



Introduction
Sarcopenia, derived from the Greek words “sarx” (flesh) and “penia” (poverty), refers to the age-related loss of skeletal muscle mass, strength, and function. With the rapid aging of the global population, e.g., the number of individuals over 60 will grow from 600 million in 2000 to 1.2 billion by 2025 and is projected to double by 2050 [1, 2], sarcopenia has emerged as one of the most pressing challenges facing modern healthcare systems [3]. This progressive syndrome affects over 60% of individuals above age 80 and represents far more than simple muscle loss; it is a complex multisystem disorder that compromises physical independence, increases fall risk and mortality, and imposes substantial economic burdens on healthcare systems worldwide [4]. Despite decades of intensive research and the formal recognition of sarcopenia as a disease by the World Health Organization in 2016, therapeutic advances have remained disappointingly limited [5]. Current approaches to impede its development rely primarily on exercise interventions and nutritional strategies, while no approved pharmacological treatments exist [6]. Perhaps more troubling, the therapeutic responses to these interventions demonstrate marked and unpredictable variability among patients, which has long been attributed to differences among individuals in genetics, compliance, or baseline fitness, but which may instead reflect a fundamental flaw in our therapeutic paradigm [7].
Universal treatment approaches for diseases in general have historically served medicine well, particularly for acute conditions, but their limitations become apparent in the case of complex age-related disorders like sarcopenia [8]. This universal treatment paradigm assumes that pathophysiological mechanisms and therapeutic responses are fundamentally similar in all patients, and required only minor modifications for factors like age, comorbidity burden, or disease severity [9]. However, mounting evidence suggests that this assumption does not apply anymore to muscle aging, during which pathophysiological pathways and metabolic hormones regulation appear to exhibit gender-specific differences [8].
The concept of sexual dimorphism in human biology extends far beyond obvious reproductive differences to encompass fundamental differences in metabolism, hormone regulation, inflammatory responses, and cellular aging processes. In skeletal muscle, these sex differences manifest throughout the lifespan but become particularly pronounced during aging, when hormonal changes result in differences between men and women in the trajectory of muscle decline [9]. Women experience precipitous muscle loss during the menopausal transition, coinciding with rapid estrogen decline, while men demonstrate paralleling gradual testosterone reduction. These distinct patterns reflect underlying differences in muscle-fiber composition, satellite-cell biology, metabolic regulation, and hormonal sensitivity that collectively suggest that sarcopenia may be a different disease in men and women rather than a single condition with variable presentations [10–12].
Through comprehensive examination of the literature describing the pathophysiological mechanisms underlying sarcopenia in human, mouse, zebrafish, and African turquoise killifish (ATK), including a detailed review of studies of three hormonal systems (apelin, insulin, and oxytocin), we demonstrate how sexual dimorphism in muscle biology creates distinct disease trajectories that demand tailored interventions. While numerous hormones influence muscle aging, including growth hormone (GH), IGF-1, thyroid hormones, and ghrelin, most of these systems primarily exhibit quantitative rather than qualitative sex differences [13–15]. For example, GH demonstrates sexually dimorphic secretion patterns (pulsatile in men versus continuous in women) but acts through fundamentally similar anabolic mechanisms in both sexes [15, 16]. Similarly, although ghrelin levels and thyroid-hormone sensitivity differ between sexes, these hormones regulate muscle metabolism through largely similar molecular pathways in both men and women [17]. In contrast, apelin, insulin, and oxytocin exhibit sex-specific interactions between sex hormones and metabolic regulation in muscle homeostasis. Each of these three peptides demonstrates qualitative differences in its mechanisms of action with estrogen versus testosterone, suggesting sex-specific differences in the modulation of sex-hormone levels, signaling pathways, and receptor sensitivity, and demonstrating sex-specific physiological outcomes [18–20]. In addition, these three systems do not act in isolation but participate together in a complex network influencing muscle metabolism and systemic energy balance. At the molecular level, these three peptide hormones converge on overlapping signaling cascades and share common downstream effectors that create synergistic and antagonistic interactions [21–26].
This review proposes that deregulation not only of sex hormones but also of peptide hormones contributes to the establishment of sarcopenia. Recognizing that sarcopenia manifests differently in men and women through distinct hormonal networks and cellular mechanisms will open unprecedented opportunities for targeted interventions that optimize outcomes for both sexes. Central to this endeavor will be a deeper understanding of sex-specific peptide-hormone deregulation, which emerges as a key mechanistic lever at the transition phase prior to the establishment of sarcopenia; this phase represents a potential therapeutic target for impeding or preventing sarcopenia progression in both men and women. The path forward will require coordinated research to characterize sex-specific mechanisms, develop appropriate biomarkers, and establish therapeutic protocols that harness these fundamental biological differences.
Global burden, diagnosis, and management of sarcopenia
Sarcopenia is one of the most significant age-related health challenges facing our rapidly aging global population. It is a complex syndrome that is associated with increased risk of falls and fractures and higher rates of hospitalization, disability, and mortality, and that directly impacts an individual’s daily life and independence [4, 27–29]. The progressive loss of skeletal muscle mass, strength, and function typically begins as early as age 30 and accelerates as we age [4, 30]. The substantial public health significance of sarcopenia is reflected in prevalence estimates of 10-16% in elderly individuals worldwide [2]. The formal recognition of sarcopenia as a disease by the World Health Organization and in the International Classification of Diseases (ICD-10: M62.84) in 2016 marked a pivotal moment in geriatric medicine [5, 31]. However, despite decades of research and therapy development, sarcopenia remains a pressing challenge, as to date we are able only to slow down its irreversible development, and not treat it [27, 28, 32]. As our global population continues to age and average lifespan increases, addressing sarcopenia has become critical, as longer lifespan does not necessarily translate to a longer healthy life.
A significant advancement in sarcopenia research has been the recognition of “possible sarcopenia,” defined as the reduction of skeletal-muscle strength with or without decreased muscle performance, occurring in the absence of confirmed low muscle mass [29, 33]. This pre-morbid status represents a transitional state between normal muscle health and established sarcopenia, offering an important window for early intervention. The identification of possible sarcopenia has proven to be valuable, as loss of skeletal muscle strength alone has been demonstrated to increase the risk of all-cause mortality, cardiovascular mortality, myocardial infarction, strokes, and injuries from falls [34]. In addition, the recognition of possible sarcopenia underlines the importance of understanding peptide-hormone deregulation (discussed in detail below); specifically, determining whether peptide-hormone deregulation takes place during the transitional “possible sarcopenia” state will help us to assess the potential of targeting peptide hormones as a means of impeding or preventing progression toward established sarcopenia.
Clinical diagnosis
The diagnostic process, all steps of which are performed by specialists, begins with muscle-strength assessment. The primary measure used for this first test is handgrip strength, because of the simplicity of the test and the strong correlation of hand strength with overall strength, although the test results may not fully reflect the strength of larger muscle groups and or overall mobility capability [35–37]. Next, specialists select one or more subsequent tests depending on the severity of muscle-strength assessment. Lower-body function is evaluated through chair-stand tests, while mobility is assessed via the Short Physical Performance Battery (SPPB) [35, 38]. Muscle mass is assessed via dual-energy X-ray absorptiometry (DXA) as the reference standard [39, 40], while CT and MRI offer superior muscle-quality assessment but are limited by cost and availability [41, 42]. More accessible alternatives for muscle-mass assessment include bioelectrical impedance analysis [43, 44], although its accuracy is affected by hydration status, and ultrasound [45, 46], which shows promise as a portable real-time option but currently lacks standardized protocols for reproducible use. Despite the value of the above diagnostic tests in assessing muscle strength, the recent recognition of “possible sarcopenia” demonstrates their limitations in diagnosing sarcopenia; hence, new diagnostic methods are needed, such as the use of biomarkers.
Biomarkers
The identification of reliable biomarkers for sarcopenia remains an active research area [47]. Key molecular markers include atrogin-1 (FBXO32) and MuRF1, which are regulated by the Akt1/FOXO1 pathway and upregulated prior to muscle-atrophy onset, linking sarcopenia to the ubiquitin proteasome system for muscle protein degradation [48–50]. Myostatin levels exhibit sex-specific differences in their association with skeletal muscle homeostasis, with myostatin acting as a homeostatic regulator in men while showing stronger association with sarcopenia development in women [51–55]. Conversely, IGF-1 is a sarcopenia biomarker in women, where serum IGF-1 levels associate with frailty and low muscle mass, but not in men [56]. Similarly, the cutoff values of serum creatinine-to-cystatin C ratio required for sarcopenia screening differ between men and women, as do the associations of this ratio with frailty outcomes [57–59]. These findings underscore that biomarker validation, while essential for characterization of early-stage sarcopenia, must account for sexual dimorphism in muscle biology. While various inflammatory markers show promise, they require further validation with sex-stratified analyses before clinical implementation [60, 61]. The challenge will be to develop biomarkers that are both clinically accessible and sufficiently accurate for sarcopenia diagnosis and monitoring across both sexes, which will require sex-informed reference ranges and diagnostic thresholds.
Sarcopenia management
Despite the absence of pharmacological treatments specifically for sarcopenia, a multimodal management approach combining exercise, nutritional, and emerging therapeutic strategies has shown efficacy in attenuating muscle loss and improving functional outcomes in both men and women [6, 62]. Resistance training remains the cornerstone of sarcopenia management, with robust evidence demonstrating efficacy in improving muscle mass, strength, and functional performance [6, 62, 63]. Progressive resistance-training protocols consistently show significant improvements through enhanced muscle-protein synthesis, satellite-cell activation, and improved mitochondrial function [6, 64]. However, optimal parameters vary based on baseline fitness, age, comorbidities, and sex-specific physiological differences.
Nutritional strategies have been developed that address age-related protein metabolism changes through high-quality protein supplementation including leucine, creatine, vitamin D, and micronutrients (vitamins C and E, omega-3 fatty acids); such strategies show promise, although individual responses vary considerably [6, 62, 65].
While no approved pharmacological treatments exist for sarcopenia, myostatin inhibitors and activin-receptor antagonists demonstrate muscle-mass increases, although functional improvements are inconsistent and cardiovascular concerns persist [66, 67]. Hormone-replacement strategies show muscle and strength benefits but present risks (cardiovascular/prostate effects in men, virilization in women), and their complex interactions with other hormonal systems remain poorly understood, limiting therapeutic optimization until there is a better understanding of these interactions, in particular, how the interactions differ between women and men [68–71].
Pathophysiological processes in sarcopenia
The development of sarcopenia involves multiple interconnected pathophysiological processes that collectively drive progressive muscle deterioration, including mitochondrial dysfunction, chronic inflammation, hormonal decline, neuromuscular junction degradation, and impaired protein synthesis, with type II fibers (fast-twitch anaerobic) preferentially lost [72–74]. Understanding these mechanisms is essential for developing therapeutic interventions and identifying prevention targets.
Hormonal changes
Sarcopenia has been associated with age-related decline in sex hormones and the consequent inability of the hormones to support the function of satellite cells, which are the resident muscle stem cells crucial for muscle repair and regeneration [75–77]. The broader hormonal decline includes decreased levels of anabolic hormones such as growth hormone, estrogen, testosterone, ghrelin, thyroid hormones, and insulin-like growth factor-1 (IGF-1) [78–84], combined with an age-related increase in the activity of catabolic hormones including cortisol and pro-inflammatory cytokines, creating an environment that favors muscle loss and compromises protein synthesis and cellular repair mechanisms [85–88]. However, recent studies demonstrate that testosterone supplementation can promote satellite-cell entry into the cell cycle, thereby increasing their number [89].
Muscle stem cells
Sarcopenia is intimately linked to dysfunction of satellite cells [89, 90]. Under normal physiological conditions, satellite cells remain in a reversible quiescent state, ready to activate upon muscle injury or demand for growth [91–93]. However, aging disrupts this delicate regulatory system through multiple interconnected mechanisms. The decline in satellite-cell numbers occurs in the early stages of muscle aging and is likely due to physiological changes affecting the satellite-cell niche and cell-autonomous alterations that together disturb the proper balance between cell quiescence, proliferation, and apoptosis [90, 94, 95]. As individuals age, the micro-environment within muscle tissue changes, disrupting normal quiescence [94, 95]. More importantly, geriatric satellite cells lose their normal quiescent state with age, mediated by the derepressing of p16(INK4), which results in conversion of the normally reversible activation-quiescent state to an irreversible senescent state, thereby limiting muscle-tissue repair and regeneration [95–97]. In geriatric mice, both the loss of muscle fibers and depletion of activated muscle stem cells correlate with satellite-cell entry into this senescent state [95], highlighting the interconnected nature of cellular aging and tissue deterioration.
Proteostasis
Central to sarcopenia disease is the disruption of proteostasis, the cellular process responsible for maintaining protein balance within muscle fibers [98, 99]. Age-related physiological changes create an imbalance between muscle-protein synthesis and breakdown that favors catabolism over anabolism. Specifically, declines in anabolic hormones (testosterone, growth hormone, IGF-1) have been shown to reduce muscle-protein synthesis, promote atrophy, and increase anabolic resistance [100, 101]. This shift is driven by impaired protein regulation and reduced responsiveness of the mTORC1 and MAPK signaling pathways to contraction-induced stimuli [102]. This results in net muscle-protein loss and accumulation of damaged proteins within muscle fibers, both of which compromise the structural integrity and functional capability of muscle [99, 103].
Mitochondrial biogenesis
Concurrently with muscle aging, progressive decline in mitochondrial biogenesis and oxidative function is another fundamental mechanism impairing cellular energy production and the muscle’s ability to meet physiological demands prior to sarcopenia onset [104–106]. The decline in mitochondrial integrity, network organization, and ATP production occurs before sarcomere breakdown [107], linking energetic failure to the progressive loss of muscle mass, strength, and function characteristic of the disease [104, 106, 108].
Neuromuscular system
The age-related progressive loss of motor neurons and deterioration of neuromuscular junction (NMJ) integrity contributes to both muscle atrophy and reduced functional performance [109, 110]. During aging, NMJs undergo profound structural and functional changes, including endplate fragmentation, widening of synaptic clefts, and altered acetylcholine-receptor distribution [111–113]. The loss of motor neurons during aging initiates the denervation-reinnervation cycle, whereby surviving motor neurons attempt to compensate through axonal sprouting [109, 110], a mechanism that progressively fails as increasing numbers of denervated fibers are unable to be successfully reinnervated or replaced [82, 109, 110].
Inflammation
Chronic systemic low-grade inflammation, also termed “inflammaging,” further disrupts normal muscle maintenance by elevating pro-inflammatory cytokines and promoting protein breakdown while inhibiting protein synthesis [88, 114]. Sources of inflammaging include accumulation of senescent cells that secrete inflammatory factors (the senescence-associated secretory phenotype, or SASP), increased visceral adiposity, and mitochondrial dysfunction [115, 116]. Inflammaging is characterized by increased levels of interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP), each of which can activate proteolytic pathways such as the ubiquitin-proteasome system [88, 114]. Beyond the direct effects of inflammaging on protein turnover, inflammaging profoundly impairs muscle metabolic health by contributing to insulin resistance through interference with insulin-receptor signaling cascades and disruption of glucose-transporter translocation, thereby compromising the muscle’s anabolic capacity and creating a state of “anabolic resistance” whereby muscle becomes less responsive to growth-promoting stimuli such as nutrition and exercise [117–119].
The inflammatory milieu also disrupts satellite-cell function, by impairing their activation, proliferation, and differentiation capacity, thereby compromising the muscle’s regenerative potential [120, 121]. Importantly, men and women exhibit distinct inflammatory profiles and tissue-specific responses to inflammation, both of which contribute to sex-specific sarcopenia trajectories [10, 12].
The regulatory network for apelin, insulin, and oxytocin as a sex-specific strategy for sarcopenia management
Apelin, insulin, and oxytocin are peptide hormones that are key regulators of muscle homeostasis, enhancing muscle health through complementary processes. Age-related decline in their signaling may contribute significantly to sarcopenia, yet the complex interplay of these hormonal changes during aging remains poorly characterized, particularly regarding sex-specific differences. Developing effective therapies requires comprehensive characterization of age-related hormonal networks and their sex-specific variations.
Apelin
Apelin, originally identified as the endogenous ligand for the APJ receptor (now termed APLNR), is produced through proteolytic processing of a 77-amino acid precursor protein and exists in multiple bioactive forms, including apelin-36, -17, and -13, each exhibiting distinct biological activities and tissue-specific expression patterns [122, 123]. The apelin/APLNR system is distributed widely throughout the body, with particularly high expression levels in skeletal muscle, the cardiovascular system, adipose tissue, and the central nervous and reproductive systems, positioning it as a critical regulator of energy homeostasis and metabolic function [124–127].
In skeletal muscle, apelin functions as a potent myokine that orchestrates multiple aspects of muscle physiology, including glucose uptake, fatty-acid oxidation, mitochondrial biogenesis, satellite-cell proliferation and activation, and contractile protein synthesis [124, 128, 129]. The peptide exerts its effects through binding to APLNR, a G-protein-coupled receptor that activates downstream signaling cascades involving AMP-activated protein kinase (AMPK), mammalian target of rapamycin (mTOR), and peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α) [130]. These pathways collectively enhance muscle oxidative capacity, improve insulin sensitivity, and promote anabolic processes essential for muscle maintenance and repair [130]. Apelin levels decline significantly with age but correlate positively with the beneficial effects of exercise in older people, suggesting a mechanistic link between apelin deficiency and sarcopenia [124].
Insulin
Insulin, which is secreted by pancreatic β-cells, is the master regulator of glucose homeostasis and anabolic metabolism [131]. Insulin orchestrates these metabolic functions by binding to insulin receptors on target tissues, triggering the PI3K/Akt/mTOR signaling pathway, which simultaneously promotes nutrient uptake and storage, enhances protein synthesis, inhibits protein breakdown, and stimulates cellular growth and proliferation. In skeletal muscle, which accounts for approximately 70-80% of glucose disposal under physiological conditions, this set of insulin-initiated processes creates a net anabolic environment supporting muscle-mass maintenance and growth through inhibition of the ubiquitin-proteasome system and autophagy [132]. Insulin also directly promotes the proliferation and differentiation of muscle satellite stem cells, increasing the expression of proliferation markers (Ki67, PCNA, Pax7) and differentiation markers (MYOD, MYOG, MYH) via PI3K-Akt and MAPK signaling [133, 134], and enhancing myotube formation and creatine-kinase activity [133, 134].
Oxytocin
Oxytocin, a neuropeptide hormone synthesized in the hypothalamus and evolutionary conserved across vertebrates, was recently shown to function as an important regulator of muscle homeostasis and regeneration, beyond its classical roles in parturition, lactation, and social bonding [135, 136]. Oxytocin exerts its effects through binding to oxytocin receptors (OXTR) and to G-protein-coupled receptors, both of which activate complex intracellular signaling cascades involving calcium mobilization, protein kinase C activation, MAPK/ERK, AKT, and AMPK signaling, and downstream transcriptional factors such as MyoD, all of which are essential for muscle function, maintenance, and repair [77, 137, 138].
OXTR expression is present in both mature myofibers and satellite cells; in both sites, oxytocin signaling influences proliferation, differentiation, and fusion dynamics critical for developmental myogenesis and regenerative response to injury [77]. Oxytocin also influences metabolic processes, including glucose uptake, insulin sensitivity, and mitochondrial function [77, 139]. OXTR expression levels are modulated by mechanical loading, nutritional status, the hormonal milieu, and aging [77].
The apelin-insulin-oxytocin complex regulatory network
A key feature of this hormonal triad is their convergence on shared downstream effectors, particularly AMPK and GLUT4 translocation, through distinct upstream mechanisms, enabling complementary and potentially synergistic regulation of muscle metabolism (Figure 1).
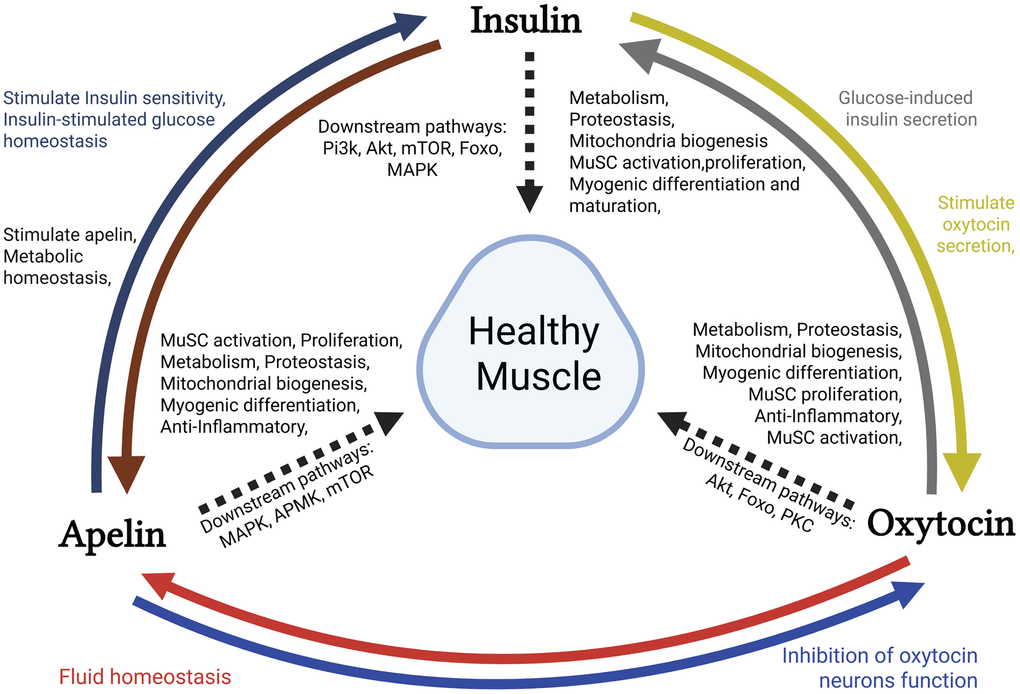
Figure 1. The apelin-insulin-oxytocin axis: a multi-hormonal network for muscle health. Schematic representation of the coordinated effects of insulin, oxytocin, and apelin on muscle health and systemic homeostasis. The colored arrows illustrate how these hormones are influenced by one another. Dashed black arrows denote downstream signaling pathways and indicate pathway-mediated effects on healthy muscle tissue. Key downstream pathways include MAPK/AMPK/mTOR (apelin), PI3K/AKT/mTOR/Foxo/MAPK (insulin), and Akt/Foxo/PKC (oxytocin). All three hormones promote muscle satellite cell (MuSC) activation, proliferation, metabolism, proteostasis, mitochondrial biogenesis, and myogenic differentiation, ultimately contributing to overall metabolic homeostasis. The diagram illustrates the synergistic and overlapping mechanisms by which these hormones maintain healthy muscle tissue and anabolic-catabolic balance.
Apelin-insulin hormonal network
Apelin regulates glucose and lipid metabolism, insulin sensitivity, and energy homeostasis through pathways such as AMPK, PI3K/AKT/mTOR, and eNOS, and also through interacting with insulin signaling [23–26]. Apelin has a complex role in glucose homeostasis, as apelin inhibits glucose-stimulated insulin secretion from pancreatic islets at lower concentrations (1-104 nmol/L) but stimulates it at higher concentrations (10μM) [23, 140]. In addition, in insulin-resistant states, apelin enhances insulin-stimulated glucose uptake by activating AMPK and promoting GLUT4 translocation through pathways distinct from but complementary to insulin’s PI3K/AKT route. Insulin drives GLUT4 to the cell surface via PI3K/AKT-mediated phosphorylation of TBC1D4, apelin acts through AMPK to phosphorylate a closely related but distinct protein, TBC1D1, achieving the same result through an independent upstream cascade. In insulin resistance, PI3K/AKT pathway is impaired, yet the AMPK/TBC1D1 route remains functional. Apelin can therefore drive GLUT4 translocation and glucose uptake even when insulin’s own signaling is compromised, providing a parallel route to the same destination making this mechanism particularly relevant for combating insulin resistance in sarcopenia [141, 142].
Conversely, insulin directly regulates apelin expression in both human and mouse adipocytes through the activation of PI3K, protein kinase C, and MAPK signaling pathways [143]. In obese patients, elevated plasma apelin levels correlate with increased insulin concentrations, establishing apelin as a novel adipokine linked to obesity-associated insulin sensitivity. The dysregulation of insulin-apelin signaling may therefore affect muscle-adipose tissue crosstalk and metabolic homeostasis in insulin-resistant conditions [143].
Insulin-oxytocin hormonal network
Oxytocin is produced in the hypothalamus then released into the circulation and also by a subpopulation of sympathetic neurons that directly innervate adipose tissue [144]. Oxytocin enhances glucose uptake and lipid utilization in muscle and adipose tissue [144, 145] positioning oxytocin as a key integrator linking central neuroendocrine control with peripheral energy homeostasis. Oxytocin stimulates glucose-induced insulin secretion through calcium-CaMKK-AMPK pathways [137, 146]. Central insulin in turns activates hypothalamic oxytocin neurons to release oxytocin into circulation, creating a feedback loop that establishes oxytocin as both regulator and downstream effector of insulin signaling [147]. This axis is particularly relevant postprandially, when rising insulin levels activate hypothalamic oxytocin neurons that promote glucose disposal and lipid oxidation. In skeletal muscle, oxytocin-receptor activation enhances insulin sensitivity through increased GLUT4 translocation, improved mitochondrial oxidative capacity, and lipid oxidation, all via AMPK-dependent and calcium-dependent signaling cascades [137, 148]. In adipose tissue, oxytocin promotes browning of white adipocytes and thermogenic activity, contributing to energy expenditure [149, 150].
Oxytocin-apelin hormonal network
The apelin-oxytocin relationship exhibits anatomical and functional connections within the hypothalamus, where the two peptides co-localize in magnocellular neurons of the supraoptic and paraventricular nuclei [151, 152]. Apelin regulates hypothalamic oxytocin neurons through receptor binding, with intracerebroventricular apelin administration in rats suppressing both magnocellular and parvocellular oxytocin neuron function [153–155]. However, apelin expression is not exclusive to oxytocinergic neurons [151]; some apelin-positive cells are vasopressinergic [153–155]. Because oxytocin neurons express apelin receptors, oxytocin may influence apelin expression through autocrine or paracrine signaling, although direct experimental evidence is lacking. Apelin’s regulatory influence appears context-specific, with distinct inhibitory effects during lactation [153] and variable effects in other physiological states [154]. During water deprivation, apelin and vasopressin are reciprocally regulated in a coordinated negative feedback loop to conserve fluid. Vasopressin rises and promotes renal water retention, directly counteracting the dehydration stimulus. Simultaneously, apelin falls in the plasma and accumulates within the hypothalamic neurons rather than being released [151, 155, 156]. The withdrawal of apelin removes its inhibitory brake on vasopressin neurons, allowing them to fire in optimized phasic bursts and sustain maximal vasopressin release [155]. The two peptides thus act in concert: rising vasopressin retains water at the kidney, while falling apelin amplifies that response, and together constitutes the negative feedback that resists further fluid loss [155, 156].
The sexual dimorphism of apelin, insulin, and oxytocin
The apelin/sex hormone axis
Apelin and its receptor (APLNR) are expressed throughout the hypothalamic-pituitary-gonadal axis, where apelin directly modulates sex-hormone secretion (estrogen, progesterone, testosterone) (Figure 2) while inhibiting gonadotropin (LH, FSH) release at the pituitary and hypothalamic levels [157, 158].
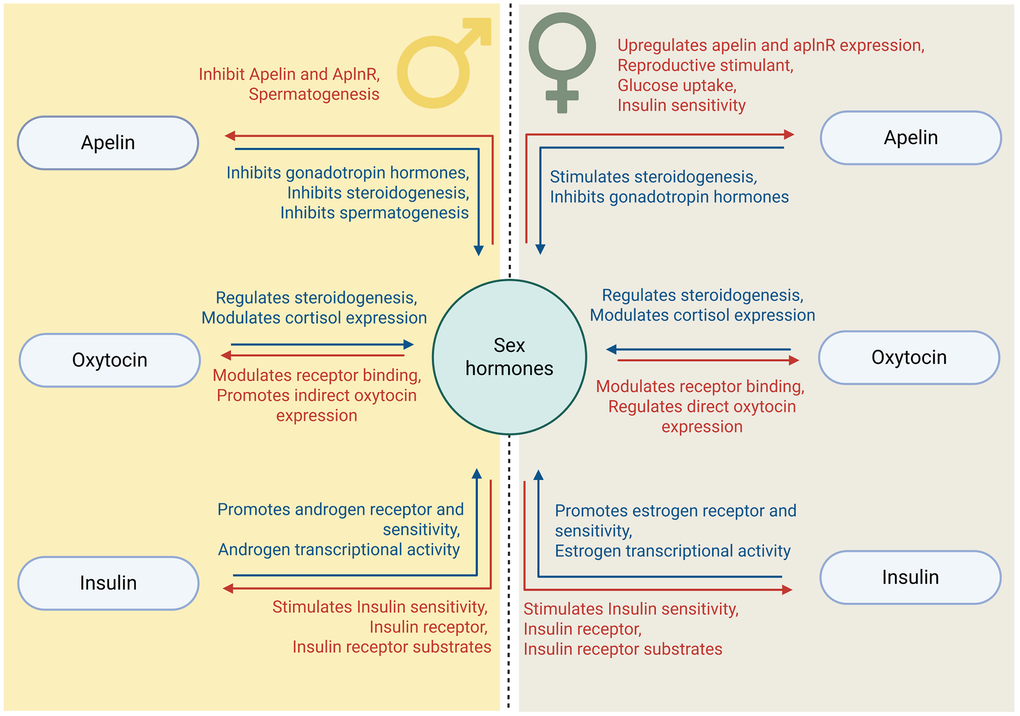
Figure 2. Crosstalk between apelin, oxytocin, or insulin and sex-hormone pathways: a sex-dimorphic perspective. Schematic illustration of the sex-specific bidirectional interactions between metabolic hormones (apelin, insulin, and oxytocin) and sex hormones. The central horizontal dashed line separates the male (left) and female (right) regulatory patterns. Blue text indicates effects on sex-hormone production and signaling, while red text shows the reciprocal effects of sex hormones on metabolic-hormone expression and function. Bidirectional arrows represent mutual regulatory relationships, demonstrating that metabolic hormones influence sex-hormone synthesis and receptor activity, and sex hormones modulate the expression and sensitivity of metabolic-hormone systems.
In females, estrogen upregulates apelin and APLNR expression in reproductive tissues while progesterone downregulates them [157, 159, 160]. In ovarian cancer cells, APLNR and estrogen receptor-α (ERα) engage in direct crosstalk [161, 162]. The levels of circulating apelin are higher during women’s reproductive years, with menstrual cycle variations [163, 164]. In ovarian tissues, apelin stimulates estradiol and progesterone production through the MAPK/ERK, PI3K/Akt, and AMPK signaling pathways, enhancing follicular development, promoting cell proliferation, and amplifying IGF-1 and FSH effects on steroid synthesis [20, 165, 166]. Concurrent postmenopausal declines in estrogen and apelin contribute to muscle loss [167, 168], coinciding with decreased muscle-glucose uptake and mitochondrial dysfunction [169, 170].
In males, the apelin-APLNR system tends to suppress testosterone production rather than be stimulated by it [171]. Apelin and APLNR are expressed in testicular Leydig cells and seminiferous tubules [172]. In diabetic mice, elevated apelin and APLNR are associated with reduced testosterone production and impaired spermatogenesis [172]. In diabetic mice and human testicular tissue, central apelin-13 administration suppresses LH and testosterone levels while reducing Leydig cell numbers, whereas blocking the apelin receptor (with ML221 antagonist) restores testosterone production and improves spermatogenesis [172–174].
The insulin/sex hormone axis
Insulin and sex hormones engage in complex bidirectional regulation that shapes metabolic homeostasis (Figure 2). For example, estrogen enhances insulin sensitivity by upregulating insulin-receptor expression, GLUT4, and insulin receptor substrate (IRS) signaling while reducing inflammatory cytokines (TNF-α, IL-6) [175–177]. Estrogen receptor-α (ERα) activation promotes mitochondrial biogenesis and oxidative metabolism, collectively protecting insulin signaling [178, 179].
Testosterone similarly enhance insulin sensitivity through insulin-receptor expression, IRS/PI3K/Akt phosphorylation, GLUT4 upregulation, and improved mitochondrial function and muscle-fiber composition [180–182]. Testosterone also directly activates the Akt, ERK, and mTOR pathways [183, 184], although these effects differ by muscle-fiber type, metabolic state, and hormonal context [182, 185, 186].
In the reverse direction, insulin-activated pathways (PI3k, Akt, MAPK/ERK) promote ERα phosphorylation [187, 188] can activate ERα in a ligand-independent manner [188, 189]. Insulin also increases androgen receptor (AR) expression, sensitivity, and transcriptional activity. Chronic hyperinsulinemia amplifies AR signaling, while insulin deficiency impairs androgen action [190, 191].
Additionally, insulin modulates local sex-hormone bioavailability by regulating steroidogenic enzymes (CYP19A1, 5α-reductase) and suppressing synthesis of hepatic SHBG (sex hormone binding globulin) via hepatic nuclear factor 4α (HNF-4α) inhibition [192, 193], such that hyperinsulinemia increases the bioavailable concentrations of both androgens and estrogens.
Compared to men, women generally maintain superior skeletal-muscle insulin sensitivity throughout most of the lifespan, attributable to estrogen’s multifaceted protective effects [194–196]. Following menopause, however, rapid estrogen decline leads to accelerated muscle-insulin resistance development over 2-5 years [197, 198] with decreased muscle-glucose uptake, impaired insulin-stimulated protein synthesis, increased intramuscular lipid accumulation, and heightened inflammatory-mediated insulin resistance [197–199], creating a pathological cascade whereby insulin resistance and muscle loss reinforce one another [200–203].
The trajectory of testosterone in men is fundamentally different from the estrogen trajectory in women [204–206]. Testosterone decline occurs gradually, which contributes to a slower development of muscle-insulin resistance [184, 207, 208] and allows for compensatory mechanisms and metabolic adaptation that together may partially impede rapid muscle deterioration [208]. Men’s greater baseline muscle mass provides a glucose disposal capacity that is greater than that in women and that may mask early metabolic consequences, potentially delaying clinical sarcopenia recognition [209–212].
The oxytocin/sex hormone axis
Age-related decline in circulating oxytocin and muscle OXTR expression in women and men is implicated in sarcopenia pathogenesis, with sex hormones fundamentally shaping these declines [77, 213, 214].
Oxytocin and sex hormones form a bidirectional regulatory network influencing reproductive function and muscle homeostasis (Figure 2). Estrogen directly upregulates OXTR gene expression through estrogen-response elements in the OXTR promoter and enhances hypothalamic oxytocin synthesis [152, 215, 216]; consequently, women maintain higher levels of circulating oxytocin throughout the lifespan compared to men, with concentrations peaking during ovulation [217, 218].
Testosterone’s effects are mediated largely through aromatization to estradiol rather than through direct androgenic action [219, 220]. Estrogen treatment fully restores oxytocin responsiveness in male reproductive tissues, while testosterone alone is ineffective, demonstrating that androgens regulate oxytocin-receptor expression only after conversion to estrogen [221–223].
Progesterone inhibits OXTR binding and downstream signaling, providing cycle-dependent modulation that is particularly important in maintaining uterine quiescence during pregnancy [224, 225]. Oxytocin reciprocally influences sex hormones through direct modulation of gonadal steroidogenesis (stimulating testosterone and DHT in Leydig cells and progesterone in granulosa cells), and through indirect suppression of the cortisol-driven HPA axis [226, 227]. Oxytocin inhibits pituitary ACTH secretion and adrenal cortisol responsiveness [228, 229], thereby reducing the cortisol-mediated antagonism of sex-hormone action, gonadal steroidogenesis suppression, and muscle-protein degradation, all of which contributes to sarcopenia.
In muscle, oxytocin-estrogen interactions support anti-inflammatory cytokines [230], growth-factor activation [231], satellite-cell activation and proliferation [232], muscle repair, and protein synthesis through AKT/FoxO1 and PKC pathway activation [11, 233], with estrogen amplifying both oxytocin production and muscle responsiveness [223]. This creates a positive feedback with estrogen stimulating OXT and its receptor while oxytocin contributes to muscle maintenance and regeneration [77]. The menopausal transition sharply disrupts this positive feedback loop: estrogen decline reduces OXTR expression and sensitivity, impairs regenerative capacity, compromises satellite-cell function [11, 232, 234], and prolongs post-exercise inflammatory responses [235–238], deficits that are partially restored by oxytocin administration in preclinical models [239].
Compared to women, men show lower baseline oxytocin levels and more gradual changes in muscle function with age [238, 240, 241]. For example, in contrast to women, men maintain the capacity for explosive muscle contraction throughout much of aging, which may be the result of a testosterone-OXTR interactions [241–243], i.e., testosterone modulates OXTR expression preferentially in type II (fast-twitch) fibers, altering muscle-fiber-type composition and myonuclear organization [139, 242–244]. When testosterone levels fall below critical thresholds, as in clinical hypogonadism, the oxytocin system’s muscle-protective functions become significantly compromised, potentially accelerating sarcopenia [71, 245, 246].
This fundamental dimorphism has direct consequences for therapy. Treatment efficacy in sarcopenia differs significantly between sexes [183]. For example, ACE inhibitors and statins show stronger cardiovascular benefits in men, while calcium-channel blockers are more effective in women and statins carry greater muscle-related adverse effects in women at equivalent doses [247, 248]. In addition, resistance-training protocols optimized for male physiology may yield suboptimal results in postmenopausal women, who require different loading parameters and recovery periods due to altered collagen synthesis [64, 249]. Further, testosterone replacement dramatically improves muscle mass and strength in hypogonadal men [250], while similar androgen interventions in women may cause virilization without proportional muscle benefit [251]; conversely, selective estrogen-receptor modulators show promise for muscle quality in postmenopausal women but lack equivalent efficacy in aging men [170, 252]. This variability, often attributed to genetic differences or compliance, may more accurately reflect a failure to account for the sex-specific mechanisms underlying muscle aging and regeneration.
Apelin, insulin, and oxytocin in muscle pathophysiology
Apelin
Under physiological conditions, apelin supports the perivascular stem-cell niche, enhancing satellite-cell function and muscle regeneration, and promotes mitochondrial function, metabolism, and adaptive responses to exercise stress [124, 253]. It stimulates muscle stem cells (MuSCs) to enhance endogenous repair in muscular dystrophy and sarcopenia models, promotes proteostasis through autophagy induction, and is essential for metabolic adaptation during high-intensity exercise [124, 254, 255]. In parallel, apelin–APLNR signaling independently enhances muscle glucose utilization and systemic insulin sensitivity via endothelial pathways [26]. In skeletal muscle, apelin also promotes mitochondrial biogenesis by increasing mitochondrial-protein expression, which in turn enhances respiratory-chain activity, ATP production, and coupling efficiency [124, 256]. At the same time, by inhibiting NF-κB–linked inflammatory pathways and oxidative stress, apelin supports a more anti-inflammatory, metabolically efficient muscle phenotype [257].
Under pathological conditions, deficiency of either apelin or APLNR causes dramatic age-related muscle-function alteration (Figure 3), including a shift toward smaller slow-twitch type fibers and defective IGF-1 signaling [253]. Mice deficient in apelin or APLNR present dramatic muscle-function alterations with age, while apelin restoration triggers mitochondriogenesis, autophagy, anti-inflammatory pathways in myofibers, and regenerative capacity in MuSCs [124]. Apelin associated with serine protease HtrA1 is useful for sarcopenia diagnosis, particularly in men [258]. Chronic inflammatory conditions and cancer-associated cachexia show suppressed apelin expression, potentially accelerating muscle wasting [259].
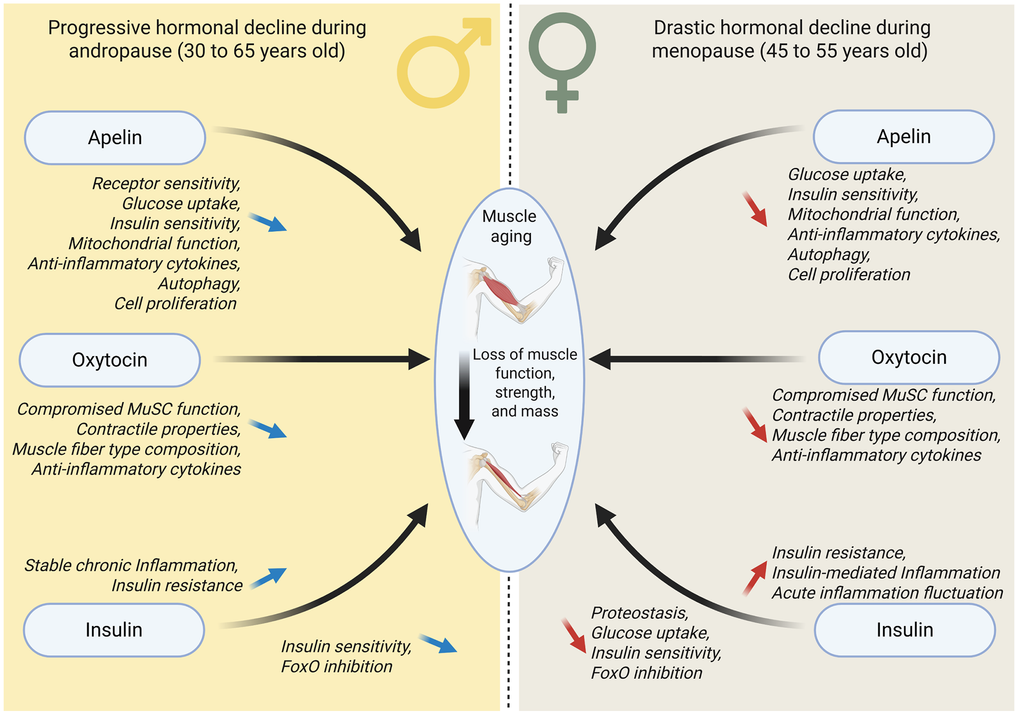
Figure 3. Sexual dimorphism in age-related hormonal changes and muscle aging. Sex-specific effects of age-related hormonal decline on muscle aging. The diagram contrasts the progressive hormonal decline during male andropause (30-65 years of age, left) with the rapid hormonal decline during female menopause (45-55 years of age, right). Black arrows indicate the declining hormone levels converging on muscle aging, and consequent loss of muscle function, strength, and mass. Blue arrows indicate progressive decline in hormone levels and their effects, while red arrows indicate rapid decline. Black italic text describes the compromised beneficial effects of each hormone in males (progressive loss), and the compromised effects in females (rapid loss). Both sexes experience reduced apelin, insulin, and signaling, leading to impaired muscle satellite cell (MuSC) function, altered muscle-fiber composition, decreased mitochondrial function, and increased inflammation, although the timeline and rate of decline differ between males and females.
Insulin
Age-related decline in muscle-insulin sensitivity is a critical factor in sarcopenia development, as impaired insulin signaling directly compromises glucose utilization and protein anabolism [260–262]. Insulin maintains muscle mass by suppressing protein degradation via FoxO inhibition, and enhancing protein synthesis when amino acids are available [262, 263]; notably, insulin-receptor signaling is more critical than IGF-1 signaling for muscle proteostasis, as combined receptor deletion in mice cause severe wasting [263]. Diabetic individuals show impaired insulin-stimulated muscle-protein synthesis even with sufficient amino acids [262]. Insulin infusion enhances mitochondrial biogenesis, mitochondrial protein synthesis, and ATP production in skeletal muscle, these benefits are recapitulated physiologically by normal post-meal insulin levels [264]; insulin deprivation leads to mitochondrial dysfunction, while insulin treatment restores mitochondrial content and function [264]. Insulin exhibits complex inflammatory effects, suppressing certain inflammatory pathways in healthy tissue through immune-signaling modulation. These anti-inflammatory effects of insulin are lost in diabetes or obesity, where chronic inflammation impairs insulin signaling, which further reduces insulin’s ability to suppress inflammation and worsen insulin resistance, establishing a harmful cycle [260–262].
Aging-associated insulin resistance compromises the metabolic environment necessary for muscle maintenance and impairs contraction. At pathophysiologically high concentrations, estradiol binds directly to insulin and insulin receptors, potentially contributing to insulin resistance in hyperestrogenemic conditions (Figure 3).
Oxytocin
Oxytocin activates Ca2+–CaMKK–AMPK signaling and glucose uptake in C2C12 mouse myoblast culture [137], and promotes myogenic differentiation and myoblast fusion while stimulating satellite-cell activation and proliferation in both mice and humans [11, 77]. Systemic oxytocin administration restores muscle regenerative capacity in aged mice [77].
Oxytocin simultaneously blocks catabolic programs through OXTR-mediated suppression of lysosomal, proteasomal, and autophagy pathways (reducing MuRF1, atrogin1, and LC3 expression) while activating anabolic processes that increase protein synthesis and muscle mass in vivo [136, 138]. The premature sarcopenia observed in oxytocin-knockout mice, combined with evidence that oxytocin restores muscle mass and protein synthesis in cachexia models and increases lean mass in humans, suggests that this loss reflects the combined failure of both proteolysis suppression and anabolic support, rather than either mechanism alone [77].
Oxytocin also promotes mitochondrial biogenesis and function, increasing NRF1 and TFAM expression, improving oxidative capacity, and reducing oxidative stress and ROS production [265, 266]. In addition, oxytocin robustly reduces inflammation by downregulating pro-inflammatory cytokines (IL-6, TNFα, IL-1β), inhibiting NF-κB signaling, and attenuating immune-cell activation in muscle and macrophages [267] (Figure 3).
Inflammatory and catabolic environments in cancer cachexia, inflammatory myopathies, and diabetes-related muscle loss likely impair oxytocin signaling, with women showing greater susceptibility to inflammation suppression of OXTR function and more severe associated muscle loss compared to men [268].
Modes and models of aging
Modes of aging
Mechanistically, aging represents a complex interplay between programmed processes and stochastic damage accumulation [269]. Programmed processes include genetically encoded limits such as telomere attrition (each cell division erodes chromosome caps until triggering growth arrest or apoptosis) and hormonal decline (growth hormone, sex steroids, and peptide hormones follow predetermined timelines) [269, 270]. Simultaneously, stochastic damage accumulates through reactive oxygen species, DNA lesions, protein misfolding, and lipid peroxidation, modulated by environmental factors such as sedentary lifestyles [271, 272].
Sarcopenia exemplifies this interplay. While genetic factors account for only 25% of overall lifespan, they account for 30-85% of muscle-strength variation among individuals and 50-80% of lean mass [273]. Eight-year follow-up of active older adults showed declines in muscle strength (10.2%), muscle mass (5.4%), and gait speed (28.6%), yet these individuals far outperformed sedentary controls [274], demonstrating that inactivity accelerates muscle-strength decline and that programmed aging continues despite optimal lifestyle.
The following primary hallmarks of aging initiate muscle damage: genomic instability, epigenetic alterations, and proteostatic collapse [275]. Antagonistic hallmarks, including satellite cell dysfunction, mitochondrial failure, and cellular senescence, represent processes that are initially protective but become harmful with age, accumulating SASP-secreting cells and impairing regenerative capacity [275]. These two categories of responses converge on integrative phenotypes: stem-cell exhaustion, chronic inflammation promoting protein breakdown, and NMJ damage causing denervation that collectively drive the functional decline characteristic of sarcopenia [87, 276].
Models of aging
A spectrum of model systems, from invertebrates to clinical cohorts, has been deployed to dissect the mechanisms of sarcopenia, each offering distinct trade-offs between experimental tractability and physiological relevance [277].
Invertebrate models, C. elegans (Caenorhabditis elegans) and Drosophila (Drosophila melanogaster), provide genetic tractability and short lifespans [277] and have been instrumental in identifying conserved aging pathways such as insulin/IGF-1, TOR, sirtuins, and FOXO [278, 279]. However, these organisms lack vertebrate-specific features such as adaptive immunity and complex endocrine regulation. On the other hand, both organisms are largely post-mitotic in muscle tissue, enabling study of contractile-apparatus maintenance in isolation from the confounding effects of regeneration present in vertebrate models [280–282].
Non-mammalian vertebrates combine the advantages of invertebrate and vertebrate models. Zebrafish (Danio rerio) recapitulate histological and molecular hallmarks of human muscle aging including satellite cells and anatomically distinct fiber types; zebrafish and humans have a high level of genetic orthology; and a broad range of tractable transgenic tools are available for zebrafish, allowing rapid mechanistic dissection [87, 277, 283]. The African turquoise killifish (Nothobranchius furzeri, ATK), the shortest-lived captive vertebrate (4–6 months) [284, 285], compresses the full aging trajectory into an experimentally accessible window. Notably, research using ATK has revealed sexual dimorphism in the response to dietary restriction [286–289], with females deriving greater lifespan and muscle-aging benefit than males.
Rodent models remain the preclinical standard because of their close physiological and metabolic similarity to humans [10, 290]. Mice and rats have proven to be valuable for sarcopenia research. Natural aging studies in these organisms (18–24 months in mice; 24–30 months in rats) consistently show sex-dimorphic sarcopenia progression, often earlier and more severe in males, with this difference attributable to hormonal, metabolic, and inflammatory differences between females and males [10, 291]. The availability of genetically modified mouse strains, including an accelerated aging mouse model (SAMP8) [292] and muscle-specific knockout mice (Klotho) [293], enables mechanistic dissection of pathways implicated in muscle wasting. Of all the widely used animal models, the mouse is the closest to human physiologically, and with its extensively characterized muscle biology, it is an essential model for validating therapeutic candidates in a mammalian context before transitioning to clinical trials [294].
Human-derived models, which include primary myoblast cultures from aged donors [94, 295], 3D myobundles engineered from induced pluripotent stem cells (iPSCs) [296, 297], and patient-derived iPSC lines [298], bridge preclinical findings and clinical application [299]. Cultures of satellite cells and myoblasts from young and old donors have demonstrated that intrinsic cellular aging (reduced proliferative capacity, increased senescence) and extrinsic niche factors both contribute to muscle decline [299–301], and that female- and male-derived myoblasts differ in responses to oxidative stress and hormonal signals [302]. A limitation of human-derived in vitro models is that standard culture conditions do not faithfully reflect the aged muscle environment, as they strip away systemic factors: such as circulating inflammatory mediators, hormonal decline, and neuromuscular interactions, that drive aging in vivo [303, 304]. This becomes apparent when myogenic precursor cells from young and old donors are cultured under optimal conditions, as they display similar proliferative and differentiation profiles, suggesting that the age-related dysfunction observed in vivo is largely context-dependent rather than intrinsic to the cells themselves [295, 305]. However, in vitro models can better approximate aged muscle when deliberately modified, for example through prolonged culture or exposure to senescence-inducing factors, which introduces age-associated cellular changes and makes these systems more suitable for mechanistic studies and therapeutic screening [306].
Clinical trials remain the ultimate validation platform, yet fewer than 30% of sarcopenia clinical intervention report sex-disaggregated outcomes, a critical gap given the fundamentally dimorphic nature of the condition. Hormone-targeted therapies (e.g., apelin-receptor agonists) have faced translational setbacks due to on-target off-tissue effects [307–310], and because hormonal profiles differ fundamentally between men and women, tissue-selective or biased agonist approaches may be essential to achieving sex-appropriate therapeutic outcomes. Next-generation biased agonists such as WN561 show promise by selectively activating the G-protein pathway of APLNR while eliminating β-arrestin signaling thereby preserving cardioprotective benefits with a reduced off-target side effect profile, pending further clinical validation [311].
Optimal intervention timing and modality differ by sex: in women, initiating resistance and aerobic training with optimized protein intake during the perimenopausal transition appears most effective, while men benefit from sustained protocols that address gradual insulin resistance in the context of declining androgens. Current research increasingly focuses on individualized, multimodal combination therapies tailored to sex-specific hormonal regulation. The demonstrated ability of individuals to recover from sarcopenic states with appropriate interventions offers hope for maintaining functional independence and quality of life in aging populations.
The availability of multiple models for the study of muscle aging establishes a powerful translational pipeline: discover fundamental mechanisms in invertebrates → validate in a vertebrate with a short lifespan (African turquoise killifish) and a versatile regenerative model (zebrafish) → translate to mammalian physiology (rodents) → ensure translational fidelity in human-derived systems → validate in clinical trials (Figure 4). Each model is valuable for investigating sexual dimorphism in neuromuscular aging and identifying sex-specific hormonal alterations that drive accelerated muscle degeneration, together advancing progress towards targeted interventions for sarcopenia that will be effective in both sexes. Together, these models form a complementary testing platform where cross-species-validated findings are far more likely to translate successfully to human interventions than use of a single model organism.
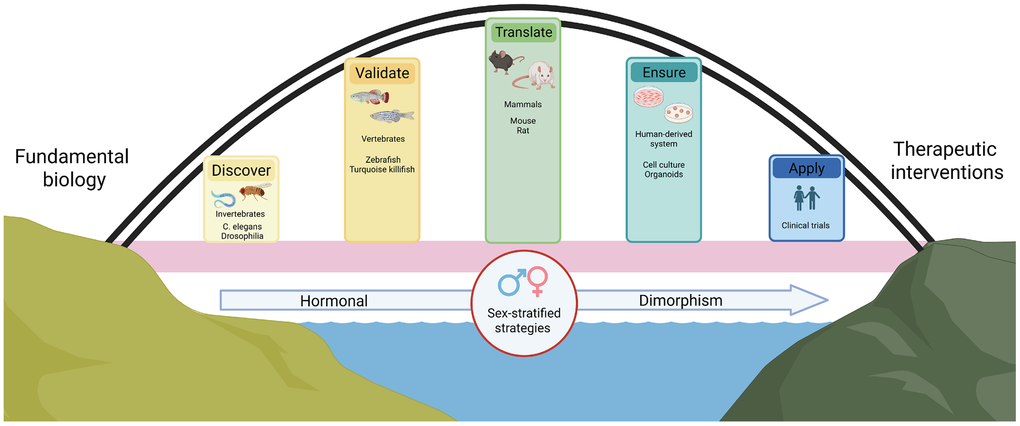
Figure 4. Bridging models from fundamental biology to sex-stratified therapeutic interventions. Schematic representation of the translational-research pipeline for developing sex-stratified therapeutic interventions. The arch illustrates the bridging progression from fundamental biology (left) to therapeutic interventions (right), encompassing five key stages: Discover (invertebrate models: C. elegans, Drosophila), Validate (vertebrate models: zebrafish, African turquoise killifish), Translate to preclinical (mammalian models: mouse, rat), Ensure (human-derived systems: cell culture, organoids), and Apply (clinical trials in humans). The foundational layers emphasize the importance of considering hormonal sexual dimorphism throughout all stages of research, converging in sex-stratified therapeutic strategies that account for biological differences between males and females.
Conclusion
The apelin, insulin, and oxytocin systems exemplify how hormonal regulation of muscle metabolism, energy homeostasis, and glucose disposal operates through interconnected, sex-specific mechanisms that undergo dramatic transformation with aging. In women, estrogen acts as a central orchestrator, simultaneously enhancing apelin signaling, maintaining insulin sensitivity, and amplifying oxytocin responsiveness to preserve muscle mass throughout reproductive years. Estrogen increases expression of apelin and its receptor, enhances receptor sensitivity, and supports integrated metabolic control. The abrupt withdrawal of estrogen at menopause triggers coordinated deterioration across all three systems, producing rapid, synchronized collapse in muscle homeostasis with declining apelin levels, accelerated insulin resistance, and compromised oxytocin signaling. This cascading dysfunction contributes to the characteristic pattern of rapid muscle loss in postmenopausal women. Men experience a fundamentally different trajectory, where gradual testosterone decline produces slower, more variable changes in these regulatory networks. Testosterone supports apelin signaling while modulating receptor sensitivity, maintains muscle insulin sensitivity through effects on fiber composition and mitochondrial function, and influences oxytocin-receptor expression in a fiber-type-specific manner. The slow testosterone decline creates a trajectory of hormonal-network dysfunction different from that in women, paralleling the more gradual sarcopenia progression in aging men. With women showing greater susceptibility to inflammation-mediated disruption but also greater responsiveness to anti-inflammatory interventions, these sex-specific responses to inflammatory stress highlight the necessity of tailoring therapeutic approaches based on biological sex and hormonal status.
Each peptide hormone in the apelin-insulin-oxytocin triad demonstrates bidirectional regulatory relationships with the others, creating a sophisticated feedback system where disruption at any node throughout the cascades network can compromise muscle homeostasis and metabolic function. Apelin and oxytocin converge on shared signaling mechanisms (AMPK activation, GLUT4 translocation, and mitochondrial biogenesis), suggesting coordinated rather than redundant actions in maintaining insulin sensitivity and muscle metabolic health. Hypothalamic co-localization of apelin and oxytocin neurons enables rapid coordination of peripheral metabolic responses to feeding, fasting, and energy demands. Insulin serves as both regulator and regulated target, modulating apelin expression in adipose tissue while activating central oxytocin release, which subsequently feeds back to enhance peripheral insulin sensitivity. In aging muscle, deterioration of this hormonal network (through reduced peptide production, diminished receptor sensitivity, or impaired central-peripheral communication) contributes to the characteristic metabolic dysfunction and insulin resistance that accelerate sarcopenia progression. The synergistic actions of apelin and oxytocin on mitochondrial function suggest therapeutic potential in targeting multiple nodes simultaneously.
The convergence of apelin, insulin, and oxytocin on AMPK represents an important metabolic integration where multiple hormonal signals are transduced into coordinated cellular responses governing energy homeostasis, protein turnover, and mitochondrial function. Each hormone contributes to distinct yet complementary mechanisms: apelin uniquely supports the perivascular stem-cell niche and exercise adaptation, insulin serves as the primary regulator of protein synthesis and degradation balance, while oxytocin provides dual action that simultaneously suppresses catabolic programs and activates anabolic pathways. The profound sexual dimorphism in these systems (estrogen amplifying all three pathways in women and testosterone modulating them more gradually in men) explains why sarcopenia manifests as abrupt postmenopausal acceleration in women versus slower, progressive decline in aging men. Pathological disruption of the hormonal network, impairing satellite-cell function, compromising mitochondrial biogenesis, and exacerbating inflammation, accelerates muscle wasting. The shared effects on mitochondrial biogenesis, oxidative capacity, and anti-inflammatory signaling suggest potential synergistic therapeutic strategies targeting multiple nodes simultaneously rather than single-hormone replacement.
Understanding sarcopenia’s complex, sexually dimorphic nature requires strategic integration of complementary experimental systems. Invertebrate models provide unparalleled genetic tractability for discovering conserved molecular pathways, but their lack of satellite cells limits their regenerative capacities. Zebrafish and African turquoise killifish bridge the evolutionary gap, offering vertebrate-specific features such as satellite cells and complex neuroendocrine systems within experimentally tractable timeframes while permitting the study of extensive regenerative processes. Rodent models remain indispensable for validating biological mechanisms in mammalian physiology and testing therapeutic interventions in systems that closely recapitulate human hormonal networks. All three model organisms reveal sexual dimorphism mirroring the difference in human sarcopenia development. Human-derived models, from primary myoblast cultures to three-dimensional organoids, provide essential translational validation, demonstrating that while intrinsic cellular aging contributes to muscle decline, the aged extracellular microenvironment and systemic factors play an equally significant role. Finally, clinical trials represent the ultimate validation platform to treat sarcopenia. Cross-species validation through this translational pipeline substantially increases the probability of successful clinical translation, filtering out species-specific artifacts while identifying conserved, therapeutically actionable mechanisms. The failure of single-target hormone therapies underscores the multifactorial complexity of sarcopenia. The gender differences observed in sarcopenia onset, trajectory, severity, and response to intervention demonstrate the sexually dimorphic nature of the disease and the need for multimodal interventions that account for the biology of both females and males.
This review aims to inspire scientific community in its efforts to develop effective next-generation anti-sarcopenia therapeutics by highlighting the central role of hormonal network dysregulation in disease progression. By mapping the sex-specific patterns of apelin, insulin, and oxytocin disruption, we hope to help lay the foundation for the design of interventions tailored to biological sex and hormonal status. Targeting age-related hormonal imbalances early, for example, during “possible sarcopenia,” may offer an opportunity to intercept sarcopenia at its nascent stage, before muscle loss is established, shifting the therapeutic paradigm from treatment to prevention. It is now essential to collect and integrate data on age-related changes in apelin, insulin, and oxytocin, and the networks with which they interact, to enable design of therapies that are effective for both women and men with sarcopenia or at risk of developing it.
Author Contributions
Conceptualization: Romain Menard, Romain Madelaine; Literature analysis: Romain Menard; Writing original draft: Romain Menard; Writing, Review and Editing: Romain Menard, Romain Madelaine; Funding acquisition: Romain Madelaine; Supervision: Romain Madelaine; All authors have read and agreed to the published version of the manuscript.
Acknowledgements
We are grateful to Dr. Stephen Sampson, Grant Writer at MDI Biological Laboratory, for his thoughtful proofreading and suggestions for improving the clarity of this manuscript.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement and Consent
This review article synthesizes previously published research and does not involve primary data collection, human subjects, or animal experiments. All studies cited in this review obtained the necessary ethical approvals as reported in their original publications.
Funding
Research reported in this manuscript was supported by Institutional Development Awards (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant numbers P20GM103423 and P20GM104318 (MDIBL), as well as P20GM144265 and 3P20GM144265-01A1S1 (RM).
References
- 1. Almohaisen N, Gittins M, Todd C, Sremanakova J, Sowerbutts AM, Aldossari A, Almutairi A, Jones D, Burden S. Prevalence of Undernutrition, Frailty and Sarcopenia in Community-Dwelling People Aged 50 Years and Above: Systematic Review and Meta-Analysis. Nutrients. 2022; 14:1537. https://doi.org/10.3390/nu14081537 [PubMed]
- 2. Yuan S, Larsson SC. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism. 2023; 144:155533. https://doi.org/10.1016/j.metabol.2023.155533 [PubMed]
- 3. Sander M, Oxlund B, Jespersen A, Krasnik A, Mortensen EL, Westendorp RG, Rasmussen LJ. The challenges of human population ageing. Age Ageing. 2015; 44:185–7. https://doi.org/10.1093/ageing/afu189 [PubMed]
- 4. Sayer AA, Cooper R, Arai H, Cawthon PM, Ntsama Essomba MJ, Fielding RA, Grounds MD, Witham MD, Cruz-Jentoft AJ. Sarcopenia. Nat Rev Dis Primers. 2024; 10:68. https://doi.org/10.1038/s41572-024-00550-w [PubMed]
- 5. Cao L, Morley JE. Sarcopenia Is Recognized as an Independent Condition by an International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) Code. J Am Med Dir Assoc. 2016; 17:675–7. https://doi.org/10.1016/j.jamda.2016.06.001 [PubMed]
- 6. Najm A, Niculescu AG, Grumezescu AM, Beuran M. Emerging Therapeutic Strategies in Sarcopenia: An Updated Review on Pathogenesis and Treatment Advances. Int J Mol Sci. 2024; 25:4300. https://doi.org/10.3390/ijms25084300 [PubMed]
- 7. Alorfi NM, Alshehri FS, Ashour AM. Therapeutics for Sarcopenia and Functional Disabilities in Older Adults: A Review of Phase 4 Clinical Trials. Drug Des Devel Ther. 2025; 19:2307–14. https://doi.org/10.2147/DDDT.S507033 [PubMed]
- 8. Burks TN, Cohn RD. One size may not fit all: anti-aging therapies and sarcopenia. Aging (Albany NY). 2011; 3:1142–53. https://doi.org/10.18632/aging.100409 [PubMed]
- 9. Livshits G, Kalinkovich A. Restoration of epigenetic impairment in the skeletal muscle and chronic inflammation resolution as a therapeutic approach in sarcopenia. Ageing Res Rev. 2024; 96:102267. https://doi.org/10.1016/j.arr.2024.102267 [PubMed]
- 10. Kerr HL, Krumm K, Anderson B, Christiani A, Strait L, Li T, Irwin B, Jiang S, Rybachok A, Chen A, Dacek E, Caeiro L, Merrihew GE, et al. Mouse sarcopenia model reveals sex- and age-specific differences in phenotypic and molecular characteristics. J Clin Invest. 2024; 134:e172890. https://doi.org/10.1172/JCI172890 [PubMed]
- 11. Kitajima Y, Ono Y. Estrogens maintain skeletal muscle and satellite cell functions. J Endocrinol. 2016; 229:267–75. https://doi.org/10.1530/JOE-15-0476 [PubMed]
- 12. Della Peruta C, Lozanoska-Ochser B, Renzini A, Moresi V, Sanchez Riera C, Bouché M, Coletti D. Sex Differences in Inflammation and Muscle Wasting in Aging and Disease. Int J Mol Sci. 2023; 24:4651. https://doi.org/10.3390/ijms24054651 [PubMed]
- 13. Fernández-Garza LE, Guillen-Silva F, Sotelo-Ibarra MA, Domínguez-Mendoza AE, Barrera-Barrera SA, Barrera-Saldaña HA. Growth hormone and aging: a clinical review. Front Aging. 2025; 6:1549453. https://doi.org/10.3389/fragi.2025.1549453 [PubMed]
- 14. Jiang JJ, Chen SM, Chen J, Wu L, Ye JT, Zhang Q. Serum IGF-1 levels are associated with sarcopenia in elderly men but not in elderly women. Aging Clin Exp Res. 2022; 34:2465–71. https://doi.org/10.1007/s40520-022-02180-2 [PubMed]
- 15. Bleach R, Sherlock M, O’Reilly MW, McIlroy M. Growth Hormone/Insulin Growth Factor Axis in Sex Steroid Associated Disorders and Related Cancers. Front Cell Dev Biol. 2021; 9:630503. https://doi.org/10.3389/fcell.2021.630503 [PubMed]
- 16. Sattler FR. Growth hormone in the aging male. Best Pract Res Clin Endocrinol Metab. 2013; 27:541–55. https://doi.org/10.1016/j.beem.2013.05.003 [PubMed]
- 17. Sinha RA, Yen PM. Metabolic Messengers: Thyroid Hormones. Nat Metab. 2024; 6:639–50. https://doi.org/10.1038/s42255-024-00986-0 [PubMed]
- 18. Das M, Kumar R, Kumar V, Gurusubramanian G, Roy VK. Gender differences in expression and localization of the apelin receptor in mice skin. J Mol Histol. 2025; 56:197. https://doi.org/10.1007/s10735-025-10492-6 [PubMed]
- 19. Kawakami M, Yokota-Nakagi N, Uji M, Yoshida KI, Tazumi S, Takamata A, Uchida Y, Morimoto K. Estrogen replacement enhances insulin-induced AS160 activation and improves insulin sensitivity in ovariectomized rats. Am J Physiol Endocrinol Metab. 2018; 315:E1296–304. https://doi.org/10.1152/ajpendo.00131.2018 [PubMed]
- 20. Rak A, Drwal E, Rame C, Knapczyk-Stwora K, Słomczyńska M, Dupont J, Gregoraszczuk EL. Expression of apelin and apelin receptor (APJ) in porcine ovarian follicles and in vitro effect of apelin on steroidogenesis and proliferation through APJ activation and different signaling pathways. Theriogenology. 2017; 96:126–35. https://doi.org/10.1016/j.theriogenology.2017.04.014 [PubMed]
- 21. O’Carroll AM, Lolait SJ, Harris LE, Pope GR. The apelin receptor APJ: journey from an orphan to a multifaceted regulator of homeostasis. J Endocrinol. 2013; 219:R13–35. https://doi.org/10.1530/JOE-13-0227 [PubMed]
- 22. Han S, Englander EW, Gomez GA, Rastellini C, Quertermous T, Kundu RK, Greeley GH
Jr . Pancreatic Islet APJ Deletion Reduces Islet Density and Glucose Tolerance in Mice. Endocrinology. 2015; 156:2451–60. https://doi.org/10.1210/en.2014-1631 [PubMed] - 23. Yue P, Jin H, Aillaud M, Deng AC, Azuma J, Asagami T, Kundu RK, Reaven GM, Quertermous T, Tsao PS. Apelin is necessary for the maintenance of insulin sensitivity. Am J Physiol Endocrinol Metab. 2010; 298:E59–67.
- 24. Li C, Cheng H, Adhikari BK, Wang S, Yang N, Liu W, Sun J, Wang Y. The Role of Apelin-APJ System in Diabetes and Obesity. Front Endocrinol (Lausanne). 2022; 13:820002. https://doi.org/10.3389/fendo.2022.820002 [PubMed]
- 25. Dray C, Debard C, Jager J, Disse E, Daviaud D, Martin P, Attané C, Wanecq E, Guigné C, Bost F, Tanti JF, Laville M, Vidal H, et al. Apelin and APJ regulation in adipose tissue and skeletal muscle of type 2 diabetic mice and humans. Am J Physiol Endocrinol Metab. 2010; 298:E1161–9. https://doi.org/10.1152/ajpendo.00598.2009 [PubMed]
- 26. Hwangbo C, Wu J, Papangeli I, Adachi T, Sharma B, Park S, Zhao L, Ju H, Go GW, Cui G, Inayathullah M, Job JK, Rajadas J, et al. Endothelial APLNR regulates tissue fatty acid uptake and is essential for apelin’s glucose-lowering effects. Sci Transl Med. 2017; 9:eaad4000. https://doi.org/10.1126/scitranslmed.aad4000 [PubMed]
- 27. Avgerinou C. Sarcopenia: why it matters in general practice. Br J Gen Pract. 2020; 70:200–1. https://doi.org/10.3399/bjgp20X709253 [PubMed]
- 28. Bertschi D, Kiss CM, Beerli N, Mauthner O, Kressig RW. Impact of sarcopenia on daily functioning: a cross-sectional study among older inpatients. Aging Clin Exp Res. 2022; 34:2041–6. https://doi.org/10.1007/s40520-022-02175-z [PubMed]
- 29. Dos Santos L, Cyrino ES, Antunes M, Santos DA, Sardinha LB. Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. J Cachexia Sarcopenia Muscle. 2017; 8:245–50. https://doi.org/10.1002/jcsm.12160 [PubMed]
- 30. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019; 393:2636–46. https://doi.org/10.1016/S0140-6736(19)31138-9 [PubMed] Erratum in: Lancet. 2019; 393:2590. DOI: 10.1016/S0140-6736(19)31465-5 PMID:31258129.
- 31. Anker SD, Morley JE, von Haehling S. Welcome to the ICD-10 code for sarcopenia. J Cachexia Sarcopenia Muscle. 2016; 7:512–4. https://doi.org/10.1002/jcsm.12147 [PubMed]
- 32. Yasuda T. Selected Methods of Resistance Training for Prevention and Treatment of Sarcopenia. Cells. 2022; 11:1389. https://doi.org/10.3390/cells11091389 [PubMed]
- 33. Ali SR, Nkembo AT, Tipparaju SM, Ashraf M, Xuan W. Sarcopenia: recent advances for detection, progression, and metabolic alterations along with therapeutic targets. Can J Physiol Pharmacol. 2024; 102:697–708. https://doi.org/10.1139/cjpp-2024-0201 [PubMed]
- 34. García-Hermoso A, Cavero-Redondo I, Ramírez-Vélez R, Ruiz JR, Ortega FB, Lee DC, Martínez-Vizcaíno V. Muscular Strength as a Predictor of All-Cause Mortality in an Apparently Healthy Population: A Systematic Review and Meta-Analysis of Data From Approximately 2 Million Men and Women. Arch Phys Med Rehabil. 2018; 99:2100–13.e5. https://doi.org/10.1016/j.apmr.2018.01.008 [PubMed]
- 35. Guttikonda D, Smith AL. Sarcopenia Assessment Techniques. Clin Liver Dis (Hoboken). 2021; 18:189–92. https://doi.org/10.1002/cld.1111 [PubMed]
- 36. Fukuhara S, Kobayashi T, Hamaoka M, Naruhiko H, Oishi K, Namba Y, Oshita KO, Matsubara K, Takei D, Nakano R, Sakai H, Kuroda S, Tahara H, et al. Sarcopenia’s Impact Defined by Grip Strength and Muscle Mass on Post-hepatectomy Outcomes: A Multicenter Analysis. In Vivo. 2024; 38:2827–35. https://doi.org/10.21873/invivo.13763 [PubMed]
- 37. Lee SH, Gong HS. Measurement and Interpretation of Handgrip Strength for Research on Sarcopenia and Osteoporosis. J Bone Metab. 2020; 27:85–96. https://doi.org/10.11005/jbm.2020.27.2.85 [PubMed]
- 38. Ji S, Jung HW, Baek JY, Jang IY, Lee E. Sarcopenia as the Mobility Phenotype of Aging: Clinical Implications. J Bone Metab. 2024; 31:1–12. https://doi.org/10.11005/jbm.2024.31.1.1 [PubMed]
- 39. Juby AG, Davis CM, Minimaana S, Mager DR. Addressing the Main Barrier to Sarcopenia Identification: Utility of Practical Office-Based Bioimpedance Tools Vs. Dual Energy X-ray Absorptiometry (DXA) Body Composition for Identification of Low Muscle Mass in Older Adults. Can Geriatr J. 2023; 26:493–501. https://doi.org/10.5770/cgj.26.626 [PubMed]
- 40. Treviño-Aguirre E, López-Teros T, Gutiérrez-Robledo L, Vandewoude M, Pérez-Zepeda M. Availability and use of dual energy X-ray absorptiometry (DXA) and bio-impedance analysis (BIA) for the evaluation of sarcopenia by Belgian and Latin American geriatricians. J Cachexia Sarcopenia Muscle. 2014; 5:79–81. https://doi.org/10.1007/s13539-013-0126-6 [PubMed]
- 41. Ruby L, Sanabria SJ, Saltybaeva N, Frauenfelder T, Alkadhi H, Rominger MB. Comparison of ultrasound speed-of-sound of the lower extremity and lumbar muscle assessed with computed tomography for muscle loss assessment. Medicine (Baltimore). 2021; 100:e25947. https://doi.org/10.1097/MD.0000000000025947 [PubMed]
- 42. Kurazumi H, Suzuki R, Nawata R, Matsunaga K, Miyazaki Y, Yamashita A, Okamura T, Mikamo A, Sano M, Hamano K. Effects of computed tomography-defined sarcopenia on patients undergoing transcatheter aortic valve implantation. Interdiscip Cardiovasc Thorac Surg. 2025; 40:ivaf083. https://doi.org/10.1093/icvts/ivaf083 [PubMed]
- 43. Luengpradidgun L, Chamroonkul N, Sripongpun P, Kaewdech A, Tanutit P, Ina N, Piratvisuth T. Utility of handgrip strength (HGS) and bioelectrical impedance analysis (BIA) in the diagnosis of sarcopenia in cirrhotic patients. BMC Gastroenterol. 2022; 22:159. https://doi.org/10.1186/s12876-022-02236-7 [PubMed]
- 44. Aleixo GF, Shachar SS, Nyrop KA, Muss HB, Battaglini CL, Williams GR. Bioelectrical Impedance Analysis for the Assessment of Sarcopenia in Patients with Cancer: A Systematic Review. Oncologist. 2020; 25:170–82. https://doi.org/10.1634/theoncologist.2019-0600 [PubMed]
- 45. Zhao R, Li X, Jiang Y, Su N, Li J, Kang L, Zhang Y, Yang M. Evaluation of Appendicular Muscle Mass in Sarcopenia in Older Adults Using Ultrasonography: A Systematic Review and Meta-Analysis. Gerontology. 2022; 68:1174–98. https://doi.org/10.1159/000525758 [PubMed]
- 46. Hida T, Ando K, Kobayashi K, Ito K, Tsushima M, Kobayakawa T, Morozumi M, Tanaka S, Machino M, Ota K, Kanbara S, Ito S, Ishiguro N, et al. < Editors’ Choice > Ultrasound measurement of thigh muscle thickness for assessment of sarcopenia. Nagoya J Med Sci. 2018; 80:519–27. https://doi.org/10.18999/nagjms.80.4.519 [PubMed]
- 47. Sánchez-Castellano C, Martín-Aragón S, Bermejo-Bescós P, Vaquero-Pinto N, Miret-Corchado C, Merello de Miguel A, Cruz-Jentoft AJ. Biomarkers of sarcopenia in very old patients with hip fracture. J Cachexia Sarcopenia Muscle. 2020; 11:478–86. https://doi.org/10.1002/jcsm.12508 [PubMed]
- 48. Bodine SC, Baehr LM. Skeletal muscle atrophy and the E3 ubiquitin ligases MuRF1 and MAFbx/atrogin-1. Am J Physiol Endocrinol Metab. 2014; 307:E469–84. https://doi.org/10.1152/ajpendo.00204.2014 [PubMed]
- 49. Sandri M, Sandri C, Gilbert A, Skurk C, Calabria E, Picard A, Walsh K, Schiaffino S, Lecker SH, Goldberg AL. Foxo transcription factors induce the atrophy-related ubiquitin ligase atrogin-1 and cause skeletal muscle atrophy. Cell. 2004; 117:399–412. https://doi.org/10.1016/s0092-8674(04)00400-3 [PubMed]
- 50. Gumucio JP, Mendias CL. Atrogin-1, MuRF-1, and sarcopenia. Endocrine. 2013; 43:12–21. https://doi.org/10.1007/s12020-012-9751-7 [PubMed]
- 51. Baczek J, Silkiewicz M, Wojszel ZB. Myostatin as a Biomarker of Muscle Wasting and other Pathologies-State of the Art and Knowledge Gaps. Nutrients. 2020; 12:2401. https://doi.org/10.3390/nu12082401 [PubMed]
- 52. Ishibashi C, Nakanishi K, Nishida M, Shinomiya H, Shinzawa M, Kanayama D, Yamamoto R, Kudo T, Nagatomo I, Yamauchi-Takihara K. Myostatin as a plausible biomarker for early stage of sarcopenic obesity. Sci Rep. 2024; 14:28629. https://doi.org/10.1038/s41598-024-79534-5 [PubMed]
- 53. Choi SJ, Lee MS, Kang DH, Ko GJ, Lim HS, Yu BC, Park MY, Kim JK, Kim CH, Hwang SD, Kim JC, Won CW, An WS. Myostatin/Appendicular Skeletal Muscle Mass (ASM) Ratio, Not Myostatin, Is Associated with Low Handgrip Strength in Community-Dwelling Older Women. Int J Environ Res Public Health. 2021; 18:7344. https://doi.org/10.3390/ijerph18147344 [PubMed]
- 54. Bergen HR 3r, Farr JN, Vanderboom PM, Atkinson EJ, White TA, Singh RJ, Khosla S, LeBrasseur NK. Myostatin as a mediator of sarcopenia versus homeostatic regulator of muscle mass: insights using a new mass spectrometry-based assay. Skelet Muscle. 2015; 5:21. https://doi.org/10.1186/s13395-015-0047-5 [PubMed]
- 55. Peng LN, Lee WJ, Liu LK, Lin MH, Chen LK. Healthy community-living older men differ from women in associations between myostatin levels and skeletal muscle mass. J Cachexia Sarcopenia Muscle. 2018; 9:635–42. https://doi.org/10.1002/jcsm.12302 [PubMed]
- 56. Chew J, Tay L, Lim JP, Leung BP, Yeo A, Yew S, Ding YY, Lim WS. Serum Myostatin and IGF-1 as Gender-Specific Biomarkers of Frailty and Low Muscle Mass in Community-Dwelling Older Adults. J Nutr Health Aging. 2019; 23:979–86. https://doi.org/10.1007/s12603-019-1255-1 [PubMed]
- 57. Wang X, Bai Y, Zhang F, Que H. Association of sarcopenia index, based on serum creatinine and cystatin C, with incident diabetes mellitus. Eur J Med Res. 2025; 30:151. https://doi.org/10.1186/s40001-025-02405-w [PubMed]
- 58. He Q, Jiang J, Xie L, Zhang L, Yang M. A sarcopenia index based on serum creatinine and cystatin C cannot accurately detect either low muscle mass or sarcopenia in urban community-dwelling older people. Sci Rep. 2018; 8:11534. https://doi.org/10.1038/s41598-018-29808-6 [PubMed]
- 59. Singhal S, Singh S, Upadhyay AD, Dwivedi SN, Das CJ, Mohta S, Chatterjee P, Dey AB, Chakrawarty A. Serum creatinine and cystatin C-based index can be a screening biomarker for sarcopenia in older population. Eur Geriatr Med. 2019; 10:625–30. https://doi.org/10.1007/s41999-019-00197-x [PubMed]
- 60. Guo XY, Li LW. Hs-CRP/HDL-C ratio as a predictive inflammatory-lipid marker for sarcopenia: evidence from NHANES 2015-2018. Front Immunol. 2025; 16:1600421. https://doi.org/10.3389/fimmu.2025.1600421 [PubMed]
- 61. Dupont J, Antonio L, Dedeyne L, O’Neill TW, Vanderschueren D, Rastrelli G, Maggi M, Bártfai G, Casanueva FF, Giwercman A, Słowikowska-Hilczer J, Punab M, Huhtaniemi IT, et al. Inflammatory markers are associated with quality of life, physical activity, and gait speed but not sarcopenia in aged men (40-79 years). J Cachexia Sarcopenia Muscle. 2021; 12:1818–31. https://doi.org/10.1002/jcsm.12785 [PubMed]
- 62. Cacciatore S, Calvani R, Esposito I, Massaro C, Gava G, Picca A, Tosato M, Marzetti E, Landi F. Emerging Targets and Treatments for Sarcopenia: A Narrative Review. Nutrients. 2024; 16:3271. https://doi.org/10.3390/nu16193271 [PubMed]
- 63. Hurst C, Robinson SM, Witham MD, Dodds RM, Granic A, Buckland C, De Biase S, Finnegan S, Rochester L, Skelton DA, Sayer AA. Resistance exercise as a treatment for sarcopenia: prescription and delivery. Age Ageing. 2022; 51:afac003. https://doi.org/10.1093/ageing/afac003 [PubMed]
- 64. Chen N, He X, Feng Y, Ainsworth BE, Liu Y. Effects of resistance training in healthy older people with sarcopenia: a systematic review and meta-analysis of randomized controlled trials. Eur Rev Aging Phys Act. 2021; 18:23. https://doi.org/10.1186/s11556-021-00277-7 [PubMed]
- 65. Liu S, Zhang L, Li S. Advances in nutritional supplementation for sarcopenia management. Front Nutr. 2023; 10:1189522. https://doi.org/10.3389/fnut.2023.1189522 [PubMed]
- 66. Kwak JY, Kwon KS. Pharmacological Interventions for Treatment of Sarcopenia: Current Status of Drug Development for Sarcopenia. Ann Geriatr Med Res. 2019; 23:98–104. https://doi.org/10.4235/agmr.19.0028 [PubMed]
- 67. Bromer FD, Lodberg A, Eijken M, Andersen CB, Poulsen MF, Thomsen JS, Brüel A. The Effect of Anti-Activin Receptor Type IIA and Type IIB Antibody on Muscle, Bone and Blood in Healthy and Osteosarcopenic Mice. J Cachexia Sarcopenia Muscle. 2025; 16:e13718. https://doi.org/10.1002/jcsm.13718 [PubMed]
- 68. Gupta P, Kumar S. Sarcopenia and Endocrine Ageing: Are They Related? Cureus. 2022; 14:e28787. https://doi.org/10.7759/cureus.28787 [PubMed]
- 69. Engman V, Critchlow AJ, Laakkonen EK, Hansen M, Mason S, Lamon S. The Role and Regulation of Intramuscular Sex Hormones in Skeletal Muscle: A Systematic Review. J Clin Endocrinol Metab. 2025; 110:e1732–46. https://doi.org/10.1210/clinem/dgaf174 [PubMed]
- 70. Buckinx F, Aubertin-Leheudre M. Sarcopenia in Menopausal Women: Current Perspectives. Int J Womens Health. 2022; 14:805–19. https://doi.org/10.2147/IJWH.S340537 [PubMed]
- 71. Shin MJ, Jeon YK, Kim IJ. Testosterone and Sarcopenia. World J Mens Health. 2018; 36:192–8. https://doi.org/10.5534/wjmh.180001 [PubMed]
- 72. Brown AD, Davis LA, Fogarty MJ, Sieck GC. Mitochondrial Fragmentation and Dysfunction in Type IIx/IIb Diaphragm Muscle Fibers in 24-Month Old Fischer 344 Rats. Front Physiol. 2021; 12:727585. https://doi.org/10.3389/fphys.2021.727585 [PubMed]
- 73. Hedberg-Oldfors C, Lindgren U, Visuttijai K, Lööf D, Roos S, Thomsen C, Oldfors A. Respiratory chain dysfunction in perifascicular muscle fibres in patients with dermatomyositis is associated with mitochondrial DNA depletion. Neuropathol Appl Neurobiol. 2022; 48:e12841. https://doi.org/10.1111/nan.12841 [PubMed]
- 74. Di Leo V, Bernardino Gomes TM, Vincent AE. Interactions of mitochondrial and skeletal muscle biology in mitochondrial myopathy. Biochem J. 2023; 480:1767–89. https://doi.org/10.1042/BCJ20220233 [PubMed]
- 75. Tian X, Lou S, Shi R. From mitochondria to sarcopenia: role of 17β-estradiol and testosterone. Front Endocrinol (Lausanne). 2023; 14:1156583. https://doi.org/10.3389/fendo.2023.1156583 [PubMed]
- 76. La Colla A, Pronsato L, Milanesi L, Vasconsuelo A. 17β-Estradiol and testosterone in sarcopenia: Role of satellite cells. Ageing Res Rev. 2015; 24:166–77. https://doi.org/10.1016/j.arr.2015.07.011 [PubMed]
- 77. Elabd C, Cousin W, Upadhyayula P, Chen RY, Chooljian MS, Li J, Kung S, Jiang KP, Conboy IM. Oxytocin is an age-specific circulating hormone that is necessary for muscle maintenance and regeneration. Nat Commun. 2014; 5:4082. https://doi.org/10.1038/ncomms5082 [PubMed]
- 78. Shibata S, Ueno C, Ito T, Yamanouchi K, Matsuwaki T, Nishihara M. Skeletal muscle growth defect in human growth hormone transgenic rat is accompanied by phenotypic changes in progenitor cells. Age (Dordr). 2010; 32:239–53. https://doi.org/10.1007/s11357-010-9130-3 [PubMed]
- 79. Bian A, Ma Y, Zhou X, Guo Y, Wang W, Zhang Y, Wang X. Association between sarcopenia and levels of growth hormone and insulin-like growth factor-1 in the elderly. BMC Musculoskelet Disord. 2020; 21:214. https://doi.org/10.1186/s12891-020-03236-y [PubMed]
- 80. Shin HE, Walston JD, Kim M, Won CW. Sex-Specific Differences in the Effect of Free Testosterone on Sarcopenia Components in Older Adults. Front Endocrinol (Lausanne). 2021; 12:695614. https://doi.org/10.3389/fendo.2021.695614 [PubMed] Erratum in: Front Endocrinol (Lausanne). 2022; 13:876640. DOI: 10.3389/fendo.2022.876640 PMID:35317225.
- 81. Kovacheva EL, Hikim AP, Shen R, Sinha I, Sinha-Hikim I. Testosterone supplementation reverses sarcopenia in aging through regulation of myostatin, c-Jun NH2-terminal kinase, Notch, and Akt signaling pathways. Endocrinology. 2010; 151:628–38. https://doi.org/10.1210/en.2009-1177 [PubMed]
- 82. Payne AM, Zheng Z, Messi ML, Milligan CE, González E, Delbono O. Motor neurone targeting of IGF-1 prevents specific force decline in ageing mouse muscle. J Physiol. 2006; 570:283–94. https://doi.org/10.1113/jphysiol.2005.100032 [PubMed]
- 83. Sacheck JM, Ohtsuka A, McLary SC, Goldberg AL, and New Collective Author. IGF-I stimulates muscle growth by suppressing protein breakdown and expression of atrophy-related ubiquitin ligases, atrogin-1 and MuRF1. Am J Physiol Endocrinol Metab. 2004; 287:E591–601. https://doi.org/10.1152/ajpendo.00073.2004 [PubMed]
- 84. Turner JD, Rotwein P, Novakofski J, Bechtel PJ. Induction of mRNA for IGF-I and -II during growth hormone-stimulated muscle hypertrophy. Am J Physiol. 1988; 255:E513–7. https://doi.org/10.1152/ajpendo.1988.255.4.E513 [PubMed]
- 85. Gonzalez Rodriguez E, Marques-Vidal P, Aubry-Rozier B, Papadakis G, Preisig M, Kuehner C, Vollenweider P, Waeber G, Hans D, Lamy O. Diurnal Salivary Cortisol in Sarcopenic Postmenopausal Women: The OsteoLaus Cohort. Calcif Tissue Int. 2021; 109:499–509. https://doi.org/10.1007/s00223-021-00863-y [PubMed]
- 86. Liu F, Yang Q, Yang K, Sun J, Li Y, Ban B, Wang Y, Zhang M. Cortisol Circadian Rhythm and Sarcopenia in Patients With Type 2 Diabetes: A Cross-Sectional Study. J Cachexia Sarcopenia Muscle. 2025; 16:e13727. https://doi.org/10.1002/jcsm.13727 [PubMed]
- 87. Menard R, Morin E, Morse D, Halluin C, Pende M, Baanannou A, Grendler J, Fuqua H, Li J, Lancelot L, Drent J, Bonnet F, Graber JH, et al. Zebrafish genetic model of neuromuscular degeneration associated with Atrogin-1 expression. PLoS Genet. 2026; 22:e1012019. https://doi.org/10.1371/journal.pgen.1012019 [PubMed]
- 88. Minciullo PL, Catalano A, Mandraffino G, Casciaro M, Crucitti A, Maltese G, Morabito N, Lasco A, Gangemi S, Basile G. Inflammaging and Anti-Inflammaging: The Role of Cytokines in Extreme Longevity. Arch Immunol Ther Exp (Warsz). 2016; 64:111–26. https://doi.org/10.1007/s00005-015-0377-3 [PubMed]
- 89. Huo F, Liu Q, Liu H. Contribution of muscle satellite cells to sarcopenia. Front Physiol. 2022; 13:892749. https://doi.org/10.3389/fphys.2022.892749 [PubMed]
- 90. Sousa-Victor P, Muñoz-Cánoves P. Regenerative decline of stem cells in sarcopenia. Mol Aspects Med. 2016; 50:109–17. https://doi.org/10.1016/j.mam.2016.02.002 [PubMed]
- 91. Mauro A. Satellite cell of skeletal muscle fibers. J Biophys Biochem Cytol. 1961; 9:493–5. https://doi.org/10.1083/jcb.9.2.493 [PubMed]
- 92. Evano B, Khalilian S, Le Carrou G, Almouzni G, Tajbakhsh S. Dynamics of Asymmetric and Symmetric Divisions of Muscle Stem Cells In Vivo and on Artificial Niches. Cell Rep. 2020; 30:3195–206.e7. https://doi.org/10.1016/j.celrep.2020.01.097 [PubMed]
- 93. Tedesco FS, Dellavalle A, Diaz-Manera J, Messina G, Cossu G. Repairing skeletal muscle: regenerative potential of skeletal muscle stem cells. J Clin Invest. 2010; 120:11–9. https://doi.org/10.1172/JCI40373 [PubMed]
- 94. Chakkalakal JV, Jones KM, Basson MA, Brack AS. The aged niche disrupts muscle stem cell quiescence. Nature. 2012; 490:355–60. https://doi.org/10.1038/nature11438 [PubMed]
- 95. Sousa-Victor P, Gutarra S, García-Prat L, Rodriguez-Ubreva J, Ortet L, Ruiz-Bonilla V, Jardí M, Ballestar E, González S, Serrano AL, Perdiguero E, Muñoz-Cánoves P. Geriatric muscle stem cells switch reversible quiescence into senescence. Nature. 2014; 506:316–21. https://doi.org/10.1038/nature13013 [PubMed]
- 96. Park SS, Kwon ES, Kwon KS. Molecular mechanisms and therapeutic interventions in sarcopenia. Osteoporos Sarcopenia. 2017; 3:117–22. https://doi.org/10.1016/j.afos.2017.08.098 [PubMed]
- 97. Sousa-Victor P, Perdiguero E, Muñoz-Cánoves P. Geroconversion of aged muscle stem cells under regenerative pressure. Cell Cycle. 2014; 13:3183–90. https://doi.org/10.4161/15384101.2014.965072 [PubMed]
- 98. Hughes DC, Baehr LM, Waddell DS, Sharples AP, Bodine SC. Ubiquitin Ligases in Longevity and Aging Skeletal Muscle. Int J Mol Sci. 2022; 23:7602. https://doi.org/10.3390/ijms23147602 [PubMed]
- 99. Paez HG, Pitzer CR, Alway SE. Age-Related Dysfunction in Proteostasis and Cellular Quality Control in the Development of Sarcopenia. Cells. 2023; 12:249. https://doi.org/10.3390/cells12020249 [PubMed]
- 100. Latres E, Amini AR, Amini AA, Griffiths J, Martin FJ, Wei Y, Lin HC, Yancopoulos GD, Glass DJ. Insulin-like growth factor-1 (IGF-1) inversely regulates atrophy-induced genes via the phosphatidylinositol 3-kinase/Akt/mammalian target of rapamycin (PI3K/Akt/mTOR) pathway. J Biol Chem. 2005; 280:2737–44. https://doi.org/10.1074/jbc.M407517200 [PubMed]
- 101. Cuthbertson D, Smith K, Babraj J, Leese G, Waddell T, Atherton P, Wackerhage H, Taylor PM, Rennie MJ. Anabolic signaling deficits underlie amino acid resistance of wasting, aging muscle. FASEB J. 2005; 19:422–4. https://doi.org/10.1096/fj.04-2640fje [PubMed]
- 102. Fry CS, Drummond MJ, Glynn EL, Dickinson JM, Gundermann DM, Timmerman KL, Walker DK, Dhanani S, Volpi E, Rasmussen BB. Aging impairs contraction-induced human skeletal muscle mTORC1 signaling and protein synthesis. Skelet Muscle. 2011; 1:11. https://doi.org/10.1186/2044-5040-1-11 [PubMed]
- 103. Junnila RK, List EO, Berryman DE, Murrey JW, Kopchick JJ. The GH/IGF-1 axis in ageing and longevity. Nat Rev Endocrinol. 2013; 9:366–76. https://doi.org/10.1038/nrendo.2013.67 [PubMed]
- 104. Gaffney CJ, Pollard A, Barratt TF, Constantin-Teodosiu D, Greenhaff PL, Szewczyk NJ. Greater loss of mitochondrial function with ageing is associated with earlier onset of sarcopenia in C. elegans. Aging (Albany NY). 2018; 10:3382–96. https://doi.org/10.18632/aging.101654 [PubMed]
- 105. Migliavacca E, Tay SK, Patel HP, Sonntag T, Civiletto G, McFarlane C, Forrester T, Barton SJ, Leow MK, Antoun E, Charpagne A, Seng Chong Y, Descombes P, et al. Mitochondrial oxidative capacity and NAD+ biosynthesis are reduced in human sarcopenia across ethnicities. Nat Commun. 2019; 10:5808. https://doi.org/10.1038/s41467-019-13694-1 [PubMed]
- 106. Musci RV, Hamilton KL, Miller BF. Targeting mitochondrial function and proteostasis to mitigate dynapenia. Eur J Appl Physiol. 2018; 118:1–9. https://doi.org/10.1007/s00421-017-3730-x [PubMed]
- 107. Goulding RP, Charlton BT, Breedveld EA, van der Laan M, Strating AR, Noort W, Kolodyazhna A, Appelman B, van Vugt M, Grootemaat AE, van der Wel NN, de Koning JJ, Bloemers FW, Wüst RC. Skeletal muscle mitochondrial fragmentation predicts age-associated decline in physical capacity. Aging Cell. 2025; 24:e14386. https://doi.org/10.1111/acel.14386 [PubMed]
- 108. Del Campo A, Contreras-Hernández I, Castro-Sepúlveda M, Campos CA, Figueroa R, Tevy MF, Eisner V, Casas M, Jaimovich E. Muscle function decline and mitochondria changes in middle age precede sarcopenia in mice. Aging (Albany NY). 2018; 10:34–55. https://doi.org/10.18632/aging.101358 [PubMed]
- 109. Hunter SK, Pereira HM, Keenan KG. The aging neuromuscular system and motor performance. J Appl Physiol (1985). 2016; 121:982–95. https://doi.org/10.1152/japplphysiol.00475.2016 [PubMed]
- 110. Piasecki M, Ireland A, Piasecki J, Stashuk DW, Swiecicka A, Rutter MK, Jones DA, McPhee JS. Failure to expand the motor unit size to compensate for declining motor unit numbers distinguishes sarcopenic from non-sarcopenic older men. J Physiol. 2018; 596:1627–37. https://doi.org/10.1113/JP275520 [PubMed]
- 111. Arnold WD, Clark BC. Neuromuscular junction transmission failure in aging and sarcopenia: The nexus of the neurological and muscular systems. Ageing Res Rev. 2023; 89:101966. https://doi.org/10.1016/j.arr.2023.101966 [PubMed]
- 112. Deschenes MR, Flannery R, Hawbaker A, Patek L, Mifsud M. Adaptive Remodeling of the Neuromuscular Junction with Aging. Cells. 2022; 11:1150. https://doi.org/10.3390/cells11071150 [PubMed]
- 113. Clark JA, Southam KA, Blizzard CA, King AE, Dickson TC. Axonal degeneration, distal collateral branching and neuromuscular junction architecture alterations occur prior to symptom onset in the SOD1(G93A) mouse model of amyotrophic lateral sclerosis. J Chem Neuroanat. 2016; 76:35–47. https://doi.org/10.1016/j.jchemneu.2016.03.003 [PubMed]
- 114. Valbuena Perez JV, Linnenberger R, Dembek A, Bruscoli S, Riccardi C, Schulz MH, Meyer MR, Kiemer AK, Hoppstädter J. Altered glucocorticoid metabolism represents a feature of macroph-aging. Aging Cell. 2020; 19:e13156. https://doi.org/10.1111/acel.13156 [PubMed]
- 115. Prattichizzo F, De Nigris V, La Sala L, Procopio AD, Olivieri F, Ceriello A. “Inflammaging” as a Druggable Target: A Senescence-Associated Secretory Phenotype-Centered View of Type 2 Diabetes. Oxid Med Cell Longev. 2016; 2016:1810327. https://doi.org/10.1155/2016/1810327 [PubMed]
- 116. Wiley CD, Velarde MC, Lecot P, Liu S, Sarnoski EA, Freund A, Shirakawa K, Lim HW, Davis SS, Ramanathan A, Gerencser AA, Verdin E, Campisi J. Mitochondrial Dysfunction Induces Senescence with a Distinct Secretory Phenotype. Cell Metab. 2016; 23:303–14. https://doi.org/10.1016/j.cmet.2015.11.011 [PubMed]
- 117. Jung TW, Lee SH, Kim HC, Bang JS, Abd El-Aty AM, Hacımüftüoğlu A, Shin YK, Jeong JH. METRNL attenuates lipid-induced inflammation and insulin resistance via AMPK or PPARδ-dependent pathways in skeletal muscle of mice. Exp Mol Med. 2018; 50:1–11. https://doi.org/10.1038/s12276-018-0147-5 [PubMed]
- 118. Kumar P, Liu C, Hsu JW, Chacko S, Minard C, Jahoor F, Sekhar RV. Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition: Results of a pilot clinical trial. Clin Transl Med. 2021; 11:e372. https://doi.org/10.1002/ctm2.372 [PubMed]
- 119. Sanz-Cánovas J, López-Sampalo A, Cobos-Palacios L, Ricci M, Hernández-Negrín H, Mancebo-Sevilla JJ, Álvarez-Recio E, López-Carmona MD, Pérez-Belmonte LM, Gómez-Huelgas R, Bernal-López MR. Management of Type 2 Diabetes Mellitus in Elderly Patients with Frailty and/or Sarcopenia. Int J Environ Res Public Health. 2022; 19:8677. https://doi.org/10.3390/ijerph19148677 [PubMed]
- 120. Palacios D, Mozzetta C, Consalvi S, Caretti G, Saccone V, Proserpio V, Marquez VE, Valente S, Mai A, Forcales SV, Sartorelli V, Puri PL. TNF/p38α/polycomb signaling to Pax7 locus in satellite cells links inflammation to the epigenetic control of muscle regeneration. Cell Stem Cell. 2010; 7:455–69. https://doi.org/10.1016/j.stem.2010.08.013 [PubMed]
- 121. Nie M, Liu J, Yang Q, Seok HY, Hu X, Deng ZL, Wang DZ. MicroRNA-155 facilitates skeletal muscle regeneration by balancing pro- and anti-inflammatory macrophages. Cell Death Dis. 2016; 7:e2261. https://doi.org/10.1038/cddis.2016.165 [PubMed]
- 122. Shin K, Kenward C, Rainey JK. Apelinergic System Structure and Function. Compr Physiol. 2017; 8:407–50. https://doi.org/10.1002/cphy.c170028 [PubMed]
- 123. Respekta N, Pich K, Dawid M, Mlyczyńska E, Kurowska P, Rak A. The Apelinergic System: Apelin, ELABELA, and APJ Action on Cell Apoptosis: Anti-Apoptotic or Pro-Apoptotic Effect? Cells. 2022; 12:150. https://doi.org/10.3390/cells12010150 [PubMed]
- 124. Vinel C, Lukjanenko L, Batut A, Deleruyelle S, Pradère JP, Le Gonidec S, Dortignac A, Geoffre N, Pereira O, Karaz S, Lee U, Camus M, Chaoui K, et al. The exerkine apelin reverses age-associated sarcopenia. Nat Med. 2018; 24:1360–71. https://doi.org/10.1038/s41591-018-0131-6 [PubMed]
- 125. Ivanov MN, Stoyanov DS, Pavlov SP, Tonchev AB. Distribution, Function, and Expression of the Apelinergic System in the Healthy and Diseased Mammalian Brain. Genes (Basel). 2022; 13:2172. https://doi.org/10.3390/genes13112172 [PubMed]
- 126. Dagamajalu S, Rex DA, Philem PD, Rainey JK, Keshava Prasad TS. A network map of apelin-mediated signaling. J Cell Commun Signal. 2022; 16:137–43. https://doi.org/10.1007/s12079-021-00614-6 [PubMed]
- 127. Tatin F, Renaud-Gabardos E, Godet AC, Hantelys F, Pujol F, Morfoisse F, Calise D, Viars F, Valet P, Masri B, Prats AC, Garmy-Susini B. Apelin modulates pathological remodeling of lymphatic endothelium after myocardial infarction. JCI Insight. 2017; 2:e93887. https://doi.org/10.1172/jci.insight.93887 [PubMed]
- 128. Son JS, Chae SA, Wang H, Chen Y, Bravo Iniguez A, de Avila JM, Jiang Z, Zhu MJ, Du M. Maternal Inactivity Programs Skeletal Muscle Dysfunction in Offspring Mice by Attenuating Apelin Signaling and Mitochondrial Biogenesis. Cell Rep. 2020; 33:108461. https://doi.org/10.1016/j.celrep.2020.108461 [PubMed]
- 129. Perjés Á, Skoumal R, Tenhunen O, Kónyi A, Simon M, Horváth IG, Kerkelä R, Ruskoaho H, Szokodi I. Apelin increases cardiac contractility via protein kinase Cε- and extracellular signal-regulated kinase-dependent mechanisms. PLoS One. 2014; 9:e93473. https://doi.org/10.1371/journal.pone.0093473 [PubMed]
- 130. Wang Q, Wang B, Zhang W, Zhang T, Liu Q, Jiao X, Ye J, Hao Y, Gao Q, Ma G, Hao C, Cui B. APLN promotes the proliferation, migration, and glycolysis of cervical cancer through the PI3K/AKT/mTOR pathway. Arch Biochem Biophys. 2024; 755:109983. https://doi.org/10.1016/j.abb.2024.109983 [PubMed]
- 131. Rostène W, De Meyts P. Insulin: A 100-Year-Old Discovery With a Fascinating History. Endocr Rev. 2021; 42:503–27. https://doi.org/10.1210/endrev/bnab020 [PubMed]
- 132. Merz KE, Thurmond DC. Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake. Compr Physiol. 2020; 10:785–809. https://doi.org/10.1002/cphy.c190029 [PubMed]
- 133. Sumitani S, Goya K, Testa JR, Kouhara H, Kasayama S. Akt1 and Akt2 differently regulate muscle creatine kinase and myogenin gene transcription in insulin-induced differentiation of C2C12 myoblasts. Endocrinology. 2002; 143:820–8. https://doi.org/10.1210/endo.143.3.8687 [PubMed]
- 134. Tureckova J, Wilson EM, Cappalonga JL, Rotwein P. Insulin-like growth factor-mediated muscle differentiation: collaboration between phosphatidylinositol 3-kinase-Akt-signaling pathways and myogenin. J Biol Chem. 2001; 276:39264–70. https://doi.org/10.1074/jbc.M104991200 [PubMed]
- 135. Froemke RC, Young LJ. Oxytocin, Neural Plasticity, and Social Behavior. Annu Rev Neurosci. 2021; 44:359–81. https://doi.org/10.1146/annurev-neuro-102320-102847 [PubMed]
- 136. Costa DM, Cruz-Filho JD, Vasconcelos AB, Gomes-Santos JV, Reis LC, de Lucca W
Jr , Camargo EA, Lauton-Santos S, Zanon NM, Kettelhut ÍD, Navegantes LC, Mecawi AS, Badauê-Passos DJr , Lustrino D. Oxytocin induces anti-catabolic and anabolic effects on protein metabolism in the female rat oxidative skeletal muscle. Life Sci. 2021; 279:119665. https://doi.org/10.1016/j.lfs.2021.119665 [PubMed] - 137. Lee ES, Uhm KO, Lee YM, Kwon J, Park SH, Soo KH. Oxytocin stimulates glucose uptake in skeletal muscle cells through the calcium-CaMKK-AMPK pathway. Regul Pept. 2008; 151:71–4. https://doi.org/10.1016/j.regpep.2008.05.001 [PubMed]
- 138. Santos TO, Cruz-Filho JD, Costa DM, Silva RP, Anjos-Santos HC, Santos JR, Reis LC, Kettelhut ÍD, Navegantes LC, Camargo EA, Lauton-Santos S, Badauê-Passos D
Jr , Mecawi AS, Lustrino D. Non-canonical Ca2+- Akt signaling pathway mediates the antiproteolytic effects induced by oxytocin receptor stimulation in skeletal muscle. Biochem Pharmacol. 2023; 217:115850. https://doi.org/10.1016/j.bcp.2023.115850 [PubMed] - 139. Conte E, Romano A, De Bellis M, de Ceglia M, Rosaria Carratù M, Gaetani S, Maqoud F, Tricarico D, Camerino C. Oxtr/TRPV1 expression and acclimation of skeletal muscle to cold-stress in male mice. J Endocrinol. 2021; 249:135–48. https://doi.org/10.1530/JOE-20-0346 [PubMed]
- 140. O’Harte FP, Parthsarathy V, Hogg C, Flatt PR. Apelin-13 analogues show potent in vitro and in vivo insulinotropic and glucose lowering actions. Peptides. 2018; 100:219–28. https://doi.org/10.1016/j.peptides.2017.12.004 [PubMed]
- 141. Kido K, Egawa T, Watanabe S, Kawanaka K, Treebak JT, Hayashi T. Fasting potentiates insulin-mediated glucose uptake in rested and prior-contracted rat skeletal muscle. Am J Physiol Endocrinol Metab. 2022; 322:E425–35. https://doi.org/10.1152/ajpendo.00412.2021 [PubMed]
- 142. Shrestha MM, Lim CY, Bi X, Robinson RC, Han W. Tmod3 Phosphorylation Mediates AMPK-Dependent GLUT4 Plasma Membrane Insertion in Myoblasts. Front Endocrinol (Lausanne). 2021; 12:653557. https://doi.org/10.3389/fendo.2021.653557 [PubMed]
- 143. Boucher J, Masri B, Daviaud D, Gesta S, Guigné C, Mazzucotelli A, Castan-Laurell I, Tack I, Knibiehler B, Carpéné C, Audigier Y, Saulnier-Blache JS, Valet P. Apelin, a newly identified adipokine up-regulated by insulin and obesity. Endocrinology. 2005; 146:1764–71. https://doi.org/10.1210/en.2004-1427 [PubMed]
- 144. Li E, Wang L, Wang D, Chi J, Lin Z, Smith GI, Klein S, Cohen P, Rosen ED. Control of lipolysis by a population of oxytocinergic sympathetic neurons. Nature. 2024; 625:175–80. https://doi.org/10.1038/s41586-023-06830-x [PubMed]
- 145. Deblon N, Veyrat-Durebex C, Bourgoin L, Caillon A, Bussier AL, Petrosino S, Piscitelli F, Legros JJ, Geenen V, Foti M, Wahli W, Di Marzo V, Rohner-Jeanrenaud F. Mechanisms of the anti-obesity effects of oxytocin in diet-induced obese rats. PLoS One. 2011; 6:e25565. https://doi.org/10.1371/journal.pone.0025565 [PubMed]
- 146. Hattori K, Shimizu M, Yamachi M, Tezuka K, Fukushima T, Yokota S, Okano T, Misaka S, Hidema S, Kanai K, Shimomura K, Maejima Y. Oxytocin modulates insulin and GLP-1 secretion in pancreatic islets. Aging (Albany NY). 2025; 17:1139–47. https://doi.org/10.18632/aging.206244 [PubMed]
- 147. Zhang B, Nakata M, Nakae J, Ogawa W, Yada T. Central insulin action induces activation of paraventricular oxytocin neurons to release oxytocin into circulation. Sci Rep. 2018; 8:10415. https://doi.org/10.1038/s41598-018-28816-w [PubMed]
- 148. Ding C, Leow MK, Magkos F. Oxytocin in metabolic homeostasis: implications for obesity and diabetes management. Obes Rev. 2019; 20:22–40. https://doi.org/10.1111/obr.12757 [PubMed]
- 149. Yuan J, Zhang R, Wu R, Gu Y, Lu Y. The effects of oxytocin to rectify metabolic dysfunction in obese mice are associated with increased thermogenesis. Mol Cell Endocrinol. 2020; 514:110903. https://doi.org/10.1016/j.mce.2020.110903 [PubMed]
- 150. McConn BR, Koskinen A, Denbow DM, Gilbert ER, Siegel PB, Cline MA. Central injection of oxytocin reduces food intake and affects hypothalamic and adipose tissue gene expression in chickens. Domest Anim Endocrinol. 2019; 67:11–20. https://doi.org/10.1016/j.domaniend.2018.10.005 [PubMed]
- 151. Reaux-Le Goazigo A, Morinville A, Burlet A, Llorens-Cortes C, Beaudet A. Dehydration-induced cross-regulation of apelin and vasopressin immunoreactivity levels in magnocellular hypothalamic neurons. Endocrinology. 2004; 145:4392–400. https://doi.org/10.1210/en.2004-0384 [PubMed]
- 152. Patisaul HB, Scordalakes EM, Young LJ, Rissman EF. Oxytocin, but not oxytocin receptor, is rRegulated by oestrogen receptor beta in the female mouse hypothalamus. J Neuroendocrinol. 2003; 15:787–93. https://doi.org/10.1046/j.1365-2826.2003.01061.x [PubMed]
- 153. Bodineau L, Taveau C, Lê Quan Sang HH, Osterstock G, Queguiner I, Moos F, Frugière A, Llorens-Cortes C. Data supporting a new physiological role for brain apelin in the regulation of hypothalamic oxytocin neurons in lactating rats. Endocrinology. 2011; 152:3492–503. https://doi.org/10.1210/en.2011-0206 [PubMed]
- 154. Tobin VA, Bull PM, Arunachalam S, O’Carroll AM, Ueta Y, Ludwig M. The effects of apelin on the electrical activity of hypothalamic magnocellular vasopressin and oxytocin neurons and somatodendritic Peptide release. Endocrinology. 2008; 149:6136–45. https://doi.org/10.1210/en.2008-0178 [PubMed]
- 155. De Mota N, Reaux-Le Goazigo A, El Messari S, Chartrel N, Roesch D, Dujardin C, Kordon C, Vaudry H, Moos F, Llorens-Cortes C. Apelin, a potent diuretic neuropeptide counteracting vasopressin actions through inhibition of vasopressin neuron activity and vasopressin release. Proc Natl Acad Sci USA. 2004; 101:10464–9. https://doi.org/10.1073/pnas.0403518101 [PubMed]
- 156. Girault-Sotias PE, Gerbier R, Flahault A, de Mota N, Llorens-Cortes C. Apelin and Vasopressin: The Yin and Yang of Water Balance. Front Endocrinol (Lausanne). 2021; 12:735515. https://doi.org/10.3389/fendo.2021.735515 [PubMed]
- 157. Anima B, Gurusubramanian G, Roy VK. Expression of Apelin and Apelin Receptor Protein in the Hypothalamo-Pituitary-Ovarian Axis during the Estrous Cycle of Mice. Neuroendocrinology. 2024; 114:234–49. https://doi.org/10.1159/000534838 [PubMed]
- 158. Kurowska P, Barbe A, Różycka M, Chmielińska J, Dupont J, Rak A. Apelin in Reproductive Physiology and Pathology of Different Species: A Critical Review. Int J Endocrinol. 2018; 2018:9170480. https://doi.org/10.1155/2018/9170480 [PubMed]
- 159. Anima B, Gurusubramanian G, Roy VK. Hormonal dependent expression of apelin and apelin receptor in the ovary and uterus of mice. Reprod Biol. 2024; 24:100918. https://doi.org/10.1016/j.repbio.2024.100918 [PubMed]
- 160. Castan-Laurell I, El Boustany R, Pereira O, Potier L, Marre M, Fumeron F, Valet P, Gourdy P, Velho G, Roussel R. Plasma Apelin and Risk of Type 2 Diabetes in a Cohort From the Community. Diabetes Care. 2020; 43:e15–6. https://doi.org/10.2337/dc19-1865 [PubMed]
- 161. Hoffmann M, Gogola J, Ptak A. Apelin abrogates the stimulatory effects of 17β-estradiol and insulin-like growth factor-1 on proliferation of epithelial and granulosa ovarian cancer cell lines via crosstalk between APLNR and ERα/IGF1R. Mol Biol Rep. 2019; 46:6325–38. https://doi.org/10.1007/s11033-019-05073-2 [PubMed]
- 162. Schüler-Toprak S, Weber F, Skrzypczak M, Ortmann O, Treeck O. Expression of estrogen-related receptors in ovarian cancer and impact on survival. J Cancer Res Clin Oncol. 2021; 147:2555–67. https://doi.org/10.1007/s00432-021-03673-9 [PubMed]
- 163. Zaki M, Kamal S, Ezzat W, Hassan N, Yousef W, Ryad H, Mohamed R, Youness E, Basha W, Elhosary Y. Serum apelin levels and metabolic risk markers in obese women. J Genet Eng Biotechnol. 2017; 15:423–9. https://doi.org/10.1016/j.jgeb.2017.05.002 [PubMed]
- 164. Gao Y, Xin C, Fan H, Sun X, Wang H. Circulating apelin and chemerin levels in patients with polycystic ovary syndrome: A meta-analysis. Front Endocrinol (Lausanne). 2023; 13:1076951. https://doi.org/10.3389/fendo.2022.1076951 [PubMed]
- 165. Roche J, Ramé C, Reverchon M, Mellouk N, Cornuau M, Guerif F, Froment P, Dupont J. Apelin (APLN) and Apelin Receptor (APLNR) in Human Ovary: Expression, Signaling, and Regulation of Steroidogenesis in Primary Human Luteinized Granulosa Cells. Biol Reprod. 2016; 95:104. https://doi.org/10.1095/biolreprod.116.141754 [PubMed]
- 166. Kim YS, Song HK, Suh SW. Crystallization and preliminary X-ray analysis of a complex between the Bowman-Birk trypsin inhibitor from barley and porcine pancreatic trypsin. Acta Crystallogr D Biol Crystallogr. 1999; 55:1244–6. https://doi.org/10.1107/s0907444999005065 [PubMed]
- 167. Motlani V, Motlani G, Pamnani S, Sahu A, Acharya N. Endocrine Changes in Postmenopausal Women: A Comprehensive View. Cureus. 2023; 15:e51287. https://doi.org/10.7759/cureus.51287 [PubMed]
- 168. Jang SH, Paik IY, Ryu JH, Lee TH, Kim DE. Effects of aerobic and resistance exercises on circulating apelin-12 and apelin-36 concentrations in obese middle-aged women: a randomized controlled trial. BMC Womens Health. 2019; 19:23. https://doi.org/10.1186/s12905-019-0722-5 [PubMed]
- 169. Rai R, Ghosh AK, Eren M, Mackie AR, Levine DC, Kim SY, Cedernaes J, Ramirez V, Procissi D, Smith LH, Woodruff TK, Bass J, Vaughan DE. Downregulation of the Apelinergic Axis Accelerates Aging, whereas Its Systemic Restoration Improves the Mammalian Healthspan. Cell Rep. 2017; 21:1471–80. https://doi.org/10.1016/j.celrep.2017.10.057 [PubMed]
- 170. Collins BC, Laakkonen EK, Lowe DA. Aging of the musculoskeletal system: How the loss of estrogen impacts muscle strength. Bone. 2019; 123:137–44. https://doi.org/10.1016/j.bone.2019.03.033 [PubMed]
- 171. Song K, Jing T, Yang X, Xia J, Wang Z, Luo F, Qiu C, Liu Z, Zhao XY, Wang G, Ou X. Mechanistic insights into targeting APLN/APJ for ameliorating testosterone deficiency and reproductive disorders in diabetic mice. Cell Commun Signal. 2025; 23:469. https://doi.org/10.1186/s12964-025-02474-8 [PubMed]
- 172. Song K, Yang X, An G, Xia X, Zhao J, Xu X, Wan C, Liu T, Zheng Y, Ren S, Wang M, Chang G, Cronin SJ, et al. Targeting APLN/APJ restores blood-testis barrier and improves spermatogenesis in murine and human diabetic models. Nat Commun. 2022; 13:7335. https://doi.org/10.1038/s41467-022-34990-3 [PubMed]
- 173. Sandal S, Tekin S, Seker FB, Beytur A, Vardi N, Colak C, Tapan T, Yildiz S, Yilmaz B. The effects of intracerebroventricular infusion of apelin-13 on reproductive function in male rats. Neurosci Lett. 2015; 602:133–8. https://doi.org/10.1016/j.neulet.2015.06.059 [PubMed]
- 174. Das M, Gurusubramanian G, Roy VK. Apelin receptor antagonist (ML221) treatment has a stimulatory effect on the testicular proliferation, antioxidants system and steroidogenesis in adult mice. Neuropeptides. 2023; 101:102354. https://doi.org/10.1016/j.npep.2023.102354 [PubMed]
- 175. Tao Z, Cheng Z. Hormonal regulation of metabolism-recent lessons learned from insulin and estrogen. Clin Sci (Lond). 2023; 137:415–34. https://doi.org/10.1042/CS20210519 [PubMed]
- 176. Gregorio KC, Laurindo CP, Machado UF. Estrogen and Glycemic Homeostasis: The Fundamental Role of Nuclear Estrogen Receptors ESR1/ESR2 in Glucose Transporter GLUT4 Regulation. Cells. 2021; 10:99. https://doi.org/10.3390/cells10010099 [PubMed]
- 177. Jiang Q, Li W, Zhu X, Yu L, Lu Z, Liu Y, Ma B, Cheng L. Estrogen receptor β alleviates inflammatory lesions in a rat model of inflammatory bowel disease via down-regulating P2X7R expression in macrophages. Int J Biochem Cell Biol. 2021; 139:106068. https://doi.org/10.1016/j.biocel.2021.106068 [PubMed]
- 178. Zhou Z, Moore TM, Drew BG, Ribas V, Wanagat J, Civelek M, Segawa M, Wolf DM, Norheim F, Seldin MM, Strumwasser AR, Whitney KA, Lester E, et al. Estrogen receptor α controls metabolism in white and brown adipocytes by regulating Polg1 and mitochondrial remodeling. Sci Transl Med. 2020; 12:eaax8096. https://doi.org/10.1126/scitranslmed.aax8096 [PubMed]
- 179. Gupte AA, Pownall HJ, Hamilton DJ. Estrogen: an emerging regulator of insulin action and mitochondrial function. J Diabetes Res. 2015; 2015:916585. https://doi.org/10.1155/2015/916585 [PubMed]
- 180. Allemand MC, Irving BA, Asmann YW, Klaus KA, Tatpati L, Coddington CC, Nair KS. Effect of testosterone on insulin stimulated IRS1 Ser phosphorylation in primary rat myotubes--a potential model for PCOS-related insulin resistance. PLoS One. 2009; 4:e4274. https://doi.org/10.1371/journal.pone.0004274 [PubMed]
- 181. Martínez Báez A, Ayala G, Pedroza-Saavedra A, González-Sánchez HM, Chihu Amparan L. Phosphorylation Codes in IRS-1 and IRS-2 Are Associated with the Activation/Inhibition of Insulin Canonical Signaling Pathways. Curr Issues Mol Biol. 2024; 46:634–49. https://doi.org/10.3390/cimb46010041 [PubMed]
- 182. Kelly DM, Jones TH. Testosterone: a metabolic hormone in health and disease. J Endocrinol. 2013; 217:R25–45. https://doi.org/10.1530/JOE-12-0455 [PubMed]
- 183. Antinozzi C, Marampon F, Corinaldesi C, Vicini E, Sgrò P, Vannelli GB, Lenzi A, Crescioli C, Di Luigi L. Testosterone insulin-like effects: an in vitro study on the short-term metabolic effects of testosterone in human skeletal muscle cells. J Endocrinol Invest. 2017; 40:1133–43. https://doi.org/10.1007/s40618-017-0686-y [PubMed]
- 184. Pitteloud N, Mootha VK, Dwyer AA, Hardin M, Lee H, Eriksson KF, Tripathy D, Yialamas M, Groop L, Elahi D, Hayes FJ. Relationship between testosterone levels, insulin sensitivity, and mitochondrial function in men. Diabetes Care. 2005; 28:1636–42. https://doi.org/10.2337/diacare.28.7.1636 [PubMed]
- 185. Kapoor D, Goodwin E, Channer KS, Jones TH. Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes. Eur J Endocrinol. 2006; 154:899–906. https://doi.org/10.1530/eje.1.02166 [PubMed]
- 186. Grossmann M, Thomas MC, Panagiotopoulos S, Sharpe K, Macisaac RJ, Clarke S, Zajac JD, Jerums G. Low testosterone levels are common and associated with insulin resistance in men with diabetes. J Clin Endocrinol Metab. 2008; 93:1834–40. https://doi.org/10.1210/jc.2007-2177 [PubMed]
- 187. Kato S, Endoh H, Masuhiro Y, Kitamoto T, Uchiyama S, Sasaki H, Masushige S, Gotoh Y, Nishida E, Kawashima H, Metzger D, Chambon P. Activation of the estrogen receptor through phosphorylation by mitogen-activated protein kinase. Science. 1995; 270:1491–4. https://doi.org/10.1126/science.270.5241.1491 [PubMed]
- 188. Campbell RA, Bhat-Nakshatri P, Patel NM, Constantinidou D, Ali S, Nakshatri H. Phosphatidylinositol 3-kinase/AKT-mediated activation of estrogen receptor alpha: a new model for anti-estrogen resistance. J Biol Chem. 2001; 276:9817–24. https://doi.org/10.1074/jbc.M010840200 [PubMed]
- 189. Pollard KJ, Daniel JM. Nuclear estrogen receptor activation by insulin-like growth factor-1 in Neuro-2A neuroblastoma cells requires endogenous estrogen synthesis and is mediated by mutually repressive MAPK and PI3K cascades. Mol Cell Endocrinol. 2019; 490:68–79. https://doi.org/10.1016/j.mce.2019.04.007 [PubMed]
- 190. Fan W, Yanase T, Morinaga H, Okabe T, Nomura M, Daitoku H, Fukamizu A, Kato S, Takayanagi R, Nawata H. Insulin-like growth factor 1/insulin signaling activates androgen signaling through direct interactions of Foxo1 with androgen receptor. J Biol Chem. 2007; 282:7329–38. https://doi.org/10.1074/jbc.M610447200 [PubMed]
- 191. Xu W, Qadir MM, Nasteska D, Mota de Sa P, Gorvin CM, Blandino-Rosano M, Evans CR, Ho T, Potapenko E, Veluthakal R, Ashford FB, Bitsi S, Fan J, et al. Architecture of androgen receptor pathways amplifying glucagon-like peptide-1 insulinotropic action in male pancreatic β cells. Cell Rep. 2023; 42:112529. https://doi.org/10.1016/j.celrep.2023.112529 [PubMed]
- 192. Silva RS, Mattoso Miskulin Cardoso AP, Giometti IC, D’Aprile L, Garcia Santos FA, Maruyama AS, Medeiros de Carvalho Sousa LM, Unniappan S, Kowalewski MP, de Carvalho Papa P. Insulin induces steroidogenesis in canine luteal cells via PI3K-MEK-MAPK. Mol Cell Endocrinol. 2022; 540:111518. https://doi.org/10.1016/j.mce.2021.111518 [PubMed]
- 193. Sacchi S, Marinaro F, Tondelli D, Lui J, Xella S, Marsella T, Tagliasacchi D, Argento C, Tirelli A, Giulini S, La Marca A. Modulation of gonadotrophin induced steroidogenic enzymes in granulosa cells by d-chiroinositol. Reprod Biol Endocrinol. 2016; 14:52. https://doi.org/10.1186/s12958-016-0189-2 [PubMed]
- 194. Nicolaisen TS, Sjøberg KA, Carl CS, Richter EA, Kiens B, Fritzen AM, Lundsgaard AM. Greater molecular potential for glucose metabolism in adipose tissue and skeletal muscle of women compared with men. FASEB J. 2024; 38:e23845. https://doi.org/10.1096/fj.202302377R [PubMed]
- 195. Engelhardt LJ, Grunow JJ, Wollersheim T, Carbon NM, Balzer F, Spranger J, Weber-Carstens S. Sex-Specific Aspects of Skeletal Muscle Metabolism in the Clinical Context of Intensive Care Unit-Acquired Weakness. J Clin Med. 2022; 11:846. https://doi.org/10.3390/jcm11030846 [PubMed] Erratum in: J Clin Med. 2022; 11:5496. DOI: 10.3390/jcm11195496 PMID:36233843.
- 196. Gado M, Tsaousidou E, Bornstein SR, Perakakis N. Sex-based differences in insulin resistance. J Endocrinol. 2024; 261:e230245. https://doi.org/10.1530/JOE-23-0245 [PubMed]
- 197. Mandrup CM, Egelund J, Nyberg M, Enevoldsen LH, Kjær A, Clemmensen AE, Christensen AN, Suetta C, Frikke-Schmidt R, Steenberg DE, Wojtaszewski JF, Hellsten Y, Stallknecht BM. Effects of menopause and high-intensity training on insulin sensitivity and muscle metabolism. Menopause. 2018; 25:165–75. https://doi.org/10.1097/GME.0000000000000981 [PubMed]
- 198. Ribas V, Drew BG, Zhou Z, Phun J, Kalajian NY, Soleymani T, Daraei P, Widjaja K, Wanagat J, de Aguiar Vallim TQ, Fluitt AH, Bensinger S, Le T, et al. Skeletal muscle action of estrogen receptor α is critical for the maintenance of mitochondrial function and metabolic homeostasis in females. Sci Transl Med. 2016; 8:334ra54. https://doi.org/10.1126/scitranslmed.aad3815 [PubMed]
- 199. De Paoli M, Zakharia A, Werstuck GH. The Role of Estrogen in Insulin Resistance: A Review of Clinical and Preclinical Data. Am J Pathol. 2021; 191:1490–8. https://doi.org/10.1016/j.ajpath.2021.05.011 [PubMed]
- 200. Hingst JR, Onslev JD, Holm S, Kjøbsted R, Frøsig C, Kido K, Steenberg DE, Larsen MR, Kristensen JM, Carl CS, Sjøberg K, Thong FS, Derave W, et al. Insulin Sensitization Following a Single Exercise Bout Is Uncoupled to Glycogen in Human Skeletal Muscle: A Meta-analysis of 13 Single-Center Human Studies. Diabetes. 2022; 71:2237–50. https://doi.org/10.2337/db22-0015 [PubMed]
- 201. Glouzon BK, Barsalani R, Lagacé JC, Dionne IJ. Muscle mass and insulin sensitivity in postmenopausal women after 6-month exercise training. Climacteric. 2015; 18:846–51. https://doi.org/10.3109/13697137.2015.1083002 [PubMed]
- 202. Hyvärinen M, Juppi HK, Taskinen S, Karppinen JE, Karvinen S, Tammelin TH, Kovanen V, Aukee P, Kujala UM, Rantalainen T, Sipilä S, Laakkonen EK. Metabolic health, menopause, and physical activity-a 4-year follow-up study. Int J Obes (Lond). 2022; 46:544–54. https://doi.org/10.1038/s41366-021-01022-x [PubMed]
- 203. Wang X, Yang D, Li J, Jin L, Xia S, Jin F. Association between menopause-related symptoms and muscle mass index among perimenopausal and postmenopausal women and the mediating role of estrogen levels. Front Endocrinol (Lausanne). 2025; 16:1628612. https://doi.org/10.3389/fendo.2025.1628612 [PubMed]
- 204. Dandona P, Dhindsa S, Ghanim H, Saad F. Mechanisms underlying the metabolic actions of testosterone in humans: A narrative review. Diabetes Obes Metab. 2021; 23:18–28. https://doi.org/10.1111/dom.14206 [PubMed]
- 205. Bianchi VE, Locatelli V. Testosterone a key factor in gender related metabolic syndrome. Obes Rev. 2018; 19:557–75. https://doi.org/10.1111/obr.12633 [PubMed]
- 206. Ottarsdottir K, Nilsson AG, Hellgren M, Lindblad U, Daka B. The association between serum testosterone and insulin resistance: a longitudinal study. Endocr Connect. 2018; 7:1491–500. https://doi.org/10.1530/EC-18-0480 [PubMed]
- 207. Yeap BB, Chubb SA, Hyde Z, Jamrozik K, Hankey GJ, Flicker L, Norman PE. Lower serum testosterone is independently associated with insulin resistance in non-diabetic older men: the Health In Men Study. Eur J Endocrinol. 2009; 161:591–8. https://doi.org/10.1530/EJE-09-0348 [PubMed]
- 208. Zitzmann M. Testosterone deficiency, insulin resistance and the metabolic syndrome. Nat Rev Endocrinol. 2009; 5:673–81. https://doi.org/10.1038/nrendo.2009.212 [PubMed]
- 209. Cleasby ME, Jamieson PM, Atherton PJ. Insulin resistance and sarcopenia: mechanistic links between common co-morbidities. J Endocrinol. 2016; 229:R67–81. https://doi.org/10.1530/JOE-15-0533 [PubMed]
- 210. Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: findings from the National Health and Nutrition Examination Survey III. PLoS One. 2010; 5:e10805. https://doi.org/10.1371/journal.pone.0010805 [PubMed]
- 211. Pedauyé-Rueda B, García-Fernández P, Maicas-Pérez L, Maté-Muñoz JL, Hernández-Lougedo J. Different Diagnostic Criteria for Determining the Prevalence of Sarcopenia in Older Adults: A Systematic Review. J Clin Med. 2024; 13:2520. https://doi.org/10.3390/jcm13092520 [PubMed]
- 212. Gentile G, De Stefano F, Sorrentino C, D’Angiolo R, Lauretta C, Giovannelli P, Migliaccio A, Castoria G, Di Donato M. Androgens as the “old age stick” in skeletal muscle. Cell Commun Signal. 2025; 23:167. https://doi.org/10.1186/s12964-025-02163-6 [PubMed] Erratum in: Cell Commun Signal. 2025; 23:225. DOI: 10.1186/s12964-025-02234-8 PMID:40375106.
- 213. de Jong JC, Attema BJ, van der Hoek MD, Verschuren L, Caspers MP, Kleemann R, van der Leij FR, van den Hoek AM, Nieuwenhuizen AG, Keijer J. Sex differences in skeletal muscle-aging trajectory: same processes, but with a different ranking. Geroscience. 2023; 45:2367–86. https://doi.org/10.1007/s11357-023-00750-4 [PubMed]
- 214. Velders M, Diel P. How sex hormones promote skeletal muscle regeneration. Sports Med. 2013; 43:1089–100. https://doi.org/10.1007/s40279-013-0081-6 [PubMed]
- 215. Nomura M, McKenna E, Korach KS, Pfaff DW, Ogawa S. Estrogen receptor-beta regulates transcript levels for oxytocin and arginine vasopressin in the hypothalamic paraventricular nucleus of male mice. Brain Res Mol Brain Res. 2002; 109:84–94. https://doi.org/10.1016/s0169-328x(02)00525-9 [PubMed]
- 216. Acevedo-Rodriguez A, Mani SK, Handa RJ. Oxytocin and Estrogen Receptor β in the Brain: An Overview. Front Endocrinol (Lausanne). 2015; 6:160. https://doi.org/10.3389/fendo.2015.00160 [PubMed]
- 217. Amico JA, Seif SM, Robinson AG. Elevation of oxytocin and the oxytocin-associated neurophysin in the plasma of normal women during midcycle. J Clin Endocrinol Metab. 1981; 53:1229–32. https://doi.org/10.1210/jcem-53-6-1229 [PubMed]
- 218. Engel S, Klusmann H, Ditzen B, Knaevelsrud C, Schumacher S. Menstrual cycle-related fluctuations in oxytocin concentrations: A systematic review and meta-analysis. Front Neuroendocrinol. 2019; 52:144–55. https://doi.org/10.1016/j.yfrne.2018.11.002 [PubMed]
- 219. Hiroi R, Lacagnina AF, Hinds LR, Carbone DG, Uht RM, Handa RJ. The androgen metabolite, 5α-androstane-3β,17β-diol (3β-diol), activates the oxytocin promoter through an estrogen receptor-β pathway. Endocrinology. 2013; 154:1802–12. https://doi.org/10.1210/en.2012-2253 [PubMed]
- 220. Dai D, Li QC, Zhu QB, Hu SH, Balesar R, Swaab D, Bao AM. Direct Involvement of Androgen Receptor in Oxytocin Gene Expression: Possible Relevance for Mood Disorders. Neuropsychopharmacology. 2017; 42:2064–71. https://doi.org/10.1038/npp.2017.76 [PubMed]
- 221. Filippi S, Luconi M, Granchi S, Vignozzi L, Bettuzzi S, Tozzi P, Ledda F, Forti G, Maggi M. Estrogens, but not androgens, regulate expression and functional activity of oxytocin receptor in rabbit epididymis. Endocrinology. 2002; 143:4271–80. https://doi.org/10.1210/en.2002-220384 [PubMed]
- 222. Tribollet E, Audigier S, Dubois-Dauphin M, Dreifuss JJ. Gonadal steroids regulate oxytocin receptors but not vasopressin receptors in the brain of male and female rats. An autoradiographical study. Brain Res. 1990; 511:129–40. https://doi.org/10.1016/0006-8993(90)90232-z [PubMed]
- 223. Vignozzi L, Filippi S, Luconi M, Morelli A, Mancina R, Marini M, Vannelli GB, Granchi S, Orlando C, Gelmini S, Ledda F, Forti G, Maggi M. Oxytocin receptor is expressed in the penis and mediates an estrogen-dependent smooth muscle contractility. Endocrinology. 2004; 145:1823–34. https://doi.org/10.1210/en.2003-0962 [PubMed]
- 224. Bishop CV. Progesterone inhibition of oxytocin signaling in endometrium. Front Neurosci. 2013; 7:138. https://doi.org/10.3389/fnins.2013.00138 [PubMed]
- 225. Krishnaswamy N, Danyod G, Chapdelaine P, Fortier MA. Oxytocin receptor down-regulation is not necessary for reducing oxytocin-induced prostaglandin F(2alpha) accumulation by interferon-tau in a bovine endometrial epithelial cell line. Endocrinology. 2009; 150:897–905. https://doi.org/10.1210/en.2008-0704 [PubMed]
- 226. Yamamoto K, Nakano Y, Iwata N, Soejima Y, Suyama A, Hasegawa T, Otsuka F. Oxytocin enhances progesterone production with upregulation of BMP-15 activity by granulosa cells. Biochem Biophys Res Commun. 2023; 646:103–9. https://doi.org/10.1016/j.bbrc.2023.01.073 [PubMed]
- 227. Assinder SJ, Johnson C, King K, Nicholson HD. Regulation of 5alpha-reductase isoforms by oxytocin in the rat ventral prostate. Endocrinology. 2004; 145:5767–73. https://doi.org/10.1210/en.2004-0711 [PubMed]
- 228. Windle RJ, Kershaw YM, Shanks N, Wood SA, Lightman SL, Ingram CD. Oxytocin attenuates stress-induced c-fos mRNA expression in specific forebrain regions associated with modulation of hypothalamo-pituitary-adrenal activity. J Neurosci. 2004; 24:2974–82. https://doi.org/10.1523/JNEUROSCI.3432-03.2004 [PubMed]
- 229. Neumann ID, Wigger A, Torner L, Holsboer F, Landgraf R. Brain oxytocin inhibits basal and stress-induced activity of the hypothalamo-pituitary-adrenal axis in male and female rats: partial action within the paraventricular nucleus. J Neuroendocrinol. 2000; 12:235–43. https://doi.org/10.1046/j.1365-2826.2000.00442.x [PubMed]
- 230. Mehdi SF, Pusapati S, Khenhrani RR, Farooqi MS, Sarwar S, Alnasarat A, Mathur N, Metz CN, LeRoith D, Tracey KJ, Yang H, Brownstein MJ, Roth J. Oxytocin and Related Peptide Hormones: Candidate Anti-Inflammatory Therapy in Early Stages of Sepsis. Front Immunol. 2022; 13:864007. https://doi.org/10.3389/fimmu.2022.864007 [PubMed]
- 231. Carter CS, Kenkel WM, MacLean EL, Wilson SR, Perkeybile AM, Yee JR, Ferris CF, Nazarloo HP, Porges SW, Davis JM, Connelly JJ, Kingsbury MA. Is Oxytocin “Nature’s Medicine”? Pharmacol Rev. 2020; 72:829–61. https://doi.org/10.1124/pr.120.019398 [PubMed]
- 232. Oxfeldt M, Dalgaard LB, Farup J, Hansen M. Sex Hormones and Satellite Cell Regulation in Women. Transl Sports Med. 2022; 2022:9065923. https://doi.org/10.1155/2022/9065923 [PubMed]
- 233. Devost D, Carrier ME, Zingg HH. Oxytocin-induced activation of eukaryotic elongation factor 2 in myometrial cells is mediated by protein kinase C. Endocrinology. 2008; 149:131–8. https://doi.org/10.1210/en.2007-0548 [PubMed]
- 234. Seko D, Fujita R, Kitajima Y, Nakamura K, Imai Y, Ono Y. Estrogen Receptor β Controls Muscle Growth and Regeneration in Young Female Mice. Stem Cell Reports. 2020; 15:577–86. https://doi.org/10.1016/j.stemcr.2020.07.017 [PubMed]
- 235. Willoughby DS, Florez C, Davis J, Keratsopoulos N, Bisher M, Parra M, Taylor L. Decreased Neuromuscular Function and Muscle Quality along with Increased Systemic Inflammation and Muscle Proteolysis Occurring in the Presence of Decreased Estradiol and Protein Intake in Early to Intermediate Post-Menopausal Women. Nutrients. 2024; 16:197. https://doi.org/10.3390/nu16020197 [PubMed]
- 236. Li DCW, Rudloff S, Langer HT, Norman K, Herpich C. Age-Associated Differences in Recovery from Exercise-Induced Muscle Damage. Cells. 2024; 13:255. https://doi.org/10.3390/cells13030255 [PubMed] Erratum in: Cells. 2025; 14:1564. DOI: 10.3390/cells14191564. PMID:41090801.
- 237. Du Y, Xu C, Shi H, Jiang X, Tang W, Wu X, Chen M, Li H, Zhang X, Cheng Q. Serum concentrations of oxytocin, DHEA and follistatin are associated with osteoporosis or sarcopenia in community-dwelling postmenopausal women. BMC Geriatr. 2021; 21:542. https://doi.org/10.1186/s12877-021-02481-7 [PubMed]
- 238. Enns DL, Tiidus PM. The influence of estrogen on skeletal muscle: sex matters. Sports Med. 2010; 40:41–58. https://doi.org/10.2165/11319760-000000000-00000 [PubMed]
- 239. Dieli-Conwright CM, Spektor TM, Rice JC, Sattler FR, Schroeder ET. Hormone therapy attenuates exercise-induced skeletal muscle damage in postmenopausal women. J Appl Physiol (1985). 2009; 107:853–8. https://doi.org/10.1152/japplphysiol.00404.2009 [PubMed]
- 240. Yamamoto S, Arakaki R, Noguchi H, Takeda A, Uchishiba M, Kamada S, Mineda A, Kon M, Kawakita T, Kinouchi R, Yamamoto Y, Yoshida K, Shinohara N, Iwasa T. New discoveries on the interaction between testosterone and oxytocin in male rats - Testosterone-mediated effects of oxytocin in the prevention of obesity. Physiol Behav. 2023; 266:114199. https://doi.org/10.1016/j.physbeh.2023.114199 [PubMed]
- 241. Zhang Z, Zhao LD, Johnson SE, Rhoads ML, Jiang H, Rhoads RP. Oxytocin is involved in steroid hormone-stimulated bovine satellite cell proliferation and differentiation in vitro. Domest Anim Endocrinol. 2019; 66:1–13. https://doi.org/10.1016/j.domaniend.2018.07.003 [PubMed]
- 242. Horwath O, Apró W, Moberg M, Godhe M, Helge T, Ekblom M, Hirschberg AL, Ekblom B. Fiber type-specific hypertrophy and increased capillarization in skeletal muscle following testosterone administration in young women. J Appl Physiol (1985). 2020; 128:1240–50. https://doi.org/10.1152/japplphysiol.00893.2019 [PubMed]
- 243. Guilherme JP, Semenova EA, Borisov OV, Larin AK, Moreland E, Generozov EV, Ahmetov II. Genomic predictors of testosterone levels are associated with muscle fiber size and strength. Eur J Appl Physiol. 2022; 122:415–23. https://doi.org/10.1007/s00421-021-04851-w [PubMed]
- 244. Hevener AL, Zhou Z, Moore TM, Drew BG, Ribas V. The impact of ERα action on muscle metabolism and insulin sensitivity - Strong enough for a man, made for a woman. Mol Metab. 2018; 15:20–34. https://doi.org/10.1016/j.molmet.2018.06.013 [PubMed]
- 245. Oura M, Son BK, Song Z, Toyoshima K, Nanao-Hamai M, Ogawa S, Akishita M. Testosterone/androgen receptor antagonizes immobility-induced muscle atrophy through Inhibition of myostatin transcription and inflammation in mice. Sci Rep. 2025; 15:10568. https://doi.org/10.1038/s41598-025-95115-6 [PubMed]
- 246. Shigehara K, Kato Y, Izumi K, Mizokami A. Relationship between Testosterone and Sarcopenia in Older-Adult Men: A Narrative Review. J Clin Med. 2022; 11:6202. https://doi.org/10.3390/jcm11206202 [PubMed]
- 247. Ziaeian B, Fonarow GC. Statins and the Prevention of Heart Disease. JAMA Cardiol. 2017; 2:464. https://doi.org/10.1001/jamacardio.2016.4320 [PubMed]
- 248. Hunt NB, Emmens JE, Irawati S, de Vos S, Bos JH, Wilffert B, Hak E, de Boer RA. Sex disparities in the effect of statins on lipid parameters: The PharmLines Initiative. Medicine (Baltimore). 2022; 101:e28394. https://doi.org/10.1097/MD.0000000000028394 [PubMed]
- 249. Cho EJ, Choi Y, Jung SJ, Kwak HB. Role of exercise in estrogen deficiency-induced sarcopenia. J Exerc Rehabil. 2022; 18:2–9. https://doi.org/10.12965/jer.2244004.002 [PubMed]
- 250. Skinner JW, Otzel DM, Bowser A, Nargi D, Agarwal S, Peterson MD, Zou B, Borst SE, Yarrow JF. Muscular responses to testosterone replacement vary by administration route: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2018; 9:465–81. https://doi.org/10.1002/jcsm.12291 [PubMed]
- 251. Almeida M, Laurent MR, Dubois V, Claessens F, O’Brien CA, Bouillon R, Vanderschueren D, Manolagas SC. Estrogens and Androgens in Skeletal Physiology and Pathophysiology. Physiol Rev. 2017; 97:135–87. https://doi.org/10.1152/physrev.00033.2015 [PubMed]
- 252. McMillin SL, Minchew EC, Lowe DA, Spangenburg EE. Skeletal muscle wasting: the estrogen side of sexual dimorphism. Am J Physiol Cell Physiol. 2022; 322:C24–37. https://doi.org/10.1152/ajpcell.00333.2021 [PubMed]
- 253. Kilpiö T, Skarp S, Perjés Á, Swan J, Kaikkonen L, Saarimäki S, Szokodi I, Penninger JM, Szabó Z, Magga J, Kerkelä R. Apelin regulates skeletal muscle adaptation to exercise in a high-intensity interval training model. Am J Physiol Cell Physiol. 2024; 326:C1437–50. https://doi.org/10.1152/ajpcell.00427.2023 [PubMed]
- 254. Le Moal E, Liu Y, Collerette-Tremblay J, Dumontier S, Fabre P, Molina T, Dort J, Orfi Z, Denault N, Boutin J, Michaud J, Giguère H, Desroches A, et al. Apelin stimulation of the vascular skeletal muscle stem cell niche enhances endogenous repair in dystrophic mice. Sci Transl Med. 2024; 16:eabn8529. https://doi.org/10.1126/scitranslmed.abn8529 [PubMed]
- 255. Kedlian VR, Wang Y, Liu T, Chen X, Bolt L, Tudor C, Shen Z, Fasouli ES, Prigmore E, Kleshchevnikov V, Pett JP, Li T, Lawrence JE, et al. Human skeletal muscle aging atlas. Nat Aging. 2024; 4:727–44. https://doi.org/10.1038/s43587-024-00613-3 [PubMed]
- 256. Frier BC, Williams DB, Wright DC. The effects of apelin treatment on skeletal muscle mitochondrial content. Am J Physiol Regul Integr Comp Physiol. 2009; 297:R1761–8. https://doi.org/10.1152/ajpregu.00422.2009 [PubMed]
- 257. Wang X, Zhang L, Li P, Zheng Y, Yang Y, Ji S. Apelin/APJ system in inflammation. Int Immunopharmacol. 2022; 109:108822. https://doi.org/10.1016/j.intimp.2022.108822 [PubMed]
- 258. Chen YY, Chiu YL, Kao TW, Peng TC, Yang HF, Chen WL. Cross-sectional associations among P3NP, HtrA, Hsp70, Apelin and sarcopenia in Taiwanese population. BMC Geriatr. 2021; 21:192. https://doi.org/10.1186/s12877-021-02146-5 [PubMed]
- 259. Re Cecconi AD, Barone M, Forti M, Lunardi M, Cagnotto A, Salmona M, Olivari D, Zentilin L, Resovi A, Persichitti P, Belotti D, Palo F, Takakura N, et al. Apelin Resistance Contributes to Muscle Loss during Cancer Cachexia in Mice. Cancers (Basel). 2022; 14:1814. https://doi.org/10.3390/cancers14071814 [PubMed]
- 260. Dagdeviren S, Jung DY, Friedline RH, Noh HL, Kim JH, Patel PR, Tsitsilianos N, Inashima K, Tran DA, Hu X, Loubato MM, Craige SM, Kwon JY, et al. IL-10 prevents aging-associated inflammation and insulin resistance in skeletal muscle. FASEB J. 2017; 31:701–10. https://doi.org/10.1096/fj.201600832R [PubMed]
- 261. Shou J, Chen PJ, Xiao WH. Mechanism of increased risk of insulin resistance in aging skeletal muscle. Diabetol Metab Syndr. 2020; 12:14. https://doi.org/10.1186/s13098-020-0523-x [PubMed]
- 262. Abdulla H, Smith K, Atherton PJ, Idris I. Role of insulin in the regulation of human skeletal muscle protein synthesis and breakdown: a systematic review and meta-analysis. Diabetologia. 2016; 59:44–55. https://doi.org/10.1007/s00125-015-3751-0 [PubMed]
- 263. O’Neill BT, Lee KY, Klaus K, Softic S, Krumpoch MT, Fentz J, Stanford KI, Robinson MM, Cai W, Kleinridders A, Pereira RO, Hirshman MF, Abel ED, et al. Insulin and IGF-1 receptors regulate FoxO-mediated signaling in muscle proteostasis. J Clin Invest. 2016; 126:3433–46. https://doi.org/10.1172/JCI86522 [PubMed]
- 264. Stump CS, Short KR, Bigelow ML, Schimke JM, Nair KS. Effect of insulin on human skeletal muscle mitochondrial ATP production, protein synthesis, and mRNA transcripts. Proc Natl Acad Sci USA. 2003; 100:7996–8001. https://doi.org/10.1073/pnas.1332551100 [PubMed]
- 265. Bordt EA, Smith CJ, Demarest TG, Bilbo SD, Kingsbury MA. Mitochondria, Oxytocin, and Vasopressin: Unfolding the Inflammatory Protein Response. Neurotox Res. 2019; 36:239–56. https://doi.org/10.1007/s12640-018-9962-7 [PubMed]
- 266. Lawson EA. Understanding oxytocin in human physiology and pathophysiology: A path towards therapeutics. Compr Psychoneuroendocrinol. 2024; 19:100242. https://doi.org/10.1016/j.cpnec.2024.100242 [PubMed]
- 267. An X, Sun X, Hou Y, Yang X, Chen H, Zhang P, Wu J. Protective effect of oxytocin on LPS-induced acute lung injury in mice. Sci Rep. 2019; 9:2836. https://doi.org/10.1038/s41598-019-39349-1 [PubMed]
- 268. Friuli M, Eramo B, Valenza M, Scuderi C, Provensi G, Romano A. Targeting the Oxytocinergic System: A Possible Pharmacological Strategy for the Treatment of Inflammation Occurring in Different Chronic Diseases. Int J Mol Sci. 2021; 22:10250. https://doi.org/10.3390/ijms221910250 [PubMed]
- 269. Fraser HC, Kuan V, Johnen R, Zwierzyna M, Hingorani AD, Beyer A, Partridge L. Biological mechanisms of aging predict age-related disease co-occurrence in patients. Aging Cell. 2022; 21:e13524. https://doi.org/10.1111/acel.13524 [PubMed]
- 270. Schmeer C, Kretz A, Wengerodt D, Stojiljkovic M, Witte OW. Dissecting Aging and Senescence-Current Concepts and Open Lessons. Cells. 2019; 8:1446. https://doi.org/10.3390/cells8111446 [PubMed]
- 271. Sánchez-Rodríguez MA, Zacarías-Flores M, Correa-Muñoz E, Arronte-Rosales A, Mendoza-Núñez VM. Oxidative Stress Risk Is Increased with a Sedentary Lifestyle during Aging in Mexican Women. Oxid Med Cell Longev. 2021; 2021:9971765. https://doi.org/10.1155/2021/9971765 [PubMed]
- 272. El Assar M, Álvarez-Bustos A, Sosa P, Angulo J, Rodríguez-Mañas L. Effect of Physical Activity/Exercise on Oxidative Stress and Inflammation in Muscle and Vascular Aging. Int J Mol Sci. 2022; 23:8713. https://doi.org/10.3390/ijms23158713 [PubMed]
- 273. Pratt J, Boreham C, Ennis S, Ryan AW, De Vito G. Genetic Associations with Aging Muscle: A Systematic Review. Cells. 2019; 9:12. https://doi.org/10.3390/cells9010012 [PubMed]
- 274. Teraž K, Marusic U, Kalc M, Šimunič B, Pori P, Grassi B, Lazzer S, Narici MV, Blenkuš MG, di Prampero PE, Reggiani C, Passaro A, Biolo G, et al. Sarcopenia parameters in active older adults - an eight-year longitudinal study. BMC Public Health. 2023; 23:917. https://doi.org/10.1186/s12889-023-15734-4 [PubMed]
- 275. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. Hallmarks of aging: An expanding universe. Cell. 2023; 186:243–78. https://doi.org/10.1016/j.cell.2022.11.001 [PubMed]
- 276. Damanti S, Senini E, De Lorenzo R, Merolla A, Santoro S, Festorazzi C, Messina M, Vitali G, Sciorati C, Manfredi AA, Rovere-Querini P. Molecular constraints of sarcopenia in the ageing muscle. Front Aging. 2025; 6:1588014. https://doi.org/10.3389/fragi.2025.1588014 [PubMed]
- 277. Christian CJ, Benian GM. Animal models of sarcopenia. Aging Cell. 2020; 19:e13223. https://doi.org/10.1111/acel.13223 [PubMed]
- 278. Zhang P, Judy M, Lee SJ, Kenyon C. Direct and indirect gene regulation by a life-extending FOXO protein in C. elegans: roles for GATA factors and lipid gene regulators. Cell Metab. 2013; 17:85–100. https://doi.org/10.1016/j.cmet.2012.12.013 [PubMed]
- 279. Seo K, Choi E, Lee D, Jeong DE, Jang SK, Lee SJ. Heat shock factor 1 mediates the longevity conferred by inhibition of TOR and insulin/IGF-1 signaling pathways in C. elegans. Aging Cell. 2013; 12:1073–81. https://doi.org/10.1111/acel.12140 [PubMed]
- 280. Chechenova M, McLendon L, Dallas B, Stratton H, Kiani K, Gerberich E, Alekseyenko A, Tamba N, An S, Castillo L, Czajkowski E, Talley C, Brown A, Bryantsev AL. Muscle degeneration in aging Drosophila flies: the role of mechanical stress. Skelet Muscle. 2024; 14:20. https://doi.org/10.1186/s13395-024-00352-4 [PubMed]
- 281. Augustin H, Partridge L. Invertebrate models of age-related muscle degeneration. Biochim Biophys Acta. 2009; 1790:1084–94. https://doi.org/10.1016/j.bbagen.2009.06.011 [PubMed]
- 282. Chaturvedi D, Reichert H, Gunage RD, VijayRaghavan K. Identification and functional characterization of muscle satellite cells in Drosophila. Elife. 2017; 6:e30107. https://doi.org/10.7554/eLife.30107 [PubMed]
- 283. Aranda-Martínez P, Sayed RK, Fernández-Martínez J, Ramírez-Casas Y, Yang Y, Escames G, Acuña-Castroviejo D. Zebrafish as a Human Muscle Model for Studying Age-Dependent Sarcopenia and Frailty. Int J Mol Sci. 2024; 25:6166. https://doi.org/10.3390/ijms25116166 [PubMed]
- 284. Harel I, Benayoun BA, Machado B, Singh PP, Hu CK, Pech MF, Valenzano DR, Zhang E, Sharp SC, Artandi SE, Brunet A. A platform for rapid exploration of aging and diseases in a naturally short-lived vertebrate. Cell. 2015; 160:1013–26. https://doi.org/10.1016/j.cell.2015.01.038 [PubMed]
- 285. Ruparelia AA, Salavaty A, Barlow CK, Lu Y, Sonntag C, Hersey L, Eramo MJ, Krug J, Reuter H, Schittenhelm RB, Ramialison M, Cox A, Ryan MT, et al. The African killifish: A short-lived vertebrate model to study the biology of sarcopenia and longevity. Aging Cell. 2024; 23:e13862. https://doi.org/10.1111/acel.13862 [PubMed]
- 286. Terzibasi E, Lefrançois C, Domenici P, Hartmann N, Graf M, Cellerino A. Effects of dietary restriction on mortality and age-related phenotypes in the short-lived fish Nothobranchius furzeri. Aging Cell. 2009; 8:88–99. https://doi.org/10.1111/j.1474-9726.2009.00455.x [PubMed]
- 287. Astre G, Atlan T, Goshtchevsky U, Oron-Gottesman A, Smirnov M, Shapira K, Velan A, Deelen J, Levy T, Levanon EY, Harel I. Genetic perturbation of AMP biosynthesis extends lifespan and restores metabolic health in a naturally short-lived vertebrate. Dev Cell. 2023; 58:1350–64.e10. https://doi.org/10.1016/j.devcel.2023.05.015 [PubMed]
- 288. McKay A, Costa EK, Chen J, Hu CK, Chen X, Bedbrook CN, Khondker RC, Thielvoldt M, Priya Singh P, Wyss-Coray T, Brunet A. An automated feeding system for the African killifish reveals the impact of diet on lifespan and allows scalable assessment of associative learning. Elife. 2022; 11:e69008. https://doi.org/10.7554/eLife.69008 [PubMed]
- 289. Sandhi S, Somers H, Cox M, Nobrega C, Seaman R, Bakers E, Letchner O, Reeve R, Menard R, Godwin J, Paulmann A, Rogers A, Valenzano DR, et al. Sexually Dimorphic Response to Dietary Restriction-induced Longevity and Muscle Rejuvenation in Nothobranchius furzeri. bioRxiv. 2026: 2026.02.09.704879. https://doi.org/10.64898/2026.02.09.704879 [PubMed]
- 290. Börsch A, Ham DJ, Mittal N, Tintignac LA, Migliavacca E, Feige JN, Rüegg MA, Zavolan M. Molecular and phenotypic analysis of rodent models reveals conserved and species-specific modulators of human sarcopenia. Commun Biol. 2021; 4:194. https://doi.org/10.1038/s42003-021-01723-z [PubMed]
- 291. Owen AM, Fry CS. Decoding the decline: unveiling drivers of sarcopenia. J Clin Invest. 2024; 134:e183302. https://doi.org/10.1172/JCI183302 [PubMed]
- 292. Huang Y, Wu B, Shen D, Chen J, Yu Z, Chen C. Ferroptosis in a sarcopenia model of senescence accelerated mouse prone 8 (SAMP8). Int J Biol Sci. 2021; 17:151–62. https://doi.org/10.7150/ijbs.53126 [PubMed]
- 293. Bose C, Megyesi J, Karaduta O, Singh SP, Swaminathan S, Shah SV. Iron Chelation Prevents Age-Related Skeletal Muscle Sarcopenia in Klotho Gene Mutant Mice, a Genetic Model of Aging. J Cachexia Sarcopenia Muscle. 2025; 16:e13678. https://doi.org/10.1002/jcsm.13678 [PubMed]
- 294. Oyabu M, Sato T, Kawaguchi R, Yoshioka K, Ito N, Eguchi T, Gotoh H, Yoshizawa T, Ogawa Y, Ono Y, Miura S, Kamei Y. Multi-dimensional metabolomic remodeling under diverse muscle atrophic stimuli in vivo. Cell Rep. 2025; 44:116097. https://doi.org/10.1016/j.celrep.2025.116097 [PubMed]
- 295. George T, Velloso CP, Alsharidah M, Lazarus NR, Harridge SD. Sera from young and older humans equally sustain proliferation and differentiation of human myoblasts. Exp Gerontol. 2010; 45:875–81. https://doi.org/10.1016/j.exger.2010.07.006 [PubMed]
- 296. Rao L, Qian Y, Khodabukus A, Ribar T, Bursac N. Engineering human pluripotent stem cells into a functional skeletal muscle tissue. Nat Commun. 2018; 9:126. https://doi.org/10.1038/s41467-017-02636-4 [PubMed]
- 297. Maffioletti SM, Sarcar S, Henderson AB, Mannhardt I, Pinton L, Moyle LA, Steele-Stallard H, Cappellari O, Wells KE, Ferrari G, Mitchell JS, Tyzack GE, Kotiadis VN, et al. Three-Dimensional Human iPSC-Derived Artificial Skeletal Muscles Model Muscular Dystrophies and Enable Multilineage Tissue Engineering. Cell Rep. 2018; 23:899–908. https://doi.org/10.1016/j.celrep.2018.03.091 [PubMed]
- 298. Park S, Shin MK, Jeong DS, Yeo XY, Kim YJ, Muhammad J, Kim M, Gu S, Lee JE, Park Y, Lim SB, Mun JY, Jung S, et al. Human Pluripotent Stem Cell-Derived Skeletal Muscle Organoid Model of Aging-Induced Sarcopenia. J Cachexia Sarcopenia Muscle. 2025; 16:e70045. https://doi.org/10.1002/jcsm.70045 [PubMed]
- 299. Beccafico S, Riuzzi F, Puglielli C, Mancinelli R, Fulle S, Sorci G, Donato R. Human muscle satellite cells show age-related differential expression of S100B protein and RAGE. Age (Dordr). 2011; 33:523–41. https://doi.org/10.1007/s11357-010-9197-x [PubMed]
- 300. Soriano-Arroquia A, Gostage J, Xia Q, Bardell D, McCormick R, McCloskey E, Bellantuono I, Clegg P, McDonagh B, Goljanek-Whysall K. miR-24 and its target gene Prdx6 regulate viability and senescence of myogenic progenitors during aging. Aging Cell. 2021; 20:e13475. https://doi.org/10.1111/acel.13475 [PubMed]
- 301. Son YH, Kim WJ, Shin YJ, Lee SM, Lee B, Lee KP, Lee SH, Kim KJ, Kwon KS. Human primary myoblasts derived from paraspinal muscle reflect donor age as an experimental model of sarcopenia. Exp Gerontol. 2023; 181:112273. https://doi.org/10.1016/j.exger.2023.112273 [PubMed]
- 302. Davegårdh C, Hall Wedin E, Broholm C, Henriksen TI, Pedersen M, Pedersen BK, Scheele C, Ling C. Sex influences DNA methylation and gene expression in human skeletal muscle myoblasts and myotubes. Stem Cell Res Ther. 2019; 10:26. https://doi.org/10.1186/s13287-018-1118-4 [PubMed]
- 303. Kim B, Lee DI, Basisty N, Dai DF. Cellular Models of Aging and Senescence. Cells. 2025; 14:1278. https://doi.org/10.3390/cells14161278 [PubMed]
- 304. Strässler ET, Aalto-Setälä K, Kiamehr M, Landmesser U, Kränkel N. Age Is Relative-Impact of Donor Age on Induced Pluripotent Stem Cell-Derived Cell Functionality. Front Cardiovasc Med. 2018; 5:4. https://doi.org/10.3389/fcvm.2018.00004 [PubMed]
- 305. Alsharidah M, Lazarus NR, George TE, Agley CC, Velloso CP, Harridge SD. Primary human muscle precursor cells obtained from young and old donors produce similar proliferative, differentiation and senescent profiles in culture. Aging Cell. 2013; 12:333–44. https://doi.org/10.1111/acel.12051 [PubMed]
- 306. Mestre R, García N, Patiño T, Guix M, Fuentes J, Valerio-Santiago M, Almiñana N, Sánchez S. 3D-bioengineered model of human skeletal muscle tissue with phenotypic features of aging for drug testing purposes. Biofabrication. 2021; 13. https://doi.org/10.1088/1758-5090/ac165b [PubMed]
- 307. Winkle P, Goldsmith S, Koren MJ, Lepage S, Hellawell J, Trivedi A, Tsirtsonis K, Abbasi SA, Kaufman A, Troughton R, Voors A, Hulot JS, Donal E, et al. A First-in-Human Study of AMG 986, a Novel Apelin Receptor Agonist, in Healthy Subjects and Heart Failure Patients. Cardiovasc Drugs Ther. 2023; 37:743–55. https://doi.org/10.1007/s10557-022-07328-w [PubMed]
- 308. Gargalovic P, Wong P, Onorato J, Finlay H, Wang T, Yan M, Crain E, St-Onge S, Héroux M, Bouvier M, Xu C, Chen XQ, Generaux C, et al. In Vitro and In Vivo Evaluation of a Small-Molecule APJ (Apelin Receptor) Agonist, BMS-986224, as a Potential Treatment for Heart Failure. Circ Heart Fail. 2021; 14:e007351. https://doi.org/10.1161/CIRCHEARTFAILURE.120.007351 [PubMed]
- 309. Pi Z, Johnson JA, Meng W, Phillips M, Schumacher WA, Bostwick JS, Gargalovic PS, Onorato JM, Generaux CN, Wang T, He Y, Gordon DA, Wexler RR, Finlay HJ. Identification of 6-Hydroxypyrimidin-4(1 H)-one-3-carboxamides as Potent and Orally Active APJ Receptor Agonists. ACS Med Chem Lett. 2021; 12:1766–72. https://doi.org/10.1021/acsmedchemlett.1c00385 [PubMed]
- 310. Yang P, Read C, Kuc RE, Nyimanu D, Williams TL, Crosby A, Buonincontri G, Southwood M, Sawiak SJ, Glen RC, Morrell NW, Davenport AP, Maguire JJ. A novel cyclic biased agonist of the apelin receptor, MM07, is disease modifying in the rat monocrotaline model of pulmonary arterial hypertension. Br J Pharmacol. 2019; 176:1206–21. https://doi.org/10.1111/bph.14603 [PubMed]
- 311. Wang WW, Ji SY, Zhang W, Zhang J, Cai C, Hu R, Zang SK, Miao L, Xu H, Chen LN, Yang Z, Guo J, Qin J, et al. Structure-based design of non-hypertrophic apelin receptor modulator. Cell. 2024; 187:1460–75.e20. https://doi.org/10.1016/j.cell.2024.02.004 [PubMed]