




Italian population contraction is accelerating, with births falling to approximately 370,000 in 2023, marking a record low, and deaths exceeding 660,000, raising the proportion of adults aged ≥65 years to 24.1%, the highest in the EU [1]. By 2050, the projected median age is 51 years, with over 6 million residents aged ≥80 years. Still, while aging is associated with progressive health deterioration, individuals follow heterogeneous aging trajectories: some experience early accumulation of deficits and multimorbidity, whereas others maintain functional capacity well into advanced age. Thus, the life expectancy indicator (LE; life expectancy at birth, regardless of health status) is insufficient. Policymakers and stakeholders should consider the healthspan, shifting attention toward extending years lived in good health [2]. Because healthspan is defined inconsistently across the literature, in this paper the term is used to refer to the portion of life lived in relatively good health, with preserved physical and cognitive function, reflecting the dynamic balance between damage accumulation and the capacity for physiological resilience. Eurostat’s Healthy Life Years (HLY) indicator at birth, estimates the expected years lived without long-standing activity limitation due to health problems. Other summary metrics exist, including the Healthy Life Expectancy (HALE) of World Health Organization (WHO), in which years of life are weighted according to health status [2, 3]. In Italy, in 2023, HLY at birth were 69.6 years for women and 68.5 for men, compared with life expectancy at birth of 85.4 and 81.4 years, respectively (Figure 1). In this context, a strategic response is longevity medicine, an emerging discipline focused on early detection, preventive measures, and personalized approaches that aim to extend healthspan and promote healthy aging [4]. In this paper, we use the term ‘longevity medicine’ not to denote a distinct clinical specialty, but rather a translational framework that integrates geroscience, prevention, and health-system innovation across the life course.
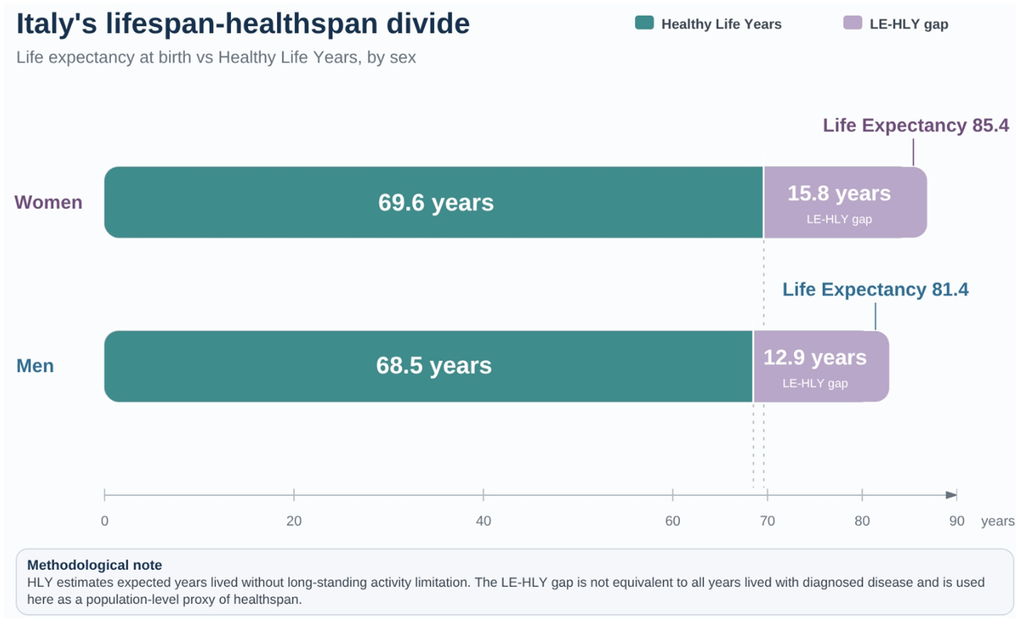
Figure 1. Italy’s lifespan–healthspan divide. Life expectancy (LE) at birth substantially exceeds Healthy Life Years (HLY) in both women and men in Italy. In 2023, women had a life expectancy of 85.4 years and 69.6 HLY, corresponding to a 15.8-year LE–HLY gap; men had a life expectancy of 81.4 years and 68.5 HLY, corresponding to a 12.9-year gap. HLY is used here as a population-level proxy of healthspan, defined as expected years lived without long-standing activity limitation. The LE–HLY gap should therefore not be interpreted as all years lived with diagnosed disease, but as an indicator of the mismatch between longevity and years lived without substantial health-related activity limitation.
Building on this definition, this position paper aims to provide a conceptual framework and strategic policy directions, positioning longevity medicine as an evidence-based, prevention-focused approach to healthy aging within the Italian SSN. Accordingly, it presents: (a) an overview of some of the most important factors contributing to the Italian lifespan-healthspan divide; (b) structural and systemic constraints of the SSN (Servizio Sanitario Nazionale - Italian National Health System); (c) conceptual foundations of longevity medicine; (d) strategic investment priorities.
Lifespan-healthspan divide: an overview of determinants
Socio-economic and regional gradients
Life expectancy differs by up to 3.8 years between northern and southern Italy, likely reflecting regional disparities in education, income, and preventive care [5]. More broadly, cohort and meta-analytic evidence suggests that socioeconomic disadvantage is associated with less favorable aging trajectories and a higher burden of multimorbidity [6–9].
Lifestyle
Survey data suggest that high adherence to the Mediterranean diet is uncommon [10]. National survey data indicate that more than 40% of Italians aged ≥65 years are sedentary, with even higher proportions among those ≥75 years old [11].
Environmental exposure
Fine particulate air pollution (PM2.5) remains an important public-health concern in Italy. European assessments indicate that ambient concentrations in several EU countries, including Italy, remain above the 2021 WHO annual guideline, while long-term exposure to PM2.5 has been associated with increased mortality risk [12, 13].
Gender differences in aging
Women in Italy live longer than men, but these additional years are more often lived with functional limitations and multimorbidity [20–22]. Gender-related differences in prescribing quality and medication safety have also been reported in older adults, underscoring the importance of sex-aware approaches to pharmacological management [23]. These differences likely reflect the interaction of biological, behavioral, and social determinants, including sex-specific disease susceptibility, differential exposure to risk factors across the life course, and gendered patterns of healthcare utilization and caregiving. From a longevity medicine perspective, these findings underscore the need for sex-aware risk stratification and prevention strategies, as well as the importance of ensuring that emerging tools—such as biomarkers of biological aging and digital monitoring platforms—are validated across both sexes and do not exacerbate existing disparities.
Digital divide
Evidence from remote areas of Italy highlights a substantial digital health gap among older adults, where limited digital health literacy constrains the adoption of telemonitoring platforms [24].
Medication burden and gender medicine
More than a quarter of community-dwelling older adults report polypharmacy, with prevalence rising with age [25]. Evidence from Italian and European studies shows that polypharmacy is associated with frailty progression and increased mortality [26, 27]. Recent studies highlight gender-specific patterns in prescribing and adverse drug reactions, underscoring the complexity of safe medication management in older adults [28, 29].
Structural and systemic constraints of the SSN
The lifespan–healthspan divide also highlights the limitations of a reactive care model, rather than a P4 model of care (predictive, preventive, personalized and participatory) [30]. Indeed, a large share of healthcare spending is devoted to individuals with chronic diseases and disabilities [31]. Without a shift toward evidence-based prevention and healthier aging across the life course, improvements in treatment pathways may be insufficient to substantially reduce the accumulation of multimorbidity. This pattern could increase pressure on healthcare systems in Italy and elsewhere, underscoring the need for timely policy attention [30, 32]. We outline here some of the major constraints of the SSN.
Fragmented and hospital-centric pathways
The regionalized organization of the SSN has contributed to substantial heterogeneity in funding, staffing, service delivery, and performance across regions and autonomous provinces [33]. Moreover, digital fragmentation persists, with incomplete interoperability of electronic health records across regions and care settings [34]. Home-care coverage for older adults has wide regional variability and often low care intensity [35, 36]. These structural features have direct implications for the feasibility of a longevity-oriented approach. Fragmentation limits the ability to construct longitudinal, life-course health trajectories, which are essential for assessing biological aging and preventive interventions. Incomplete interoperability constrains the integration of clinical, behavioral, and sensor-derived data, thereby limiting the development of robust risk stratification tools. At the same time, hospital-centric organization and low-intensity home care reduce opportunities for continuous monitoring and early intervention, which are central to prevention-oriented models of care.
Reactive financing
Diagnosis-related group reimbursement mechanisms prioritize reactive over preventive services [36, 37]. Prevention has historically accounted for a modest share of spending relative to national planning. Although modelling evidence cannot replace country-specific evaluation, some studies suggest that evidence-based preventive allocation could improve long-term health outcomes and the sustainability of the system [38].
Under-resourced multidisciplinary teams
In Italy, geriatricians represent a relatively small proportion of the specialist workforce, and comprehensive training in evidence-based geriatric care, encompassing deprescribing, functional assessment and rehabilitation planning, and data-driven decision-making, remains limited [39]. Although national specialization schools provide structured curricula in geriatrics, the modest number of trained professionals and the scarcity of widespread educational programs constrain the capacity of the health system to fully integrate geriatric principles into routine practice [40].
Digital and participatory inertia
Digital adoption remains uneven, especially among older adults in remote areas, where limited digital skills and infrastructural barriers continue to constrain uptake [41]. International pilot studies provide proof-of-concept. In Catalonia, the ProPCC program (Program to People with Complex Chronic Conditions) was associated with fewer emergency department visits and hospital stays [42], while ProACT (ProACTive Patient Centered Care) [43], tested in Ireland and Belgium, showed sustained engagement over 12 months. While these findings should be interpreted cautiously, they suggest that wider implementation may be feasible, particularly if interoperability improves and reimbursement evolves to better support digital care [44, 45].
Conceptual foundations of longevity medicine
Collectively, these environmental, demographic, socio-economic, behavioral, and healthcare-related factors converge to accelerate functional decline and increase demand for healthcare services [46]. As mentioned, a potential strategic response is the development of longevity medicine, conceived as a life-course, prevention-oriented framework aimed at extending healthspan. It combines person-centered care with an explicit focus on preserving functional capacity, rather than solely preventing individual diseases, while integrating upstream prevention targeting modifiable exposures across the lifespan. In this sense, longevity medicine may provide a framework for assessing biological aging and for testing interventions aimed at modifying aging-related risk trajectories, with particular emphasis on preserving the capacity to respond to internal and external stressors [4]. It should be conceived not merely as a discipline dedicated to the care of older adults, but as a life-course approach that also targets middle-aged populations and is complemented by preventive policies addressing the long-term impact of early-life exposures and behaviors on aging trajectories. Moreover, it should be built on the SSN, extending geriatric principles of person-centered, function-oriented care across the life course. Crucially, it should be held to the same evidence principles as any medical field: prioritizing hard outcomes (e.g., incident multimorbidity, hospitalizations and mortality) and quantifying benefits and harms (e.g., overdiagnosis, overtreatment, and inequitable access) [47, 48]. In the longevity field, as chronological age is insufficient to capture the complexity of aging, tools that quantify biological age and aging clocks become attractive [49]. At present, biological age metrics should be regarded as research tools and should not guide clinical decision-making or reimbursement policies until their reproducibility, responsiveness to intervention, and impact on patient-relevant outcomes are clearly demonstrated Two complementary frameworks are under development by several stakeholders: multi-omics and exposome [50, 51]. Multi-omics approaches use molecular layers (e.g., epigenomics, transcriptomics, proteomics, metabolomics, microbiome) to summarize the biological state and potentially predict risk beyond chronological age [52]. Conversely, the exposome aims to characterize non-genetic exposures across the life course (e.g., environmental, behavioral, and occupational) acting as upstream drivers of aging trajectories [53, 54]. Critical windows (e.g., prenatal, early childhood, mid-life) link risk and protective factors with inflammatory and epigenetic signatures, associated with multimorbidity and disability [54–56]. When considered together, these frameworks may support a more comprehensive assessment of aging-related risk, integrating modifiable exposures with molecular profiles [57]. Conversely, considering the quality of evidence informing these tools, biological-age metrics and aging clocks should be carefully treated as exploratory or surrogate tools until they demonstrate reproducibility across heterogeneous settings and responsiveness to interventions that translate into meaningful gains in healthspan extension [58]. Indeed, despite progress in the development of these tools, they are rarely used in clinical practice [59].
The following are proposed, still speculative, pillars of longevity medicine (Figure 2). It should be pointed out that the translation of longevity medicine into health systems raises important risks that should be explicitly acknowledged. Many of the proposed tools, particularly biological age metrics, multi-omic profiling, and AI-based risk stratification, remain supported primarily by associative or surrogate evidence. Premature clinical implementation may lead to overdiagnosis, overtreatment, and inefficient allocation of healthcare resources, particularly in publicly funded systems such as the SSN. Therefore, any integration into routine care should be contingent on rigorous demonstration of clinical utility, cost-effectiveness, and equity, with priority given to interventions that improve hard outcomes rather than surrogate markers.
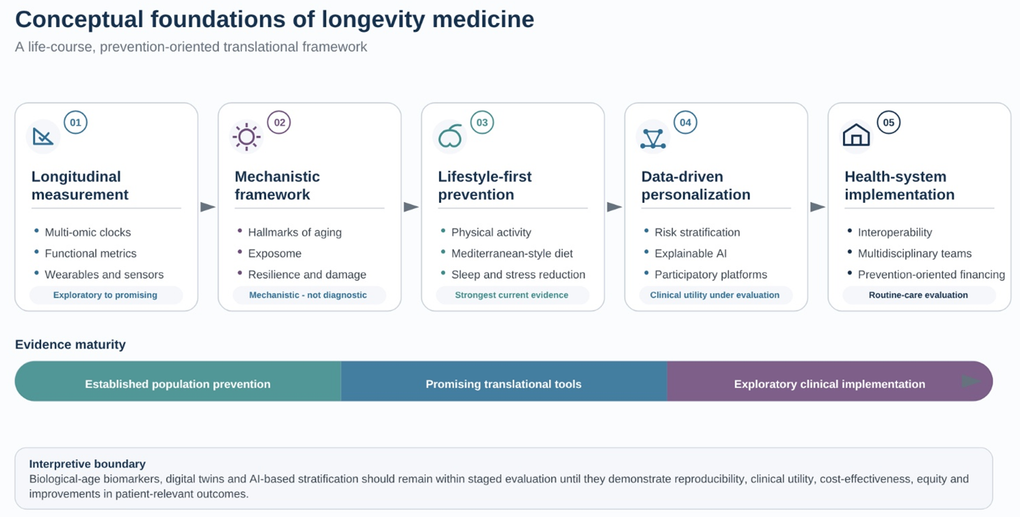
Figure 2. Conceptual foundations of longevity medicine. Longevity medicine is presented as a life-course, prevention-oriented translational framework aimed at preserving functional capacity and extending healthspan. The framework integrates longitudinal assessment of biological aging, mechanistic geroscience, evidence-based lifestyle prevention, data-driven personalization, participatory care, and health-system implementation. While lifestyle interventions currently represent the strongest evidence base, several emerging tools—including biological-age biomarkers, multi-omic profiling, wearable-derived metrics, and AI-based risk stratification—remain exploratory or surrogate and require validation against patient-relevant outcomes before routine clinical implementation.
Longitudinal measurement of biological aging
The longitudinal assessment of biological age can be informed by the combination of multi-omics aging clocks (e.g., proteomic and DNA-methylation clocks) and continuous sensor-derived metrics from consumer wearables (e.g., smartwatches) [60]. The integration of longitudinal molecular and functional data can inform the design of preventive interventions and risk prediction algorithms [61]. Such tools may predict mortality, multimorbidity, and physical function beyond chronological age [62, 63]. Indeed, composite biomarkers such as the Pace of Aging can explain a proportion of the variance in functional decline. Still, as these innovations are supported by limited human evidence, policymakers should carefully analyze the emerging evidence informing such innovations, taking into account failed trials, methodological bias, and null results [64]. This would avoid the over-extension of poor evidence to policy prescription [65].
Hallmarks of aging and lifestyle interventions
The hallmarks of aging are best viewed as a conceptual map of conserved molecular processes that drive loss of physiological integrity with age; still none have yet been clinically validated [66]. In other words, they are more a mechanistic framework than clinically validated diagnostic tools [66]. Moving from mechanistic plausibility to clinical utility will require robust biomarkers, reliable measures, and meaningful endpoints. Lifestyle interventions currently provide a stronger evidence background. Mediterranean-style diets, regular physical activity, restorative sleep, and stress reduction appear to modulate several aging-related pathways, including nutrient sensing, inflammation, mitochondrial function, and epigenetic regulation, although these effects should not be interpreted as direct readouts of any single hallmark [67–69]. By contrast, pharmacological geroprotectors, such as metformin, and emerging senolytics, remain exploratory, with uncertain human clinical endpoints [70, 71]. Experimental strategies, including heterochronic plasma exchange, are at an early stage and remain limited by major technical and translational constraints [72]. Progress in geroscience will therefore depend on developing robust measures of biological aging that can support the next generation of clinical trials [73].
Data-driven personalization and participatory implementation
Biological aging measures such as DNA-methylation clocks and DunedinPACE have shown associations with morbidity and functional decline beyond chronological age, although their clinical application remains unproven [63, 65]. Combined with multi-omic, exposomic, and sensor-derived data, these tools may help refine risk stratification and support more tailored prevention strategies, but only if they prove interpretable, feasible, and useful in routine care [60, 65]. Participatory platforms such as ProACT provide a possible implementation model by supporting self-management among older adults with multimorbidity [43]. At present, the case for personalization remains contingent on whether such data can improve decisions and outcomes in real-world settings [65].
Re-architecting health-system infrastructure for precision longevity
Moving from predominantly reactive disease care toward a more prevention-oriented approach to healthy aging may require targeted organizational adaptations within the SSN. In particular, progress relies on stronger interoperability, integration across care settings, multidisciplinary capacity, and prevention-oriented financing [35, 38]. Regional primary-care hubs can provide a pragmatic setting for remote monitoring, data integration, and referral to multidisciplinary services [44, 45]. Secure biobanks, privacy-preserving analytics, and AI-based risk stratification could contribute to this agenda, provided that their role is established through routine-care evaluation focused on clinical utility, feasibility, equity, and data governance [74–76]. Their adoption should be guided by measurable effects on hard outcomes, cost-effectiveness, and equity [45, 73, 77]. Legislative and reimbursement reforms that favor preventive, rather than reactive, interventions could support this agenda by enabling rigorous implementation and comparative evaluation [35].
Overall, these proposals should be interpreted as an agenda for staged evaluation. Their policy relevance will depend on whether stronger evidence emerges on patient-relevant outcomes, feasibility, cost-effectiveness, and equity [48].
The case for multidisciplinary translational research
Geroscience provides the translational foundation for longevity medicine by testing interventions that may extend healthspan. Progress will depend on methodological rigor, including the use of reproducible biomarkers, pragmatic trial designs, and, critically, the identification of clinically meaningful endpoints. In the context of geroscience, these should extend beyond traditional disease-specific outcomes to include trajectories of physical and cognitive function, resilience to stressors, incident multimorbidity, and other integrative measures of healthspan [78]. Within this framework, multidisciplinary translational research may help align clinical medicine, trial methodology, behavioral research, and health policy around a common task: identifying which interventions can generate measurable gains in healthspan within routine clinical care. Existing infrastructures already offer some components for this agenda. The NIH Translational Geroscience Network, European biobank infrastructures (BBMRI-ERIC), and the Italian Age-It program provide harmonized protocols and distributed cohorts that can support more comparable early-phase geroscience studies [79, 80]. Early dialogue with regulators (AIFA, EMA) can help clarify evidentiary standards for biomarker-informed endpoints and adaptive designs, while embedding health economists in trial design can generate early estimates of costs and QALYs (Quality-Adjusted Life Years) relevant to scalability, reimbursement, and policy uptake [81]. Behavioral science can strengthen this translational pathway: simple digital nudges, brief peer coaching, and integrated platforms such as ProACT may improve adherence to preventive interventions [43, 82]. Within this framework, Italy could build on existing national assets to develop a coordinated platform for translational aging research, linking biobanking, molecular profiling, clinical data, and territorial care infrastructures.
Strategic investment priorities (Figure 3)

Figure 3. Strategic investment priorities for the Italian National Health Service. Five medium-term investment priorities are proposed to support a national healthspan agenda within the Italian National Health Service: clinically validated biomarkers of biological age, interoperable digital monitoring platforms, Bayesian adaptive multimodal trials, explainable AI-based risk stratification, and longevity-informed workforce and citizen literacy. These priorities should be interpreted as a staged evaluation agenda rather than as already validated clinical solutions. Their relevance for health-system policy will depend on demonstrated clinical utility, feasibility, equity, cost-effectiveness, and measurable improvements in patient-relevant outcomes.
Biomarkers of biological age. Develop and validate biomarkers of biological age for potential use in routine care, including sex- and ethnicity-specific tools. Priority should be given to standardizing and externally validating integrated multi-omic clocks [77, 83].
Interoperable digital platforms. Adopt national standards so that data from wearables and home sensors can be integrated into SSN records, enabling scalable telemonitoring, with evaluation focused on hospitalizations, feasibility, and equity, while age-friendly design helps limit a widening digital divide [35, 36].
Bayesian adaptive multimodal trials. Use platform trials with shared control arms and Bayesian adaptive designs to potentially test nutritional, pharmacological, physical, and cognitive interventions in parallel, with the aim of improving efficiency and accelerating the evaluation of gerotherapeutics [84].
Explainable AI risk stratification. Develop privacy-preserving, explainable AI models to predict risks, with mandatory bias audits and documentation standards aligned with international best practice [75].
Age-proof workforce and citizen literacy. Introduce a longevity curriculum in medical and specialist training to build skills in multimorbidity and healthy aging and combine this with population-level communication strategies to improve health literacy [85].
Together, these priorities should be viewed as a staged agenda for evaluation; their relevance will depend on whether they deliver measurable gains in patient-relevant outcomes, feasibility, cost-effectiveness, and equity within the SSN. These proposals should be interpreted as medium-term translational priorities.
Outlook: from pilots to a national healthspan agenda
Italy’s demographic trajectory is fixed, and the COVID-19 pandemic showed its frailty, yet its repercussions for the SSN are potentially modifiable. As discussed, many scientific, digital, and organizational assets are already in place. Still, the main challenge is evidence-based implementation [86]. Scalable tools (e.g., wearable sensors, AI-assisted support, and digital exercise interventions) have shown encouraging effects on outcomes such as frailty-related measures [87–89]. If integrated into primary care with rigorous evaluation, these tools may help reduce the burden of chronic disease and disability, thereby easing pressure on the SSN [90]. One of the next steps is to move from pilots to scalable programs. Initiatives such as AGE-IT may strengthen the evidence base on aging trajectories and candidate biomarkers, while living labs could provide comparative data on effectiveness [74, 91]. If supported by stronger evidence and feasible implementation pathways, Italy could serve as a natural testbed for the development and evaluation of healthspan-oriented models of care. Given its advanced demographic aging, regional heterogeneity, and universal healthcare system, the SSN offers a unique setting to assess whether geroscience-informed interventions can deliver measurable gains in function, resilience, and multimorbidity prevention. The challenge is not only scientific, but organizational: moving from promising pilots to scalable, evidence-based programs that preserve functional capacity and resilience, and that can be rigorously evaluated and equitably implemented within the SSN.
Author Contributions
All authors contributed to the conception and scope of this article. Dr. Nicola Marino and Dr. Matteo Fiore drafted the original manuscript, and Prof. Luigi Ferrucci provided critical revisions. All authors supervised, reviewed, edited, and approved the final version.
Conflicts of Interest
C.R. is author of The Healthspan Code, Therapeutic Revolution and is co-founder of AION Healthspan, Inc. F.d’A.d.F. is supported by the following funds: ERC advanced grant TELORNAGING – 835103; ERC POC TELOVACCINE – 101113229; AIRC-IG 30471; AIRCIG 21762; AIRC 5x1000 21091; Telethon GMR23T2007; Progetti di Ricerca di Interesse Nazionale (PRIN) 2020CXFL4T; Progetti di Ricerca di Interesse Nazionale (PRIN) 2022R7LH5T AriSLA DDR&ALS FG_24_2020; POR FESR InterSLA DSB.AD004.294; Next Generation EU, in the context of the National Recovery and Resilience Plan, Investment PE8 Project Age-It; Investment CN3 National Center for Gene Therapy and Drugs based on RNA Technology. M.D. is the founder and shareholder of Cleara Biotech and an advisor for Oisin Biotechnologies and Rubedo Life Sciences. The M.D. laboratory received funding from Ono Pharmaceuticals. M.Q. is a co-founder, shareholder, and executive of Rubedo Life Sciences, a biotechnology company developing senotherapeutic therapies.
Funding
No funding was received for this paper.
References
- 1. ISTAT. Rapporto annuale 2024. LA SITUAZIONE DEL PAESE. Presentata da: Francesco Maria Chelli. 2024. https://www.istat.it/wp-content/uploads/2024/05/Rapporto-Annuale-2024.pdf.
- 2. Robine JM, Ritchie K. Healthy life expectancy: evaluation of global indicator of change in population health. BMJ. 1991; 302:457–60. https://doi.org/10.1136/bmj.302.6774.457 [PubMed]
- 3. Wolfson MC. Health-adjusted life expectancy. Health Rep. 1996; 8:41–6. [PubMed]
- 4. Martinović A, Mantovani M, Trpchevska N, Novak E, Milev NB, Bode L, Ewald CY, Bischof E, Reichmuth T, Lapides R, Navarini A, Saravi B, Roider E. Climbing the longevity pyramid: overview of evidence-driven healthcare prevention strategies for human longevity. Front Aging. 2024; 5:1495029. https://doi.org/10.3389/fragi.2024.1495029 [PubMed]
- 5. OECD. State of Health in the EU, Italy, Country Health Profile 2021. https://www.oecd.org/content/dam/oecd/en/publications/reports/2021/12/italy-country-health-profile-2021_72799112/5bb1946e-en.pdf.
- 6. Kuo PL, Moore AZ, Tanaka T, Belsky DW, Lu AT, Horvath S, Bandinelli S, Ferrucci L. Longitudinal changes in epigenetic clocks predict survival in the InCHIANTI cohort. Nat Aging. 2026; 6:534–40. https://doi.org/10.1038/s43587-026-01066-6 [PubMed]
- 7. Kuo PL, Schrack JA, Levine ME, Shardell MD, Simonsick EM, Chia CW, Moore AZ, Tanaka T, An Y, Karikkineth A, AlGhatrif M, Elango P, Zukley LM, et al. Longitudinal phenotypic aging metrics in the Baltimore Longitudinal Study of Aging. Nat Aging. 2022; 2:635–43. https://doi.org/10.1038/s43587-022-00243-7 [PubMed]
- 8. Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. 2018; 42:186–94. https://doi.org/10.1111/1753-6405.12762 [PubMed]
- 9. Ingram E, Ledden S, Beardon S, Gomes M, Hogarth S, McDonald H, Osborn DP, Sheringham J. Household and area-level social determinants of multimorbidity: a systematic review. J Epidemiol Community Health. 2021; 75:232–41. https://doi.org/10.1136/jech-2020-214691 [PubMed]
- 10. Cardamone E, Iacoponi F, Di Benedetto R, Lorenzoni G, Di Nucci A, Zobec F, Gregori D, Silano M. Adherence to Mediterranean Diet and its main determinants in a sample of Italian adults: results from the ARIANNA cross-sectional survey. Front Nutr. 2024; 11:1346455. https://doi.org/10.3389/fnut.2024.1346455 [PubMed]
- 11. ISS. Gruppo Tecnico Passi - La sorveglianza Passi d'Argento: i dati per l'Italia: attività Fisica (2023-2024). 2025. https://www.epicentro.iss.it/passi-argento/info/archivio-2025.
- 12. Beelen R, Raaschou-Nielsen O, Stafoggia M, Andersen ZJ, Weinmayr G, Hoffmann B, Wolf K, Samoli E, Fischer P, Nieuwenhuijsen M, Vineis P, Xun WW, Katsouyanni K, et al. Effects of long-term exposure to air pollution on natural-cause mortality: an analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet. 2014; 383:785–95. https://doi.org/10.1016/S0140-6736(13)62158-3 [PubMed]
- 13. EEA. European Environment Agency: Air quality status report 2025: particulate matter - PM2.5. 2025. https://www.eea.europa.eu/en/analysis/publications/air-quality-status-report-2025/particulate-matter-pm2.5.
- 14. Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci. 2015; 10:227–37. https://doi.org/10.1177/1745691614568352 [PubMed]
- 15. Kojima G, Taniguchi Y, Iliffe S, Jivraj S, Walters K. Transitions between frailty states among community-dwelling older people: A systematic review and meta-analysis. Ageing Res Rev. 2019; 50:81–8. https://doi.org/10.1016/j.arr.2019.01.010 [PubMed]
- 16. Kuiper JS, Zuidersma M, Oude Voshaar RC, Zuidema SU, van den Heuvel ER, Stolk RP, Smidt N. Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev. 2015; 22:39–57. https://doi.org/10.1016/j.arr.2015.04.006 [PubMed]
- 17. Angela Chieppa SD, Simona Mastroluca. Home alone, the one-person households at the Italian 2021 permanent census. Who are they? Where do they live? RIEDS - Rivista Italiana di Economia, Demografia e Statistica - The Italian Journal of Economic, Demographic and Statistical Studies. 2023; 77:2. https://doi.org/10.71014/sieds.v77i2.185
- 18. Sharma N, Chakrabarti S, Grover S. Gender differences in caregiving among family - caregivers of people with mental illnesses. World J Psychiatry. 2016; 6:7–17. https://doi.org/10.5498/wjp.v6.i1.7 [PubMed]
- 19. ISS. Differenze di genere: i Caregiver familiari. Marina Petrini, Antonio D’amore (Centro di riferimento per la Medicina di Genere). 2020. https://www.epicentro.iss.it/coronavirus/sars-cov-2-differenze-genere-caregiver-familiari.
- 20. Muszynska-Spielauer M, Di Giulio P, Minagawa Y, Di Lego V, Luy M. Why do women live longer than men, but spend more time in poor health? A decomposition analysis of the gender gap in unhealthy life years across Europe. Eur J Epidemiol. 2026; 41:329–36. https://doi.org/10.1007/s10654-025-01346-2 [PubMed]
- 21. Naghavi M, and GBD 2021 Italy Subnational Burden of Disease Collaborators. State of health and inequalities among Italian regions from 2000 to 2021: a systematic analysis based on the Global Burden of Disease Study 2021. Lancet Public Health. 2025; 10:e309–20. https://doi.org/10.1016/S2468-2667(25)00045-3 [PubMed]
- 22. OECD. State of Health in the EU Italy Country Health Profile 2023. https://doi.org/10.1787/633496ec-en
- 23. Zito S, Pierantozzi A, Marinelli M, Ambrosino F, Trotta F, Cangini A. [Medicines use in older adults in Italy. The OsMed National Report 2019.]. Recenti Prog Med. 2022; 113:76–83. https://doi.org/10.1701/3748.37310 [PubMed]
- 24. Vainieri M, Vandelli A, Benvenuti SC, Bertarelli G. Tracking the digital health gap in elderly: A study in Italian remote areas. Health Policy. 2023; 133:104842. https://doi.org/10.1016/j.healthpol.2023.104842 [PubMed]
- 25. Perdixi E, Cotta Ramusino M, Costa A, Bernini S, Conti S, Jesuthasan N, Severgnini M, Prinelli F, and NutBrain Study Group. Polypharmacy, drug-drug interactions, anticholinergic burden and cognitive outcomes: a snapshot from a community-dwelling sample of older men and women in northern Italy. Eur J Ageing. 2024; 21:11. https://doi.org/10.1007/s10433-024-00806-0 [PubMed]
- 26. Toh JJ, Zhang H, Soh YY, Zhang Z, Wu XV. Prevalence and health outcomes of polypharmacy and hyperpolypharmacy in older adults with frailty: A systematic review and meta-analysis. Ageing Res Rev. 2023; 83:101811. https://doi.org/10.1016/j.arr.2022.101811 [PubMed]
- 27. Bennie M, Santa-Ana-Tellez Y, Galistiani GF, Trehony J, Despres J, Jouaville LS, Poluzzi E, Morin L, Schubert I, MacBride-Stewart S, Elseviers M, Nasuti P, Taxis K. The prevalence of polypharmacy in older Europeans: A multi-national database study of general practitioner prescribing. Br J Clin Pharmacol. 2024; 90:2124–36. https://doi.org/10.1111/bcp.16113 [PubMed]
- 28. Crescioli G, Boscia E, Bettiol A, Pagani S, Spada G, Vighi GV, Bonaiuti R, Venegoni M, Vighi GD, Vannacci A, Lombardi N, On Behalf Of The MEREAFaPS Study Gr. Risk of Hospitalization for Adverse Drug Events in Women and Men: A Post Hoc Analysis of an Active Pharmacovigilance Study in Italian Emergency Departments. Pharmaceuticals (Basel). 2021; 14:678. https://doi.org/10.3390/ph14070678 [PubMed]
- 29. Piccoliori G, Mahlknecht A, Sandri M, Valentini M, Vögele A, Schmid S, Deflorian F, Engl A, Sönnichsen A, Wiedermann C. Epidemiology and associated factors of polypharmacy in older patients in primary care: a northern Italian cross-sectional study. BMC Geriatr. 2021; 21:197. https://doi.org/10.1186/s12877-021-02141-w [PubMed]
- 30. Sagner M, McNeil A, Puska P, Auffray C, Price ND, Hood L, Lavie CJ, Han ZG, Chen Z, Brahmachari SK, McEwen BS, Soares MB, Balling R, et al. The P4 Health Spectrum - A Predictive, Preventive, Personalized and Participatory Continuum for Promoting Healthspan. Prog Cardiovasc Dis. 2017; 59:506–21. https://doi.org/10.1016/j.pcad.2016.08.002 [PubMed]
- 31. Corti MC, Avossa F, Schievano E, Gallina P, Ferroni E, Alba N, Dotto M, Basso C, Netti ST, Fedeli U, Mantoan D. A case-mix classification system for explaining healthcare costs using administrative data in Italy. Eur J Intern Med. 2018; 54:13–6. https://doi.org/10.1016/j.ejim.2018.02.035 [PubMed]
- 32. Khoury MJ, Iademarco MF, Riley WT. Precision Public Health for the Era of Precision Medicine. Am J Prev Med. 2016; 50:398–401. https://doi.org/10.1016/j.amepre.2015.08.031 [PubMed]
- 33. Fiore M, Bianconi A, Acuti Martellucci C, Rosso A, Zauli E, Flacco ME, Manzoli L. Impact of the Italian Healthcare Outcomes Program (PNE) on the Care Quality of the Poorest Performing Hospitals. Healthcare (Basel). 2024; 12:431. https://doi.org/10.3390/healthcare12040431 [PubMed]
- 34. The Lancet Regional He. The Italian health data system is broken. Lancet Reg Health Eur. 2025; 48:101206. https://doi.org/10.1016/j.lanepe.2024.101206 [PubMed]
- 35. Cinelli G, Fattore G. The 2022 community-based integrated care reform in Italy: From desiderata to implementation. Health Policy. 2024; 139:104943. https://doi.org/10.1016/j.healthpol.2023.104943 [PubMed]
- 36. Ricciardi W, Tarricone R. The evolution of the Italian National Health Service. Lancet. 2021; 398:2193–206. https://doi.org/10.1016/S0140-6736(21)01733-5 [PubMed]
- 37. Rosso A, Marzuillo C, Massimi A, De Vito C, de Belvis AG, La Torre G, Federici A, Ricciardi W, Villari P. Policy and planning of prevention in Italy: Results from an appraisal of prevention plans developed by Regions for the period 2010-2012. Health Policy. 2015; 119:760–9. https://doi.org/10.1016/j.healthpol.2015.03.012 [PubMed]
- 38. Milstein R, Schreyögg J. The end of an era? Activity-based funding based on diagnosis-related groups: A review of payment reforms in the inpatient sector in 10 high-income countries. Health Policy. 2024; 141:104990. https://doi.org/10.1016/j.healthpol.2023.104990 [PubMed]
- 39. Cesari M, Thiyagarajan JA, Cherubini A, Acanfora MA, Assantachai P, Barbagallo M, Coume M, Diaz T, Fuggle N, Hammami SO, Madden K, Matijevic R, Michel JP, et al. Defining the role and reach of a geriatrician. Lancet Healthy Longev. 2024; 5:100644. https://doi.org/10.1016/j.lanhl.2024.100644 [PubMed]
- 40. Stuck AE, Masud T. Health care for older adults in Europe: how has it evolved and what are the challenges? Age Ageing. 2022; 51:afac287. https://doi.org/10.1093/ageing/afac287 [PubMed]
- 41. Galdiero C, Marrapodi R, Mele S, Scaletti A, Martinez M. Mapping digital transformation and social impact in Italian healthcare: a holistic evaluation of organizational digital maturity. BMC Health Serv Res. 2025; 25:1609. https://doi.org/10.1186/s12913-025-13473-3 [PubMed]
- 42. Mas MÀ, Miralles R, Ulldemolins MJ, Garcia R, Gràcia S, Picaza JM, Fernández MN, Rocabayera MA, Rivera M, Relaño N, Asensio MT, Laporta P, Morcillo C, et al. Evaluating Person-Centred Integrated Care to People with Complex Chronic Conditions: Early Implementation Results of the ProPCC Programme. Int J Integr Care. 2023; 23:18. https://doi.org/10.5334/ijic.7585 [PubMed]
- 43. Doyle J, Murphy E, Gavin S, Pascale A, Deparis S, Tommasi P, Smith S, Hannigan C, Sillevis Smitt M, van Leeuwen C, Lastra J, Galvin M, McAleer P, et al. A Digital Platform to Support Self-management of Multiple Chronic Conditions (ProACT): Findings in Relation to Engagement During a One-Year Proof-of-Concept Trial. J Med Internet Res. 2021; 23:e22672. https://doi.org/10.2196/22672 [PubMed]
- 44. Cresswell K, Williams R. Large-scale system-level digitalisation initiatives in the National Health Service in England: insights from three national evaluations. NPJ Digit Med. 2026; 9:301. https://doi.org/10.1038/s41746-026-02495-8 [PubMed]
- 45. Chandak A, Gudapati J, Kulkarni PB. The cost-effectiveness and patient satisfaction of telehealth in geriatric care: a systematic review. BMC Geriatr. 2025; 25:968. https://doi.org/10.1186/s12877-025-06638-6 [PubMed]
- 46. The Lancet. Making more of multimorbidity: an emerging priority. Lancet. 2018; 391:1637. https://doi.org/10.1016/S0140-6736(18)30941-3 [PubMed]
- 47. Fiore M, Ricci M, Rosso A, Flacco ME, Manzoli L. Chronic Obstructive Pulmonary Disease Overdiagnosis and Overtreatment: A Meta-Analysis. J Clin Med. 2023; 12:6978. https://doi.org/10.3390/jcm12226978 [PubMed]
- 48. Ioannidis JP. Correction: Why Most Published Research Findings Are False. PLoS Med. 2022; 19:e1004085. https://doi.org/10.1371/journal.pmed.1004085 [PubMed]
- 49. Kritchevsky SB, Cummings SR. Geroscience: A Translational Review. JAMA. 2025; 334:1094–102. https://doi.org/10.1001/jama.2025.11289 [PubMed]
- 50. Kočar E, Šket R, Vasle AH, Avguštin G, Benedik E, Seljak BK, Simić P, Martinko A, Morrison SA, Sorić M, Skrt M, Polak T, Tesovnik T, et al. Measuring biological age: Insights from omics studies. Ageing Res Rev. 2026; 114:102988. https://doi.org/10.1016/j.arr.2025.102988 [PubMed]
- 51. Hernandez H, Santamaria-Garcia H, Moguilner S, Farina FR, Legaz A, Prado P, Cuadros J, Gonzalez L, Gonzalez-Gomez R, Migeot J, Coronel-Oliveros C, Tagliazucchi E, Maito MA, et al. The exposome of healthy and accelerated aging across 40 countries. Nat Med. 2025; 31:3089–100. https://doi.org/10.1038/s41591-025-03808-2 [PubMed]
- 52. Ruden DM. The emerging role of multiomics in aging research. Epigenomics. 2025; 17:897–904. https://doi.org/10.1080/17501911.2025.2533111 [PubMed]
- 53. Pandics T, Major D, Fazekas-Pongor V, Szarvas Z, Peterfi A, Mukli P, Gulej R, Ungvari A, Fekete M, Tompa A, Tarantini S, Yabluchanskiy A, Conley S, et al. Exposome and unhealthy aging: environmental drivers from air pollution to occupational exposures. Geroscience. 2023; 45:3381–408. https://doi.org/10.1007/s11357-023-00913-3 [PubMed]
- 54. de Prado-Bert P, Ruiz-Arenas C, Vives-Usano M, Andrusaityte S, Cadiou S, Carracedo Á, Casas M, Chatzi L, Dadvand P, González JR, Grazuleviciene R, Gutzkow KB, Haug LS, et al. The early-life exposome and epigenetic age acceleration in children. Environ Int. 2021; 155:106683. https://doi.org/10.1016/j.envint.2021.106683 [PubMed]
- 55. Cánepa ET, Berardino BG. Epigenetic mechanisms linking early-life adversities and mental health. Biochem J. 2024; 481:615–42. https://doi.org/10.1042/BCJ20230306 [PubMed]
- 56. Chen MA, LeRoy AS, Majd M, Chen JY, Brown RL, Christian LM, Fagundes CP. Immune and Epigenetic Pathways Linking Childhood Adversity and Health Across the Lifespan. Front Psychol. 2021; 12:788351. https://doi.org/10.3389/fpsyg.2021.788351 [PubMed]
- 57. Argentieri MA, Amin N, Nevado-Holgado AJ, Sproviero W, Collister JA, Keestra SM, Kuilman MM, Ginos BN, Ghanbari M, Doherty A, Hunter DJ, Alvergne A, van Duijn CM. Integrating the environmental and genetic architectures of aging and mortality. Nat Med. 2025; 31:1016–25. https://doi.org/10.1038/s41591-024-03483-9 [PubMed]
- 58. Johnson AA, Shokhirev MN. First-generation versus next-generation epigenetic aging clocks: Differences in performance and utility. Biogerontology. 2025; 26:121. https://doi.org/10.1007/s10522-025-10265-4 [PubMed]
- 59. Zhang J, Hu J, Gao Y, Pang Z, Mo L, Wu IX. Are aging clocks based on routine clinical indicators trustworthy and applicable? A systematic review and critical appraisal. J Gerontol A Biol Sci Med Sci. 2026; 81:glag032. https://doi.org/10.1093/gerona/glag032 [PubMed]
- 60. Pusparum M, Thas O, Beck S, Ecker S, Ertaylan G. From ageing clocks to human digital twins in personalising healthcare through biological age analysis. NPJ Digit Med. 2025; 8:537. https://doi.org/10.1038/s41746-025-01911-9 [PubMed]
- 61. Marino N, Putignano G, Cappilli S, Chersoni E, Santuccione A, Calabrese G, Bischof E, Vanhaelen Q, Zhavoronkov A, Scarano B, Mazzotta AD, Santus E. Towards AI-driven longevity research: An overview. Front Aging. 2023; 4:1057204. https://doi.org/10.3389/fragi.2023.1057204 [PubMed]
- 62. Srour L, Bejaoui Y, She J, Alam T, El Hajj N. Deep aging clocks: AI-powered strategies for biological age estimation. Ageing Res Rev. 2025; 112:102889. https://doi.org/10.1016/j.arr.2025.102889 [PubMed]
- 63. Argentieri MA, Xiao S, Bennett D, Winchester L, Nevado-Holgado AJ, Ghose U, Albukhari A, Yao P, Mazidi M, Lv J, Millwood I, Fry H, Rodosthenous RS, et al. Proteomic aging clock predicts mortality and risk of common age-related diseases in diverse populations. Nat Med. 2024; 30:2450–60. https://doi.org/10.1038/s41591-024-03164-7 [PubMed]
- 64. Ioannidis JP. Why most published research findings are false. PLoS Med. 2005; 2:e124. https://doi.org/10.1371/journal.pmed.0020124 [PubMed]
- 65. Apsley AT, Etzel L, Ye Q, Shalev I. From population science to the clinic? Limits of epigenetic clocks as personal biomarkers. Epigenomics. 2025; 17:1447–61. https://doi.org/10.1080/17501911.2025.2603880 [PubMed]
- 66. Keshavarz M, Xie K, Schaaf K, Bano D, Ehninger D. Targeting the "hallmarks of aging" to slow aging and treat age-related disease: fact or fiction? Mol Psychiatry. 2023; 28:242–55. https://doi.org/10.1038/s41380-022-01680-x [PubMed]
- 67. Galkin F, Kovalchuk O, Koldasbayeva D, Zhavoronkov A, Bischof E. Stress, diet, exercise: Common environmental factors and their impact on epigenetic age. Ageing Res Rev. 2023; 88:101956. https://doi.org/10.1016/j.arr.2023.101956 [PubMed]
- 68. Capodici A, Mocciaro G, Gori D, Landry MJ, Masini A, Sanmarchi F, Fiore M, Coa AA, Castagna G, Gardner CD, Guaraldi F. Cardiovascular health and cancer risk associated with plant based diets: An umbrella review. PLoS One. 2024; 19:e0300711. https://doi.org/10.1371/journal.pone.0300711 [PubMed]
- 69. Rajado AT, Silva N, Esteves F, Brito D, Binnie A, Araújo IM, Nóbrega C, Bragança J, Castelo-Branco P, and ALFA Score Consortium. How can we modulate aging through nutrition and physical exercise? An epigenetic approach. Aging (Albany NY). 2023; 15:3191–217. https://doi.org/10.18632/aging.204668 [PubMed]
- 70. Wissler Gerdes EO, Misra A, Netto JM, Tchkonia T, Kirkland JL. Strategies for late phase preclinical and early clinical trials of senolytics. Mech Ageing Dev. 2021; 200:111591. https://doi.org/10.1016/j.mad.2021.111591 [PubMed]
- 71. Mohammed I, Hollenberg MD, Ding H, Triggle CR. A Critical Review of the Evidence That Metformin Is a Putative Anti-Aging Drug That Enhances Healthspan and Extends Lifespan. Front Endocrinol (Lausanne). 2021; 12:718942. https://doi.org/10.3389/fendo.2021.718942 [PubMed]
- 72. Ansere VA, Bubak MP, Miller BF, Freeman WM. Heterochronic Plasma Transfer: Experimental Design, Considerations, and Technical Challenges. Rejuvenation Res. 2023; 26:171–9. https://doi.org/10.1089/rej.2023.0035 [PubMed]
- 73. Moqri M, Herzog C, Poganik JR, Ying K, Justice JN, Belsky DW, Higgins-Chen AT, Chen BH, Cohen AA, Fuellen G, Hägg S, Marioni RE, Widschwendter M, et al. Validation of biomarkers of aging. Nat Med. 2024; 30:360–72. https://doi.org/10.1038/s41591-023-02784-9 [PubMed]
- 74. Chiti F, Conti F, Corda D, Giorgino F, Graziani A, Passarino G, Sandri M, d'Adda di Fagagna F. Improving our understanding of the biology of aging: findings from the Age-It Research Program. J Gerontol B Psychol Sci Soc Sci. 2025 (Suppl 2); 80:S122–35. https://doi.org/10.1093/geronb/gbaf197 [PubMed]
- 75. Lekadir K, Frangi AF, Porras AR, Glocker B, Cintas C, Langlotz CP, Weicken E, Asselbergs FW, Prior F, Collins GS, Kaissis G, Tsakou G, Buvat I, et al., and FUTURE-AI Consortium. FUTURE-AI: international consensus guideline for trustworthy and deployable artificial intelligence in healthcare. BMJ. 2025; 388:e081554. https://doi.org/10.1136/bmj-2024-081554 [PubMed]
- 76. Bakker E, Hendrikse NM, Ehmann F, van der Meer DS, Llinares Garcia J, Vetter T, Starokozhko V, Mol PG. Biomarker Qualification at the European Medicines Agency: A Review of Biomarker Qualification Procedures From 2008 to 2020. Clin Pharmacol Ther. 2022; 112:69–80. https://doi.org/10.1002/cpt.2554 [PubMed]
- 77. Hendrikse NM, Llinares Garcia J, Vetter T, Humphreys AJ, Ehmann F. Biomarkers in Medicines Development-From Discovery to Regulatory Qualification and Beyond. Front Med (Lausanne). 2022; 9:878942. https://doi.org/10.3389/fmed.2022.878942 [PubMed]
- 78. Rolland Y, Sierra F, Ferrucci L, Barzilai N, De Cabo R, Mannick J, Oliva A, Evans W, Angioni D, De Souto Barreto P, Raffin J, Vellas B, Kirkland JL, and G.C.T-TF group. Challenges in developing Geroscience trials. Nat Commun. 2023; 14:5038. https://doi.org/10.1038/s41467-023-39786-7 [PubMed]
- 79. Tchkonia T, Kritchevsky SB, Kuchel GA, Kirkland JL. NIA Translational Geroscience Network: An infrastructure to facilitate geroscience-guided clinical trials. J Am Geriatr Soc. 2024; 72:1605–7. https://doi.org/10.1111/jgs.18901 [PubMed]
- 80. Mate S, Kampf M, Rödle W, Kraus S, Proynova R, Silander K, Ebert L, Lablans M, Schüttler C, Knell C, Eklund N, Hummel M, Holub P, Prokosch HU. Pan-European Data Harmonization for Biobanks in ADOPT BBMRI-ERIC. Appl Clin Inform. 2019; 10:679–92. https://doi.org/10.1055/s-0039-1695793 [PubMed]
- 81. Nguyen Q, Kästel H, Hees K, Hofner B. The use of complex clinical trials: a regulatory review. Trials. 2026; 27:289. https://doi.org/10.1186/s13063-026-09674-8 [PubMed]
- 82. Moffitt TE. Behavioral and Social Research to Accelerate the Geroscience Translation Agenda. Ageing Res Rev. 2020; 63:101146. https://doi.org/10.1016/j.arr.2020.101146 [PubMed]
- 83. Manolis E, Vamvakas S, Isaac M. New pathway for qualification of novel methodologies in the European Medicines Agency. Proteomics Clin Appl. 2011; 5:248–55. https://doi.org/10.1002/prca.201000130 [PubMed]
- 84. Arjas E, Gasbarra D. Adaptive treatment allocation and selection in multi-arm clinical trials: a Bayesian perspective. BMC Med Res Methodol. 2022; 22:50. https://doi.org/10.1186/s12874-022-01526-8 [PubMed]
- 85. Roller-Wirnsberger R, Masud T, Vassallo M, Zöbl M, Reiter R, Van Den Noortgate N, Petermans J, Petrov I, Topinkova E, Andersen-Ranberg K, Saks K, Nuotio M, Bonin-Guillaume S, et al. European postgraduate curriculum in geriatric medicine developed using an international modified Delphi technique. Age Ageing. 2019; 48:291–9. https://doi.org/10.1093/ageing/afy173 [PubMed]
- 86. Piriu AA, Bufali MV, Cappellaro G, Compagni A, Torbica A. Conceptualisation and measurement of healthy ageing: Insights from a systematic literature review. Soc Sci Med. 2025; 374:117933. https://doi.org/10.1016/j.socscimed.2025.117933 [PubMed]
- 87. Fiore M, Bianconi A, Sicari G, Conni A, Lenzi J, Tomaiuolo G, Zito F, Golinelli D, Sanmarchi F. The Use of Smart Rings in Health Monitoring—A Meta-Analysis. Applied Sciences. 2024; 14:10778. https://doi.org/10.3390/app142310778
- 88. Wong SH, Tan ZY, Cheng LJ, Lau ST. Wearable technology-delivered lifestyle intervention amongst adults with overweight and obese: A systematic review and meta-regression. Int J Nurs Stud. 2022; 127:104163. https://doi.org/10.1016/j.ijnurstu.2021.104163 [PubMed]
- 89. Li R, Li Y, Wang L, Li L, Fu C, Hu D, Wei Q. Wearable Activity Tracker-Based Interventions for Physical Activity, Body Composition, and Physical Function Among Community-Dwelling Older Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Med Internet Res. 2025; 27:e59507. https://doi.org/10.2196/59507 [PubMed] Erratum in: J Med Internet Res. 2025; 27:e79133. DOI: 10.2196/79133 PMID:40879248.
- 90. Thomas SA, Browning CJ, Charchar FJ, Klein B, Ory MG, Bowden-Jones H, Chamberlain SR. Transforming global approaches to chronic disease prevention and management across the lifespan: integrating genomics, behavior change, and digital health solutions. Front Public Health. 2023; 11:1248254. https://doi.org/10.3389/fpubh.2023.1248254 [PubMed]
- 91. Kim J, Kim YL, Jang H, Cho M, Lee M, Kim J, Lee H. Living labs for health: an integrative literature review. Eur J Public Health. 2020; 30:55–63. https://doi.org/10.1093/eurpub/ckz105 [PubMed]
Social integration
Social integration is a modifiable determinant of healthspan [14]. Experiences in childhood, adolescence, and midlife shape later-life trajectories of physical, cognitive, and emotional function: early isolation or exclusion increases the risk of frailty and premature mortality, whereas stable, supportive relationships build reserve and resilience [14–16]. Census data show that almost half of older Italians live alone; although living alone does not necessarily imply social isolation, it may identify a subgroup at increased risk of reduced social support, which is relevant because social isolation has been associated with excess mortality [14, 17]. Also, caregivers, most of whom are women, are at risk of social isolation [16, 18, 19].