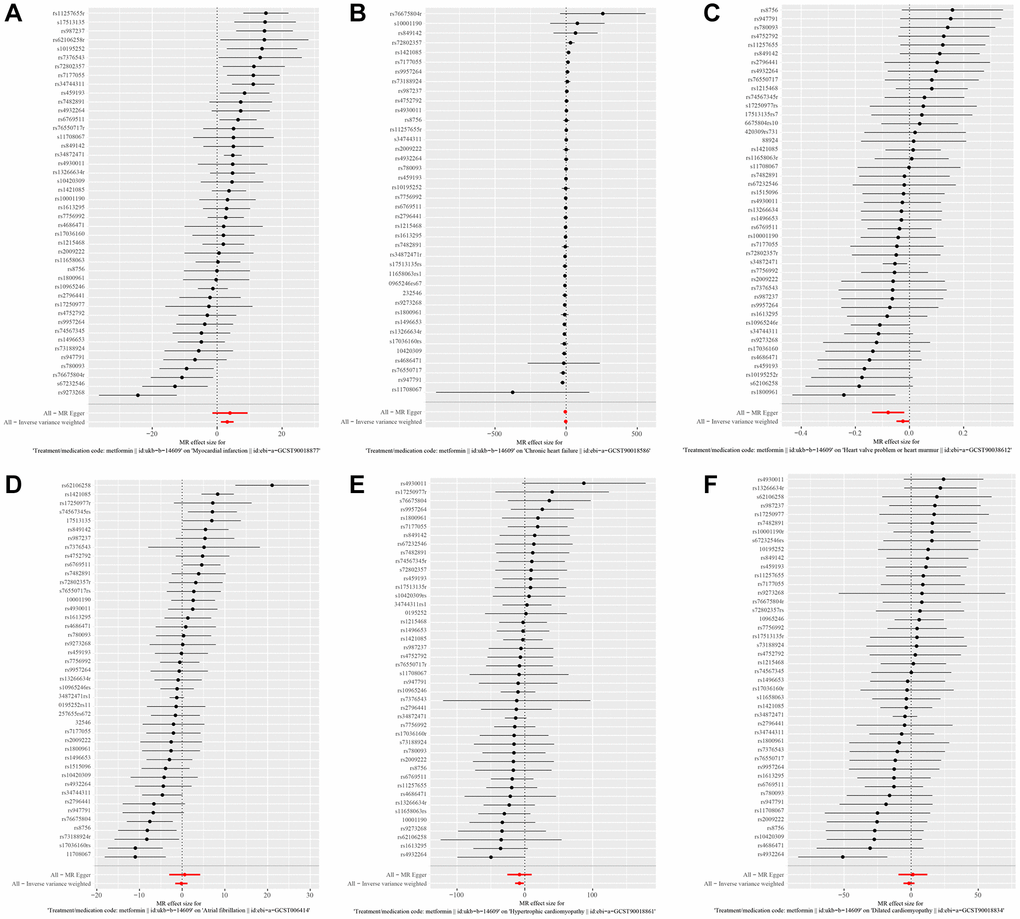
Figure 3. (A–F) show the fixed-effect IVW analysis of the causal association of metformin with Myocardial Infarction, Chronic Heart Failure, Atrial Fibrillation, Hypertrophic Cardiomyopathy, Dilated Cardiomyopathy, and valvular disease.
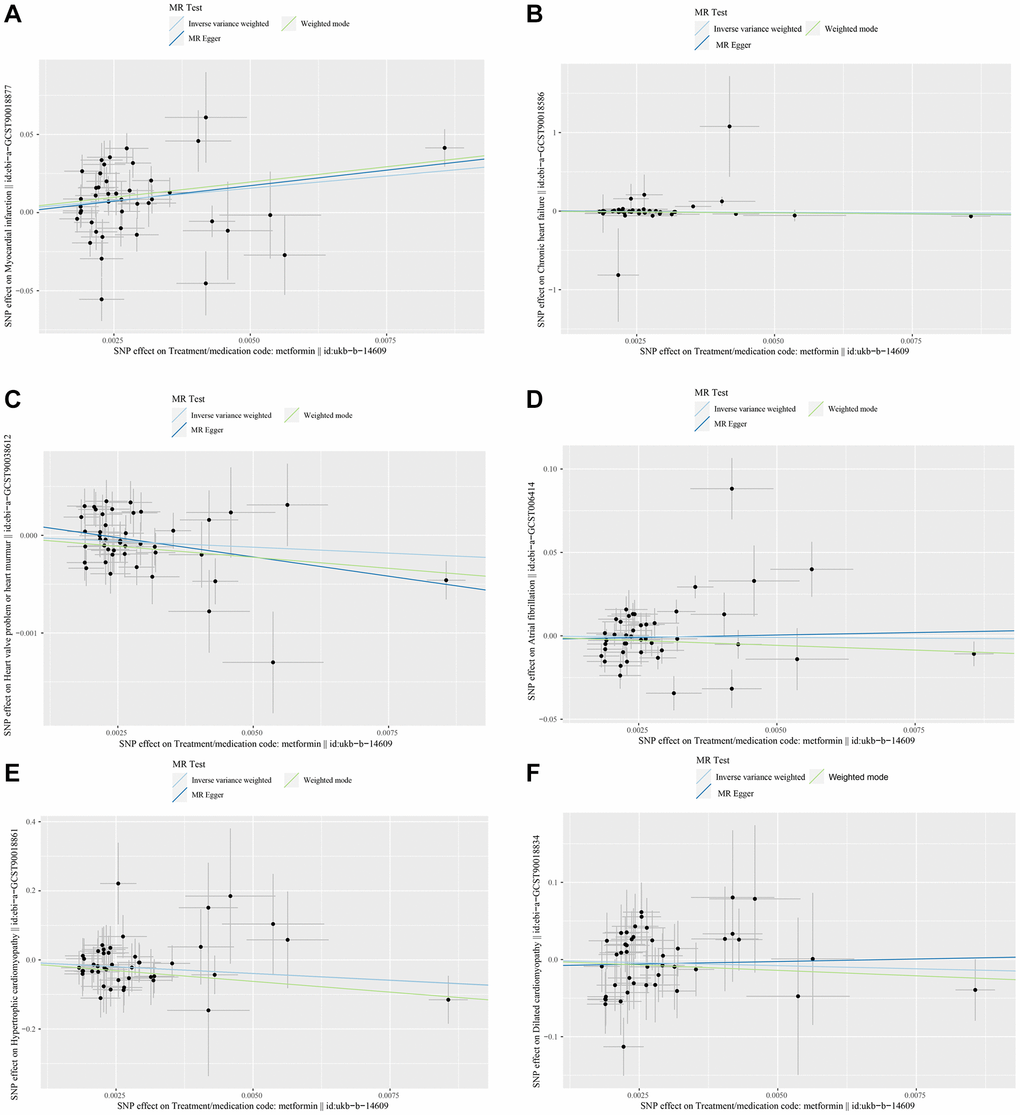
Figure 4. (A–F) show scatter plots of the effect of genetic variation on the effect of metformin treatment on Myocardial Infarction, Chronic Heart Failure, Atrial Fibrillation, Hypertrophic Cardiomyopathy, Dilated Cardiomyopathy, and valvular disease.
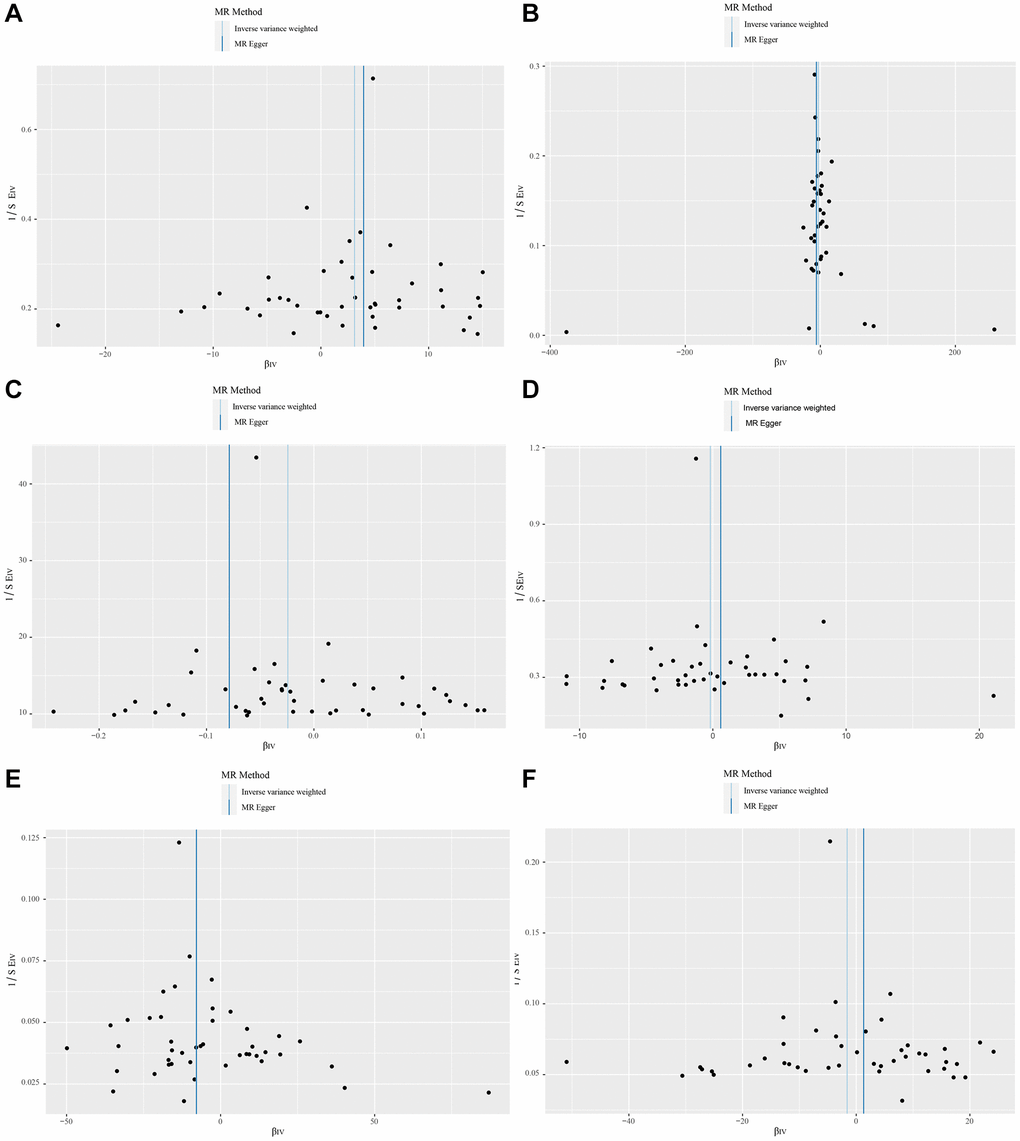
Figure 5. (A–F) show funnel plots of the causal effects of metformin on Myocardial Infarction, Chronic Heart Failure, Atrial Fibrillation, Hypertrophic Cardiomyopathy, Dilated Cardiomyopathy, and valvular disease.
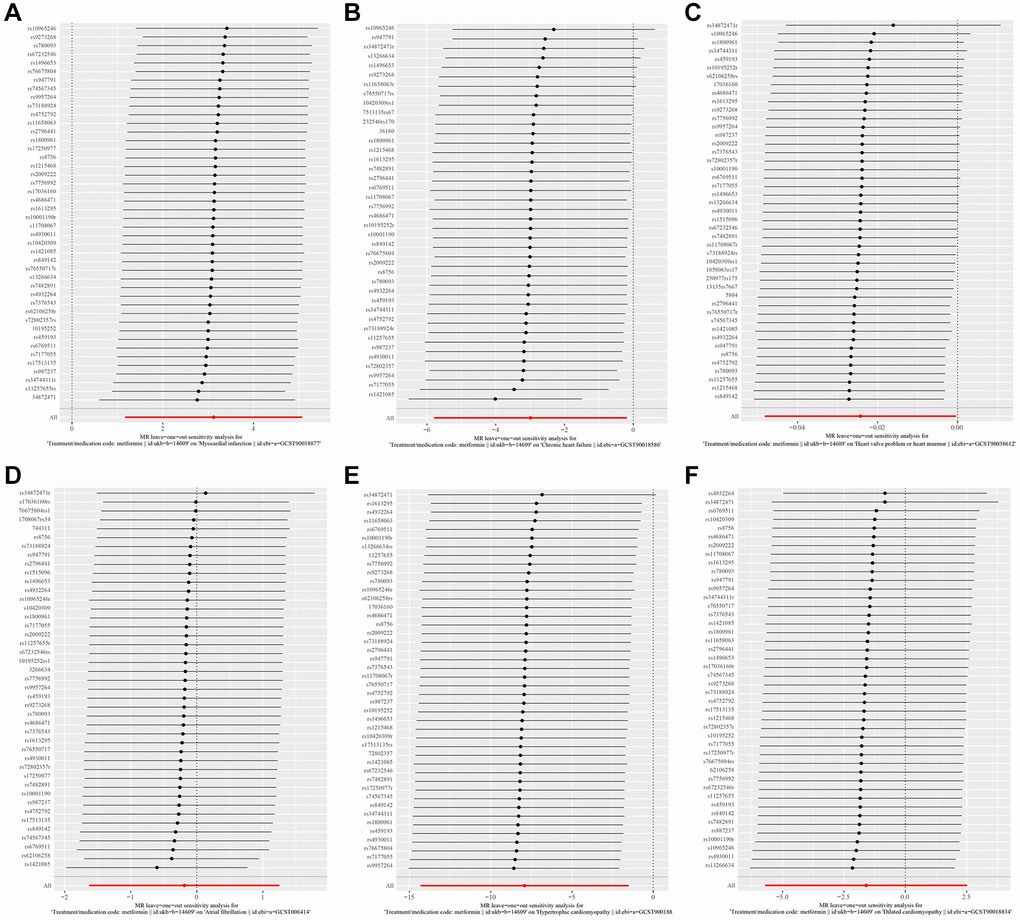
Figure 6. (A–F) show leave-one-out analysis plots of metformin on Myocardial Infarction, Chronic Heart Failure, Atrial Fibrillation, Hypertrophic Cardiomyopathy, Dilated Cardiomyopathy, and valvular disease.
Discussion
In practice, even though metformin can cause side effects such as acidosis, nausea, abdominal discomfort, and diarrhea, it is still worthwhile to study its mechanism of action in depth, as opposed to the “beneficial” effects of metformin [19]. In a series of studies such as the prevention of rheumatoid arthritis, metformin has been shown to not only lower blood glucose, but also reduce body weight and indirectly inhibit inflammation by altering the intestinal flora, thus reducing the risk of developing a number of diseases [20–24]. Available studies have demonstrated that metformin acts not only through AMP-activated protein kinase, but also through mitochondrial complex 1, growth differentiation factor 15, and glucagon-like peptide 1/glucagon [25–28]. At the same time, many basic studies have demonstrated that metformin can play a cardiovascular protective role by reducing endothelial dysfunction and reducing oxidative stress to improve inflammation [29]. Unfortunately, however, metformin is still not classified as a cardiovascular drug [30–34]. Meanwhile, most clinical studies have focused on studying the incidence of heart attack and heart failure with metformin, and there have been more studies demonstrating that metformin reduces mortality in patients with heart failure and heart attack, but relatively few studies have been done on other common heart diseases [35–37].
This study conducted a MR analysis utilizing the GWAS database. The endpoints of our research encompassed not only myocardial infarction and heart failure, but also four commonly seen clinical diseases: atrial fibrillation, valvular disease, hypertrophic cardiomyopathy, and dilated cardiomyopathy. Unexpectedly, this study revealed that metformin increased the incidence of myocardial infarction, contradicting the majority of existing studies. Currently, most research suggests that metformin can reduce endothelial inflammation and lower total cholesterol and LDL levels in the blood, playing a crucial role in mitigating the risk of myocardial infarction [38]. However, some studies argue that metformin, by activating AMP-activated protein kinase, affects energy metabolism, potentially leading to insufficient energy in cardiac cells, thereby increasing the risk of myocardial infarction. Additionally, this study indicates that metformin might affect blood viscosity or the deformability of red blood cells, and indicates changes that could lead to microcirculatory disorders and increased risk of cardiac tissue ischemia [39, 40]. This study offers a genetic variant perspective on why metformin might increase the risk of myocardial infarction, identifying 44 significant SNPs, though further research is required to understand the underlying mechanisms. This study found that metformin treatment may reduce the risk of heart failure. However, due to the existence of horizontal pleiotropy, the results of this analysis can only be excluded. Even so, there are still studies that have found that metformin can reduce the cardiovascular risk associated with insulin resistance, so new data need to be collected for MR analysis in the future [41].
Interestingly, the MR analysis introduced a novel perspective: metformin usage can reduce the risk of hypertrophic cardiomyopathy and valvular disease but shows no causal relationship with the risk of dilated cardiomyopathy. This is an unprecedented conclusion in research. The risk of developing hypertrophic cardiomyopathy, apart from genetic factors, is closely associated with high blood pressure, valvular disease, and cardiac remodeling. Thus, we hypothesize that metformin’s anti-inflammatory and anti-oxidative stress effects may protect blood vessels, indirectly reducing blood pressure and valvular damage. The mechanisms might relate to metformin’s activation of the AMPK and β-catenin pathways, with exact mechanisms awaiting further exploration, but undoubtedly closely connected with the 44 identified SNPs [42, 43].
After Benjamini-Hochberg adjustment, treatment with metformin remains significantly associated with the risk of myocardial infarction and hypertrophic cardiomyopathy, further indicating strong genetic evidence supporting the potential impact of metformin on myocardial infarction and hypertrophic cardiomyopathy. However, post-adjustment, no significant causal relationship was found between metformin and heart failure, valvular disease, or hypertrophic cardiomyopathy, which may be due to the relatively weaker effects on these diseases or the genetic instrumental variables not being strongly associated with these conditions, so that these causal relationships could not be established after adjusting for the risk of multiple comparisons. In addition, although the results changed after adjustment, the outcomes obtained after multiple corrections are generally more conservative. This also suggests that future studies may require larger sample sizes or stronger genetic instrumental variables for validation.
The strengths of the study lie in its basis on a large-scale MR analysis from a public database, reducing susceptibility to confounding factors. Additionally, robust estimations of each instrumental variable effect (with F-statistics greater than 10) prevent potential weak instrument bias. Furthermore, relevant heterogeneity and sensitivity analyses have been conducted, all affirming the reliability of the results. Additionally, this study sheds light on the protective effects of metformin against hypertrophic cardiomyopathy and valvular disease, adding a new dimension to the therapeutic implications of this widely used diabetes medication. These findings highlight the need for further investigation into the nuanced and multifaceted impact of metformin on cardiovascular health.
Limitations of the study
The present study still has some limitations. First, MR-PRESSO analysis of atrial fibrillation and heart failure revealed possible horizontal multi directionality of SNPs, which may be due to factors such as the composition of the control group and the time period of sample collection. Second, although our study was groundbreaking in suggesting a protective effect of metformin against hypertrophic cardiomyopathy and valvular disease, no causal relationship was found between metformin and dilated cardiomyopathy. Dilated cardiomyopathy is also strongly influenced by genetic factors, which warrants further research. Third, genetic variation exists between populations on different continents, and our study participants were all European, so the applicability of our findings to all ethnic groups may be limited. Finally, because the exposure factor in this study was a drug treatment, meaningful bidirectional MR analyses could not be performed.
Future directions for clinical research
First, this study screened 44 SNPs associated with metformin treatment, providing a genetic variant perspective for understanding how metformin affects cardiovascular disease risk. These findings may contribute to the future development of genetically based risk assessment tools to guide metformin use, particularly in patients with a genetic predisposition to CVD. Second, given that metformin may have different effects on different cardiovascular diseases, future studies should conduct more detailed long-term observations while expanding the study population to better understand the effects of long-term metformin use on cardiovascular health.
Conclusions
This study reveals the complex effects of metformin treatment on common cardiovascular diseases from a genetic perspective. While it is consistent with previous research in reducing the risk of heart failure, surprisingly, the use of metformin may increase the incidence risk of myocardial infarction, a finding that deviates from the established understanding of metformin’s cardiovascular impacts. Furthermore, the study found that the use of metformin could potentially lower the incidence risk of hypertrophic cardiomyopathy and valvular disease, but further verification is needed.
Supplementary Materials
Author Contributions
This study was designed by P.L. All authors contributed to the data collection and analysis. K.L. and P.L and J.Y wrote the first draft of the paper. M.L and L.Z revised the article. The final manuscript was approved by all authors. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
We sincerely appreciate the data provided by the GWAS website.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical Statement
All the data utilized in this investigation are publicly accessible and provided by the public domains. All participants were granted informed consent, and the study protocols received approval from their relevant ethical institutions.
Funding
This work was supported by the Clinical Specialist Talents’ Professional Ability Innovation and Application Research Project (No. RCLX2315029) and the 2022 Taizhou Science and Technology Support Program (Social Development) Project (No. TS202219).
References
- 1. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, et al, and American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018; 137:e67–492. https://doi.org/10.1161/CIR.0000000000000558 [PubMed]
- 2. Lloyd-Jones DM, Braun LT, Ndumele CE, Smith SC
Jr , Sperling LS, Virani SS, Blumenthal RS. Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease: A Special Report From the American Heart Association and American College of Cardiology. J Am Coll Cardiol. 2019; 73:3153–67. https://doi.org/10.1016/j.jacc.2018.11.005 [PubMed] - 3. Avogaro A, Giorda C, Maggini M, Mannucci E, Raschetti R, Lombardo F, Spila-Alegiani S, Turco S, Velussi M, Ferrannini E, and Diabetes and Informatics Study Group, Association of Clinical Diabetologists, Istituto Superiore di Sanità. Incidence of coronary heart disease in type 2 diabetic men and women: impact of microvascular complications, treatment, and geographic location. Diabetes Care. 2007; 30:1241–7. https://doi.org/10.2337/dc06-2558 [PubMed]
- 4. Luo F, Das A, Chen J, Wu P, Li X, Fang Z. Metformin in patients with and without diabetes: a paradigm shift in cardiovascular disease management. Cardiovasc Diabetol. 2019; 18:54. https://doi.org/10.1186/s12933-019-0860-y [PubMed]
- 5. Arow M, Waldman M, Yadin D, Nudelman V, Shainberg A, Abraham NG, Freimark D, Kornowski R, Aravot D, Hochhauser E, Arad M. Sodium-glucose cotransporter 2 inhibitor Dapagliflozin attenuates diabetic cardiomyopathy. Cardiovasc Diabetol. 2020; 19:7. https://doi.org/10.1186/s12933-019-0980-4 [PubMed]
- 6. Lee SG, Kim D, Lee JJ, Lee HJ, Moon RK, Lee YJ, Lee SJ, Lee OH, Kim C, Oh J, Lee CJ, Lee YH, Park S, et al. Dapagliflozin attenuates diabetes-induced diastolic dysfunction and cardiac fibrosis by regulating SGK1 signaling. BMC Med. 2022; 20:309. https://doi.org/10.1186/s12916-022-02485-z [PubMed]
- 7. Blair HA. Dapagliflozin: A Review in Symptomatic Heart Failure with Reduced Ejection Fraction. Am J Cardiovasc Drugs. 2021; 21:701–10. https://doi.org/10.1007/s40256-021-00503-8 [PubMed]
- 8. Lv Z, Guo Y. Metformin and Its Benefits for Various Diseases. Front Endocrinol (Lausanne). 2020; 11:191. https://doi.org/10.3389/fendo.2020.00191 [PubMed]
- 9. Bailey CJ. Metformin: historical overview. Diabetologia. 2017; 60:1566–76. https://doi.org/10.1007/s00125-017-4318-z [PubMed]
- 10. Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia. 2017; 60:1577–85. https://doi.org/10.1007/s00125-017-4342-z [PubMed]
- 11. Ritsinger V, Malmberg K, Mårtensson A, Rydén L, Wedel H, Norhammar A. Intensified insulin-based glycaemic control after myocardial infarction: mortality during 20 year follow-up of the randomised Diabetes Mellitus Insulin Glucose Infusion in Acute Myocardial Infarction (DIGAMI 1) trial. Lancet Diabetes Endocrinol. 2014; 2:627–33. https://doi.org/10.1016/S2213-8587(14)70088-9 [PubMed]
- 12. Griffin SJ, Leaver JK, Irving GJ. Impact of metformin on cardiovascular disease: a meta-analysis of randomised trials among people with type 2 diabetes. Diabetologia. 2017; 60:1620–9. https://doi.org/10.1007/s00125-017-4337-9 [PubMed]
- 13. Luo S, Schooling CM, Wong ICK, Au Yeung SL. Evaluating the impact of AMPK activation, a target of metformin, on risk of cardiovascular diseases and cancer in the UK Biobank: a Mendelian randomisation study. Diabetologia. 2020; 63:2349–58. https://doi.org/10.1007/s00125-020-05243-z [PubMed]
- 14. Zheng J, Xu M, Walker V, Yuan J, Korologou-Linden R, Robinson J, Huang P, Burgess S, Au Yeung SL, Luo S, Holmes MV, Davey Smith G, Ning G, et al. Evaluating the efficacy and mechanism of metformin targets on reducing Alzheimer's disease risk in the general population: a Mendelian randomisation study. Diabetologia. 2022; 65:1664–75. https://doi.org/10.1007/s00125-022-05743-0 [PubMed]
- 15. Sekula P, Del Greco M F, Pattaro C, Köttgen A. Mendelian Randomization as an Approach to Assess Causality Using Observational Data. J Am Soc Nephrol. 2016; 27:3253–65. https://doi.org/10.1681/ASN.2016010098 [PubMed]
- 16. Mingdong W, Xiang G, Yongjun Q, Mingshuai W, Hao P. Causal associations between gut microbiota and urological tumors: a two-sample mendelian randomization study. BMC Cancer. 2023; 23:854. https://doi.org/10.1186/s12885-023-11383-3 [PubMed]
- 17. Burgess S, Thompson SG, and CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011; 40:755–64. https://doi.org/10.1093/ije/dyr036 [PubMed]
- 18. Locke AE, Kahali B, Berndt SI, Justice AE, Pers TH, Day FR, Powell C, Vedantam S, Buchkovich ML, Yang J, Croteau-Chonka DC, Esko T, Fall T, et al, and LifeLines Cohort Study, and ADIPOGen Consortium, and AGEN-BMI Working Group, and CARDIOGRAMplusC4D Consortium, and CKDGen Consortium, and GLGC, and ICBP, and MAGIC Investigators, and MuTHER Consortium, and MIGen Consortium, and PAGE Consortium, and ReproGen Consortium, and GENIE Consortium, and International Endogene Consortium. Genetic studies of body mass index yield new insights for obesity biology. Nature. 2015; 518:197–206. https://doi.org/10.1038/nature14177 [PubMed]
- 19. Kim MJ, Han JY, Shin JY, Kim SI, Lee JM, Hong S, Kim SH, Nam MS, Kim YS. Metformin-associated lactic acidosis: predisposing factors and outcome. Endocrinol Metab (Seoul). 2015; 30:78–83. https://doi.org/10.3803/EnM.2015.30.1.78 [PubMed]
- 20. Liang J, Cai Y, Zhang J, Jing Z, Lv L, Zhang G, Zhang R, Liu R, Nan K, Dang X. Metformin Treatment Reduces the Incidence of Rheumatoid Arthritis: A Two-Sample Mendelian Randomized Study. J Clin Med. 2023; 12:2461. https://doi.org/10.3390/jcm12072461 [PubMed]
- 21. Hattori Y, Suzuki K, Hattori S, Kasai K. Metformin inhibits cytokine-induced nuclear factor kappaB activation via AMP-activated protein kinase activation in vascular endothelial cells. Hypertension. 2006; 47:1183–8. https://doi.org/10.1161/01.HYP.0000221429.94591.72 [PubMed]
- 22. Saisho Y. Metformin and Inflammation: Its Potential Beyond Glucose-lowering Effect. Endocr Metab Immune Disord Drug Targets. 2015; 15:196–205. https://doi.org/10.2174/1871530315666150316124019 [PubMed]
- 23. Wu H, Esteve E, Tremaroli V, Khan MT, Caesar R, Mannerås-Holm L, Ståhlman M, Olsson LM, Serino M, Planas-Fèlix M, Xifra G, Mercader JM, Torrents D, et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat Med. 2017; 23:850–8. https://doi.org/10.1038/nm.4345 [PubMed]
- 24. de la Cuesta-Zuluaga J, Mueller NT, Corrales-Agudelo V, Velásquez-Mejía EP, Carmona JA, Abad JM, Escobar JS. Metformin Is Associated With Higher Relative Abundance of Mucin-Degrading Akkermansia muciniphila and Several Short-Chain Fatty Acid-Producing Microbiota in the Gut. Diabetes Care. 2017; 40:54–62. https://doi.org/10.2337/dc16-1324 [PubMed]
- 25. Bu Y, Peng M, Tang X, Xu X, Wu Y, Chen AF, Yang X. Protective effects of metformin in various cardiovascular diseases: Clinical evidence and AMPK-dependent mechanisms. J Cell Mol Med. 2022; 26:4886–903. https://doi.org/10.1111/jcmm.17519 [PubMed]
- 26. Wang D, Day EA, Townsend LK, Djordjevic D, Jørgensen SB, Steinberg GR. GDF15: emerging biology and therapeutic applications for obesity and cardiometabolic disease. Nat Rev Endocrinol. 2021; 17:592–607. https://doi.org/10.1038/s41574-021-00529-7 [PubMed]
- 27. Al-Kuraishy HM, Al-Gareeb AI, Alexiou A, Papadakis M, Nadwa EH, Albogami SM, Alorabi M, Saad HM, Batiha GE. Metformin and growth differentiation factor 15 (GDF15) in type 2 diabetes mellitus: A hidden treasure. J Diabetes. 2022; 14:806–14. https://doi.org/10.1111/1753-0407.13334 [PubMed]
- 28. Kim MH, Jee JH, Park S, Lee MS, Kim KW, Lee MK. Metformin enhances glucagon-like peptide 1 via cooperation between insulin and Wnt signaling. J Endocrinol. 2014; 220:117–28. https://doi.org/10.1530/JOE-13-0381 [PubMed]
- 29. Schernthaner G, Brand K, Bailey CJ. Metformin and the heart: Update on mechanisms of cardiovascular protection with special reference to comorbid type 2 diabetes and heart failure. Metabolism. 2022; 130:155160. https://doi.org/10.1016/j.metabol.2022.155160 [PubMed]
- 30. De Jager J, Kooy A, Lehert P, Bets D, Wulffelé MG, Teerlink T, Scheffer PG, Schalkwijk CG, Donker AJ, Stehouwer CD. Effects of short-term treatment with metformin on markers of endothelial function and inflammatory activity in type 2 diabetes mellitus: a randomized, placebo-controlled trial. J Intern Med. 2005; 257:100–9. https://doi.org/10.1111/j.1365-2796.2004.01420.x [PubMed]
- 31. Petrie JR, Chaturvedi N, Ford I, Brouwers MCGJ, Greenlaw N, Tillin T, Hramiak I, Hughes AD, Jenkins AJ, Klein BEK, Klein R, Ooi TC, Rossing P, et al, and REMOVAL Study Group. Cardiovascular and metabolic effects of metformin in patients with type 1 diabetes (REMOVAL): a double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017; 5:597–609. https://doi.org/10.1016/S2213-8587(17)30194-8 [PubMed]
- 32. Anderson JJA, Couper JJ, Giles LC, Leggett CE, Gent R, Coppin B, Peña AS. Effect of Metformin on Vascular Function in Children With Type 1 Diabetes: A 12-Month Randomized Controlled Trial. J Clin Endocrinol Metab. 2017; 102:4448–56. https://doi.org/10.1210/jc.2017-00781 [PubMed]
- 33. Meaney E, Vela A, Samaniego V, Meaney A, Asbún J, Zempoalteca JC, Elisa ZN, Emma MN, Guzman M, Hicks J, Ceballos G. Metformin, arterial function, intima-media thickness and nitroxidation in metabolic syndrome: the mefisto study. Clin Exp Pharmacol Physiol. 2008; 35:895–903. https://doi.org/10.1111/j.1440-1681.2008.04920.x [PubMed]
- 34. Bassols J, Martínez-Calcerrada JM, Osiniri I, Díaz-Roldán F, Xargay-Torrent S, Mas-Parés B, Dorado-Ceballos E, Prats-Puig A, Carreras-Badosa G, de Zegher F, Ibáñez L, López-Bermejo A. Effects of metformin administration on endocrine-metabolic parameters, visceral adiposity and cardiovascular risk factors in children with obesity and risk markers for metabolic syndrome: A pilot study. PLoS One. 2019; 14:e0226303. https://doi.org/10.1371/journal.pone.0226303 [PubMed]
- 35. Halabi A, Sen J, Huynh Q, Marwick TH. Metformin treatment in heart failure with preserved ejection fraction: a systematic review and meta-regression analysis. Cardiovasc Diabetol. 2020; 19:124. https://doi.org/10.1186/s12933-020-01100-w [PubMed]
- 36. Charytan DM, Solomon SD, Ivanovich P, Remuzzi G, Cooper ME, McGill JB, Parving HH, Parfrey P, Singh AK, Burdmann EA, Levey AS, Eckardt KU, McMurray JJV, et al. Metformin use and cardiovascular events in patients with type 2 diabetes and chronic kidney disease. Diabetes Obes Metab. 2019; 21:1199–208. https://doi.org/10.1111/dom.13642 [PubMed]
- 37. Hong J, Zhang Y, Lai S, Lv A, Su Q, Dong Y, Zhou Z, Tang W, Zhao J, Cui L, Zou D, Wang D, Li H, et al, and SPREAD-DIMCAD Investigators. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care. 2013; 36:1304–11. https://doi.org/10.2337/dc12-0719 [PubMed]
- 38. Driver C, Bamitale KDS, Kazi A, Olla M, Nyane NA, Owira PMO. Cardioprotective Effects of Metformin. J Cardiovasc Pharmacol. 2018; 72:121–7. https://doi.org/10.1097/FJC.0000000000000599 [PubMed]
- 39. Ye Y, Perez-Polo JR, Aguilar D, Birnbaum Y. The potential effects of anti-diabetic medications on myocardial ischemia-reperfusion injury. Basic Res Cardiol. 2011; 106:925–52. https://doi.org/10.1007/s00395-011-0216-6 [PubMed]
- 40. Anfossi G, Russo I, Bonomo K, Trovati M. The cardiovascular effects of metformin: further reasons to consider an old drug as a cornerstone in the therapy of type 2 diabetes mellitus. Curr Vasc Pharmacol. 2010; 8:327–37. https://doi.org/10.2174/157016110791112359 [PubMed]
- 41. Karam HM, Radwan RR. Metformin modulates cardiac endothelial dysfunction, oxidative stress and inflammation in irradiated rats: A new perspective of an antidiabetic drug. Clin Exp Pharmacol Physiol. 2019; 46:1124–32. https://doi.org/10.1111/1440-1681.13148 [PubMed]
- 42. Liu J, Aylor KW, Chai W, Barrett EJ, Liu Z. Metformin prevents endothelial oxidative stress and microvascular insulin resistance during obesity development in male rats. Am J Physiol Endocrinol Metab. 2022; 322:E293–306. https://doi.org/10.1152/ajpendo.00240.2021 [PubMed]
- 43. Kang L, Yi J, Lau CW, He L, Chen Q, Xu S, Li J, Xia Y, Zhang Y, Huang Y, Wang L. AMPK-Dependent YAP Inhibition Mediates the Protective Effect of Metformin against Obesity-Associated Endothelial Dysfunction and Inflammation. Antioxidants (Basel). 2023; 12:1681. https://doi.org/10.3390/antiox12091681 [PubMed]