



Introduction
Stroke is a serious cerebrovascular disease associated with aging, and approximately 80% of stroke events are classified as ischemic strokes [1]. The recovery of neurological function after ischemic stroke onset requires restoring the blood supply of the ischemic brain tissue as early as possible. Mechanical thrombectomy and thrombolytic therapy using tissue plasminogen activator are two common methods to restore blood supply of ischemic brain tissue in ischemic stroke treatments [2]. However, achieving blood reperfusion of the ischemic brain tissue by mechanical thrombectomy or thrombolytic therapy may cause secondary brain injury, also known as cerebral ischemia-reperfusion (CIR) injury [3]. Studies have shown that CIR injury involves multiple mechanisms, such as mitochondrial damage, energy failure, calcium overload, and inflammation [4–6]. These mechanisms can induce neuronal cell death, which causes neurological deficits. Thus, strategies to reduce neuronal cell death may be conducive to treating brain injury after CIR.
Necroptosis is a programmed and regulated cell death and an important pathological foundation of many diseases, such as neurodegenerative diseases, ischemia-reperfusion injury, and inflammation [7–9]. Necroptosis is mainly regulated by receptor-interacting protein kinase 1 (RIPK1), receptor-interacting protein kinase 3 (RIPK3), and mixed lineage kinase domain-like pseudokinase (MLKL) [10]. Certain stimulating factors, such as ischemia-reperfusion, can initiate the tumor necrosis factor-α (TNF-α)-mediated necroptosis signaling pathway, leading to the activation of RIPK1. Activated RIPK1 interacts with RIPK3 and forms necrosomes. Activated RIPK3 in the necrosome phosphorylates MLKL and leads to the formation of oligomers, which translocate to the cytomembrane and cause cytomembrane damage and necroptotic cell death [11]. Several studies have indicated that inhibition of necroptosis can realize neuroprotective effects after CIR in mice, such as reducing cerebral infarct volume and improving motor and cognitive function [12, 13]. Therefore, suppression of necroptosis may be an essential method for the treatment of CIR injury.
Studies have demonstrated that inflammation is a significant contributor to CIR injury [14, 15]. A variety of cells, such as microglia and astrocytes, are activated following ischemic stroke [16]. These activated cells release large amounts of inflammatory mediators such as TNF-α, interleukin-1β (IL-1β), and interleukin-6 (IL-6), aggravating brain injury after CIR [16]. Furthermore, necroptosis is considered a type of cell death that can trigger inflammation. The broken necroptotic cells release various cellular contents into the extracellular environment. Some cellular components, such as damage-associated molecular patterns (DAMPs) can activate immune cells and then elicit inflammation [17], which aggravates brain injury following CIR. Multiple studies have also shown that inhibition of inflammation mitigates brain injury after CIR [18–20].
The carboxyl terminus of Hsp70-interacting protein (CHIP) encoded by the STUB1 gene is an E3 ubiquitin ligase with molecular chaperone and ubiquitin ligase (E3) activity [21, 22]. CHIP participates in cellular protein quality control by regulating the degradation of chaperone-bound proteins [23]. Studies have indicated that CHIP can negatively regulate necroptosis by enhancing the degradation of RIPK1 and RIPK3 [24, 25]. In an in vitro cell model, downregulation of CHIP expression by gene knockdown increased the levels of RIPK1 and RIPK3 [24]. CHIP deficient mice exhibit intestinal inflammation and premature death, whereas RIPK3 knockout can reverse these phenotypes [24]. Our previous study demonstrated that CHIP overexpression exerts protective effects by suppressing necroptosis in an oxygen-glucose deprivation (OGD) cell model [25]. Some studies have also shown that CHIP plays an important role in regulating the immune response [26, 27]. CHIP overexpression attenuates myocardial inflammation in a myocardial dysfunction mouse model [28]. These findings suggest the essential role of CHIP in regulating necroptosis and inflammation.
Necroptosis and inflammation are essential pathogenic mechanisms of CIR injury, and CHIP overexpression can attenuate both. Thus, we hypothesize that CHIP overexpression can ameliorate CIR injury by attenuating necroptosis and inflammation. Using a middle cerebral artery occlusion (MCAO) mouse model, the present study examined CHIP expression after CIR. Moreover, CHIP knock-in (KI) mice overexpressing CHIP in neural tissue and age-matched wild-type (WT) mice were subjected to MCAO surgery to explore whether increasing CHIP levels can exert neuroprotective effects and possible mechanisms.
Results
CHIP expression was upregulated after MCAO
CHIP overexpression can exert neuroprotective effects on many central nervous system (CNS) diseases. Studies have indicated that CHIP expression is increased in some chronic neurodegenerative disorders, such as Alzheimer’s disease [29] and spinocerebellar ataxia type 3 [30]. In the present study, we aimed to evaluate the expression of CHIP in acute neurodegenerative disorders. We established MCAO mouse models using WT mice to detect CHIP expression after CIR. Western blotting and reverse transcription-polymerase chain reaction (RT-PCR) results indicated that CHIP levels of the peri-infarct tissues were increased from 6 h to a peak at 24 h and then decreased after MCAO surgery, remaining higher at 72 h after MCAO surgery than sham surgery (Figure 1A–1C). Immunofluorescence staining results indicated that CHIP was colocalized with NeuN (the neuron marker), and CHIP levels were increased in the peri-infarct tissues at 24 h after MCAO surgery compared with sham surgery (Figure 1D, 1E). These results indicated that CHIP expression was upregulated after MCAO, and neurons might be the primary cellular sources for CHIP induction.
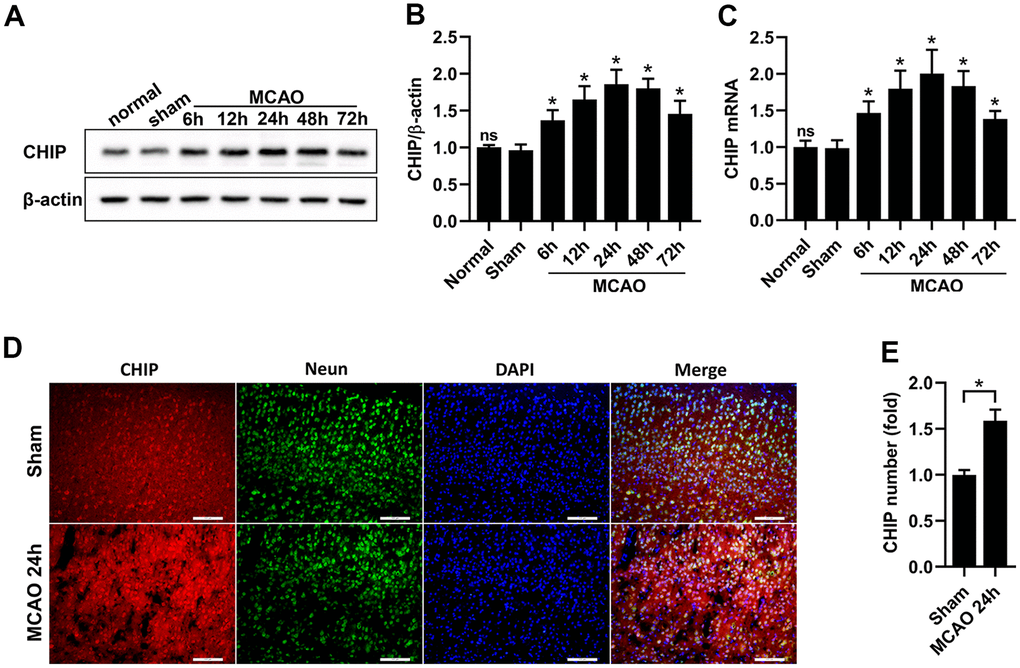
Figure 1. CHIP levels were increased after MCAO. (A, B) Western blot and quantitative analysis of CHIP at different time points after reperfusion in the sham and MCAO surgery groups. (C) The mRNA expression of CHIP. (D, E) Immunostaining and quantitative analysis of CHIP at 24 h after reperfusion in the sham and MCAO surgery groups. Scale bar =100 μm. Data are presented as the mean ± SEM; n=6/group; ns, no significant difference vs. sham group; *P < 0.05 vs. sham group.
CHIP overexpression in the brain of CHIP KI mice
We used CRISPR/Cas9 technology to construct CHIP KI mice carrying an exogenous STUB1 gene to achieve CHIP overexpression in neural tissue. CHIP KI mice and age-matched WT mice were selected to compare CHIP expression in brain tissue. Western blotting results indicated CHIP overexpression in the cortex, striatum, and hippocampus of CHIP KI mice (Figure 2A, 2B), and CHIP mRNA expression in these tissues showed a similar trend (Figure 2C). Consistently, immunochemical staining results showed that CHIP-positive numbers were significantly higher in the cortex and hippocampus of CHIP KI mice than in WT mice (Figure 2D, 2E). Thus, our results indicated that CHIP levels were markedly higher in CHIP KI mouse brains than in WT mouse brains.
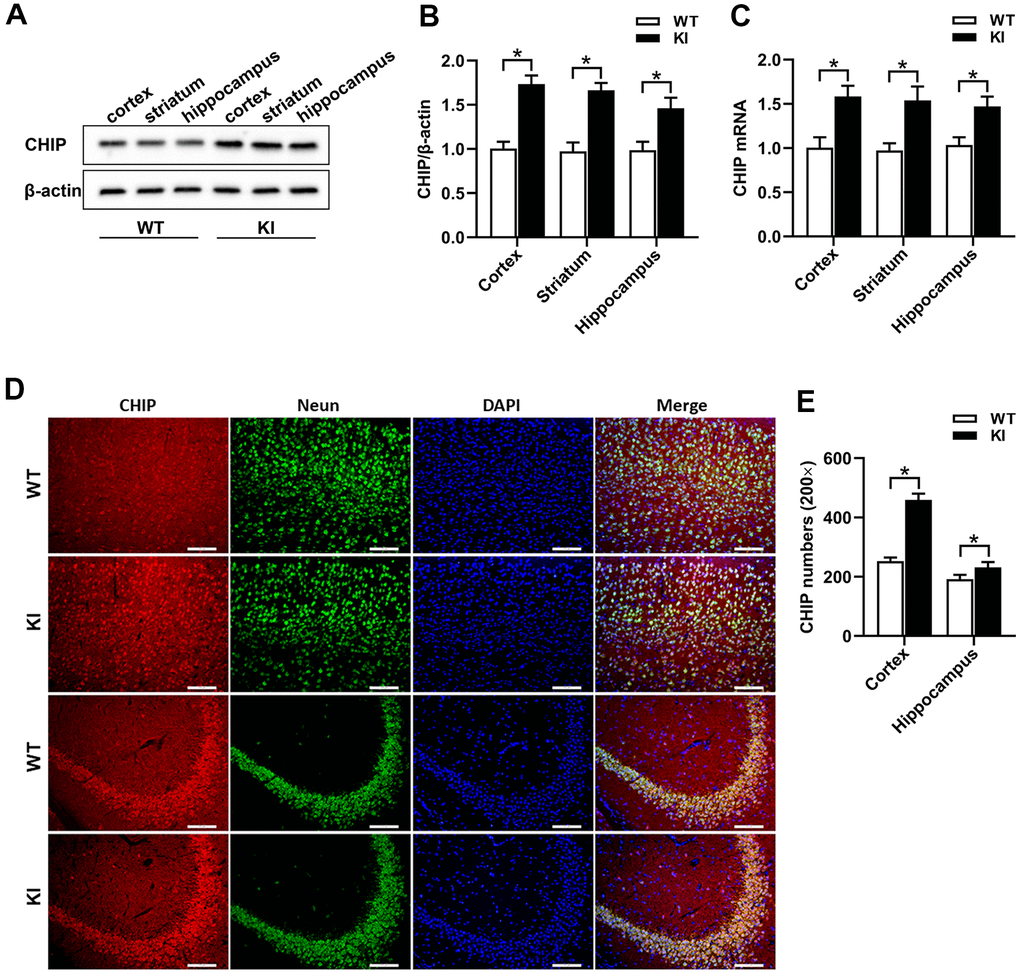
Figure 2. CHIP overexpression in CHIP KI mice. (A, B) Western blot and quantitative analysis of CHIP in the cortex, striatum, and hippocampus. (C) The mRNA expression of CHIP. (D) Immunostaining of CHIP, NeuN, and DAPI in the cortex and hippocampus of WT mice and CHIP KI mice. (E) Quantitative analysis of immunostaining showed the positive numbers of CHIP. WT, WT mice; KI, CHIP KI mice. Scale bar =100 μm. Data are presented as the mean ± SEM; n=6/group; *P < 0.05.
CHIP overexpression alleviated brain injury after MCAO
In the present study, we established MCAO mouse models using WT mice and CHIP KI mice to assess the effect of CHIP overexpression on brain injury after CIR. The cerebral infarct volume, neurological deficit scores, brain edema, and histologic characteristics of the infarct area were detected 24 h after mice were subjected to sham surgery or MCAO surgery. 2,3,5-Triphenyltetrazolium chloride (TTC) staining was performed to measure the cerebral infarct volumes of mice (Figure 3A), and the quantification results showed that the cerebral infarct volumes of CHIP KI mice were significantly decreased compared with those of WT mice after MCAO (Figure 3B). Histologic characteristics of the infarct areas were detected using hematoxylin-eosin (HE) staining and Nissl staining. The HE staining results showed that the cerebral cortex cells of both WT mice and CHIP KI mice were neatly arranged and had normal morphology after sham surgery (Figure 3C), while the cerebral cortex cells of WT mice were loosely arranged, swollen, and nuclear pyknosis after MCAO surgery, and the cerebral cortex cell damage of CHIP KI mice was less after MCAO surgery (Figure 3C). For Nissl staining, a substantial number of neurons in the infarct areas of WT mice were abnormally arranged, narrowed, and deeply stained after MCAO surgery (Figure 3C), while neuronal damage in the cortex of CHIP KI mice was reduced after MCAO surgery (Figure 3C). These results indicated that CHIP overexpression could attenuate cerebral histopathological damage after MCAO surgery. The Longa test was used to assess the neurological deficits of mice, and our results showed that Longa’s neurological scores in CHIP KI mice were lower than those of WT mice after MCAO surgery (Figure 3D), which indicated that overexpression of CHIP could improve the neurological defects in the MCAO mouse model. Brain edema was calculated by brain water content. Our results indicated that the brain water content of the ipsilateral hemisphere increased after MCAO surgery compared with sham surgery, and CHIP overexpression significantly reduced the brain water content of the ipsilateral hemisphere after MCAO (Figure 3E), which indicated that CHIP overexpression could reduce brain edema after MCAO surgery. In addition, the brain water content of the contralateral hemisphere was not significantly different between the MCAO surgery and sham surgery groups (Figure 3E). These results indicated that CHIP overexpression alleviates brain injury after MCAO surgery.
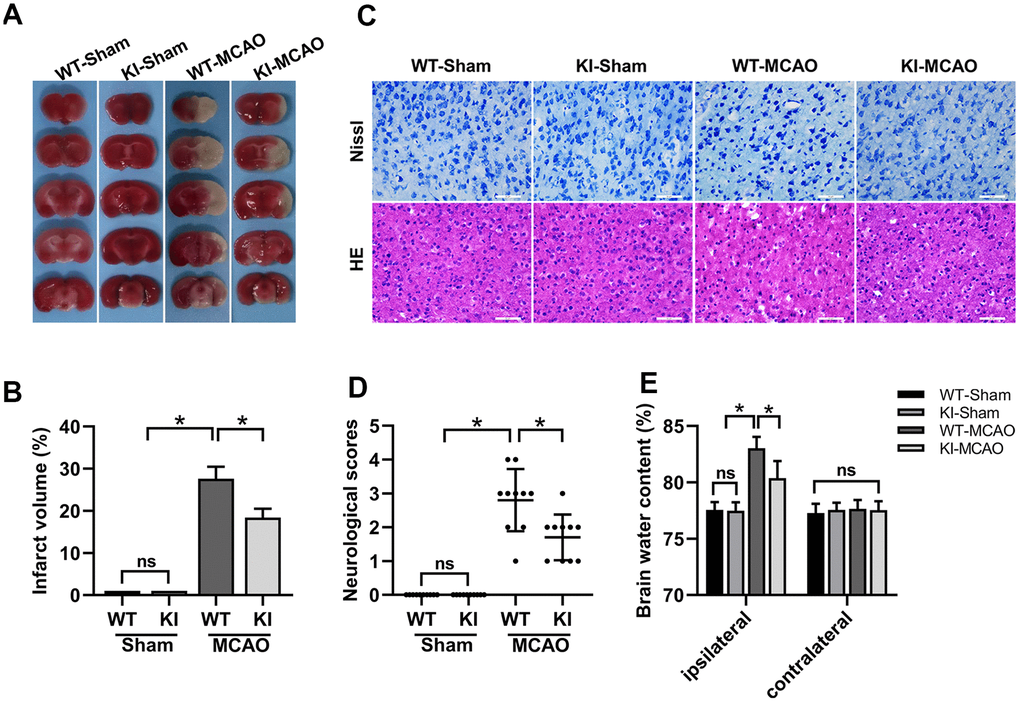
Figure 3. CHIP overexpression alleviated brain injury after MCAO. (A) TTC staining showed the cerebral infarct volume. (B) Quantitative analysis of the cerebral infarct volume. (C) HE and Nissl staining indicated the morphological characteristics. (D) Neurological scores. (E) Brain water content. Scale bar =50 μm. Data are presented as the mean ± SEM; n=6/each group and neurological scores n=10/each group; ns, no significant difference; *P < 0.05.
CHIP overexpression reduced neuronal cell death after MCAO
Neuronal cell death was detected by terminal deoxynucleotidyl transferase-mediated dUTP nick-end labeling (TUNEL) staining [31]. In the present study, TUNEL and NeuN coimmunofluorescence staining was conducted in the cortex and hippocampal CA1 regions to evaluate neuronal cell death after MCAO surgery (Figure 4A). Our results indicated that CHIP overexpression significantly reduced the number of TUNEL-positive (TUNEL+) cells in the cortex and hippocampal CA1 regions after MCAO surgery (Figure 4B), which indicated that CHIP overexpression could reduce the neuronal cell death caused by CIR.
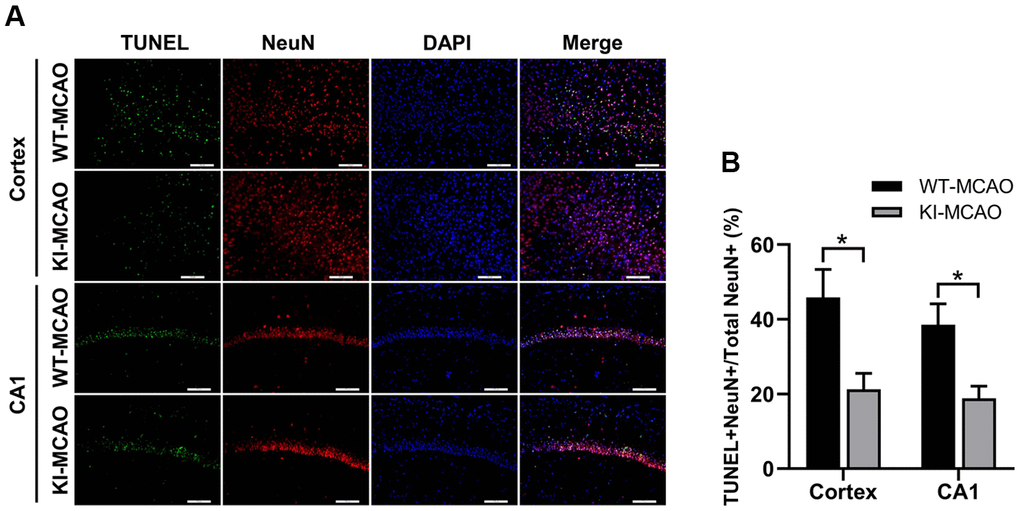
Figure 4. CHIP overexpression reduced neuronal cell death after MCAO. (A) TUNEL+ cells in the cortex and hippocampus CA1 regions were detected by TUNEL/NeuN staining after sham or MCAO surgery. (B) Quantitative analysis of total TUNEL+ ratio. Scale bar =100 μm. Data are presented as the mean ± SEM; n=6/group; ns, no significant difference; *P < 0.05.
CHIP overexpression attenuated necroptosis induced by MCAO
Necroptosis is regulated by the RIPK1/RIPK3/MLKL axis. The formation of phosphorylated RIPK3 (p-RIPK3) and phosphorylated MLKL (p-MLKL) are crucial stages in necroptosis progression and are considered hallmarks of necroptosis [32]. Thus, we checked RIPK1, RIPK3, and MLKL expression and p-RIPK3 and p-MLKL levels by western blotting to examine necroptosis after MCAO surgery (Figure 5A). Our results showed that the RIPK1, RIPK3, and MLKL levels were significantly increased in the peri-infarct tissues after MCAO surgery compared with sham surgery (Figure 5B, 5D, 5F). Concurrently, the expression of RIPK1, RIPK3, and MLKL in the CHIP KI mouse group was markedly reduced compared with that in the WT mouse group after MCAO surgery (Figure 5B, 5D, 5F). Western blotting results of p-RIPK3 and p-MLKL showed a similar trend (Figure 5C, 5E). CHIP levels in different groups are shown in Figure 5G. These results indicated that CHIP overexpression attenuates necroptosis induced by MCAO surgery.
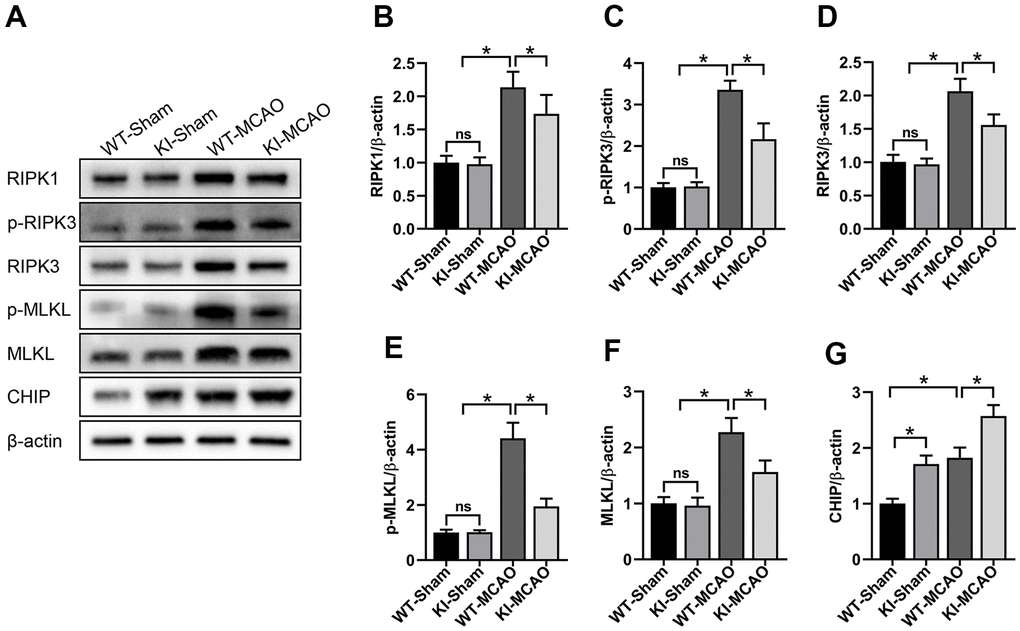
Figure 5. CHIP overexpression attenuated necroptosis induced by MCAO. (A) Western blot of RIPK1, p-RIPK3, RIPK3, p-MLKL, MLKL, and CHIP in the peri-infarct tissues after MCAO. (B–F) Quantitative analysis of RIPK1, p-RIPK3, RIPK3, p-MLKL, and MLKL in the peri-infarct tissues after MCAO. (G) Quantitative analysis of CHIP. Data are presented as the mean ± SEM; n=6/group; ns, no significant difference; *P < 0.05.
CHIP overexpression alleviated inflammation after MCAO
Inflammation contributes to brain injury following CIR. After ischemia-reperfusion, a variety of cells in brain tissue are active and release inflammatory mediators, triggering local and systemic inflammatory responses. To evaluate the effect of CHIP overexpression on inflammation after MCAO, we tested the levels of proinflammatory cytokines (TNF-α, IL-1β, and IL-6) and anti-inflammatory cytokine (interleukin-10, IL-10) in the serum and brain tissues by enzyme-linked immunosorbent assay (ELISA). Our results showed that the levels of TNF-α, IL-1β, and IL-6 were significantly increased in the serum and peri-infarct tissues after MCAO surgery (Figure 6A–6C, 6E–6G). Conversely, CHIP overexpression reduced TNF-α, IL-1β, and IL-6 levels after MCAO surgery (Figure 6A–6C, 6E–6G). Furthermore, the level of IL-10 was increased in the serum and peri-infarct tissues after MCAO, and CHIP KI mice had a higher level of IL-10 than WT mice after MCAO surgery (Figure 6D, 6H). These results suggested that CHIP overexpression exerts an anti-inflammatory effect in the MCAO mouse model.
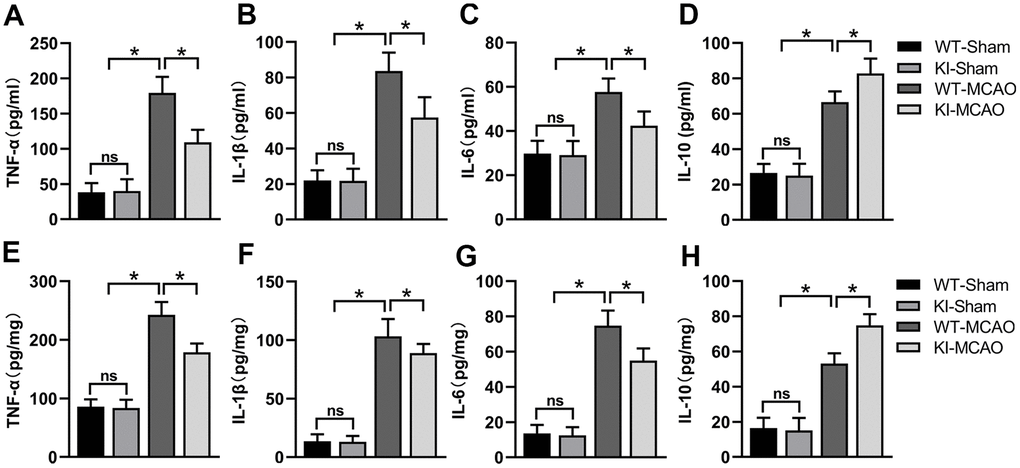
Figure 6. CHIP overexpression alleviated the inflammatory response after MCAO. (A–D) Proinflammatory mediators (TNF-α, IL-1β, IL-6) and anti-inflammatory mediator (IL-10) levels in the serum after MCAO. (E–H) Pro-inflammatory mediators (TNF-α, IL-1β, IL-6) and anti-inflammatory mediator (IL-10) in peri-infarct tissues after MCAO. Data are presented as the mean ± SEM; n=6/group; ns, no significant difference; *P < 0.05.
Discussion
In the present study, we constructed CHIP KI mice overexpressing CHIP in neural tissue and clarified the neuroprotective effects of CHIP on CIR injury using MCAO models with WT mice and CHIP KI mice. Our results indicated that CHIP expression was upregulated in the peri-infarct tissue after MCAO surgery. CHIP overexpression significantly ameliorated brain injury induced by MCAO surgery, such as improved neurological deficit scores, reduced cerebral infarct volume, and alleviated brain edema and neuronal impairment. Moreover, CHIP overexpression attenuated necroptosis and inflammation after MCAO surgery. These results indicated that the neuroprotective effects of CHIP might be due to its inhibitory effects on necroptosis and inflammation after MCAO surgery.
Previous studies have shown that CHIP overexpression exerts neuroprotective effects on some chronic neurodegenerative diseases by increasing the degradation of abnormal proteins [33, 34]. For example, CHIP overexpression mitigates memory deficits in an Alzheimer’s disease mouse model by increasing the degradation of β-amyloid protein and tau protein [35]. In addition, CHIP overexpression also has protective effects against cardiac ischemic injury [36] and some malignancies [37]. These findings indicate that upregulation of CHIP may have protective effects against multiple diseases. In the present study, we examined the role of CHIP in CIR injury, an acute neurodegenerative disease. Our results suggested that CHIP overexpression significantly ameliorated CIR injury, similar to the previous finding that CHIP overexpression exerts neuroprotective actions on acute brain injury [38]. Moreover, our previous study also indicated that increasing CHIP by anisomycin, a c-Jun N-terminal kinase agonist, can improve cell viability in an OGD cell model [25]. However, Stankowski et al. reported that chronic CHIP overexpression can be harmful to cell survival, while downregulation of CHIP expression enhanced neuronal tolerance to oxidative stress [39]. In addition, some studies have also indicated that CHIP can promote or suppress tumor progression in different tumors via different molecular mechanisms [40, 41]. Overall, these findings suggest the sophisticated functions of CHIP and different disease models can respond differently to CHIP levels.
Necroptosis, a form of programmed cell death, is induced by a series of protein kinases and is mainly regulated by RIPK1, RIPK3, and MLKL kinases. Multiple pathological conditions involve necroptosis, such as ischemia-reperfusion injury and inflammation. Studies have indicated that RIPK1 or RIPK3 inhibitors, such as necrostatin-1 (RIPK1 inhibitor) [12] and GSK’872 (RIPK3 inhibitor) [42], can protect against brain injury by blocking necroptosis after MCAO. RIPK1, RIPK3, and MLKL play a pivotal role in inducing necroptosis, and RIPK1, RIPK3, and MLKL upregulation could be common in many neurological diseases [43], including CIR injury [44]. The presence of p-RIPK3 and p-MLKL is considered a hallmark of necroptosis. Previous study has shown that CHIP attenuates necroptosis through the ubiquitylation of RIPK1 and RIPK3. Increasing CHIP levels can improve cell viability in an OGD cell model by attenuating necroptosis. In the present study, to verify the effect of CHIP on necroptosis after CIR, we constructed MCAO mouse models and detected RIPK1, RIPK3, MLKL, p-RIPK3, and p-MLKL levels. Our results indicated that RIPK1, RIPK3, and MLKL expression was significantly increased after MCAO surgery compared with sham surgery, and CHIP overexpression reduced RIPK1, RIPK3, and MLKL levels after MCAO surgery. In addition, p-RIPK3 and p-MLKL levels showed a similar trend. These results indicated that CHIP overexpression attenuates necroptosis following CIR.
Inflammation is an essential factor leading to the aggravation of brain injury caused by CIR, and reducing inflammation can mitigate brain injury after CIR. Studies have shown that inflammatory responses of damaged brain tissues involve different mechanisms, such as the activation of immune cells and necroptosis after CIR. In contrast to apoptosis, necrotic cells can release DAMPs, promoting inflammation during necroptosis. Thus, necroptosis is also considered a proinflammatory cell death mode, and blocking necroptosis can decrease inflammation [45]. Furthermore, study has shown that proinflammatory mediators, such as TNF-α, IL-1β, and IL-6, and anti-inflammatory mediators, such as IL-10, are involved in the inflammatory responses induced by CIR [46]. In the present study, we tested the levels of proinflammatory (TNF-α, IL-1β, and IL-6) and anti-inflammatory (IL-10) cytokines in the serum and peri-infarct tissues to determine whether CHIP exerts anti-inflammatory effects in MCAO mouse models. Our results showed that CHIP overexpression markedly decreased proinflammatory cytokines and increased anti-inflammatory cytokine levels, suggesting that CHIP overexpression has an anti-inflammatory effect after CIR.
Moreover, it is necessary to note that increasing CHIP levels by gene KI is difficult for clinical practice. Therefore, we need to find other ways to increase CHIP levels effectively and use them for clinical application. To date, several small-molecule agonists have been reported to upregulate CHIP expression in cell models, such as anisomycin [25], peptidoglycan [47], and 2-(4-hydroxy-3-methoxyphenyl)-benzothiazole [48]. However, it still needs to be explored whether these small-molecule agonists can upregulate CHIP expression in the brain and mitigate the brain injury induced by CIR. The adeno-associated viral vector is an effective CNS gene delivery method that can cross the blood-brain barrier [49]. Our previous study showed that adeno-associated viruses carrying the CHIP gene can upregulate CHIP expression in the mouse brain and exert protective effects in a Parkinson’s disease mouse model [50], which showed that the adeno-associated viral platform may be an efficient way to upregulate CHIP expression in the CNS. Overall, developing a safe and effective method that can induce CHIP overexpression in the CNS for CIR injury treatment may be the focus of future research.
Collectively, our study suggests that CHIP was induced in mouse brain tissue following experimental CIR, and CHIP overexpression ameliorates brain injury by attenuating necroptosis and inflammation following CIR. Taken together, CHIP may be a promising therapeutic agent for CIR injury, and its clinical application requires further research.
Materials and Methods
Animals
Adult male mice (aged 10–12 weeks, weighing 25–30 g; Henan Experimental Animal Center, Henan, China), including WT C57BL/6 mice and CHIP KI mice with a C57BL/6 background, were used in this study. CHIP KI mice were constructed as described in our previous study [50]. Briefly, CRISPR/Cas9 technology was used to construct CHIP-with-floxed-STOP-codon mice, which were crossed with Nestin-cre mice to obtain NES-CHIP mice (we named CHIP KI mice here). CHIP-KI mice can selectively increase CHIP expression in neural tissues. All mice were maintained in an environment with controlled light (12 h light/dark), humidity 55%–60%, temperature 22 ± 1° C, and group-housed at 4–5 per cage. All experiments were reviewed and approved by the Institutional Animal Care and Use Committee of Zhengzhou University, China. All experimental procedures were performed according to the guidelines of the Ethics Committee of The First Affiliated Hospital of Zhengzhou University for the care and use of experimental animals.
MCAO model
The MCAO mouse models were generated using the intraluminal filament technique [51]. Briefly, the mice were anesthetized with sodium pentobarbital and then transferred to an operating table, and their body temperatures were maintained at 37 ± 0.5° C. Next, the iodine complex was used to disinfect the incision site of the neck skin, and a midline incision at the neck was made to separate the right common carotid artery, right external carotid artery, and right internal carotid artery. A silicone-coated nylon microfilament (#L2000, Guangzhou Jialing Biotechnology Company, Guangzhou, China) was inserted into the right internal carotid artery through the right external carotid artery incision to occlude the right middle cerebral artery. The filament was withdrawn for reperfusion after it remained in position for 1 h. The mice were subjected to the same procedures in the sham surgery groups, except the right middle carotid artery was not occluded.
Experimental design
This study consisted of four parts. The first part studied the expression level of CHIP after CIR. WT mice were subjected to sham or MCAO surgery and euthanized at separate time points after reperfusion, and their brain tissues were used for western blotting, RT-PCR, and histological analyses. The second part compared the expression levels of CHIP between WT mice and CHIP KI mice. The mouse brains were harvested for western blotting, RT-PCR, and histological analysis. The animals were separated into four groups and subjected to sham or MCAO surgery in the third part and the fourth part: WT-Sham (WT mice subjected to sham surgery), KI-Sham (CHIP KI mice subjected to sham surgery), WT-MCAO (WT mice subjected to MCAO surgery), and KI-MCAO (CHIP KI mice subjected to MCAO surgery). The third part studied whether CHIP overexpression has neuroprotective roles in MCAO mouse models. Each group of animals was euthanized at 24 h after reperfusion. Their brain tissues were used for TTC staining, HE staining, Nissl staining, brain edema experiments, and TUNEL staining analyses. The fourth part examined necroptosis and inflammation after MCAO. In all experiments, the examiners were blinded to the mouse genotypes of all groups.
Neurological scores
The neurological deficits of mice were assessed according to the Longa test [52]. Briefly, the scoring criteria consisted of 0, 1, 2, 3, and 4 points, with no neurological deficits = 0 and maximal deficits = 4. Consequently, higher scores indicate worse injury.
Infarct volume
The cerebral infarct volume was measured using TTC staining. Briefly, the brain slices were incubated with 2% TTC solution (#G3005, Solarbio, Beijing, China) for 15 min at 37° C without lighting. Next, the brain slices were fixed in paraformaldehyde (#G1101, Servicebio, Wuhan, China) overnight and then photographed. TTC staining results were quantified using ImageJ software (National Institutes of Health, USA).
Brain edema
Brain edema was assessed by brain water content, calculated by the dry-wet weight method [53]. Briefly, at 24 h after reperfusion, mice were deeply anesthetized, and their brains were harvested quickly, sectioned along the midsagittal plane, and separated into the ischemic hemisphere (ipsilateral hemisphere) and nonischemic hemisphere (contralateral hemisphere). Each hemisphere was weighed immediately and then dried to obtain the wet weight and dry weight. The brain water content was calculated as [(wet weight − dry weight)/wet weight] × 100%.
Tissue preparation
The animals were deeply anesthetized following sham or MCAO surgery and subjected to different processing methods. For histological analysis, after continuous cardiac perfusion with phosphate buffer saline (PBS) and paraformaldehyde (#G1101, Servicebio), the mouse brains were extracted and fixed in paraformaldehyde overnight, dehydrated with 30% sucrose solution, and finally sectioned at 20 μm thickness. For western blot and RT-PCR analyses, the brain tissues were removed quickly and stored at −80° C after sham or MCAO surgery.
HE and Nissl staining
Histological features of the infarct areas were assessed using HE staining (#BA-4224, Baso, Zhuhai, China) and Nissl staining (#G1430, Solarbio) based on the manufacturer’s instructions. For HE staining, slices were washed in PBS to dissolve the tissue freezing medium and then submerged in hematoxylin for 3 min, washed with running water for 10 s and submerged in eosin solution for 45 s. After that, slices were dehydrated in a gradient ethanol solution, cleared in xylene, and covered with coverslips. For Nissl staining, slices were successively incubated in cresyl violet solution for 45 min at 56° C and differentiation solution for 1 min at room temperature (RT). Finally, slices were dehydrated in a gradient ethanol solution, cleared in xylene, and covered with coverslips. The images were recorded using an electron microscope (Leica DMi8, Germany).
Immunofluorescence and TUNEL staining
Slices were washed in PBS for 15 min (total 3 times, 5 min each time), and then antigen retrieval was performed using citrate antigen retrieval solution (#P0081, Beyotime, Shanghai, China) at 100° C. After that, slices were permeabilized with 0.3% Triton X-100 for 30 min and incubated with 5% normal goat serum for 60 min at RT. Slices were then incubated at 4° C overnight (approximately 12 h) with primary antibodies, including CHIP (1:200, #ab134064, Abcam) and NeuN (1:1000, #ab104224, Abcam). After that, the slices were incubated with the corresponding fluorescent antibodies, Alexa Fluor 555-labeled Donkey Anti-Rabbit IgG (1:500, #A0453, Beyotime) and Alexa Fluor 488-labeled Goat Anti-Mouse IgG (1:500, #A0428, Beyotime) for 2 h at RT. Nuclei were stained with 4′,6-diamidino-2-phenylindole (DAPI).
TUNEL (#A112-03, Vazyme Biotech, Nanjing, China) staining was used to detect neuronal cell death with DNA breakage. Coimmunostaining of TUNEL, NeuN, and DAPI was performed as previously described [54]. ImageJ software (NIH, USA) was used to analyze fluorescence images.
Western blot analysis
Brain tissues were homogenized to extract total protein. Equal amounts of protein were separated on 10% SDS-PAGE gels (#PG112, Epizyme, Shanghai, China) and then transferred to PVDF membranes (#IPFL00005, Millipore, MA, USA). After blocking with 5% bovine serum albumin for 2 h at RT, the membranes were incubated with primary antibodies against CHIP (1:10000, #ab134064, Abcam), RIPK1 (1:1000, #SAB3500420, Sigma-Aldrich), RIPK3 (1:1000, #ab62344, Abcam), MLKL (1:2000, #orb32399, Biorbyt), p-RIPK3 (1:1000, #AF7443, Affinity), p-MLKL (1:1000, #AF7420, Affinity), and β-actin (1:5000, #380624, ZEN BIO) at 4° C overnight. After that, the membranes were incubated with HRP-conjugated Goat Anti-Rabbit IgG (H+L) (1:5000, #SA00001-2, Proteintech) for 2 h at RT and then treated with enhanced chemiluminescence reagents for visualization using Image Lab software (BIO-RAD, USA).
RT-PCR analysis
Total RNA was isolated from brain tissue using an RNA isolation kit (#R401-01, Vazyme Biotech). A total of 1 μg RNA from each sample was reverse transcribed into cDNA using a cDNA synthesis kit (#R223-01, Vazyme Biotech). RT-PCR was performed using a ChamQ Universal SYBR qPCR Master Mix Kit (#Q711-02, Vazyme Biotech) on QuantStudio 5. The primer sequences were as follows: CHIP forward: 5′-CGGCAGCCCTGATAAGAGC-3′; CHIP reverse: 5′- CACAAGTGGGTTCCGAGTGAT-3′. β-actin forward: 5′- GGCTGTATTCCCCTCCATCG-3′; β-actin reverse: 5′- CCAGTTGGTAACAATGCCATGT-3′. Relative mRNA expression was quantified using the 2-ΔΔCt method, with β-actin serving as the internal control.
ELISA
The brain tissues were homogenized in PBS to obtain the tissue fluid. Blood samples were placed in sterile tubes for 1 h at RT and then centrifuged at 2000×g for 10 min at 4° C to obtain serum. ELISA kits were used to detect the concentrations of TNF-α (#E-EL-M0049c, Elabscience, Wuhan, China), IL-1β (#E-EL-M0037c, Elabscience), IL-6 (#E-EL-M0044c, Elabscience), and IL-10 (#E-EL-M0046c, Elabscience) according to the manufacturer’s instructions.
Statistical analyses
SPSS software (version 26.0; IBM Corp. USA) was used for data analysis. All data are expressed as the mean ± SEM. Two groups were compared using Student’s t test, whereas analyses of multiple groups were performed using one-way analysis of variance followed by Tukey’s post hoc test. Statistical significance was defined as a p value of < 0.05.
Author Contributions
CH Shi and YM Xu designed the research; DB Yao, S Zhang, ZW Hu did animal feeding, genotyping; DB Yao did MCAO operations; HY Luo, CY Mao, and F Liu did behavioral testing, TTC staining, and brain edema experiments; S Zhang and ZW Hu did tissue preparation; Y Fan, MB Tang did HE and Nissl staining; MJ Li, JJ Shi and JD Li did immunofluorescence and TUNEL staining; DB Yao and S Zhang did western blot and RT-PCR experiments; S Shen, LY Fan and DR Ma did ELISA experiments; DB Yao, S Zhang, and HY Luo analyzed data; DB Yao, S Zhang, and ZW Hu wrote the paper; CH Shi and YM Xu modified the paper. All authors read and approved the final manuscript.
Acknowledgments
The work was done in the Henan Key Laboratory of Cerebrovascular Diseases, The First Affiliated Hospital of Zhengzhou University, Zhengzhou University.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
This work was supported by the National Natural Science Foundation of China (Grant 81771290 and 81974211 to Dr. Changhe Shi; Grant 91849115 to Dr. Yuming Xu).
Editorial Note
This corresponding author has a verified history of publications using a personal email address for correspondence
References
- 1. Boehme AK, Esenwa C, Elkind MS. Stroke Risk Factors, Genetics, and Prevention. Circ Res. 2017; 120:472–95. https://doi.org/10.1161/CIRCRESAHA.116.308398 [PubMed]
- 2. Prabhakaran S, Ruff I, Bernstein RA. Acute stroke intervention: a systematic review. JAMA. 2015; 313:1451–62. https://doi.org/10.1001/jama.2015.3058 [PubMed]
- 3. L L, X W, Z Y. Ischemia-reperfusion Injury in the Brain: Mechanisms and Potential Therapeutic Strategies. Biochem Pharmacol (Los Angel). 2016; 5:213. https://doi.org/10.4172/2167-0501.1000213 [PubMed]
- 4. Durukan A, Tatlisumak T. Acute ischemic stroke: overview of major experimental rodent models, pathophysiology, and therapy of focal cerebral ischemia. Pharmacol Biochem Behav. 2007; 87:179–97. https://doi.org/10.1016/j.pbb.2007.04.015 [PubMed]
- 5. Hu Y, Deng H, Xu S, Zhang J. MicroRNAs Regulate Mitochondrial Function in Cerebral Ischemia-Reperfusion Injury. Int J Mol Sci. 2015; 16:24895–917. https://doi.org/10.3390/ijms161024895 [PubMed]
- 6. Liao S, Apaijai N, Chattipakorn N, Chattipakorn SC. The possible roles of necroptosis during cerebral ischemia and ischemia / reperfusion injury. Arch Biochem Biophys. 2020; 695:108629. https://doi.org/10.1016/j.abb.2020.108629 [PubMed]
- 7. Zhang S, Tang MB, Luo HY, Shi CH, Xu YM. Necroptosis in neurodegenerative diseases: a potential therapeutic target. Cell Death Dis. 2017; 8:e2905. https://doi.org/10.1038/cddis.2017.286 [PubMed]
- 8. Linkermann A, Hackl MJ, Kunzendorf U, Walczak H, Krautwald S, Jevnikar AM. Necroptosis in immunity and ischemia-reperfusion injury. Am J Transplant. 2013; 13:2797–804. https://doi.org/10.1111/ajt.12448 [PubMed]
- 9. Pasparakis M, Vandenabeele P. Necroptosis and its role in inflammation. Nature. 2015; 517:311–20. https://doi.org/10.1038/nature14191 [PubMed]
- 10. Grootjans S, Vanden Berghe T, Vandenabeele P. Initiation and execution mechanisms of necroptosis: an overview. Cell Death Differ. 2017; 24:1184–95. https://doi.org/10.1038/cdd.2017.65 [PubMed]
- 11. Jun-Long H, Yi L, Bao-Lian Z, Jia-Si L, Ning Z, Zhou-Heng Y, Xue-Jun S, Wen-Wu L. Necroptosis Signaling Pathways in Stroke: From Mechanisms to Therapies. Curr Neuropharmacol. 2018; 16:1327–39. https://doi.org/10.2174/1570159X16666180416152243 [PubMed]
- 12. Deng XX, Li SS, Sun FY. Necrostatin-1 Prevents Necroptosis in Brains after Ischemic Stroke via Inhibition of RIPK1-Mediated RIPK3/MLKL Signaling. Aging Dis. 2019; 10:807–17. https://doi.org/10.14336/AD.2018.0728 [PubMed]
- 13. Li J, Zhang J, Zhang Y, Wang Z, Song Y, Wei S, He M, You S, Jia J, Cheng J. TRAF2 protects against cerebral ischemia-induced brain injury by suppressing necroptosis. Cell Death Dis. 2019; 10:328. https://doi.org/10.1038/s41419-019-1558-5 [PubMed]
- 14. Jean WC, Spellman SR, Nussbaum ES, Low WC. Reperfusion injury after focal cerebral ischemia: the role of inflammation and the therapeutic horizon. Neurosurgery. 1998; 43:1382–96. https://doi.org/10.1097/00006123-199812000-00076 [PubMed]
- 15. Jin R, Yang G, Li G. Inflammatory mechanisms in ischemic stroke: role of inflammatory cells. J Leukoc Biol. 2010; 87:779–89. https://doi.org/10.1189/jlb.1109766 [PubMed]
- 16. Jin R, Liu L, Zhang S, Nanda A, Li G. Role of inflammation and its mediators in acute ischemic stroke. J Cardiovasc Transl Res. 2013; 6:834–51. https://doi.org/10.1007/s12265-013-9508-6 [PubMed]
- 17. Wallach D, Kang TB, Dillon CP, Green DR. Programmed necrosis in inflammation: Toward identification of the effector molecules. Science. 2016; 352:aaf2154. https://doi.org/10.1126/science.aaf2154 [PubMed]
- 18. Hao MQ, Xie LJ, Leng W, Xue RW. Trim47 is a critical regulator of cerebral ischemia-reperfusion injury through regulating apoptosis and inflammation. Biochem Biophys Res Commun. 2019; 515:651–57. https://doi.org/10.1016/j.bbrc.2019.05.065 [PubMed]
- 19. Liang Q, Yang J, He J, Chen X, Zhang H, Jia M, Liu K, Jia C, Pan Y, Wei J. Stigmasterol alleviates cerebral ischemia/reperfusion injury by attenuating inflammation and improving antioxidant defenses in rats. Biosci Rep. 2020; 40:BSR20192133. https://doi.org/10.1042/BSR20192133 [PubMed]
- 20. Liu H, Wu X, Luo J, Wang X, Guo H, Feng D, Zhao L, Bai H, Song M, Liu X, Guo W, Li X, Yue L, et al. Pterostilbene Attenuates Astrocytic Inflammation and Neuronal Oxidative Injury After Ischemia-Reperfusion by Inhibiting NF-κB Phosphorylation. Front Immunol. 2019; 10:2408. https://doi.org/10.3389/fimmu.2019.02408 [PubMed]
- 21. Ballinger CA, Connell P, Wu Y, Hu Z, Thompson LJ, Yin LY, Patterson C. Identification of CHIP, a novel tetratricopeptide repeat-containing protein that interacts with heat shock proteins and negatively regulates chaperone functions. Mol Cell Biol. 1999; 19:4535–45. https://doi.org/10.1128/MCB.19.6.4535 [PubMed]
- 22. Connell P, Ballinger CA, Jiang J, Wu Y, Thompson LJ, Höhfeld J, Patterson C. The co-chaperone CHIP regulates protein triage decisions mediated by heat-shock proteins. Nat Cell Biol. 2001; 3:93–96. https://doi.org/10.1038/35050618 [PubMed]
- 23. Alberti S, Böhse K, Arndt V, Schmitz A, Höhfeld J. The cochaperone HspBP1 inhibits the CHIP ubiquitin ligase and stimulates the maturation of the cystic fibrosis transmembrane conductance regulator. Mol Biol Cell. 2004; 15:4003–10. https://doi.org/10.1091/mbc.e04-04-0293 [PubMed]
- 24. Seo J, Lee EW, Sung H, Seong D, Dondelinger Y, Shin J, Jeong M, Lee HK, Kim JH, Han SY, Lee C, Seong JK, Vandenabeele P, Song J. CHIP controls necroptosis through ubiquitylation- and lysosome-dependent degradation of RIPK3. Nat Cell Biol. 2016; 18:291–302. https://doi.org/10.1038/ncb3314 [PubMed]
- 25. Tang MB, Li YS, Li SH, Cheng Y, Zhang S, Luo HY, Mao CY, Hu ZW, Schisler JC, Shi CH, Xu YM. Anisomycin prevents OGD-induced necroptosis by regulating the E3 ligase CHIP. Sci Rep. 2018; 8:6379. https://doi.org/10.1038/s41598-018-24414-y [PubMed]
- 26. Zhan S, Wang T, Ge W. Multiple functions of the E3 ubiquitin ligase CHIP in immunity. Int Rev Immunol. 2017; 36:300–12. https://doi.org/10.1080/08830185.2017.1309528 [PubMed]
- 27. Yang M, Wang C, Zhu X, Tang S, Shi L, Cao X, Chen T. E3 ubiquitin ligase CHIP facilitates Toll-like receptor signaling by recruiting and polyubiquitinating Src and atypical PKC{zeta}. J Exp Med. 2011; 208:2099–112. https://doi.org/10.1084/jem.20102667 [PubMed]
- 28. Wang L, Zhang TP, Zhang Y, Bi HL, Guan XM, Wang HX, Wang X, Du J, Xia YL, Li HH. Protection against doxorubicin-induced myocardial dysfunction in mice by cardiac-specific expression of carboxyl terminus of hsp70-interacting protein. Sci Rep. 2016; 6:28399. https://doi.org/10.1038/srep28399 [PubMed]
- 29. Sahara N, Murayama M, Mizoroki T, Urushitani M, Imai Y, Takahashi R, Murata S, Tanaka K, Takashima A. In vivo evidence of CHIP up-regulation attenuating tau aggregation. J Neurochem. 2005; 94:1254–63. https://doi.org/10.1111/j.1471-4159.2005.03272.x [PubMed]
- 30. Hu ZW, Yang ZH, Zhang S, Liu YT, Yang J, Wang YL, Mao CY, Zhang QM, Shi CH, Xu YM. Carboxyl Terminus of Hsp70-Interacting Protein Is Increased in Serum and Cerebrospinal Fluid of Patients With Spinocerebellar Ataxia Type 3. Front Neurol. 2019; 10:1094. https://doi.org/10.3389/fneur.2019.01094 [PubMed]
- 31. Zhang Y, Li M, Li X, Zhang H, Wang L, Wu X, Zhang H, Luo Y. Catalytically inactive RIP1 and RIP3 deficiency protect against acute ischemic stroke by inhibiting necroptosis and neuroinflammation. Cell Death Dis. 2020; 11:565. https://doi.org/10.1038/s41419-020-02770-w [PubMed]
- 32. He S, Huang S, Shen Z. Biomarkers for the detection of necroptosis. Cell Mol Life Sci. 2016; 73:2177–81. https://doi.org/10.1007/s00018-016-2192-3 [PubMed]
- 33. Wang T, Wang W, Wang Q, Xie R, Landay A, Chen D. The E3 ubiquitin ligase CHIP in normal cell function and in disease conditions. Ann N Y Acad Sci. 2020; 1460:3–10. https://doi.org/10.1111/nyas.14206 [PubMed]
- 34. Zhang S, Hu ZW, Mao CY, Shi CH, Xu YM. CHIP as a therapeutic target for neurological diseases. Cell Death Dis. 2020; 11:727. https://doi.org/10.1038/s41419-020-02953-5 [PubMed]
- 35. Lee S, Choi BR, Kim J, LaFerla FM, Park JH, Han JS, Lee KW, Kim J. Sulforaphane Upregulates the Heat Shock Protein Co-Chaperone CHIP and Clears Amyloid-β and Tau in a Mouse Model of Alzheimer’s Disease. Mol Nutr Food Res. 2018; 62:e1800240. https://doi.org/10.1002/mnfr.201800240 [PubMed]
- 36. Naito AT, Okada S, Minamino T, Iwanaga K, Liu ML, Sumida T, Nomura S, Sahara N, Mizoroki T, Takashima A, Akazawa H, Nagai T, Shiojima I, Komuro I. Promotion of CHIP-mediated p53 degradation protects the heart from ischemic injury. Circ Res. 2010; 106:1692–702. https://doi.org/10.1161/CIRCRESAHA.109.214346 [PubMed]
- 37. Seo J, Han SY, Seong D, Han HJ, Song J. Multifaceted C-terminus of HSP70-interacting protein regulates tumorigenesis via protein quality control. Arch Pharm Res. 2019; 42:63–75. https://doi.org/10.1007/s12272-018-1101-8 [PubMed]
- 38. Cabral-Miranda F, Nicoloso-Simões E, Adão-Novaes J, Chiodo V, Hauswirth WW, Linden R, Chiarini LB, Petrs-Silva H. rAAV8-733-Mediated Gene Transfer of CHIP/Stub-1 Prevents Hippocampal Neuronal Death in Experimental Brain Ischemia. Mol Ther. 2017; 25:392–400. https://doi.org/10.1016/j.ymthe.2016.11.017 [PubMed]
- 39. Stankowski JN, Zeiger SL, Cohen EL, DeFranco DB, Cai J, McLaughlin B. C-terminus of heat shock cognate 70 interacting protein increases following stroke and impairs survival against acute oxidative stress. Antioxid Redox Signal. 2011; 14:1787–801. https://doi.org/10.1089/ars.2010.3300 [PubMed]
- 40. Cheng L, Zang J, Dai HJ, Li F, Guo F. Ubiquitin ligase CHIP functions as an oncogene and activates the AKT signaling pathway in prostate cancer. Int J Oncol. 2018; 53:203–14. https://doi.org/10.3892/ijo.2018.4377 [PubMed]
- 41. Wang Y, Ren F, Wang Y, Feng Y, Wang D, Jia B, Qiu Y, Wang S, Yu J, Sung JJ, Xu J, Zeps N, Chang Z. CHIP/Stub1 functions as a tumor suppressor and represses NF-κB-mediated signaling in colorectal cancer. Carcinogenesis. 2014; 35:983–91. https://doi.org/10.1093/carcin/bgt393 [PubMed]
- 42. Chen T, Pan H, Li J, Xu H, Jin H, Qian C, Yan F, Chen J, Wang C, Chen J, Wang L, Chen G. Inhibiting of RIPK3 attenuates early brain injury following subarachnoid hemorrhage: Possibly through alleviating necroptosis. Biomed Pharmacother. 2018; 107:563–70. https://doi.org/10.1016/j.biopha.2018.08.056 [PubMed]
- 43. Liu T, Bao YH, Wang Y, Jiang JY. The role of necroptosis in neurosurgical diseases. Braz J Med Biol Res. 2015; 48:292–98. https://doi.org/10.1590/1414-431X20144310 [PubMed]
- 44. Yang M, Lv Y, Tian X, Lou J, An R, Zhang Q, Li M, Xu L, Dong Z. Neuroprotective Effect of β-Caryophyllene on Cerebral Ischemia-Reperfusion Injury via Regulation of Necroptotic Neuronal Death and Inflammation: In Vivo and in Vitro. Front Neurosci. 2017; 11:583. https://doi.org/10.3389/fnins.2017.00583 [PubMed]
- 45. Dhuriya YK, Sharma D. Necroptosis: a regulated inflammatory mode of cell death. J Neuroinflammation. 2018; 15:199. https://doi.org/10.1186/s12974-018-1235-0 [PubMed]
- 46. Zhang Z, Xu C, Hao J, Zhang M, Wang Z, Yin T, Lin K, Liu W, Jiang Q, Li Z, Wang D, Mao Z, Tong H, Zhang L. Beneficial consequences of Lupeol on middle cerebral artery-induced cerebral ischemia in the rat involves Nrf2 and P38 MAPK modulation. Metab Brain Dis. 2020; 35:841–48. https://doi.org/10.1007/s11011-020-00565-8 [PubMed]
- 47. Meng Y, Chen C, Wang L, Wang X, Tian C, Du J, Li HH. Toll-like receptor-2 ligand peptidoglycan upregulates expression and ubiquitin ligase activity of CHIP through JNK pathway. Cell Physiol Biochem. 2013; 32:1097–105. https://doi.org/10.1159/000354509 [PubMed]
- 48. Hiyoshi H, Goto N, Tsuchiya M, Iida K, Nakajima Y, Hirata N, Kanda Y, Nagasawa K, Yanagisawa J. 2-(4-Hydroxy-3-methoxyphenyl)-benzothiazole suppresses tumor progression and metastatic potential of breast cancer cells by inducing ubiquitin ligase CHIP. Sci Rep. 2014; 4:7095. https://doi.org/10.1038/srep07095 [PubMed]
- 49. Deverman BE, Pravdo PL, Simpson BP, Kumar SR, Chan KY, Banerjee A, Wu WL, Yang B, Huber N, Pasca SP, Gradinaru V. Cre-dependent selection yields AAV variants for widespread gene transfer to the adult brain. Nat Biotechnol. 2016; 34:204–209. https://doi.org/10.1038/nbt.3440 [PubMed]
- 50. Hu Z, Mao C, Wang H, Zhang Z, Zhang S, Luo H, Tang M, Yang J, Yuan Y, Wang Y, Liu Y, Fan L, Zhang Q, et al. CHIP protects against MPP+/MPTP-induced damage by regulating Drp1 in two models of Parkinson’s disease. Aging (Albany NY). 2021; 13:1458–72. https://doi.org/10.18632/aging.202389 [PubMed]
- 51. Liu X, Hu R, Pei L, Si P, Wang C, Tian X, Wang X, Liu H, Wang B, Xia Z, Xu Y, Song B. Regulatory T cell is critical for interleukin-33-mediated neuroprotection against stroke. Exp Neurol. 2020; 328:113233. https://doi.org/10.1016/j.expneurol.2020.113233 [PubMed]
- 52. Bachour SP, Hevesi M, Bachour O, Sweis BM, Mahmoudi J, Brekke JA, Divani AA. Comparisons between Garcia, Modo, and Longa rodent stroke scales: Optimizing resource allocation in rat models of focal middle cerebral artery occlusion. J Neurol Sci. 2016; 364:136–40. https://doi.org/10.1016/j.jns.2016.03.029 [PubMed]
- 53. Lo AC, Chen AY, Hung VK, Yaw LP, Fung MK, Ho MC, Tsang MC, Chung SS, Chung SK. Endothelin-1 overexpression leads to further water accumulation and brain edema after middle cerebral artery occlusion via aquaporin 4 expression in astrocytic end-feet. J Cereb Blood Flow Metab. 2005; 25:998–1011. https://doi.org/10.1038/sj.jcbfm.9600108 [PubMed]
- 54. Li QQ, Ding DH, Wang XY, Sun YY, Wu J. Lipoxin A4 regulates microglial M1/M2 polarization after cerebral ischemia-reperfusion injury via the Notch signaling pathway. Exp Neurol. 2021; 339:113645. https://doi.org/10.1016/j.expneurol.2021.113645 [PubMed]